Headaches: from history keys for the future - Francesco De Cesaris, MD Headache Center and Clinical Pharmacology - ASIAM Aggiornamento medico
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Headaches: from history
keys for the future
Francesco De Cesaris, MD
Headache Center and Clinical Pharmacology
Azienda Ospedaliera Universitaria Careggi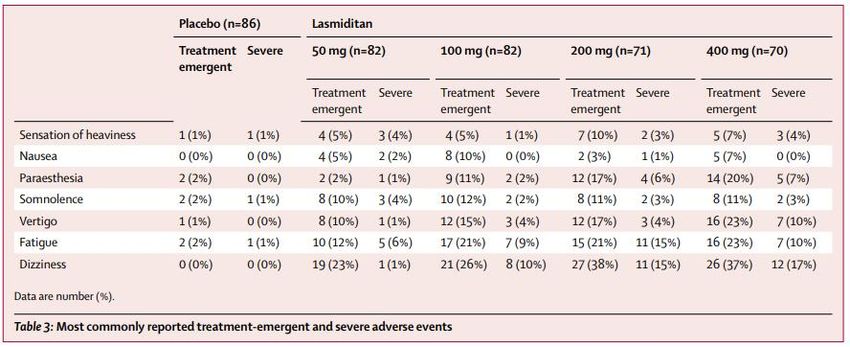
Financial disclosure (last two years)
Host to congresses and travel grants: Allergan, Eli Lilly,
Lusofarmaco, Novartis, Teva
Speaker at conferences: Angelini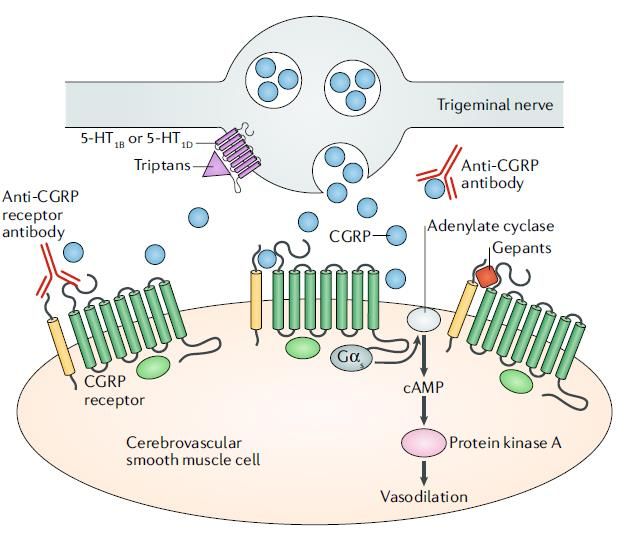

Primary Headache Disorders
Cluster
Clinical Comparison Migraine Headache Tension-Type Headache
Typical age of onset, Adolescence or
20-401,2 Any age, peaks at 40-493
years menarche1
Sex ratio: M/F
MF1,2 M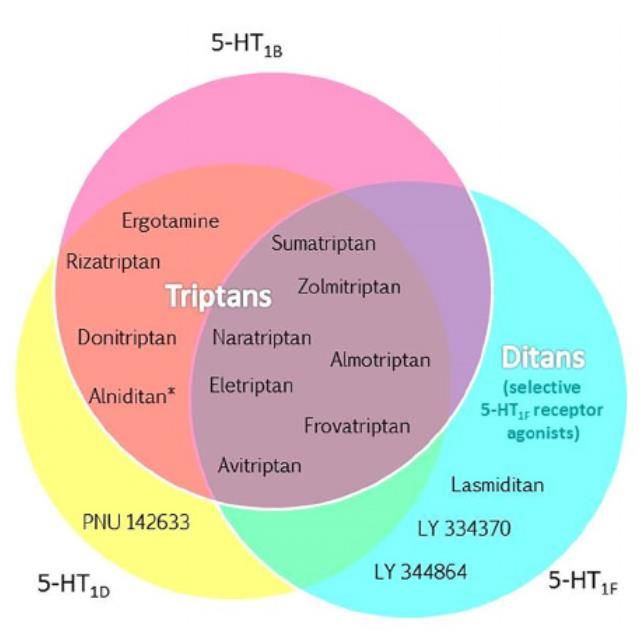
Algorithmic Approach to Diagnosing
Migraine
Headache
1,2
Red Flags Investigate
Comfort
Signs
Primary Headache
Disorder
Identify
Episodic Chronic
(
Possible Clinical Trajectories
of Episodic Migraine1,2
10%a Evolution to symptom-free over
Remission
prolonged period of time
84%a Relative clinical stability and no
EM Persistence markers of progression
Clinical
♦ Evolution to HFEM or CM
3% Functional
Progression
♦ Development of allodynia
Anatomical
aAn additional 3% of patients exhibit partial remission.2 ♦ Change in the PAG
CM=Chronic Migraine; EM=Episodic Migraine; HFEM=High-Frequency Episodic Migraine;
PAG=Periaqueductal Gray.
1. Lipton RB. Neurology. 2009;72(Suppl. 5):S3-S7. 2. Bigal ME, Lipton RB. Curr Opin Neurol.
♦ Lesions in the brain
2008;21:301-308.
♦ White matter hyperintensities
ICHD-3 Diagnostic Criteria for
1.3 Chronic Migraine
A. Headache (tension-type-like and/or migraine-like) on ≥15 days/month for >3
monthsa and fulfilling Criteria B and C
B. Occurring in a patient who has had ≥5 attacks fulfilling criteria for migraine
without aura and/or criteria for migraine with aura
C. On ≥8 days per month for >3 months, fulfilling any of the followinga:
1. Criteria C and D for 1.1 Migraine Without Aura
2. Criteria B and C for 1.2 Migraine With Aura
3. Believed by the patient to be migraine at onset and relieved by a
triptan or ergot derivative
D. Not better accounted for by another ICHD-3 diagnosis
aCharacterization offrequently recurring headache generally requires a headache diary to record information on pain and associated symptoms day-by-day for ≥1 month.
Sample diaries are available at http://www.headaches.org/.
ICHD-3=International Classification of Headache Disorders-3.
IHS. Cephalalgia. 2013;33:629-808.
Transition of Episodic Migraine to Chronic
Migraine1
Patients may transition among these 3 migraine states in the direction of
increasing and decreasing frequency
Transitions occur over weeks to months2
Back-transitions are common2,3
Low/ moderate- Chronic migraine
High-frequency
frequency episodic with/without
No migraine episodic migraine headache-free
migraine periods
0-9 days/month 10-14 days/month ≥15 days/month
1. Lipton RB. Neurology. 2009;72(Suppl. 5):S3-S7. 2. Katsarava Z, et al. Curr Pain Headache Rep. 2012;16:86-92. 3. Jancin B. Clin Psych News. 27 Sept 2012.
Clinical develop of chronic migraine
Every year 2,5% of patient affected by episodic migraine develops
chronic migraine1
Risk factors are2,3,4
Modifiable
Not modifiable
• Obesity
• Age
• Mood depression
• Sex
• Drug abuse
• Race
• Stress
• Cervical damage
• Caffeine abuse
• Snoring
• Allodynia
1.Bigal ME, et al. Headache 2008;48:1157–68.
2.Bigal ME, et al. Headache 2006;46:1334–43.
3.Lipton RB. Headache 2011;51:77–83.
4.Bigal ME, et al. Headache 2009;49:S21–33.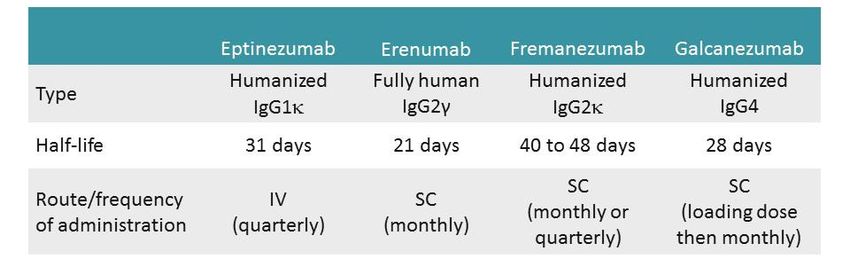
Some considerations on
chronic headaches
❖Chronic headaches are one of the most frequent
reason of access to headache centers
❖May be primary or secondary: the possibility of a
secondary headache must ever be conseidered
❖The two types of chronic headaches more
frequently diagnosed are chronic migraine and
chronic type tension headacheMedication-overuse headache (MOH) Headache occurring on 15 or more days per month developing as a consequence of regular overuse of acute or symptomatic headache medication (on 10 or more, or 15 or more days per month, depending on the medication) for more than 3 months. It usually, but not invariably, resolves after the overuse is stopped Diagnostic criteria: A. Headache occurring on 15 days per month in a patient with a pre- existing headache disorder B. Regular overuse for >3 months of one or more drugs that can be taken for acute and/or symptomatic treatment of headache C. Not better accounted for by another ICHD-3 diagnosis
Migraine: Epidemiology1 Affects ~36 million Americans1-4 Affects women more than mena Episodic migraine (EM):
Migraine prevalence
Donne Uomini
30
n=3738
Prevalnza dell’emicrania (%)
25
20
15
10
5
0
20 30 40 50 60 70 80 100
Età (anni)
Silberstein et al. Neurol Clin 1996;14:421-34Disability due to migraine
80
n=3738
60
52
Patient (%)
40 39
20
9
0
Normal activity Moderate impairment Higher impairment
Lipton et al., 2001In the age group 15–49 years, migraine is the top cause of YLDs (years lived with disability). Let us not forget that these are the productive years, when education is completed, families formed, children raised, careers built and prospects for the whole remainder of life established.
Costs of chronic migraine
Chronic migraine is associated
Ricoveri/ED
to higher costs than episodic Visite da parte
migraine dell’assistenza sanitaria
Trattamenti
Patient affected by chronic Farmaci
migraine perform more visits
and exams and go frequently to
emergency department than
Costo annuo (€)
patients affected by episodic
migraine
Medical costs for patients €1092.48
affected by chronic migraine are
three times more than for
episodic migraine
UK Francia Germania Italia Spagna
Figura adattata da Bloudek LM, et al. 2012
ED = pronto soccorso; CM = emicrania cronica; EM = emicrania episodica.
1. Bloudek L.M et al. J Headache Pain 2012;13:361–78.Migraine Comorbidities
Several comorbid diseases occur in migraineurs with greater frequency than in
the general population
Neurologic
Non-
headache Cardiac
pain
Migraine
Psychiatric Vascular
Other
Scher AI, et al. Curr Opin Neurol. 2005;18:305-310.Comorbidity Profiles of CM and EM Populations
Differ on Multiple Dimensions
Patients (%) With Statistically Different
‡
Conditions Between CM and EM
‡
‡
‡ ‡
‡ ‡ ‡
*
‡ *
‡ ‡ ‡
‡ *
†
* *
*p≤.05; †p≤.01; ‡p≤.001 for comparisons between CM and EM.
aPatient Health Questionnaire-9.
bSelf-report of a physician diagnosis.
CM=Chronic Migraine; COPD=Chronic Obstructive Pulmonary Disease; EM=Episodic Migraine.
Buse DC, et al. J Neurol Neurosurg Psychiatry. 2010;81:428-432.A Neurophysiological Model of Migraine
Pathogenesis1-3
Modulating Factors Cortical Waves ↑BBB Permeability
Drugs Cortical-spreading depression
Environment Astrocyte Ca2+ waves Aura
Gender/hormones CBF changes (hyperemia followed by Visual
Genes oligemia)2 Sensory
Ionic/metabolic Cognitive
Activation of Pain Receptors
Release of nociceptive messengers (SP,
NO, ANP)
Vascular/metabolic uncoupling
Release of vasoactive peptides (CGRP,
NKA, SP) →
Neurogenic inflammation, vasodilation,
protein extravasation3
Migraine
Disturbance of Cortical and/or Attack
Brainstem Excitability Brainstem Activation
Trigeminal nucleus caudalis Sensory Sensitivity
ANP=Atrial Natriuretic Peptide; BBB=Blood-Brain Barrier; CBF=Cerebral Blood Flow; Photo/phonophobia
CGRP=Calcitonin Gene-Related Peptide; NKA=Neurokinin A; NO=Nitric Oxide; Dorsolateral pons Cutaneous allodynia
SP=Substance P. Central sensitization Nausea
1. Charles A, Brennan KC. Handb Clin Neurol. 2010;97:99-108. 2. Olesen J, et al. Ann Vertigo
Neurol. 1981;9:344-352. 3. Malhotra R. Ann Indian Acad Neurol. 2016;19:175-182.Prevalenza dell’emicrania in
Toscana
Popolazione 3.173.234
adulta1
Prevalenza
dell’emicrania 2 368.095 11,6%
Diagnosticati3 143.557 39%
> 4 gg al mese di emicrania 4 66.036 46%
trattati con almeno una
terapia di profilassi5 12.936 20%
pazienti che non
persistono in terapia 10.737 83%
a 12 mesi6
1. DEMOISTAT 2017; 2. Roncolato et al.. Eur. Neurol. 2000; 3. Decision Resources Group Migraine Report 2014; 4.
Estimated according ELMA Research; 5. Studio di Real World Evidence “Consumo di risorse e costi in pazienti affetti
da emicrania” condotto da CLICON in collaborazione con Novartis - DATA ON FILE; 6. Studio di Real World
Evidence EPIMIG “Epidemiologia dell’emicrania cronica ed episodica e relativi pattern di utilizzo dei farmaci”
condotto da HEALTH SEARCH in collaborazione con Novartis – DATA ON FILEMigraine Preventive-Treatment
US, Canadian, and European guidelines2-5 include the
1 following circumstances under
Guidelines
which migraine preventive treatment should be considered:
Recurring migraine attacks that significantly interfere with a patient’s quality of
life and daily routine despite trigger management, appropriate use of acute
medications, and lifestyle modification strategies
Frequent headaches,a because of the risk of chronic migraine
Acute medication failure, contraindication, overuse, or unmanageable side
effects
Patient preference (ie, desire to have as few acute attacks as possible)
Certain migraine conditions:
– Hemiplegic migraine
– Basilar migraine (migraine with brainstem aura)
– Frequent, prolonged, or uncomfortable aura symptoms
– Migrainous infarction
a4 or more attacks per month, or 8 or more headache days per month.
US=United States.
1. Silberstein SD. Continuum (Minneap Minn). 2015;21:973-989. 2. Silberstein SD, et al. Neurology. 2012;78:1337-1345. 3. Holland S, et al. Neurology. 2012;78:1346-1353.
4. Pringsheim T, et al. Can J Neurol Sci. 2012;39(2 Suppl. 2):S1-S59. 5. Carville S, et al. BMJ. 2012;345:e5765.Agents for Prevention of Migraine1,2
5 FDA-approved agents:
– Propranolol (beta-adrenergic blocking agent)
– Timolol (beta-adrenergic blocking agent)
– Divalproex sodium (antiepileptic)
– Topiramate (antiepileptic)
– OnabotulinumtoxinA
FDA=Food and Drug Administration.
1.Bamford CC. In: The Cleveland Clinic Manual of Headache Therapy. 2015:122. 2. http://www.tafp.org/Media/Default/Page/professional-development/TFMS/syllabus/Migraine-
FriedmanHutchinson-Handout.pdf (Accessed March 2017).Classification: Migraine-Preventive
Therapies1,2,a
Level A: Established Efficacy
Antiepileptic Drugs β-Blockers Triptanb
Divalproex sodium Metoprolol Frovatriptan
Sodium valproate Propranolol
Topiramate Timolol
Level B: Probably Effective
Antidepressants/SSRI/SSNRI/TCA β-Blockers Triptansb
Amitriptyline Atenolol Naratriptan
Venlafaxine Nadolol Zolmitriptan
Level C: Possibly Effective
ACE Angiotensin Antiepileptic
Inhibitor Receptor Blocker α-Agonists β-Blockers Drug Antihistamine
Lisinopril Candesartan Clonidine Nebivolol Carbamazepine Cyproheptadine
Guanfacine Pindolol
aRecommended guidelines: Not all medications are FDA approved for treatment of migraine.
bFor short-term, menstrually associated migraine prevention.
ACE=Angiotensin-Converting Enzyme; FDA=Food and Drug Administration; SSRI=Selective Serotonin Reuptake Inhibitor; SSNRI= Selective Serotonin-Norepinephrine
Reuptake Inhibitor; TCA=Tricyclic Antidepressant.
1. Estemalik E, Tepper S. Neuropsychiatr Dis Treat. 2013;9:709-720. 2. Silberstein SD, et al. Neurology. 2012;78:1337-1345.BonTA ha dimostrato una riduzione della frequenza giornaliera dell'emicrania
rispetto al placebo1-3
Variazione media dei giorni di cefalea alla settimana 24 Variazione nella frequenza di giorni di emicrania/mese
rispetto al baseline1,2,3 alla settimana 24 rispetto al baseline1,2
Variazione Variazione
media media
rispetto rispetto
al baseline al baseline N=338 N=358
N=341
N=347
p≤0.006 BonTA Placebo
p≤0.002
Nota: trattandosi di studi diversi, condotti su popolazioni diverse, non sono direttamente confrontabili.
1. PREEMPT1 - Aurora SK, et al. Cephalalgia. 2010;30(7):793-803
2. PREEMPT2 - Diener HC, et al. Cephalalgia. 2010;30(7):804-814
3. COMPEL Study: Blumenfeld et al. J Headache and Pain. 2018;19 (13):1-12.Immediata diminuzione della cefalea dopo interruzione dei farmaci per il
trattamento acuto
Analgesico singolo Ergotamina
Analgesici in associazione Triptani
3 100
90
80
Pazienti con cefalea (%)
Intensità della cefalea
2 70
60
50
40
1
30
20
10
0 0
1 2 3 4 5 6 7 8 9 10 11 12 13 14 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Giorni di interruzione della terapia Giorni di interruzione della terapia
Figura adattata da: Diener HC and Limmroth V Lancet Neurol 2004;3:475–83Risultati a lungo termine con il trattamento profilattico rispetto all’interruzione
improvvisa dei farmaci per il trattamento acuto1
Controlli Controlli
Solo interruzione improvvisa Solo interruzione improvvisa
Profilassi dall’inizio Profilassi dall’inizio
30
60
riduzione dei giorni di cefalea/mese (%)
25 p=0.01
Pazienti che mostrano il 50% di
No. di giorni di cefalea/mese
50
20
40
15
30
10
20
5 10
0 0
0 1 2 3 4 5 6 7 8 9 10 11 12
Mese 3 Mese 5 Mese 12
Mesi dopo l’interruzione Mesi dopo l’interruzione
Figura adattata da Hagen K, et al. 2009
1. Hagen K et al. Cephalalgia 2009;29:221–32Current Therapeutic Strategies to Counteract CGRP signalling
Edvinsson et al., 2018
Nat. Rev. Neurol.anti-CGRP Biologics
CGRP biologics - Overview
CGRP biologics
Overview of placebo-controlled Phase 3 clinical trials in Migraine
Eptinezumab Erenumab Fremanezumab Galcanezumab
PROMISE1 PROMISE2 ST RIVE ARISE LIBERT Y HALO-EM HALO-CM EVOLVE1 EVOLVE2 REGAIN
3 Months 3 Months 6 Months 3 Months 3 Months 3 Months 3 Months 6 Months 6 Months 3 Months
0
-2 140
Monthly Migraine days
70
70
100 225
-4 30
140 675
p
300 p 675 120 240
p 675 120 240
p 225 120 240
225
-6
-8 100
300
-10
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
1
2
3
4
5
6
7
8
9Responder rates to CGRP biologics in episodic migraineurs
Galcanezumab
Galcanezumab Is the Only Agent Within the Class Investigated With ≥75% and 100% Response Rates as Pre-specified Endpoints in Clinical Trials
Mean % of Patients Months 1 to 6
Mean % of Patients Months 1 to 6
PBO
PBO
GMB 120 mg GMB 120 mg
62% ***pEarly Response: Evidence of a readily accessible therapeutic target
Galcanezumab
0 EVOLVE 1 EVOLVE 2
PBO
LS Mean Change From Baseline (SE)
PBO
LS Mean Change From Baseline (SE)
GMB 120 mg GMB 120 mg
-1
-2
Improvement
Improvement
-3
-4
*** *** ***
***
-5 *** ***
*** ***
***pMaintenance of Effect Over Time
LS Mean Change From Baseline (SE)
Improvement
Galcanezumab 120 mg
MHD baseline 9,72
MHD overall reduction -5.6 (95% CI: -6.3, − 5.0)
Camporeale, et al. BMC Neurol. 2018;18(1):188.The “placebo-like” tolerability of CGRP biologics
Dropout due to Adverse Effects
25.0
22.5
% of patients 20.0
17.5
15.0
12.5
10.0
7.5
5.0
2.5
0.0
Va lol
ez b
en b
ne ab
e
e
ab
tin line
a
To oat
at
a
o
um
um
um
m
m
an
ti
r
zu
rip
ra
lp
ez
op
pi
yt
an
Er
Pr
Am
ca
Ep
em
al
G
FrCGRP biologics – Future Perspectives
Add-on therapy with existing complementary preventive therapies
Add-on therapy with future treatments (gepants, ditans…)
Efficacy in menstrual migraine
Efficacy in MOH and need for withdrawal
Efficacy in TACs, tensive and other types of headache
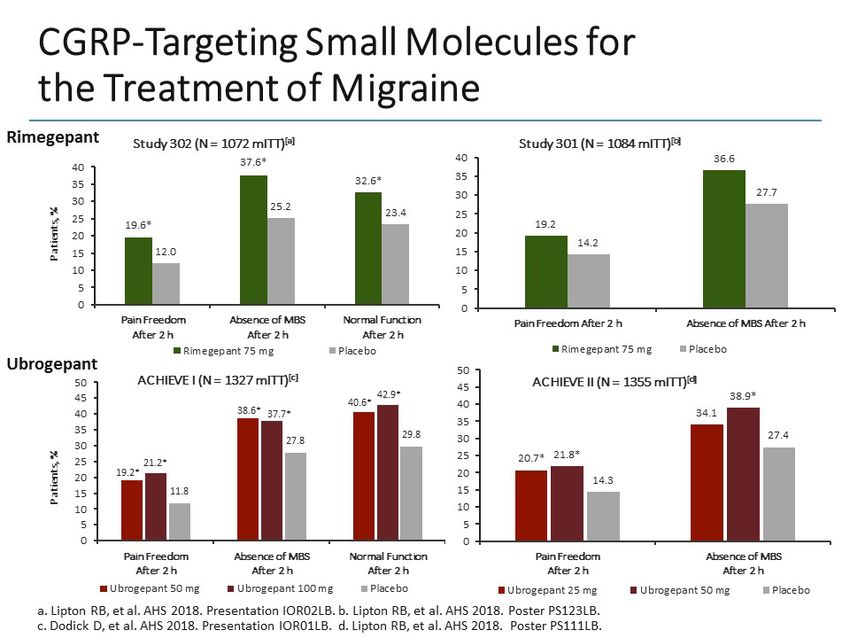
Identification of biomarkes for efficacy predictabilityGEPANTS
Gepants: a historical snapshot
• Several positive phase 2 and 3 trials with olcegepant and telcagepant as abortive agents in migraine were
overshadowed by hepatotoxicity concerns emerging in a study with telcagepant dosed twice daily for 3 months
and revealing elevated liver enzymes in 13 patients.
• Telcagepant's development was terminated in 2011 and development of gepants abandoned
• However, in 2015 a renewed interest emerged for new, potent gepants such as ubrogepant (MK-1602), atogepant
(MK-8031/AGN-241689) and Rimegepant.ATOGEPANT
CGP-MD-01 Phase 2b/3 clinical trial to evaluate the efficacy, safety, and tolerability of orally administered atogepant for 12 weeks for the
prevention of episodic migraine.
Higher potency and longer half-life than ubrogepant making it suitable for preventive treatment.
834 adult patients 18/75 years, history of migraine for at least 1 year, 4 to 14 migraine/probable migraine headache days per month
Randomization (2:1:2:1:2:1)
Placebo
Atogepant 10-mg QD,
Atogepant 30-mg QD and BID
Atogepant 60-mg QD and BID
Primary endpoint: change from baseline in mean monthly migraine days across 12-week treatment period
Placebo Atogepant Atogepant Atogepant Atogepant Atogepant
10 mg QD 30 mg QD 60 mg QD 30 mg BID 60 mg BID
(N=178) (N=92) (N=182) (N=177) (N=79) (N=87)
Change from Baseline
LS Mean (SE) -2.85 (0.23) -4.00 (0.32) -3.76 (0.23) -3.55 (0.23) -4.23 (0.35) -4.14 (0.33)
Atogepant vs Placebo
Adjusted p- 0.0236 0.0390 0.0390 0.0034 0.0031
value
Well tolerated, there was no signal of hepatotoxicity
Atogepant could be submitted to regulators by 2021.Triptans and Gepants head to head….
DITANS
Triptans’ binding to 5HT1 receptor subtypes
Phase 3, studies SAMURAI (NCT02439320) and SPARTAN (NCT02605174)
Inclusion criteria: Moderate migraine disability and 3–8 migraine attacks per month (SAMURAI > 80% pz had cardiovascular risk).
Patients:
SAMURAI, 1:1:1 ratio of lasmiditan 200/100 mg or placebo (2231 patients)
SPARTAN, 1:1:1:1 ratio of lasmiditan 200/100/50 mg or placebo (3007 patients)
SAMURAI
% of pain free : Lasmiditan 32.2%, Placebo 15.3%,
% of MBS-free: Lasmiditan 40.7%, Placebo 29.5%,
SPARTAN
% of pain free Lasmiditan 38.8%, Placebo 21.3%
% of MBS-free Lasmiditan 48.7%, Placebo 33.5%
Pain free 2h MBS free 2h
60
SPARTAN
SAMURAI
SPARTAN
% of patients
40 SAMURAI
pConclusions
• Both Gepants and Ditans proved efficacious in several Phase III studies for the
symptomatic treatment of episodic migraine
• Atogepant proved efficacious also in prevention of episodic migraine
• Data streghten the patogenetic role of neuronal modulation of CGRP release
• Hepatoxicity of gepants is not a «class effect»
• Ditans’ tolerability profile might be of concernTreatments Under Investigation for Migraine
You can also read