Getting answers from babies about autism
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Review
Getting answers from babies
about autism
Mayada Elsabbagh and Mark H. Johnson
Centre for Brain and Cognitive Development, Birkbeck, University of London, Henry Wellcome Building, London, WC1E 7HX, UK
Because autism is rarely diagnosed before two years of several characteristics of ASD might not be atypical, but
age, little is known about its early symptoms and causes. their co-occurrence and severity within an individual
In order to determine the earliest manifestations of the determine whether they manifest as normative differ-
condition, recent interest has focused on infants at ences, as opposed to diagnosable symptoms. The BAP
genetic risk for autism. Current evidence indicates that includes overlapping clinical characteristics [7] as well
overt behavioural symptoms emerge around the end of as differences in face processing [6,8], theory of mind [9],
the first year. However, studies using laboratory brain executive function [10,11] and central coherence [12].
function measures have reported differences in groups Further interest in studying infant siblings comes from
of infants at-risk compared with low-risk controls during the field of developmental cognitive neuroscience, where
their first year. Some infants displaying such early differ- studying atypical developmental trajectories is thought to
ences, however, do not subsequently receive a diagno- illuminate basic mechanisms that underlie the emergence
sis. As the search for early markers continues, infants at- of typical social and cognitive skills and their associated
risk present a persuasive model for gene by environment brain functions. This would in turn help address challen-
interactions leading to variable developmental path- ging questions regarding the development of the ‘social
ways. brain’ [13]. Recently, several new methods have been
developed for studying behaviour, cognition and brain
What can babies tell us about autism? function in very young infants (Figure 1; Box 2). Our goal
Autism Spectrum Disorders (ASD) affect 1 in 100 to150 in this article is to present an overview of current infant
children [1]. The annual societal cost of ASD in the UK siblings research within a broader context of developmen-
exceeds £27 billion [2]. Our current knowledge of the early tal cognitive neuroscience, and to explore the potential
neural, behavioural and cognitive profile is very poor, and implications that studies of infant siblings have on our
little is known about the underlying causes of ASD or the basic understanding of gene and environment interactions
process through which symptoms emerge. Because a con- in early functional brain development.
firmed diagnosis of ASD can only be made from around two
or three years of age (Box 1) researchers, until recently, Does ASD emerge over time?
have relied on limited retrospective data on infants Early signs
younger than two years of age prior to diagnosis [3,4]. It Despite recent advances in our understanding of the
is against this background of scientific and clinical chal- genetic and neurobiological basis of ASD, the condition
lenges that investigators have recently turned to the pro- is currently diagnosed on the basis of behavioural charac-
spective study of younger siblings of children already teristics that can take qualitatively different forms in
diagnosed with ASD (often referred to as ‘infant siblings’). infancy. Tools currently used for screening and diagnosis,
Although community-based studies are needed to deter- relating to the three areas affected in ASD (social abilities,
mine recurrence risk in these infants, some studies report communication and repetitive behaviours), have been vali-
that around 20 per cent of younger siblings go on to dated for children of 18 months and older but not for
a diagnosis. Studies with this risk group have only younger infants (Box 1). Thus, most approaches to study-
recently begun in earnest, in part due to the large number ing infant siblings aim to identify risk markers through
of infants that are required to be studied over a period of precursors of later developing symptoms. Because ASD is a
several years before revealing the minority who receive a complex condition that encompasses characteristics out-
diagnosis. side the social domain (e.g. motor coordination and visual
Another motivation for research in this area is that attention), some investigators view these as equally
infants at-risk, by virtue of being genetic relatives of important candidate risk markers, despite the fact that
children with autism, might share some characteristics such characteristics are not specific to, or universal in ASD
with affected individuals, even if they do not themselves go [4,14,15].
on to receive a diagnosis. In adults the Broader Autism Emerging findings indicate that during their first year
Phenotype (BAP) refers to behavioural and brain charac- many infants who go on to a later diagnosis show surpris-
teristics associated with ASD found not only in affected ingly few overt behavioural signs of atypicality. As a group,
individuals, but also in their relatives [5–7]. As such, these infants might interact well with their caregivers and
show the expected level of social reciprocity for their age
Corresponding author: Elsabbagh, M. (m.elsabbagh@bbk.ac.uk). [15–17]. However, during their second year they begin to
1364-6613/$ – see front matter ß 2009 Elsevier Ltd. All rights reserved. doi:10.1016/j.tics.2009.12.005 81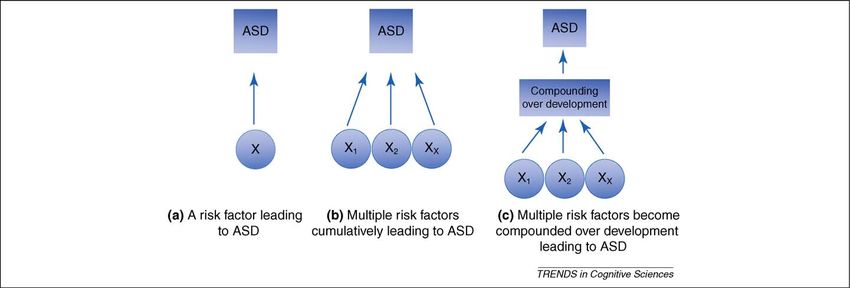
Review Trends in Cognitive Sciences Vol.14 No.2
Box 1. Diagnosis and characteristics of ASD in young
children
The process of identifying and diagnosing ASD varies among
clinicians and communities. Three elements are commonly re-
garded as essential. These are surveillance, screening and diagnosis
[56]. Diagnostic evaluation requires specialist and interdisciplinary
clinical judgement relying on a variety of sources including direct
observation and assessment as well as parent report. Increasingly,
validated instruments including the Autism Diagnostic Observation
Schedule (ADOS) and the Autism Diagnostic Interview (ADI) are
used in the clinical setting. These instruments can lead to
provisional diagnoses from as early as 18 months of age but tend
to be more reliable with increasing age of the child.
Despite the lack of information about ASD in the very early years,
some research has focused on young children diagnosed with ASD
at 2 to 3 years of age (see [4] for a detailed review). The evidence
indicates that ASD in early childhood is associated with impair-
ments in several social-communicative skills including social
orienting and scanning, face and eye contact processing, imitation,
and communication [57,58]. Impairments in joint attention are
specifically characteristic of young children with ASD, relative to
children with developmental delay or other conditions. Moreover,
individual differences in joint attention skills among children with
autism have been associated with difficulties in other social and
communication skills. It has therefore been proposed that early
impairment in joint attention might lead to difficulties in other areas
of development [57,58].
After the onset of these symptoms in the early years, different sets
of abilities show varying trajectories of development. For example,
some abilities, such as face processing, can begin as significantly
impaired but over time compensatory strategies and atypical neural
systems can restore behavioural performance to within the typical
range. By contrast, difficulties in joint attention remain characteristic
of young children with ASD.
show differences across a range of measures, summarised
in Table 1. These early signs of ASD, that can first appear
around 12 months, include several precursors to later
developing symptoms in social and communicative beha-
viours. Other studies indicate that early signs might in-
clude behaviours that fall outside the range used in
diagnosing ASD in children, for example motor and tem-
peramental characteristics. The nature of early beha-
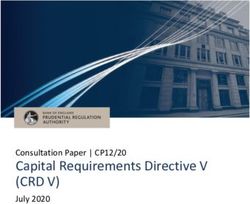
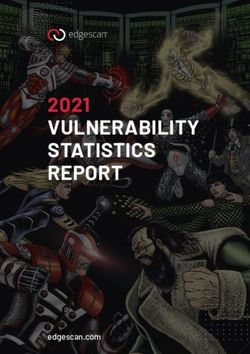
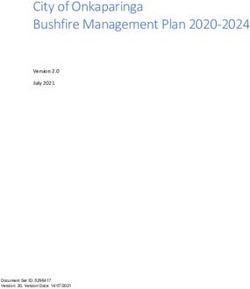
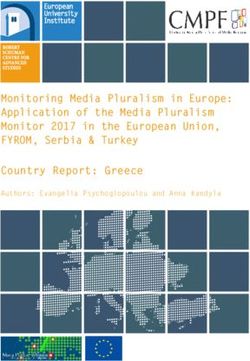
vioural signs seems to vary between infants and can Figure 1. Converging clinical and experimental research methods for studying
also change over time. Even by 18 months, diagnosis is autism in infancy. (a) The Autism Observation Schedule for Infants (AOSI) is a
semi-structured tool for the assessment of early behavioural expression of risk for
at best tentative and its stability is poor. However, differ-
autism in infants. (b) A baby with her parents having an EEG sensor net fitted in
ences in the affected group do become increasingly clear preparation for a study. (c) Group-level differences between infants at-risk for
after this age. autism and a control group in treatment of direct gaze relative to averted gaze
revealed by ERP [32].
Different pathways towards an ASD diagnosis?
notion that there are multiple pathways to ASD. Tradition-
The lack of uniformity in the nature and timing of early
ally, two subgroups have been hypothesised based on their
markers among infants, and their probabilistic nature in
trajectory of symptoms [24]. The first trajectory character-
terms of predicting diagnosis, has generated interest in the
ises infants whose symptoms appear early in development
and become clearer with age. The second trajectory
Table 1. Characteristics of ASD emerging between 12 and 24 involves typical initial stages of development followed by
months. Early signs are variable and initially have low a phase of ‘regression’. Prospective studies of infant sib-
predictive value that then increases with age lings have lent support to the first of these trajectories in
Deficits and delays in emerging joint attention [17,18] which early subtle signs first appear around the end of the
Decreased response to name [19] first year then develop into clearer symptoms by two years.
Decreased imitation [15] Notwithstanding this pattern, the evidence also indicates
Delays in verbal and non-verbal communication [20]
significant variation in the rate of change over time among
Motor delay [17]
Elevated frequency of repetitive behaviours, e.g. hand waving [21] infant siblings [25–27]. In some cases of ASD, delays or
Atypical visuo-motor exploration of objects [22] atypicality can begin later and appear more gradually,
Extremes of temperament [23] leading to a plateau in typical skills. The regression
Decreased flexibility in disengaging visual attention [15] pathway hypothesised to occur in a minority of children
82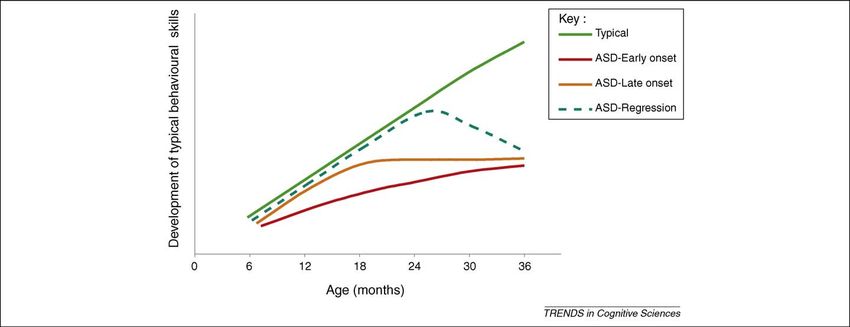
Review Trends in Cognitive Sciences Vol.14 No.2
Box 2. Methods for studying emerging ASD Getting beneath behaviour
Whereas the majority of infant siblings studies to date
Several complementary approaches for investigating ASD symp-
toms or precursors in the early years have been pursued. One of the have searched for atypicalities in social behaviour, a few
first innovative behavioural approaches, the Autism Observation laboratories have recently used methods from developmen-
Scale for Infants (AOSI), utilises a battery of risk markers [14,37,59]. tal cognitive neuroscience with this risk group. The motiv-
The semi-structured method (Figure 1a) focuses on precursors of ation is that more direct measurements of brain function or
symptoms found in older children, including response to name, eye
contact, social reciprocity and imitation. The battery also includes
cognition might reveal indicators of atypical development
items assessing atypical visual and motor skills. Some infants later before these become evident in the overt social behaviour of
diagnosed with ASD begin to be differentiated from the control the infant. Because work with such methods is relatively
group of infants with no family history of autism at around 12 new, there is little current data on the predictive value of
months. At that age, siblings who do not go on to a diagnosis can the measures in relation to diagnostic outcome at three
also exhibit some markers of risk falling between affected siblings
and control groups.
years or beyond. However, in contrast to the behavioural
Clinical research methods have been complemented by experi- studies described above, such methods have already docu-
mental methods such as direct measurement of naturally occurring mented differences during the first year between groups of
activity in the brain (EEG; Figure 1b). For example, converging infant siblings and low-risk control groups. For example,
analytic methods have revealed group-level differences in response
measurement of saccadic reaction time in tasks targeting
to pictures displaying direct compared to averted gaze within the
first year of life in infant siblings (Figure 1c), as well as baseline developing brain attention networks have shown reduced
differences in resting EEG response. These findings might reflect flexibility in disengaging from a central stimulus to orient
early manifestations of genetic risk for ASD across multiple towards a peripheral one [28], a finding parallel to that
developing neural systems, including eye gaze processing, a observed in older children diagnosed with ASD [29].
developmental precursor to joint attention.
Furthermore, the study of contrast thresholds in infants
Due to the technical challenges involved in using structural brain
imaging methods with infants, technologies such as Magnetic at-risk highlighted differences in neural systems mediat-
Resonance Imaging have only recently started to be used in studies ing early visual processing [30]. More direct electrophysio-
with infant siblings. One hypothesis currently being tested is logical measurement of brain activity using Event Related
whether an atypically rapid rate of brain growth can be used as an Potentials (ERP) has found early group differences in
early marker of ASD. This builds on previous findings of differences
in brain size in young children [60] and underconnectivity in adults
response to face stimuli [31] and in sensitivity to the
with ASD [61]. The proposal is that variations in head growth direction of eye gaze, a developmental precursor to joint
trajectory within the infancy period lead to both functional and attention [32]. Other emerging findings indicate differ-
anatomical consequences, which could explain the variability in ences in the risk group in resting state spontaneous
trajectories of emerging symptoms [62]. A promising future
EEG activity at the gamma frequency [32].
development will be the incorporation of multiple behavioural,
brain imaging, and genetic measures within individual infants. There are at least three reasons for differences in the
overall pattern of results from measures of overt social
behaviour and measures of underlying brain functions.
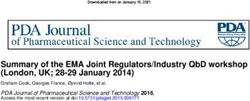
diagnosed with ASD has yet to be established in infant First, as mentioned above, it might be that methods from
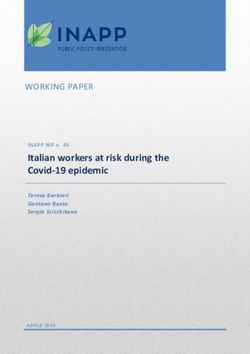
siblings studies. These hypothetical trajectories (Figure 2) developmental cognitive neuroscience are simply more
are based on findings from behavioural studies, and it sensitive at indicating risk in individual infants earlier
remains possible that clearer or more consistent trajec- in development. Until studies using these methods have
tories will become apparent when underlying functional followed up large cohorts of infants at-risk to the point of
brain development is understood. diagnosis this issue will remain unresolved. A second
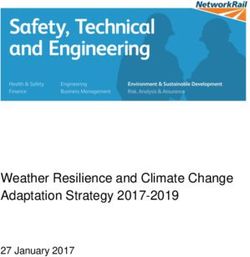
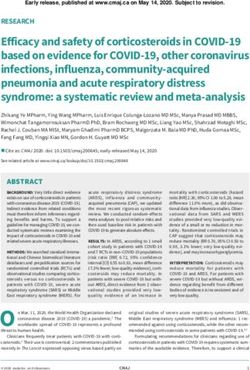
Figure 2. Siblings studies have highlighted variation in the nature and rate of change in behaviour in infants at risk. This has led to proposals of hypothetical variable
trajectories as illustrated. Available findings support variability in onset of clear behavioural symptoms whereas the regression trajectory has not been established in infant
siblings.
83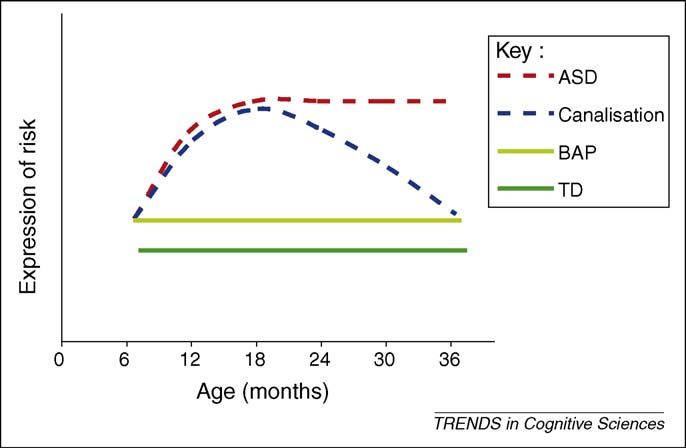
Review Trends in Cognitive Sciences Vol.14 No.2
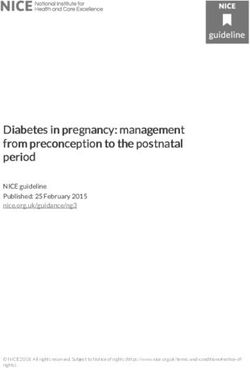
account builds on the view of some authors that their perturbation affects some individuals and not others [39].
findings constitute group-level differences that are not In Figure 3 we illustrate some of the underlying assump-
attributable to the small number of infants going on to tions about how genetic or environmental risk factors oper-
receive an ASD diagnosis (Box 2), and thus that they ating within the infancy period give rise to later behavioural
represent an early form of the BAP. This account might outcomes. Although our focus here are those factors leading
help explain some of the current inconsistencies in describ- to ASD, it is likely that similar factors might also contribute
ing the behavioural phenotype in ‘unaffected’ siblings to other behavioural phenotypes such as those observed in
(those who do not go on to receive a later diagnosis). When language or attention disorders [28].
considering behaviour, unaffected siblings appear to Since pioneering studies have estimated heritability for
muddy the waters in terms of finding early markers for ASD to exceed 90% [40,41] much research has focused on
ASD. Behavioural differences between this group, affected genetic risk as contributing to the emergence of the con-
siblings and low-risk control infants are difficult to detect dition. Once viewed as a realistic endeavour, the search for
at six months of age [16,33,34]. Between 12 and 24 months, candidate genes as causal factors has been hampered by
groups inconsistently overlap in some early signs [35–37]. heterogeneity in DNA loci and variable penetrance and
At least in some studies, affected and unaffected siblings expression. Most geneticists have now abandoned the
continue to be indistinguishable early in this developmen- notion of susceptibility genes of major effect as accounting
tal period but diverge in their trajectories over time [37]. for a large number of ASD cases. Emerging consensus
Interestingly, by school age, unaffected siblings reach focuses on genetic heterogeneity, where at least some cases
typical levels of functioning with very few residual delays appear to result from de novo mutations in the form of rare
or deficits [38]. In summary, according to this view varia- copy number variants, leading to genomic imbalance and
bility in the expression of behavioural risk within the first change in gene expression [42]. In such cases, genetic
years might reflect an infant BAP revealed more clearly mutations might be the overriding risk factor giving rise
through measurement of underlying brain and cognitive to ASD (Figure 3a).
functions. However, it is important to emphasise that such
A third account of the diverging results between mutations, along with all of the other genetic factors dis-
measures of overt social behaviour and those of underlying covered so far, account for no more than 20% of ASD cases,
brain and cognitive functions is more speculative in view of with no individual factor explaining more than 1 to 2%.
limited data on infant siblings. It is possible that in most Therefore, a ‘gene-dosage’ model is increasingly popular, in
infants, expression of risk is measurable in the form of which susceptibility to ASD might be determined by cumu-
subtle aspects of brain and cognitive function. It is only in a lative genetic and non-genetic effects reaching a threshold
subset of these infants that initially subtle differences [42–45]. According to the gene-dosage model, infant sib-
become compounded, leading into a developmental trajec- lings’ outcome is determined by the nature, proportion, or
tory that results in an ASD outcome. In the majority of combination of genetic and non-genetic ‘hits’ (Figure 3b).
infants, however, well-described processes of brain adap- In addition to considering genetic factors, some models
tation and plasticity (discussed next) may restore the also emphasise the role of the early environment in deter-
developmental trajectory to a typical course. mining outcomes. For example, in some cases typical allelic
variation determines children’s response to different early
Babies at-risk for ASD and gene–environment social or physical environments resulting in the emergence
interaction of developmental disorders [39]. In this context, environ-
Researchers in areas of genetics and developmental psycho- mental risk is viewed as additive to the ‘gene dose’, and
pathology have invoked gene by environment interaction thus influences the infant’s overall susceptibility to
to help explain why an early genetic or environmental adverse outcome (Figure 3b). Thus, specific combinations
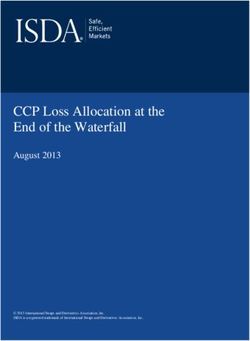
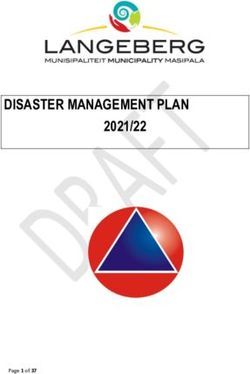
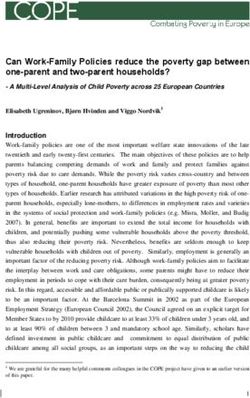
Figure 3. Different models for how single or multiple genetic and/or environmental risk factors in infancy lead to ASD behavioural outcomes in childhood. In model c, risk
factors predict outcomes through dynamic changes over the course of development. Alternatively, the developmental process might buffer initial vulnerability, canalising
the impact of risk.
84Review Trends in Cognitive Sciences Vol.14 No.2
of genetic and environmental risk factors can determine
the nature of the resulting phenotype, that is ASD or
another developmental condition, as well as variability
in expression ranging from severe diagnosable outcomes
to milder normative characteristics. Consistent with this
model, findings from infant siblings research indicate
variability in the early expression of risk, but much work
will be required in future studies to specify which combi-
nations lead to which outcomes (also Box 3).
Although relatively simple Gene by Environment
models might help explain the onset of some developmen-
tal disorders [39], in other cases the effects of their inter-
action seem to be more complex. For example, evidence
from research on language, and literacy impairment
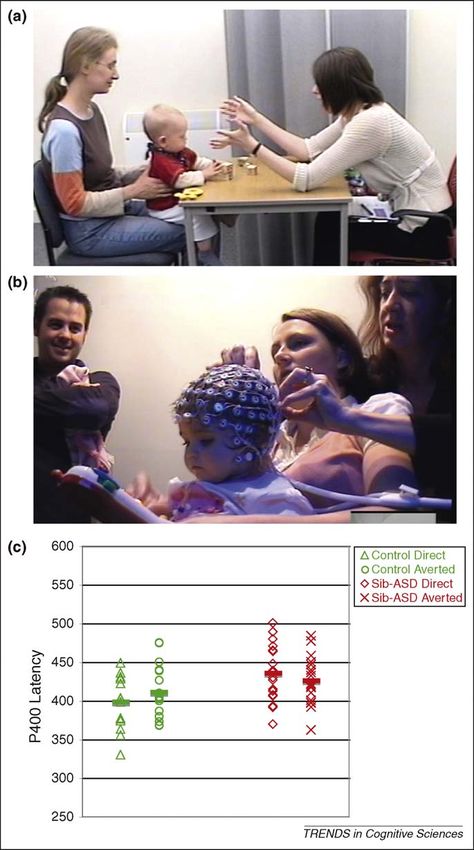
[46,47], as well as conditions such as Williams Syndrome, Figure 4. Hypothetical trajectories for expression of risk in infant siblings at both
where the genetic underpinnings are clearly understood neural and behavioural levels. The ASD trajectory is characterised by a high-dose
of mediating risk factors, the impact of which becomes compounded and amplified
[48], supports probabilistic and indirect mapping between over time. The BAP characterises infants with a low-dose of risk factors leading to
genetic and/or environmental factors and developmental sub-clinical expression of the condition. Canalisation involves similar initial
outcomes [49] (Figure 3c). In these cases the favoured view expression of risk but eventual restoration of the typical developmental trajectory.
is that dynamic gene by environment interactions during
the period of maximal brain plasticity lead to variable Examples of hypothetical developmental trajectories in
developmental trajectories, not readily predicted by a infant siblings based on the latter account are illustrated in
simple model of additive risk. Figure 4. In the ‘affected’ group, early and widespread,
Computational models (neural networks) designed to albeit subtle differences, in multiple brain systems might
illuminate non-linear interactions between genetic and become compounded over time as a result of atypical
environmental factors [50] have reaffirmed older ideas in interactions between brain systems and the external
the literature about the different effects of early pertur- environment. A second group show less initial sub-clinical
bations on developmental trajectories [51]. In some cases, an characteristics and continue within the BAP profile over
early perturbation can reset a developmental trajectory time. A third possibility is that although early manifes-
along a different route, as a result of the compounding of tations of risk can be observed in infant siblings as a group,
atypical brain computations or behaviour eliciting or canalisation restores the trajectory of development back to
recruiting an atypical environment. In other cases, the its typical path. Such dynamic pathways within the early
typical developmental trajectory can be resilient in the face developmental period might arise as a consequence of
of genetic or early environmental ‘hits’ through canalisation, compensatory plasticity in the developing brain. However,
a process through which brain adaptation and plasticity it has been recently proposed that even some older chil-
maintains or restores the typical trajectory. Such trajectory dren, who already exhibit a clear profile of autistic symp-
differences, emerging from the dynamic interaction of toms, may reach optimal outcomes [52]. The precise factors
multiple factors over time, are not easily decomposable into involved in this adaptation in infancy or in childhood have
separate genetic and environmental contributions. yet to be verified.
Box 3. Taking individual differences seriously: infant intermediate phenotypes?
There is currently growing interest in using laboratory methods as tion here is that diagnosed forms of ASD, which are themselves
biomarkers of risk for a diagnosis of ASD later in life. Biomarkers are highly variable, are extremes of what is otherwise typical variation.
defined as measurable factors specifically associated with a particular Even in clinical circles, once viewed as essential for screening
condition, which can be used to ascertain an individual’s suscept- specificity, access to services, treatment design, and reducing
ibility for that condition [63]. Although developing such biomarkers is heterogeneity of participants in research, categorical approaches are
a long-term aim of research on infant siblings, findings have already gradually being complemented by dimensional ones in ASD [66] and
highlighted that individual differences need to be considered in other developmental disorders [46,67]. It is probable that the
seriously as these can reflect different developmental pathways to development of such infant intermediate phenotypes based on
outcome. experimental methods will significantly advance research across
A standard approach in infant siblings research focuses on these various disciplines. A further implication of recent findings from
identifying group differences in early behaviours as defined by infant siblings is that such intermediate phenotypes need not be static
clinical outcomes, for example ASD vs. unaffected. These category over development. In other words, understanding the impact of
groups are defined through cut-off scores across a number of dynamic gene by environment interactions in how these character-
instruments such as the ADOS and the ADI and in combination with istics change over time will be essential.
expert clinical judgment. One disadvantage of this approach is that Infant siblings research has introduced new challenges for infancy
potentially meaningful variability in the data might be lost. Increas- science, which traditionally tests group performance on single
ingly, researchers in areas of genetics have advocated the use of measures. Group studies on infant siblings have demonstrated
dimensional intermediate or endo-phenotypes, viewed as closer to success in improving our understanding of the early ASD phenotype
the genotype than complex clinical characterisation [64,65]. Specifi- and have allowed comparisons with existing research. However,
cally, measures of quantitative traits associated with ASD and future success rests on our ability to complement group data with
overlapping with other disorders are viewed as better candidates validation of dimensional and longitudinal measures for assessing
for gene mapping than diagnostic classification [45,46]. The assump- both risk and outcome.
85Review Trends in Cognitive Sciences Vol.14 No.2
Box 4. Outstanding questions References
1 Baird, G. et al. (2006) Prevalence of disorders of the autism spectrum in
Will a combination of risk markers early in infancy be more a population cohort of children in South Thames: the Special Needs and
effective than individual markers of risk in predicting diagnostic autism Project (SNAP). Lancet 15, 210–215
outcomes for ASD or other overlapping conditions? 2 Knapp, M. et al. (2007) Economic consequences of autism in the UK,
Are brain measures more sensitive than behavioural methods in Foundation for People with Learning Disabilities, (UK)
identifying and quantifying risk and outcomes? 3 Palomo, R. et al. (2006) Autism and family home movies: a
Will laboratory methods provide viable future biomarkers of risk? comprehensive review. J. Dev. Behav. Pediatr. 27, S59–68
Will infant siblings research provide more objective methods for 4 Elsabbagh, M. and Johnson, M.H. (2007) Infancy and autism: Progress,
diagnosing ASD than the current behavioural criteria? prospects, and challenge. Prog. Brain Res. 164, 355–383
Can we develop early intervention or prevention techniques that 5 Bolton, P. et al. (1994) A case-control family history study of autism.
target those infants who are likely to go on to serious symptoms? J. Child Psychol. Psychiatry 35, 877–900
Can putative canalisation in some infant siblings provide a model 6 Dawson, G. et al. (2002) Defining the broader phenotype of autism:
for intervention in those who are subsequently affected? genetic, brain, and behavioral perspectives. Dev. Psychopathol. 14,
581–611
7 Pickles, A. et al. (2000) Variable expression of the autism broader
phenotype: findings from extended pedigrees. J. Child Psychol.
Different models for gene by environment interactions Psychiatry 41, 491–502
provide exciting opportunities for future research on infant 8 Dalton, K.M. et al. (2007) Gaze-fixation, brain activation, and amygdala
siblings (Box 4). Genotyping of participating families has volume in unaffected siblings of individuals with autism. Biol.
Psychiatry 61, 512–1512
already begun in some projects. By contrast, there is
9 Baron-Cohen, S. and Hammer, J. (1997) Parents of children with
currently less focus on environmental factors. In this Asperger Syndrome: what is the cognitive phenotype? J. Cogn.
regard, most researchers are rightly cautious in view of Neurosci. 9, 548–554
the recent past, where an influential theory attributed the 10 Belmonte, M. et al. (2009) Visual attention in autism families:
cause of ASD to parenting style [53]. This idea has been ‘unaffected’ sibs share atypical frontal activation. J. Child Psychol.
Psychiatry DOI: 10.1111/j.1469-7610.2009.02153.x
dismissed by converging evidence including some of the
11 Hughes, C. et al. (1999) Towards a cognitive phenotype for autism:
findings reviewed here. However, models that incorporate increased prevalence of executive dysfunction and superior spatial
environmental influence raise the possibility that modu- span amongst siblings of children with autism. J. Child Psychol.
lating the early social environment might help infants Psychiatry 40, 705–718
overcome the adverse impact of genetic vulnerability. It 12 Happé, F. et al. (2001) Exploring the cognitive phenotype of autism:
weak ‘‘central coherence’’ in parents and siblings of children with
is against this background that some scientists are begin- autism: I Experimental tests. J. Child Psychol. Psychiatry 42, 299–307
ning to pilot behavioural interventions based on modifying 13 Johnson, M.H. et al. (2005) The emergence of the social brain network:
the early social environment for the prodromal period of evidence from typical and atypical development. Dev. Psychopathol. 17,
the condition, modelled after those designed for very young 599–619
affected children. The success or otherwise of such inter- 14 Zwaigenbaum, L. et al. (2005) Behavioral manifestations of autism in
the first year of life. Int. J. Dev. Neurosci. 23, 143–152
ventions will help determine the extent to which early 15 Bryson, S.E. et al. (2007) A prospective case series of high-risk infants
environmental factors can influence outcome in infants who developed autism. J. Autism Dev. Disord. 37, 12–24
at-risk [54,55]. 16 Landa, R. and Garrett-Mayer, E. (2006) Development in infants with
autism spectrum disorders: a prospective study. J. Child Psychol.
Psychiatry 47, 629–638
Concluding remarks
17 Yoder, P. et al. (2009) Predicting social impairment and ASD diagnosis
Attempting to understand the ways in which genes, brains in younger siblings of children with autism spectrum disorder. J.
and the environment operate and interact is an enormous Autism Dev. Disord. DOI: 10.1007/s10803-009-0753-0
challenge. Owing to the fruitful integration of theories from 18 Sullivan, M. et al. (2007) Response to Joint Attention in Toddlers at
different disciplines, innovative methodologies, and a suc- Risk for autism spectrum disorder: A Prospective Study. J. Autism Dev.
Disord. 37, 37–48
cessful alliance of scientists, babies and their families, we
19 Nadig, A.S. et al. (2007) A prospective study of response to name in
are at the cusp of very exciting discoveries. Studies of infant infants at risk for autism. Arch. Pediatr. Adolesc Med. 161, 378–383
siblings of children affected by ASD are beginning to reveal 20 Mitchell, S. et al. (2006) Early language and communication
how genetic risk for developing the condition takes them development of infants later diagnosed with autism spectrum
through diverging routes in their development. In addition disorder. J. Dev. Behav. Pediatr. 27, S69–78
21 Loh, A. et al. (2007) Stereotyped motor behaviors associated with
to advancing basic and clinical science, research with infant autism in high-risk infants: a pilot videotape analysis of a sibling
siblings provides promising opportunities for exploring sample. J. Autism Dev. Disord. 37, 25–36
whether early interventions are successful in reducing 22 Ozonoff, S. et al. (2008) Atypical object exploration at 12 months of age
the impact of the adverse symptoms in at least some cases. is associated with autism in a prospective sample. Autism 12, 457–
472
23 Garon, N. et al. (2009) Temperament and its relationship to autistic
Acknowledgements
symptoms in a high-risk infant sib cohort. J. Abnorm. Child Psychol.
We wish to sincerely thank all the families taking part in the British
37, 59–78
Autism Study of Infant Siblings (BASIS, www.basisnetwork.org). We
24 Lord, C. et al. (2004) Regression and word loss in autistic spectrum
wish to specifically thank those families and researchers who have given
disorders. J. Child Psychol. Psychiatry 45, 936–955
consent to the use of their photographs. BASIS is approved by the London
25 Landa, R.J. et al. (2007) Social and communication development in
Multicentre Research Ethics Committee, UK. Although the specific views
toddlers with early and later diagnosis of autism spectrum disorders.
expressed are our own, we are grateful to our collaborators Patrick
Arch. Gen. Psychiatry 64, 853–864
Bolton, Tony Charman, Andrew Pickles, Atsushi Senju, Teodora Gliga,
26 Ozonoff, S. et al. (2008) The onset of autism: Patterns of symptom
Janice Fernandes and Kim Davies for helpful discussion. This research is
emergence in the first years of life. Autism Res. 1, 320–328
supported by the UK Medical Research Council (G0701484) and Autism
27 Landa, R.J. (2008) Diagnosis of autism spectrum disorders in the first 3
Speaks, UK. ME is supported by a Leverhulme Trust Early Career
years of life. Nat. Clin. Prac. Neurol. 4, 138–147
Fellowship.
86Review Trends in Cognitive Sciences Vol.14 No.2
28 Elsabbagh, M. et al. (2009) Visual orienting in the early broader autism 48 Karmiloff-Smith, A. (2009) Nativism versus neuroconstructivism:
phenotype: disengagement and facilitation. J. Child Psychol. rethinking the study of developmental disorders. Dev. Psychol. 45, 56–63
Psychiatry 50, 637–642 49 Karmiloff-Smith, A. (1998) Development itself is the key to
29 Landry, R. and Bryson, S.E. (2004) Impaired disengagement of understanding developmental disorders. Trends Cogn. Sci. 2, 389–398
attention in young children with autism. J. Child Psychol. 50 Elman, J. et al. (1996) Rethinking Innateness: A Connectionist
Psychiatry 45, 1115–1122 Perspective on Development, MIT Press
30 McCleery, J.P. et al. (2007) Abnormal magnocellular pathway visual 51 Waddington, C.H. (1966) Principles of development and differentiation,
processing in infants at risk for autism. Biol. Psychiatry 62, 1007–1014 Macmillan Company
31 McCleery, J.P. et al. (2009) Atypical faces vs. object processing and 52 Helt, M. et al. (2008) Can children with autism recover? If so, how?.
hemispheric asymmetries in 10-month-old infants at risk for autism. Neuropsychol. Rev. 18, 339–366
Biol. Psychiatry 66, 950–957 53 Bettelheim, B. (1967) The Empty Fortress: Infantile Autism and the
32 Elsabbagh, M. et al. (2009) Neural correlates of eye gaze processing in Birth of the Self, Free Press
the infant broader autism phenotype. Biol. Psychiatry 65, 31–38 54 Dawson, G. (2008) Early behavioral intervention, brain plasticity, and
33 Cassel, T.D. et al. (2007) Early Social and emotional communication in the prevention of autism spectrum disorder, Dev. Psychopathol 20,
the infant siblings of children with autism spectrum disorders: An 775–803
examination of the broad phenotype. J. Autism Dev. Disord. 37, 122– 55 Green, J. and Dunn, G. (2008) Using intervention trials in
132 developmental psychiatry to illuminate basic science. Br. J.
34 Yirmiya, N. et al. (2006) The development of siblings of children with Psychiatry 192, 323–325
autism at 4 and 14 months: social engagement, communication, and 56 Zwaigenbaum, L. et al. (2009) Clinical assessment and management of
cognition. J. Child Psychol. Psychiatry 47, 511–523 toddlers with suspected autism spectrum disorder: insights from
35 Presmanes, A.G. et al. (2007) Effects of different attentional cues on studies of high-risk infants. Pediatrics 123, 1383–13891
responding to joint attention in younger siblings of children with 57 Charman, T. et al. (1997) Infants with autism: an investigation of
autism spectrum disorders. J. Autism Dev. Disord. 37, 133–144 empathy, pretend play, joint attention, and imitation. Dev. Psychol. 33,
36 Toth, K. et al. (2007) Early social, imitation, play, and language 781–789
abilities of young non-autistic siblings of children with autism. J. 58 Swettenham, J. et al. (1998) The frequency and distribution of
Autism Dev. Disord. 37, 145–157 spontaneous attention shifts between social and non-social stimuli
37 Bryson, S.E. et al. (2008) The Autism Observation Scale for Infants: in autistic, typically developing and non-autistic developmentally
scale development and reliability data. J. Autism Dev. Disord. 38, delayed infants. J. Child Psychol. Psychiatry 39, 747–753
731–738 59 Brian, J. et al. (2008) Clinical assessment of autism in high-risk 18-
38 Gamliel, I. et al. (2007) The development of young siblings of children month-olds. Autism 12, 433–456
with autism from 4 to 54 months. J. Autism Dev. Disord. 37, 171–183 60 Hazlett, H.C. et al. (2007) Magnetic resonance imaging and head
39 Stevens, S.E. et al. (2009) Dopamine transporter gene polymorphism circumference study of brain size in autism: birth through age 2
moderates the effects of severe deprivation on ADHD symptoms: years. Arch. Gen. Psychiatry 62, 1366–1376
Developmental continuities in gene-environment interplay. Am. J. 61 Murias, M. et al. (2007) Resting state cortical connectivity reflected in
Med. Genet. Part B Neuropsychiatr. Genet. 150B, 753–761 EEG coherence in individuals with autism. Biol. Psychiatry 62, 270–
40 Bailey, A. et al. (1995) Autism as a strongly genetic disorder: evidence 273
from a British twin study. Psychol. Med. 25, 63–77 62 Lewis, J.D. and Elman, J.L. (2008) Growth-related neural
41 Autism Genome Project (2007) Mapping autism risk loci using genetic reorganization and the autism phenotype: a test of the hypothesis
linkage and chromosomal rearrangements. Nat. Genet. 39, 319–328 that altered brain growth leads to altered connectivity. Dev. Sci. 11,
42 Cook, E. and Scherer, S.W. (2008) Copy-number variations associated 135–155
with neuropsychiatric conditions. Nature 455, 919–923 63 Lanphear, B. and Bearer, C. (2005) Biomarkers in paediatric research
43 Constantino, J.N. and Todd, R.D. (2005) Intergenerational and practice. Arch. Dis. Child 90, 594–600
transmission of subthreshold autistic traits in the general 64 Skuse, D. (2001) Endophenotypes and child psychiatry. Br. J.
population. Biol. Psychiatry 57, 655–660 Psychiatry 178, 395–396
44 Zhao, X. et al. (2007) A unified genetic theory for sporadic and inherited 65 Losh, M. and Piven, J. (2007) Social-cognition and the broad autism
autism. Proc. Natl. Acad. Sci. U S A 104, 12831–12836 phenotype: identifying genetically meaningful phenotypes. Child
45 Abrahams, B.S. and Geschwind, D.H. (2008) Advances in autism Psychol. Psychiatry 48, 105–112
genetics: on the threshold of a new neurobiology. Nat. Rev. Genet. 9, 66 Gotham, K. et al. (2009) Standardizing ADOS scores for a measure of
341–355 severity in autism spectrum disorders. J. Autism Dev. Disord. 39,
46 Newbury, D.F. et al. (2005) Genetic influences on language impairment 693–705
and phonological short-term memory. Trends Cogn. Sci. 9, 528–534 67 Bishop, D.V. and Snowling, M.J. (2004) Developmental dyslexia and
47 Snowling, M.J. et al. (2007) Children at family risk of dyslexia: a follow- specific language impairment: same or different? Psychol. Bull. 130,
up in early adolescence. J. Child Psychol. Psychiatry 48, 609–618 858–886
87You can also read