Francesco Lucio Clinical case Pleural mesothelioma - Appuntamenti a Fisica
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Clinical case Pleural mesothelioma Francesco Lucio
Malignat Pleural Mesothelioma
• Mesothelioma is a rare malignant
tumour originating from the cells
lining the mesothelial surface of
the coelomic cavities of the body.
The background incidence of
MPM is very low.
• Asbestos is the principal
etiological agent of MPM. The first
studies on the association
between asbestos and MPM were
published in the 1960s. Since
most asbestos exposure is work-
related, mesothelioma is an
occupational disease in the
majority of cases
J.P. van Meerbeeck et al. / Critical Reviews in Oncology/Hematology 78 (2011) 92–111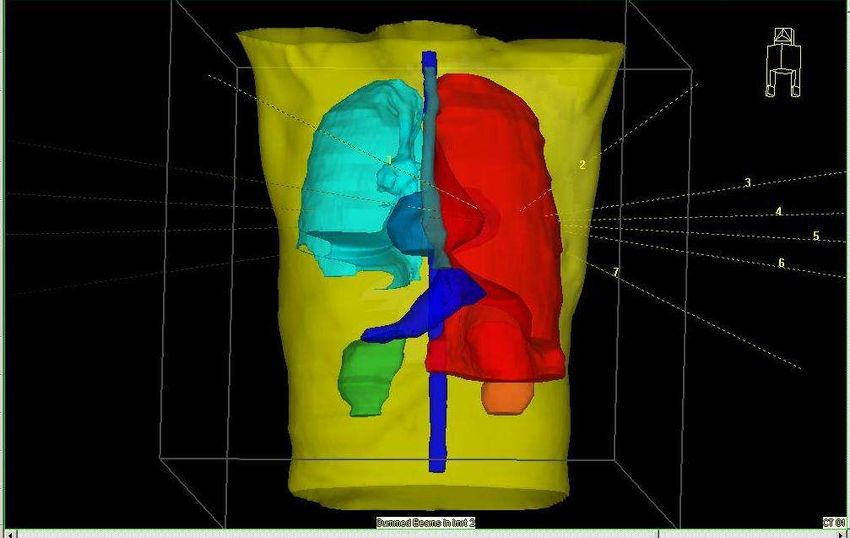
Consumo di amianto (1915-1992) e decessi1 per mesotelioma
osservati2 (1970-1999) e previsti (2000-2030) in Italia
Stima1 picco
Anno in cui l'amianto è stato proibito 2017:
1992
820-940 MM
3000 900
40-45 per anno
anni* 800
2500
700 Consumo procapite
Consumo di amianto pro capite
(Tonnnellate per milione di ab.)
Numero annuale di decessi
2000 600 Ossevati
Atteso
500
1500 Proiezione
400
1000 300 Media Mobile su 5 per.
(Ossevati)
200 Media Mobile su 5 per.
500 (Consumo procapite)
100
2017
0 0 1Peto et al
1912
1917
1922
1927
1932
1937
1942
1947
1952
1957
1962
1967
1972
1977
1982
1987
1992
1997
2002
2007
2012
2017
2022
2027
*Selikoff IARC Scientific Publication
Anno
FABIO MONTANARO1, ALESSANDRO MARINACCIO2 et al.
1 Uomini, 25-89 anni 1977
2 Stimati: decessi per tumore pleurico * 0.73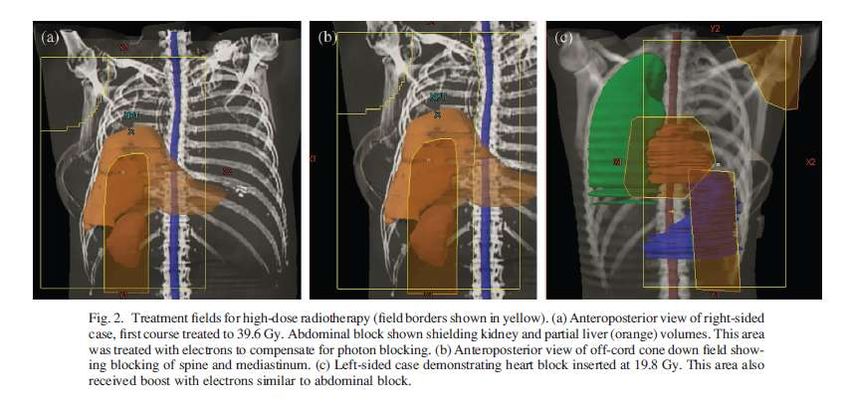
Terapia dei Mesoteliomi Nessuna terapia • (supporto) • Radioterapia esclusiva •Pleurectomia/Decorticazion e • P/D + RT postoperatoria + •PleuroPneumonEctomia/PP E PPE + RT postoperatoria +/- • + + CT
Radiotherapy in MPM
• Palliative radiotherapy:
– for palliation of symptoms for patients with advanced disease
– As for other palliative indications,hypofractionation with 4G fractions is
currently advocated, for a total dose bio-equivalence of 30–36 Gy.
• Prophylactic radiotherapy
– to reduce recurrences at sites of diagnostic or therapeutic instrument
insertion
– irradiation with a 7 Gray (Gy) fractionation for three consecutive days, in
the four weeks
• Postoperative/Radical Treatment
– RT as part of multimodal definitive treatment to improve locoregional
control after resection of early stage disease
– total dose more than 54 Gy to the hemithorax. The use of radiation
therapy to the full hemithorax is limited by critical organs (lung, liver,
heart, spinal cord, esophagus and Kidney).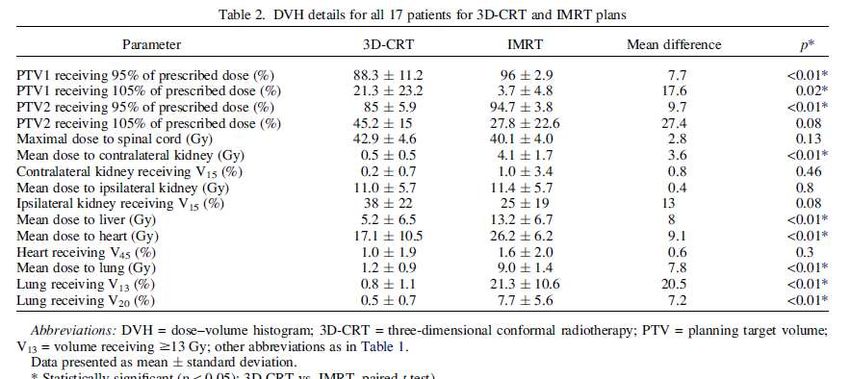
Radiotherapy
ESOPHAGUS
CONTROLATERAL
LUNG
STOMACH PTV
CONTROLATERAL
IPSLATERAL
KIDNEY KIDNEY
SPINE
Large irregularly shaped area at risk
Proximity of critical structures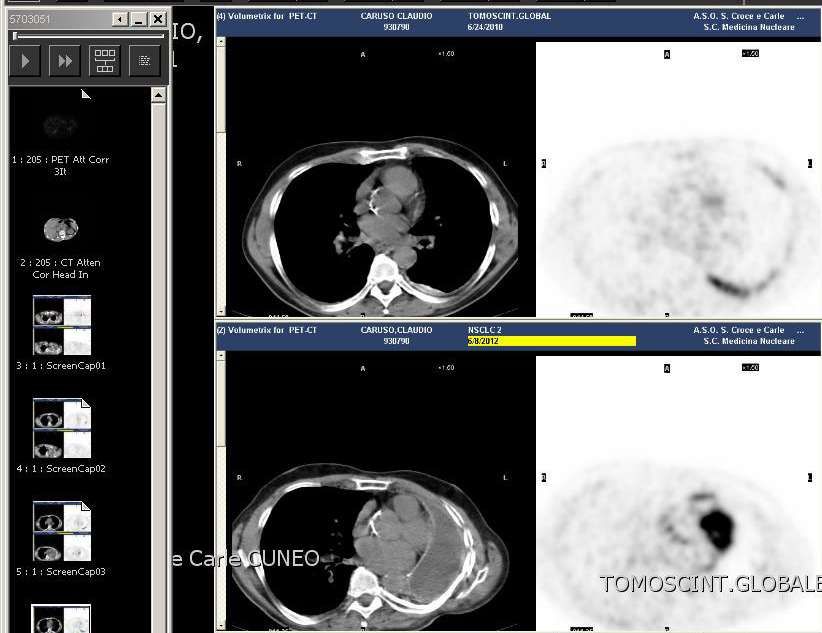
3D CRT
• Moderate dose radiotherapy MDRT
– AP/PA 30 Gy
– The mediastinum was treated to an additional 10 Gy
for a cumulative dose of 40 Gy.
A. M. ALLEN et al.2007
3D CRT
• High Dose RT
A. M. ALLEN et al.2007
– AP/PA 39.6 Gy
– Abdominal block to shield kifney and partial liver- area treat with
electrons.
– AP/PA off cord to block spine and mediastinum. Heart block eventually
for left lung
– Boost 14.4 Gy
e-
e-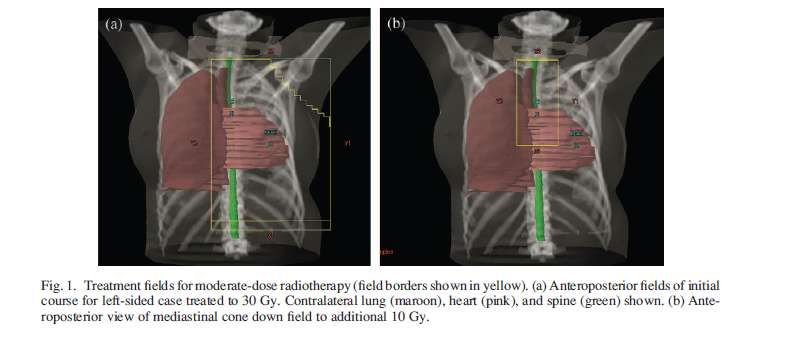
ADJUVANT MALIGNANT MESOTHELIOMA
RADIOTHERAPY: HOW MANY DIFFICULTIES!
Russi, Lucio et al IJROBP 2006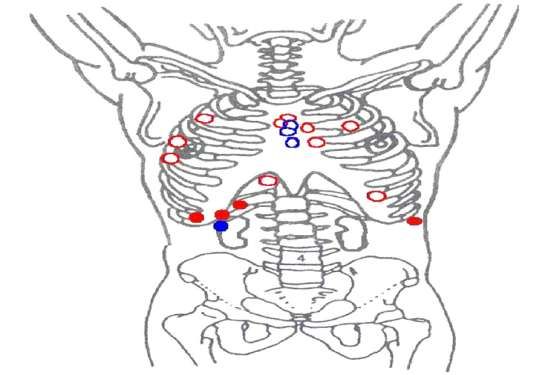
3D CRT – moderate vs high
radiotherapy
A. M. ALLEN et al.2007
It suggested that a greater radiation dose and a larger volume to include
the entire hemithorax and adjacent areas could perhaps reduce the
locoregional failure rateQuale Bersaglio?
65% 30%
P/D 11%
EPP
Flores 22%
Flores
‘08
P/D
21%
39%
Pleurectomia/decortica EPP PleuroPneumonEctomia
zione [P/D] rimozione di:
– rimuove la pleura e il Polmone
Pleura parietale e viscerale
mesotelioma senza
Diaframma
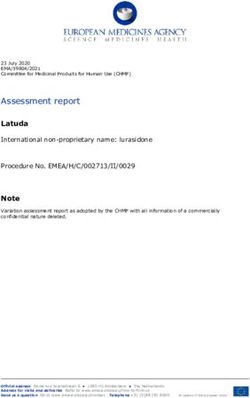
rimuovere il polmone. Pericardio3D CRT vs IMRT
PTV1
45Gy
PTV2 56-
57Gy
KRAYENBUEHL et al, Int. J. Radiation Oncology Biol. Phys., Vol. 69, No. 5, pp. 1593–1599, 20073D CRT vs IMRT
IMRT seems to be the superior technique to deliver
greater doses with better dose homogeneity, even
though the larger doses to the OARs, especially in the
contralateral lung, must be taken into consideration
KRAYENBUEHL et al, Int. J. Radiation Oncology Biol. Phys., Vol. 69, No. 5, pp. 1593–1599,
2007IMRT vs tomotherapy Target homogeneity and coverage could be significantly improved with tomotherapy
IMRT vs tomotherapy slight advantages in normal tissue sparing
IMRT vs RA
RA demonstrated similar target coverage and better dose sparing to the OARs
compared with fixed-gantry IMRT.
The time required to deliver the dose was much lower
M. SCORSETTI et al. 2010WARNING
Fatal Radiation Pneumonitis
Conventional RT N° of pts % of Fatal RP
Toronto General Hospital 29 0%
University of Padua 15 0%
MSKCC 54 0%
BWH 183 0%
IMRT N° of pts % of Fatal RP
Allen, BWH ’06 13 46%
NKI, Denmark ’08 26 15%
Miles, Duke ’08 13 8%
Rice, MDACC ‘07 63 10%
Gupta et al. 2009WARNING
New DVH for controlateral lung
DVHs for controlateral lung
Study
MLD V20
Allen, BWH ’06 > 13 Gy > 15%
Miles, Duke ’08 > 11 Gy > 7%
Rice, MDACC ‘07 > 8.5 Gy > 7%
most frequent side effects
ipsilateral kidney is largely included in
the radiation field,
contralateral kidney should in fact
contribute to the entire renal perfusionClinical Case
Patient Profile
• Uomo
• 30/1/51 59 anni
• Esposizione professionale all’amianto
• 25/5/2010 biopsia pleurica
• 22/6/2010 chirurgia mediastino scopia cervicale
• 6/7/10 pleuropneumectomia
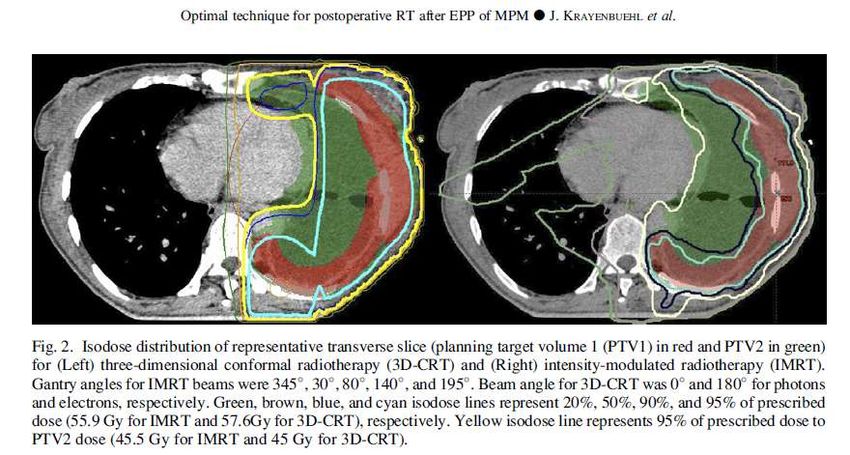
• istologico pT1bpN0IMRT
11/11/2010 inizio PORT
1.8 Gy x 27 sed = 48.6Gy
S&S 7 beams – 83 segments
46 GyCI95=0.16 DVH
HImax=1.16 D98=44.7Gy
D50=48.5Gy
V5=30%
MLD =5Gy D2=51.8Gy
V20=2.5%Pre-treatment dosimetry
Gamma(4% 3mm)= 96.5%
Omnipro with EBT in CIRS
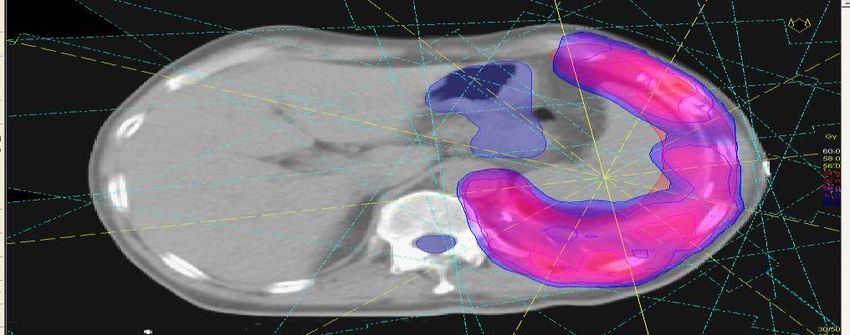
phantomPET – CT 8/6/2012
2010
Captazione
pleurica
2012Conclusion
Conclusion –The most appropriate timing … should be discussed upfront in a multidisciplinary board, including radiation oncologists. –Dose of radiation for adjuvant treatment following EPP should be 50–54 Gy in 1.8–2 Gy daily fractions, with 60 Gy delivered to macroscopic residual tumors if any. –IMRT is a promising treatment technique… –reduce radiation exposure of the remaining lung, as the risk of fatal pneumonitis with IMRT (V20 < 10%; mean lung dose preferably
You can also read