Lipoid Pneumonia: Spectrum of Clinical and Radiologic Manifestations
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
C a r d i o p u l m o n a r y I m a g i n g • P i c t o r i a l E s s ay
Betancourt et al.
Lipoid Pneumonia
Cardiopulmonary Imaging
Pictorial Essay
Lipoid Pneumonia: Spectrum
of Clinical and Radiologic
Manifestations
Sonia L. Betancourt 1 OBJECTIVE. Lipoid pneumonia results from accumulation of lipids in the alveoli and
Santiago Martinez-Jimenez 2 can be either exogenous or endogenous in cause based on the source of the lipid. Exogenous
Santiago E. Rossi 3 lipoid pneumonia is caused by inhalation or aspiration of animal fat or vegetable or mineral
Mylene T. Truong1 oil. Endogenous lipoid pneumonia is usually associated with bronchial obstruction. The pur-
Jorge Carrillo 4 pose of this article is to review the pathogenesis and clinical and radiologic manifestations of
exogenous and endogenous lipoid pneumonia.
Jeremy J. Erasmus1
CONCLUSION. The ability to recognize the radiologic manifestations of lipoid pneumo-
Betancourt SL, Martinez-Jimenez S, Rossi SE, nia is important because, in the appropriate clinical setting, these findings can be diagnostic.
Truong MT, Carrillo J, Erasmus JJ
L
ipoid pneumonia is uncommon and use of oil-based nose drops, can be acute
and, although it is difficult to de- or chronic in presentation [1].
termine the precise clinical inci- Acute exogenous lipoid pneumonia is un-
dence, autopsy series have re- common and typically is caused by an ep-
ported a frequency of only 1.0–2.5% [1]. isode of aspiration of a large quantity of a
However, it is important to be aware of the petroleum-based product [3, 4] (Fig. 1). Al-
various radiologic manifestations of lipoid though acute pneumonitis after aspiration
pneumonia because, in the appropriate clini- of petroleum-based products typically oc-
cal setting, these findings can be diagnostic. curs in children due to accidental poisoning,
Unfortunately, lipoid pneumonia can mimic acute exogenous lipoid pneumonia also oc-
the clinical and radiologic features of other curs in performers (fire-eaters) who use liq-
Keywords: aspiration, endogenous lipoid pneumonia, diseases including primary lung carcinoma, uid hydrocarbons for flame blowing.
exogenous lipoid pneumonia and histopathologic confirmation of the di- Chronic exogenous lipoid pneumonia usu-
agnosis may be necessary. ally results from repeated episodes of aspira-
DOI:10.2214/AJR.09.3040
Lipoid pneumonia can be either exogenous tion or inhalation of animal fat or mineral or
Received May 9, 2009; accepted after revision or endogenous in cause based on the source of vegetable oils over an extended period. Al-
June 14, 2009. the lipid. Exogenous lipoid pneumonia usual- though chronic exogenous lipoid pneumonia
1
ly occurs when animal fats or mineral or veg- typically occurs in older patients, it also has
Division of Diagnostic Imaging, Department of
etable oils are aspirated or inhaled [1], where- been reported in children, especially those
Diagnostic Radiology, The University of Texas M. D.
Anderson Cancer Center, Unit 0371, 1515 Holcombe Blvd., as endogenous lipoid pneumonia results from with a predisposition to aspiration, including
Houston, TX 77030. Address correspondence to S. L. lipid accumulation within intraalveolar mac- mental retardation and cleft palate, as well as
Betancourt (slbetancour@mdanderson.org). rophages in the setting of bronchial obstruc- in infants when mineral oil is used as a lu-
2
tion, chronic pulmonary infection, pulmonary bricant to facilitate feeding [1]. Chronic ex-
Department of Diagnostic Radiology, Duke University
Medical Center, Durham, NC.
alveolar proteinosis, or fat storage diseases ogenous lipoid pneumonia also can occur in
[2]. Because awareness and understanding of patients without a predisposing anatomic or
3
Centro de Diagnostico Enrique Rossi, Buenos Aires, lipoid pneumonia are essential in improving functional abnormality in swallowing. The
Argentina. diagnostic interpretation and appropriate pa- aspiration of fats or oils has been reported in
4 tient management, we review the pathogene- patients with a history of chronic use of min-
Departmento de Radiologia, Universidad Nacional de
Colombia, Hospital Universitario Mayor, Bogota, sis and clinical and radiologic manifestations eral oil or petroleum-based lubricants and
Colombia. of lipoid pneumonia. decongestants such as Vaseline (Unilever),
Vicks VapoRub, and lip gloss [1, 5] (Fig. 2).
AJR 2010; 194:103–109 Exogenous Lipoid Pneumonia Chronic exogenous lipoid pneumonia also
Exogenous lipoid pneumonia, initially de- can result from inhalation of mineral oil and
0361–803X/10/1941–103
scribed in 1925 by Laughlen in four patients has been described in a variety of indus-
© American Roentgen Ray Society with a prolonged history of laxative ingestion trial occupations, including those involved
AJR:194, January 2010 103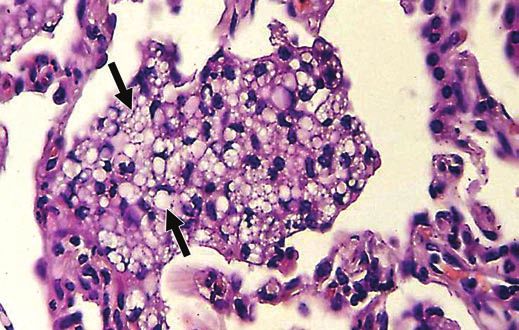
Betancourt et al.
in the lubrication and cleaning of machin- Radiologic Manifestations Characteristically, chronic exogenous li-
ery and the spraying of pesticides or paints Acute exogenous lipoid pneumonia can poid pneumonia manifests as an adipose-con-
[6]. Additionally, chronic exogenous lipoid manifest radiologically within 30 minutes of taining mass [1] (Fig. 8). Although the mass is
pneumonia has been reported as a result of the episode of aspiration or inhalation, and typically irregular or spiculated as a result of
embolization after rectal or subcutaneous pulmonary opacities can be seen in most pa- chronic inflammation and secondary fibrosis,
administration of mineral oils [7]. tients within 24 hours [9]. The opacities are the presence of fat in the mass is, with a few
typically ground-glass or consolidative, bi- exceptions, a diagnostic feature of exogenous
Pathophysiology lateral, and segmental or lobar in distribu- lipoid pneumonia. Specifically, hamartomas
The development of parenchymal abnor- tion and predominantly involve the middle and lung metastases from primary extratho-
malities in lipoid pneumonia is dependent on and lower lobes [10] (Fig. 5). Other manifes- racic sarcomas such as chondrosarcomas or
the type, amount, frequency, and length of tations of acute exogenous lipoid pneumonia liposarcomas can manifest as fat-containing
time of aspirated or inhaled oils or fats. Miner- include poorly marginated nodules, pneuma- lung nodules. Cavitation and calcification of
al oil (a mixture of inert, long-chain, saturated toceles, pneumomediastinum, pneumotho- the mass occasionally can occur.
hydrocarbons obtained from petroleum) and rax, and pleural effusions [9, 10]. Pneu- Other manifestations of chronic exogenous
vegetable-based oils tend to cause minimal to matoceles usually occur within regions of lipoid pneumonia are single or multiple nod-
mild inflammatory reactions (Fig. 3). The in- ground-glass or consolidative opacities, typ- ules or masses that may or may not contain
traalveolar oils can coalesce in the alveoli and ically manifest radiologically within 2–30 fat (Fig. 9). In the absence of fat, the nodules
become encapsulated by fibrous tissue, result- days after aspiration or inhalation, and are or masses can be indistinguishable from pri-
ing in a nodule or mass (paraffinoma) (Fig. 4). more common in patients who have aspirated mary lung cancer [13–16]. Furthermore, be-
Conversely, animal fats are hydrolyzed by or inhaled a large amount of mineral oils or cause of the inflammatory component, lipoid
lung lipases into free fatty acids that trigger petroleum-based products [11]. Pneumotho- pneumonia can have increased uptake of 18F-
a severe inflammatory reaction that manifests rax and pneumomediastinum are rare and FDG on PET and can thus be misinterpreted
as focal edema and intraalveolar hemorrhage have been reported to occur within 4 days af- as malignancy [17]. The radiologic manifesta-
[5]. Fatty acids either remain in the alveolar ter hydrocarbon aspiration. Importantly, they tions of chronic exogenous lipoid pneumonia
spaces or are phagocytosed by macrophag- are associated with a poor prognosis. can improve slowly over time but typically re-
es that then migrate to the interlobular septa. CT can reveal areas of fat attenuation main stable even if the exposure to vegetable
Regardless of location, the inflammatory re- as low as −30 HU within the consolidative or mineral oils or animal fats is discontinued
sponse can destroy the alveolar walls and the opacities and nodules, a finding diagnostic of [1]. Fibrosis and destruction of normal lung
interstitium, and the resultant fibrosis can oc- lipoid pneumonia. However, even though the architecture can result in cor pulmonale.
casionally progress to end-stage lung disease. attenuation of the opacities or nodules can
be low at initial presentation, the presence Endogenous Lipoid Pneumonia
Clinical Findings of superimposed inflammation can be a con- Endogenous lipoid pneumonia, also called
Acute exogenous lipoid pneumonia typi- founding factor by increasing the attenuation “cholesterol pneumonia” or “golden pneumo-
cally manifests clinically as cough, dyspnea, so that the fat component becomes less con- nia,” is an obstructive pneumonitis. Endoge-
and low-grade fever that usually resolve with spicuous or obscured [1, 10, 12]. nous lipoid pneumonia is a histopathologic di-
supportive therapy [1]. In contrast, patients The radiologic manifestations of acute ex- agnosis made on the basis of the characteristic
with chronic exogenous lipoid pneumonia are ogenous lipoid pneumonia typically improve appearance of the obstructive pneumonitis.
frequently asymptomatic on presentation and or resolve over time. Resolution of opacities Macroscopically, there is parenchymal con-
are only identified because of an incidental- is variable and usually occurs within 2 weeks solidation that has a characteristic yellowish
ly detected abnormality on radiologic imag- to 8 months [3]. Typically, resolution is com- discoloration due to the accumulation of lipid
ing. Most of these patients are elderly (sixth plete, although minimal scarring can occur. in the alveoli [18]. Histologically, there is an
or seventh decade of life); have an anatomic Similar to acute exogenous lipoid pneu- accumulation of lipid-filled macrophages and
or functional alteration to swallowing, with a monia, chronic exogenous lipoid pneumo- eosinophilic proteinaceous material derived
predisposition to aspiration; and have a histo- nia most frequently manifests as ground- from degenerating cells, including surfactant
ry of topical application or ingestion of lipids glass or consolidative opacities involving from type II pneumocytes, in the alveoli distal
[1]. However, a history of exposure to animal one or more segments, typically with a peri- to the bronchial obstruction.
fats or mineral or vegetable oils may not be bronchovascular distribution and predomi- Polarized light microscopy after staining
elicited, and a careful clinical history to iden- nant involvement of the lower lobes (Fig. 6). with sulfuric acid and acetic acid (Schultz
tify the source of aspirated or inhaled lipid Architectural distortion associated with the stain) usually reveals cholesterol crystals,
may be required. Symptomatic patients most consolidative opacities has been reported, a finding diagnostic of endogenous lipoid
frequently present with chronic cough or dysp- and thickening of the interlobular septa or fi- pneumonia. Endogenous lipoid pneumonia
nea. Although fever, weight loss, chest pain, brosis in the adjacent lungs can occur in the typically manifests radiologically as consoli-
and hemoptysis are less common at presenta- later stages due to the transportation of oils dative opacities distal to a central obstruct-
tion [1, 2], Gondouin et al. [8] reported fever from the alveoli into the lung interstitium ing lesion [19] (Fig. 10). However, unlike ex-
and weight loss in 39% and 34% of patients, (Fig. 7). Additionally, ground-glass opacities ogenous lipoid pneumonia, the accumulation
respectively. Auscultation of the lungs is nor- with associated interlobular septal thicken- of lipid-rich cellular debris does not mani-
mal in most patients but can reveal crepita- ing (crazy-paving pattern) with a basilar pre- fest radiologically as lipid-containing opaci-
tions or wheezes [1]. dominance have also been described. ties with low attenuation typical of lipid.
104 AJR:194, January 2010
Lipoid Pneumonia
Historically, endogenous lipoid pneumonia chial occlusion and typically manifests as an enous lipid pneumonia: a retrospective multi-
typically has been reported as being caused obstructive pneumonitis containing lipid dis- centre study of 44 cases in France. Eur Respir J
by non–small cell lung cancers but also can tal to a centrally located mass. However, un- 1996; 7:1463–1469
occur as a manifestation of infection and oth- like exogenous lipoid pneumonia, the accu- 9 Haas C, Lebas FX, Le Jeunne C, Lowenstein W,
er diseases that are not associated with bron- mulation of lipid-rich cellular debris does Durand H, Hugues FC. Pneumopathies caused by
chial obstruction. In this regard, an associa- not manifest radiologically as lipid-con- inhalation of hydrocarbons: apropos of 3 cases.
tion between endogenous lipoid pneumonia taining opacities, and the diagnosis is histo- Ann Med Interne (Paris) 2000; 151:438–447
and repetitive episodes of fungal pneumonia pathologic. Several other entities, including 10. Brechot JM, Buy JN, Laaban JP, Rochemaure J.
recently has been reported [20]. Additionally, pulmonary infections, lipid storage diseases, Computed tomography and magnetic resonance
in pulmonary alveolar proteinosis (PAP), the and pulmonary alveolar proteinosis are con- findings in lipoid pneumonia. Thorax 1991; 46:
alveoli are usually filled with protein and lipid sidered within the spectrum of endogenous 738–739
material resembling surfactant. PAP typical- lipoid pneumonia. The imaging findings in 11. Bandla HP, Davis SH, Hopkins NE. Lipoid pneu-
ly manifests on CT as ground-glass opacities, these diseases vary, and the clinical and his- monia: a silent complication of mineral oil aspira-
often with superimposed thickening of the in- tologic findings are often necessary to con- tion. Pediatrics 1999; 103:E19
terlobular and intralobular interstitia (crazy- firm the diagnosis. 12. Laurent F, Philippe JC, Vergier B, et al. Exoge-
paving pattern) [18]. Niemann-Pick disease, nous lipoid pneumonia: HRCT, MR, and patho-
a lipid-storage disorder in which accumula- References logic findings. Eur Radiol 1999; 9:1190–1196
tion of intraalveolar and interstitial fat-laden 1. Baron SE, Haramati LB, Rivera VT. Radiological 13. Brody JS, Levin B. Interlobular septa thickening
macrophages and sphingomyelin occurs, is and clinical findings in acute and chronic exoge- in lipid pneumonia. Am J Roentgenol Radium
also within the spectrum of endogenous li- nous lipoid pneumonia. J Thorac Imaging 2003; Ther Nucl Med 1962; 88:1061–1069
poid pneumonia. The radiologic manifesta- 18:217–224 14. Davis EW, Hampton AO, Bickham CE, Winship
tions of Niemann-Pick disease include diffuse 2. Woodhead M, Parkes WR. Disorders caused by T. Lipoid pneumonia simulating tumor. J Thorac
ground-glass opacities and thickening of in- other organic agents. In: Parkes WR, ed. Occupa- Surg 1954; 28:212–219
terlobular and intralobular interstitia, as well tional lung disorders, 3rd ed. Oxford, United 15. Scully RE, Galdabini JJ, McNeely BU. Case re-
as centrilobular nodular opacities [21]. Kingdom: Butterworth-Heinemann, 1994:778– cords of the Massachusetts General Hospital:
793 weekly clinicopathological exercises—case 22—
Conclusion 3. Kitchen JM, O’Brien DE, McLaughlin AM. Per- 1977. N Engl J Med 1977; 296:1279–1287
Lipoid pneumonia can be either exoge- ils of fire eating: an acute form of lipoid pneumo- 16. Spencer H. Pathology of the lung, 2nd ed. New
nous or endogenous in cause, and awareness nia or fire eater’s lung. Thorax 2008; 63:401, 439 York, NY: Pergamon Press, 1968:508
of these two different entities is important 4. Lifshitz M, Sofer S, Gorodischer R. Hydrocarbon 17. Tahon F, Berthezene Y, Hominal S, et al. Exoge-
in clinical practice. In addition, knowledge poisoning in children: a 5-year retrospective nous lipoid pneumonia with unusual CT pattern
of the various ways that a patient can be ex- study. Wilderness Environ Med 2003; 14:78–82 and FDG positron emission tomography scan
posed to lipid-containing material can help to 5. Seo JB, Im JG, Kim WS, Seong CK, Song JW, findings. Eur Radiol 2002; 12[suppl 3]:S171–
solicit a clinical history of lipid aspiration or Chung JH. Shark liver oil–induced lipoid pneu- S173
inhalation and facilitate the diagnosis of ex- monia in pigs: correlation of thin-section CT and 18. Gaerte SC, Meyer CA, Winer-Muram HT, Tarver
ogenous lipoid pneumonia. In fact, this infor- histopathologic findings. Radiology 1999; 212: RD, Conces DJ Jr. Fat-containing lesions of the
mation, together with the ability to recognize 88–96 chest. RadioGraphics 2002; 22[spec no]:S61–S78
the range of manifestations of exogenous li- 6. Bernabeu R, Méndez Martínez P, Abellan Mar- 19. Tamura A, Hebisawa A, Fukushima K. Lipoid
poid pneumonia, is essential in the diagnosis tínez MC, et al. Acute lipoid pneumonia caused by pneumonia in lung cancer: radiographic and
of this entity. In this regard, although the ra- accidental aspiration of Vaseline used in nasogas- pathological features. Jpn J Clin Oncol 1998; 28:
diologic findings of exogenous lipoid pneu- tric intubation. Arch Broncopneumol 2000; 36: 492–496
monia can be nonspecific, lipid-containing 485–487 20. Itoh Y, Segawa H, Kito K, et al. Lipoid pneumonia
opacities on CT images are diagnostic if there 7. Rabah R, Evans RW, Yunis EJ. Mineral oil embo- with chronic myelomonocytic leukemia. Pathol
is a history of use or occupational exposure to lization and lipid pneumonia in an infant treated Res Pract 2009; 205:143–147
lipid-containing materials. for Hirschsprung’s disease. Pediatr Pathol 1987; 21. Hansell DM, Armstrong P, Lynch DA, McAdams
In contradistinction, endogenous lipoid 7:447–455 HP. Imaging of diseases of the chest. Philadel-
pneumonia usually occurs as a result of bron- 8. Gondouin A, Manzoni P, Ranfaing E, et al. Exog- phia, PA: Elsevier, 2005:493–495
AJR:194, January 2010 105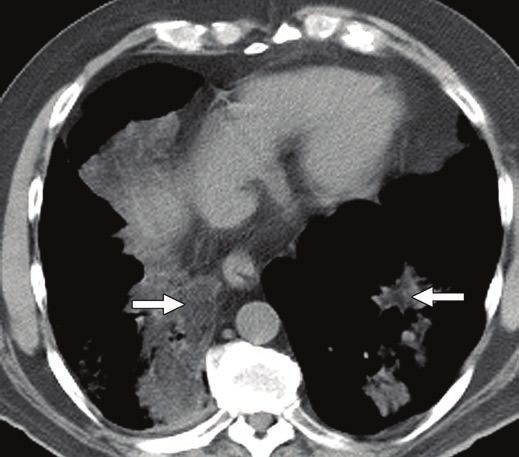
Betancourt et al.
Fig. 1—Acute exogenous lipoid pneumonia in 54-year-old woman after episode
of aspiration of large volume of mineral oil. High-resolution CT image shows
geographic distribution of ground-glass opacities and associated thickening of
interlobular septa (crazy-paving pattern). Note that although opacities may be
present soon after aspiration, radiologic manifestations of acute exogenous lipoid
pneumonia can take up to 24 hours to develop.
A B
Fig. 2—Chronic exogenous lipoid pneumonia due to repeated episodes of aspiration of mineral oil in 65-year-old woman with scleroderma manifesting as progressive
dyspnea and nonproductive cough.
A, Axial CT image (coned view) of right lower lobe shows geographic distribution of ground-glass opacities with associated interlobular septal thickening.
B, Photomicrograph shows intraalveolar and interstitial accumulation of lipid-laden macrophages (arrows), characteristic pathologic manifestation of lipoid pneumonia.
(H and E, original magnification ×100)
106 AJR:194, January 2010Lipoid Pneumonia
A B
Fig. 3—Chronic exogenous lipoid pneumonia in 63-year-old woman due to chronic aspiration of Vaseline (Unilever) petroleum-based lubricant.
A, Axial CT image shows consolidative and ground-glass opacities bilaterally. Note mild architectural distortion associated with consolidative opacities in left lower lobe.
B, CT image shows areas of fat attenuation within consolidation (arrows), finding diagnostic of lipoid pneumonia.
A B
Fig. 4—Exogenous lipoid pneumonia in asymptomatic 80-year-old man due to chronic aspiration of mineral oil manifesting as nodule (paraffinoma).
A, Coronal CT image shows spiculated left upper lobe nodule (arrow) and nodular opacities in left lower lobe. Note spiculation, typically indicative of malignancy, is due to
inflammatory reaction incited by mineral oil.
B, Coronal CT image shows fat attenuation within nodule (arrows), diagnostic of chronic lipoid pneumonia.
AJR:194, January 2010 107Betancourt et al.
A B
Fig. 5—Exogenous lipoid pneumonia in 56-year-old woman with history of partial gastrectomy and single episode of mineral oil aspiration.
A, Chest radiograph shows ground-glass opacities (arrows) in right lung.
B, Coronal high-resolution CT image shows ground-glass opacities with superimposed interlobular thickening bilaterally (crazy-paving pattern). Biopsy revealed
intraalveolar fat globules, confirming diagnosis of lipoid pneumonia.
Fig. 6—Exogenous lipoid pneumonia in 80-year-old man resulting from chronic Fig. 7—Exogenous lipoid pneumonia in 53-year-old man due to chronic aspiration
aspiration of mineral oil. Axial CT image shows consolidation and ground-glass of petroleum-based lubricant (Vaseline, Unilever). Axial CT image shows masslike
opacities in middle lobe and focal nodular opacities in left lower lobe. Note that consolidative opacity in middle lobe (arrows) and scattered consolidative and
although exogenous lipoid pneumonia typically has predominant lower lobe ground-glass opacities in right lower lobe and left lung. Note mild architectural
involvement, all lobes can be affected. distortion associated with consolidative opacity in middle lobe is result of
inflammation and scarring that occur due to transportation of oil from alveoli into
lung interstitium.
108 AJR:194, January 2010Lipoid Pneumonia
Fig. 8—Exogenous lipoid pneumonia in 78-year-old woman with history of chronic Fig. 9—Exogenous lipoid pneumonia in 42-year-old woman with history of colon
constipation and ingestion of vegetable oil laxative daily. Axial CT image shows cancer, constipation, and chronic ingestion of oil laxatives. Axial CT image
irregular masslike opacity (arrows) in middle lobe. Note fat attenuation within (coned view) shows multiple left lower lobe nodules with fat attenuation (arrows),
mass. Presence of fat is diagnostic feature of exogenous lipoid pneumonia. consistent with lipoid pneumonia.
A B
Fig. 10—Endogenous lipoid pneumonia in 49-year-old man due to central
bronchial obstruction who presented with 6-week history of hemoptysis and
fever. (Courtesy of Madewell JE, The University of Texas M. D. Anderson Cancer
Center, Houston, TX)
A, Chest radiograph shows masslike consolidation (arrows) in right lung.
B, Photograph of gross pathologic specimen after partial right upper lobe
resection shows well-circumscribed consolidation that has characteristic white-
yellow discoloration due to accumulation of lipid in alveoli (arrows).
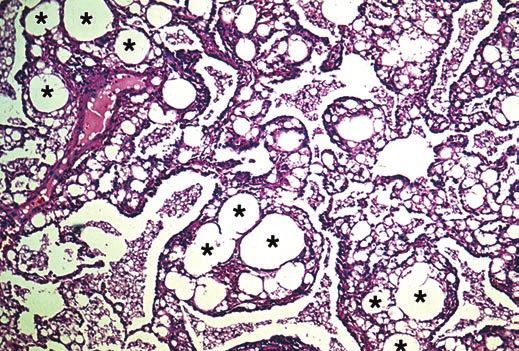
C, Photomicrograph shows lipid-filled macrophages (asterisks). Note that after
staining with sulfuric acid and acetic acid (Schultz stain) (not shown), polarized
light microscopy revealed cholesterol crystals consistent with diagnosis of
endogenous lipoid pneumonia. (H and E, ×40)
C
AJR:194, January 2010 109You can also read

















































