Getting Hives Just Thinking About It! - Approach to the work up and management of urticaria - Massachusetts General ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Getting Hives Just Thinking
About It!
Approach to the work up and
management of urticaria
Sarina B. Elmariah, MD, PhD
Director, MGH Itch and
Neurocutaneous Disorders Clinic
Massachusetts General Hospital
Harvard Medical School
www.mghcme.org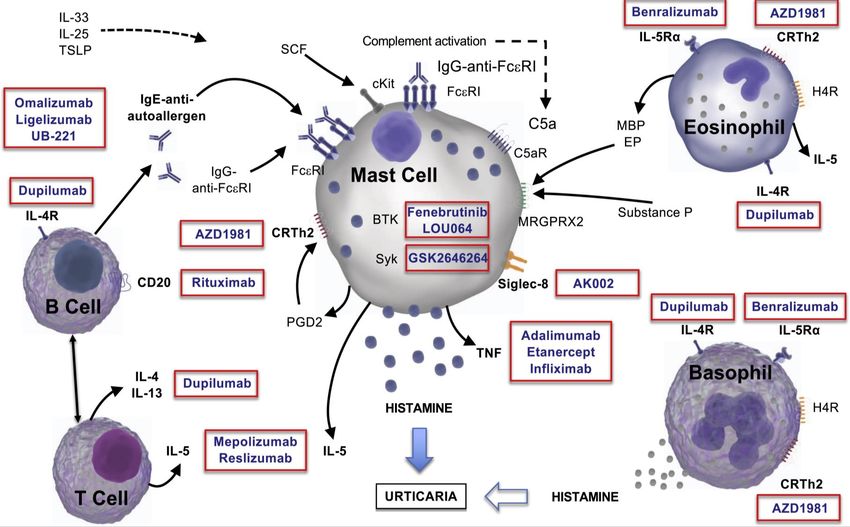
Disclosures
I have the following relevant financial relationship
with a commercial interest to disclose:
• Sanofi/Regeneron
• RAPT Therapeutics
• Menlo Therapeutics
• Trevi Therapeutics
www.mghcme.org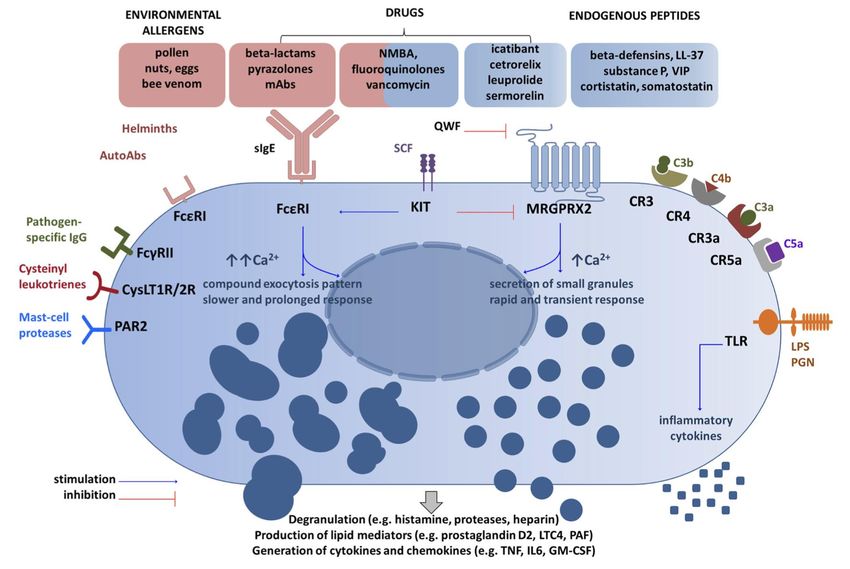
PART I: OVERVIEW OF URTICARIA
www.mghcme.org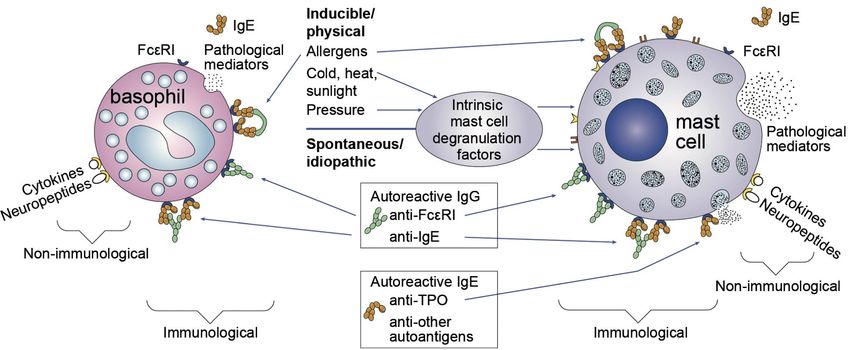
What are urticaria?
• Aka hives or wheals
• Evanescent, pruritic, pink
edematous papules or plaques that
typically have a peripheral flare of
pallor
• Lesions last < 24 hrs
• If >24 hours, consider other urticarial
dermatoses or vasculitis
• Round, annular or serpiginous
• Affect any part of the body
• Can be associated with angioedema
(deep swellings)
Images from Bolognia, J, Schaffer JV, and Cerroni L. Dermatology 4th Ed. 2018
www.mghcme.org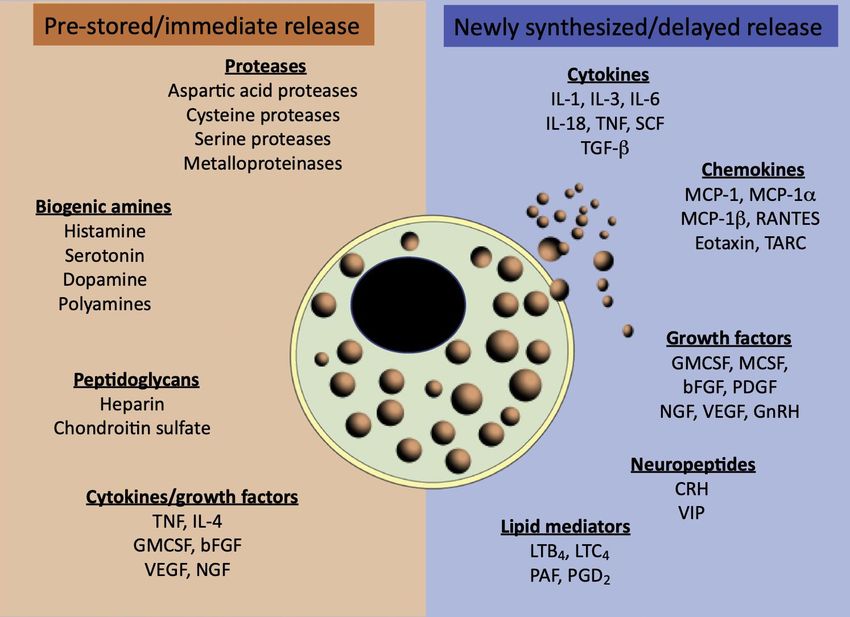
Clinical Subtypes
Spontaneous Inducible
• Mechanical urticaria
• Acute: < 6 weeks
– Dermatographism
• Chronic: > 6 weeks, – Delayed pressure
most days • Contact urticaria
– Autoimmune urticaria – Chemical contact
– Cold contact
• Episodic: recurrent but – Heat contact
Epidemiology
• Acute urticaria affects up to ~20-25% population overall
• Chronic urticaria has a lifetime prevalence of 1.8%, and will
affect up to 1% of the population at any given time.
– 40% CU associated with angioedema
– ~20% are inducible or physical urticarias
– ~80% spontaneous or idiopathic urticaria (prevalence 1% in US,
similar in other countries)
• 30-60% of these are considered autoimmune
• 2:1 predominance in women
• Affects all ages, peaks between 3rd to 5th decades
www.mghcme.org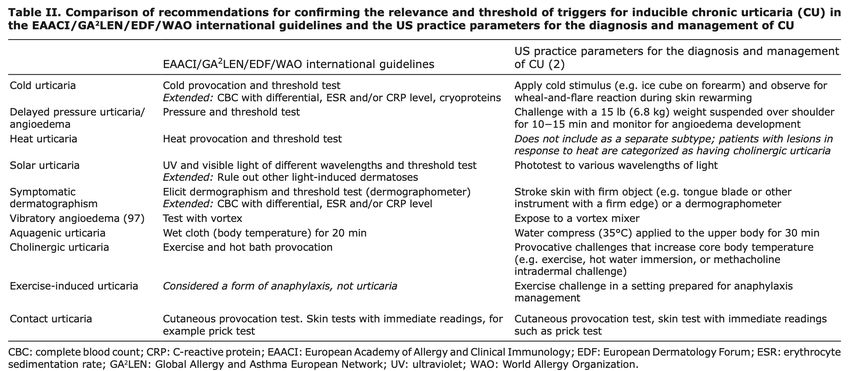
PART II: PATHOPHYSIOLOGY AND
DIAGNOSTIC WORK UP OF URTICARIA
www.mghcme.org
Pathophysiology
Beck LA, et al., Acta Derm Venereol. 2017 Feb 8;97(2):149-158.
www.mghcme.org
Porebski G, et al. Front Immunol. 2018 Dec 20;9:3027
www.mghcme.org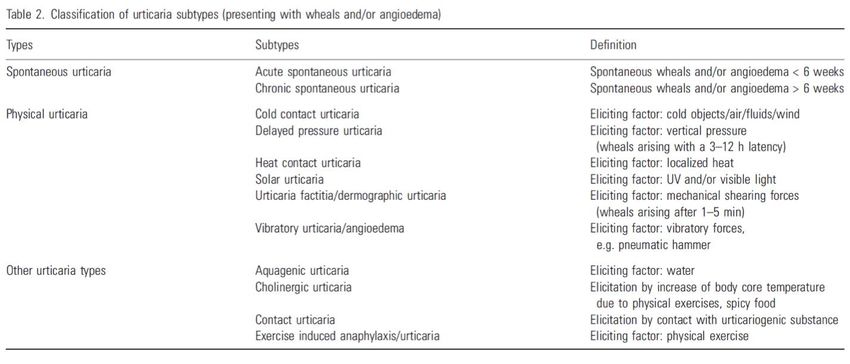
Autoimmune urticaria
• Functional IgG
autoantibodies cause
degranulation of mast cells
• Majority of autoantibodies
bind extracellular subunit
of FcƐRI
• 10% of chronic urticarial
pts have IgG against Fc
portion of IgE
Bolognia, Jean, Julie V. Schaffer, and Lorenzo Cerroni. Dermatology 4th Ed. 2018.
www.mghcme.orgImmediate symptoms of itch, Influx of inflammatory cells, pro-
burning, edema and erythema inflammatory cytokine release and
due to vasodilation and neural increased vasodilation
activation Forsythe P., Trends Neurosci. 2019 Jan;42(1):43-55.
www.mghcme.orgClinical Subtypes
Zuberbier T et al., Allergy 2009: 64: 1417-1426.
www.mghcme.orgAutoimmune urticaria
• Common
• Estimated to account for ~30-50% cases of
chronic spontaneous urticaria
• Round, annular, or serpiginous edematous
papules and plaques develop spontaneous,
resolve within 24 hours
• Extracutaneous symptoms include Image from AsthmaAllergyNetwork.org
headaches, fatigue, joint pain, wheezing,
n/v, diarrhea, other GI sx
• Often associated with co-morbid
autoimmune thyroid disease, SLE, RA,
Sjogren’s, etc, celiac and emerging data
suggesting increases odds of atopic
diseases, vitiligo, Henoch Schonlein pupura,
IBD
www.mghcme.org
Kolkhir P, et al. Autoimmun Rev. 2017 Dec;16(12):1196-1208Autoimmune urticaria
• Diagnostic test: screen for 2 basic mechanisms
• Type I (IgE-autoantibodies to autoantigens, e.g.,
thyroperoxidase (TPO))
• Type II (IgG-autoantibodies to IgE or FcεRI) identified
on autologous serum skin test (ASST) or
immunoassays
• The autoantibodies anti-IgE and IgG anti-FceRI were
found in sera from ~45–55% of patients with CU.
Table from Confino-Cohen R et al, JACI. 2012 May;129(5):1307-13
www.mghcme.orgPressure urticaria
Dermatographism Delayed Pressure Urticaria
• Deep, pruritic and painful swellings after
• Affects ~5% of people sustained pressure
• Develops within 30 min to 12 hours
• Develops within seconds to minutes
after skin stroke after onset of pressure, can last days
• Commonly affects shoulders (F), waist,
• Diagnostic test: scratch skin with soles, genitalia
broken tongue depressor ▪ Diagnostic test: apply 2.5kg weight to
Images from Bolognia J. Dermatology 4th Ed. 2018
thigh/back for 20min, monitor for 8 hrs
www.mghcme.orgContact urticaria
• Common, often arises due
to occupational exposure
• Environmental (plants,
animals), food, cosmetics,
preservatives
• Wheals develop within ~30
min following external
exposure with triggering
substance, typically resolve
within few hours
• Extracutaneous symptoms
include wheezing, rhinitis,
lip or throat swelling, n/v/d,
anaphylaxis
From DermNetNZ.org
www.mghcme.orgContact urticaria
• Diagnostic test:
• Open and scratch tests: substance is applied,
gently rubbed or occluded for 15 min on skin
• Prick testing: intradermal injection of substance
• RAST testing: serum IgE
• At risk occupations
• Agricultural, dairy workers: cow dander, grains and
feeds
• Food workers: cheese, egg, milk, shellfish, fruit, flour
and wheat
• Bakers: ammonia persulfate, flour, a-amylase
• Dental workers: latex, acrylate, epoxy, toothpaste
• Medical/veterinary: latex
• Electronic workers: acrylate, latex
• Hairdressers: ammonia persulfate, latex
Images from Giménez-Arnau A.. Rev Environ Health. 2014;29(3):207-15.; DermNetNZ.org www.mghcme.orgCold contact urticaria
• Primary: 95% of cold urticarias
– Affects 0.05% general population, typically young to middle-aged adults
– Usually idiopathic, but may be associated with viral infections or following URIs
– Develop 2–5 minutes after exposure and last for 1–2 hours
– ~ 25-30% patients report resolution after 5-10 years
– Associated with flushing, HA, syncope, abdominal pain, hypotension, anaphylaxis
• Secondary cold contact urticaria
– Lasts >24 hours
– Associated with cryoglobulinemia,
Cryofibrinogenemia, cold agglutinins,hemolysins
– Check Hep B/C, EBV, evaluate for
Lymphoproliferative disorders
• Familial cold urticaria: rare
– Burning itching plaques last up to 48 hours
– Mutation in NLRP3, cryopyrin gene (same as Muckle-Wells syndrome)
– Associated with fever, HA, leukocytosis
Images from Bolognia, J, Schaffer JV, and Cerroni L. Dermatology 4th Ed. 2018
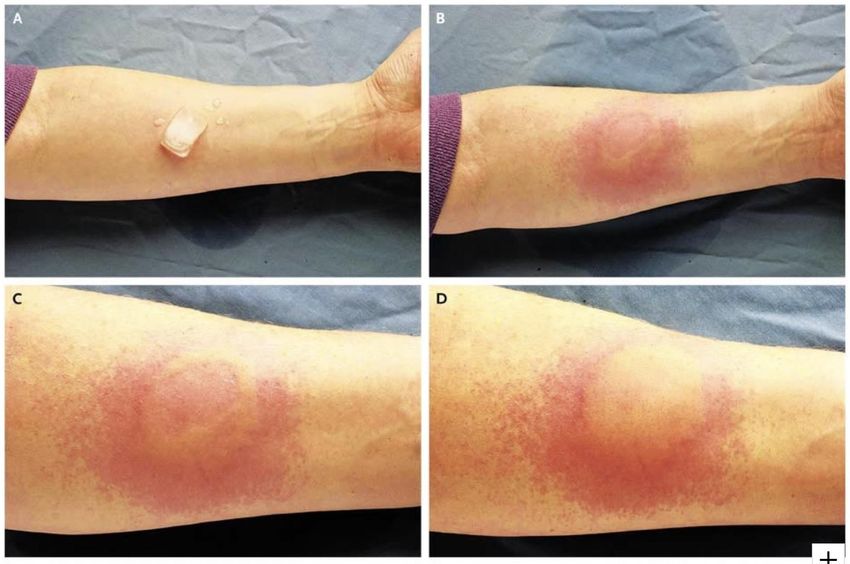
www.mghcme.orgCold contact urticaria
• Diagnostic test: apply an ice cube against the skin of the forearm for 1-5
minutes, monitor for development of hive within 10 minutes
Images from Huissoon A, Krishna MT. N Engl J Med. 2008 Feb 21;358(8):e9
www.mghcme.org‘Neurovascular’ subtypes
Cholinergic urticaria Adrenergic Urticaria
▪ Common (est up to 20%) in young adults, • Very rare
unusual in elderly
• Multiple 1-3mm red or pink papules with
▪ Numerous pinpoint to 3mm edematous papules blanched or pale, vasoconstricted halo
with pronounced flare, stinging and pain > itch
• Triggers include trauma, emotional upset,
▪ Arise within 15 min of rise in core body temp coffee, chocolate, and ginger.
▪ May have systemic symptoms (faint, wheezing),
but also associated with cold urticaria, • May have associated with wheezing,
dermatographism, and aquagenic urticaria palpitations, parasthesias and malaise
▪ Diagnostic test: exercise to induce sweating or • Diagnostic test: id injection of 5-15 ng of Epi
partial immersion in hot bath 42C for 10 min or 3-10 ng of NE in 0.02 mL of saline
Images from Fukunaga A et al., Clin Auton Res. 2018 Feb;28(1):103-113., Bolognia et al. Dermatology 4th Ed. 2018
www.mghcme.orgAquagenic urticaria
▪ Very rare, < 100 cases reported
▪ Predominantly affects women, onset in
puberty
▪ 1-3 mm folliculocentric wheals with
surrounding 1-3 cm erythematous flares
▪ Develop 20-30 mins following contact
with water, sweat or tears, and typically
resolve after 60 mins
▪ Associated with pruritus, burning and
prickling or stinging.
▪ Rarely associated with wheezing or SOB
▪ Associations reported with cystic
fibrosis, HIV, and occult thyroid papillary
carcinoma Images from Robles-Tenorio A, et al., Clin Case Rep. 2020 Sep 24;8(11):2121-2124.
Bolognia et al. Dermatology 4th Ed. 2018
www.mghcme.orgAquagenic urticaria
• Diagnostic test: apply a cloth soaked in room temperature water to the
patient’s skin for 20 minutes monitor for development of hive within 30
minutes
Images from Robles-Tenorio A, et al., Clin Case Rep. 2020 Sep 24;8(11):2121-2124.
www.mghcme.orgSolar urticaria
• Uncommon, represents < 0.5% of all
urticaria cases and 7% of all
photodermatoses
• Predominately affects women, onset in
young adults (median age 35 years)
• Erythema, edematous papules occurs
within minutes of sunlight, lasts < 60 mins
• May occur on sun-exposed areas or those
covered with thin, white clothing
• May be associated with nausea, headache,
syncope, wheezing or dyspnea
• Diagnostic test: Photo provocation testing
to UVA, UVB and visible light. Need to
assess every 10 minutes for an hour.
Images from Bolognia, J, Schaffer JV, and Cerroni L. Dermatology 4th Ed. 2018
www.mghcme.orgDiagnostic evaluation
• History
• Examination
– Helpful in some cases of inducible urticaria
• Diagnostic testing
– Allergy provocation testing
– Autoimmune profiles
– Infectious disease evaluation
www.mghcme.orgKey elements of history
Zuberbier T et al., Allergy. 2018;73:1393–1414.
www.mghcme.orgKey elements of examination
• In general, exact etiology cannot be
determined by physical examination.
• However, occasional features may help
distinguish subtypes:
• Generalized vs localized
• Large plaques vs small papules
• Erythematous flare vs pale vasoconstriction
Zuberbier T et al., Allergy. 2018;73:1393–1414.
www.mghcme.orgASST = autologous
serum skin test
(wheal/flare
develops at site of
patient’s own
intradermally
injected serum)
largely replaced by
immunoassays for
the auto-antibodies
Radonjic-Hoesli S et al. Clin Rev Allergy Immunol. 2018 Feb;54(1):88-101.
www.mghcme.orgEvaluating patients with chronic urticaria
• Routine: CBC w/ diff, ESR, CRP, TSH
• As indicated by HPI, PE or ROS: ANA,
RF, cryoglobulins, anti-TPO antibodies,
anti-IgE and anti-FcεRI antibodies,
Hep B/C serologies, stool O + P
• Skin biopsies are usually NOT helpful
unless vasculitis is expected (e.g.
‘painful’ urticaria which last >24-72
hours)
Bolognia, J, Schaffer JV, and Cerroni L. Dermatology 4th Ed. 2018
www.mghcme.orgInducible vs Autoimmune
Saini SS, Kaplan AP. J Allergy Clin Immunol Pract. 2018 Jul-Aug;6(4):1097-1106.
www.mghcme.orgDiagnostic evaluation of CU:
Practice Guidelines
Beck LA et al. Acta Derm Venereol. 2017 Feb 8;97(2):149-158.
www.mghcme.orgTests to confirm inducible CU:
Practice Guidelines
Beck LA et al. Acta Derm Venereol. 2017 Feb 8;97(2):149-158.
www.mghcme.orgPART III: MANAGEMENT OF
URTICARIA
www.mghcme.orgUS Guidelines on CU Treatment
Beck LA et al. Acta Derm Venereol. 2017 Feb 8;97(2):149-158.
www.mghcme.orgAntihistamines
Bolognia, J, Schaffer JV, and Cerroni L. Dermatology 4th Ed. 2018
www.mghcme.orgAntihistamines
• 40-50% of CU patients at tertiary clinics will clear/almost clear at licensed
doses of anti-histamines
• For refractory cases:
• Increase to 4-6x l recommended dose
• Combine antihistamines (non-sedating /long-acting with sedating at night)
• If adding H2 antihistamines, ranitidine is preferable. Cimetidine interferes with
hepatic drug metabolism and binds androgen receptors.
• Special considerations
• For cold urticaria, try cyproheptadine (anti-cholinergic)
• For adrenergic urticaria, add propranolol to antihistamine regimen
• In pregnancy, loratadine and cetirizine thought to be safest
• Avoid chlorpheniramine close to delivery and during breastfeeding
• In patients > 65 yo, avoid chlorpheniramine, hydroxyzine and diphenhydramine
due to more potent anti-cholinergic and neuropsychiatric effects. The AGS Beers
Criteria panel advises 2nd generation H1-antihistamines (cetirizine or loratadine).
www.mghcme.orgLeukotriene receptor antagonists
• Rationale: Cysteinyl leukotriene injection causes a wheal and
flare response
• Efficacy: Few small RCTs demonstrating mixed results for efficacy
• 3 showed benefit over placebo (Erbagzi 2002, Pacor 2001,
Bagenstose 2004)
• No benefit compared with placebo (Reimers 2002)
• Less benefit than 2nd gen. antihistamines (Di Lorenzo 2004)
• SEs: headache, GI infections, sedation in trials, real world data
suggesting possible neuropsychiatric SEs
• Tips: Might be worth a 2-4 weeks trial, but if unhelpful would
discontinue.
www.mghcme.orgAnti-inflammatory agents
Hydroxychloroquine Dapsone
• Rationale: Disrupts T-cell receptor • Rationale: Sulfone antimicrobial with
cross-linking dependent calcium antineutrophilic effects
signaling and Ag processing
• Efficacy: 2 RCTs showing benefit
• Efficacy: 1 RCT showing benefit (Engin, 2008, Morgan, 2015)
(Reeves 2004)
• SEs: dose-related hemolysis,
• SEs: GI upset; retinopathy after 5 yrs methemoglobinemia, peripheral
neuropathy, GI distress,
• Tips: hepatotoxicity, agranulocytosis,
DRESS
– Consider when co-morbid
autoimmune disease
– Takes at least 3-6 months to • Tips:
work – Use this occasionally
– Need baseline and annual – Requires G6PD screening at
ophtho exam baseline and Hgb and LFT
monitoring
www.mghcme.orgAnti-inflammatory agents
Methotrexate Colchicine
• Rationale: MOA unclear but may include • Rationale: antineutrophilic effects
increased adenosine levels, apoptosis in
activated CD4 T cells, and decreased • Efficacy: Case series and negative RCT
neutrophil chemotaxis (Pho 2011; Lawlor 1989)
• Efficacy: anecdotal success in my
patients; case series and negative RCTs
(Perez 2009; Sharma 2014; Leducq 2020) • SEs: dose-related GI distress and diarrhea
• SEs: potential for GI sx, stomatitis, h/a,
fatigue, hematologic abnormalities; • Tips:
rarely, hepatoxicity, pulmonary toxicity, – Rarely helpful in my patients, limited
and myelosuppression evidence
• Tips: – Infrequent lab monitoring
– Consider when co-morbid
autoimmune disease
– Takes at least 1-2 months to work
– Need frequent lab monitoring
www.mghcme.orgCyclosporine
• Rationale: Inhibits calcineurin and suppresses T cell function; inhibits
IgE-induced histamine release from basophils and MCs
• Efficacy: 2 dbRCTs, numerous observational and prospective studies
(Grattan 2000, Vena 2006)
• SEs: Nephrotoxicity, hypertension, infection, (malignancy at higher
doses), hirsutism, h/a, paresthesia, n/v, abdominal pain
• Tips:
– Use for more rapid control, but will transition over to alternative agents
after 6 months
– Requires frequent monitoring of BP and q4-8 week labs including CSA
levels, BUN/Cr, Magnesium
www.mghcme.orgImmunosuppressants
Tacrolimus Mycophenolate
• Rationale: Calcineurin inhibitor, • Rationale: Inhibits inosine-50-
inhibits IgE-mediated MC and monophosphate dehydrogenase,
basophil degranulation depletes activated lymphocytes
• Efficacy: No RCTs, 1 retrospective • Efficacy: Case series and open label
study (Kessel, 2005) study (Zimmerman 2012, Shahar 2006)
• SEs: nephrotoxicity, infection, • SEs: GI distress and diarrhea, infection,
malignancy, h/a, GI upset h/a
• Tips: •Tips:
– Requires frequent BP and –Useful in my patients, but limited
laboratory monitoring (renal evidence
function, hepatic function, –Frequent lab monitoring (q2-3
electrolytes, glucose) months) www.mghcme.orgBiologics
Kolkhir P, et al. Ann Allergy Asthma Immunol. 2020 Jan;124(1):2-12.
www.mghcme.orgOmalizumab
• Rationale: Monoclonal antibody directed against IgE
• Efficacy: Multiple RCTs demonstrating efficacy (Maurer 2013; Saini
2015; Kaplan 2013; Maurer 2018)
• SEs: well-tolerated overall, but h/a, nasopharyngitis, arthralgia, viral
URI, nausea, sinusitis, and cough
• Tips:
– Generally safe and well-tolerated, but expensive
– Requires in-office administration with 25 min monitoring
afterwards, epi-pen
www.mghcme.org• N = 323
• Omalizumab q4weeks at 75 mg, 150
mg, and 300 mg doses (x3) or
placebo
• 16 week observation period
• Both the 150 mg and the 300 mg
groups showed significant
improvement in itch and hive scores
compared with placebo
• Complete resolution 44% at 300 mg
and 22% at 150 mg
• No long-term effect in remission
Maurer M et al., N Engl J Med 2013; 368:924-935
www.mghcme.org• Open label phase: omalizumab q4weeks at 300 mg
(x6)
• N = 205
• Subsequent 24 week double blinded phase with
investigator-assessed clinical worsening →
transitioned to open label omalizumab treatment
and continued through week 48
• N = 134
• CIU relapse: 60% placebo vs 21% omalizumab
• DLQI worsening: 66% placebo vs 20% omalizumab
Maurer M, et al, JACI. 2018 Mar;141(3):1138-1139.e7
www.mghcme.orgAlternatives
• Limited to case reports or small case series
▪ TNF inhibitors (etanercept, infliximab, adalimumab)
▪ B cell targeted therapies (rituximab)
▪ Anti-IL-1 therapies (anakinra)
▪ IVIG (has case reports and small OLS)
▪ Many immunomodulatory activities including modulation of adhesion,
complement function, cytokine levels, and autoantibodies
▪ Limited known efficacy, but generally well-tolerated
▪ In phase III trials
▪ Ligelizumab
▪ Ph IIb trial Ligelizumab with placebo and omalizumab comparators
▪ Complete clearance: 51% ligelizumab 72 mg SC q4 weeks vs 26%
omalizumab 300 mg q4 weeks vs 0% placebo
Maurer M. et al., N Engl J Med. 2019 Oct 3;381(14):1321-1332.
www.mghcme.orgTreatment considerations
• Combination therapy may be required
• Optimal duration of therapy is unknown
• Treat until patient has achieved 3-6 symptom-free months
• Then, attempt to taper with clinical monitoring for CU
recurrence
• Taper anti-inflammatory and immunosuppressive agents
every 3-6 weeks
• Taper omalizumab frequency to q6-8 weeks or as tolerated
www.mghcme.orgAgent Typical Dose Improvement Efficacy Risk Labs Cost
LTRA 10 mg QD 2-4 wk Low Minimal None $$
(B)
HCQ 200 mg BID Up to 12 wk Moderate Low Baseline: LFT, BUN/Cr $
(C)
Dapsone 100 mg QD with 1-6 wk Moderate Low-moderate Baseline: G6PD, CBC, LFT $
reduction as tolerated (C) Monthly: CBC, LFT x6 mo., then periodically
SSZ 500 mg BID withA nasty case of hives
Thank you!
www.mghcme.orgYou can also read