IGA News Spring 2019 - Patron: Dame Maggie Smith - International Glaucoma Association
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
IGA News
Spring 2019
???
?? ? e x it
B r
Patron: Dame Maggie Smith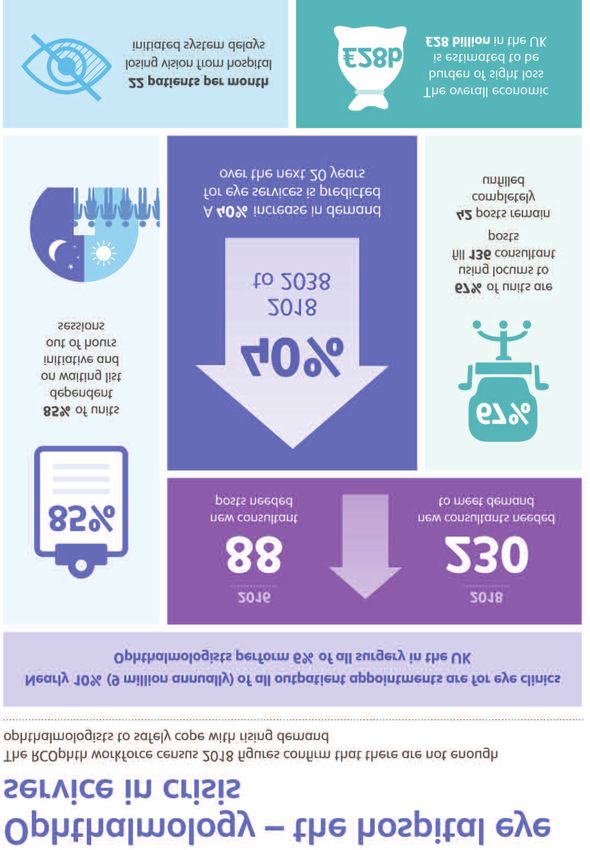
Contents Letter from the editor Page 1 News Page 2 Research Page 17 Research grants Page 21 Talking glaucoma Page 25 Experience Page 31 Support groups Page 34 INTERNATIONAL GLAUCOMA ASSOCIATION Woodcote House,15 Highpoint Business Village Henwood, Ashford, Kent TN24 8DH Sightline helpline: 01233 64 81 70 General enquiries: 01233 64 81 64 Email: info@iga.org.uk Website: www.glaucoma-association.com Design/artwork: Yes Design Printed by: Fuller Davies Ltd Charity registered in England & Wales No. 274681, in Scotland No. SC041550IGA’s new Online Cover: The impact of Brexit on the supply of medicines

Letter from the editor
Royal College of Ophthalmologists -
is planning a special glaucoma edition
in January 2020, and we’re honoured
to have been asked to submit a
patient-centred review article.
This is our opportunity to
reach thousands of medical
professionals and tell them
what matters most to
glaucoma patients, so we
want to hear from you!
Welcome to our
Spring 2019 edition. Please do get in touch and tell
us the things you would like
This IGA News kicks off with ophthalmologists to know.
Brexit. Many members have been How can they change their practice
worried about the supply of to improve the lives of patients?
medication post-Brexit, so we put Do you have examples of care
some questions to the main excellence to share, or examples
pharmaceutical companies on your of problems we should all strive to
behalf. Their responses are on pages avoid? Do you find it easy to be
two to five. open and honest with consultants?
What do you struggle with most
This edition also brings you a long when visiting the eye clinic? Let us
News section followed by details of know and we’ll tell the professionals.
our recent campaigning activities, You can email us at info@iga.org.uk
including World Glaucoma Week in or write to us at the address on the
March, plus plans for Ramadan in left. I’d love to hear from you.
May and Glaucoma Awareness Week
in June. I’m also delighted to bring
you information about the most
recent IGA-funded research grants in
optometry and ophthalmology.
Karen Osborn
Finally, I’d like to ask for your help. Chief Executive
Eye – the official journal of the
News Spring 2019 1
News
The impact of Brexit on the supply of medicines…
As 29 March draws closer we are receiving more and more calls from people
worried about supplies of eye drops post Brexit. So we put some questions to
the leading pharmaceutical providers of drops: Santen, Allergan,Thea, Novartis
and Pfizer. We asked:
• What impact do you think Brexit will have on the availability of your
glaucoma and ocular hypertension eye drops for people in the UK?
• What are the key factors affecting availability, and is your company able
to take any action to alleviate any potential supply issues?
• Do you envisage that any availability issues will affect all geographic regions
and all types of clinical centres equally?
• Have you been given any guidance from the UK Government?
• Is there any advice you would offer people living with glaucoma and OHT
in the UK who may face supply issues in the coming months?
Inevitably there is a lead-in time for a magazine like IGA News, so whilst this
edition will hit your doormats at around Brexit Day Zero, the responses were
given in mid-February 2019. (We asked the companies to limit their responses
to 400 words, for obvious reasons). Our grateful thanks go to all the companies
for their replies.
First up was Craig Wallace, Santen’s General Manager UK & Ireland,
who told us: “Yes, Brexit creates some uncertainty and potential risks to the
supply of medicines. The level of risk will depend upon the complexity of a
company’s supply chain, how disrupted the normal flow of goods are if a hard
Brexit occurs and what level of contingency a company has built.
“As I am sure you are aware the UK government are concerned about this
which is why there is a standing Health Select Committee reviewing this topic.
The Department of Health has also written to all manufacturers asking us all to
build additional stocks where we can and have asked us all for details of how our
2 News Spring 2019
News
products flow into the UK, so they can put alternative routes into the UK
avoiding usual entry points like Dover if this contingency is required. The UK
Pharmaceutical trade association for branded medicines, ABPI, has been advising its
member companies for well over a year to prepare for a hard Brexit.
“At Santen we have one of the most comprehensive ranges of glaucoma medicines
of any pharmaceutical company, plus important medicines for dry eye disease,
infection and allergy. Meeting the needs of patients and our customers and
maintaining our supply chain is therefore critical.
“As a result we have had a Brexit task force in place since 2017, chaired by me with
experts from across our business. We carried out a comprehensive risk assessment
across our business and this confirmed the supply of our medicines was our biggest
risk since all of our products are imported into the UK from Europe. As a result,
we have implemented a comprehensive Brexit contingency plan that has significantly
increased stock levels of all of our products held in the UK at our wholesaler. We
will have approximately three months of supplies vs the four weeks normally held.
We also have several months of additional supplies held in our European
distribution centre in Germany that can be shipped to the UK to maintain stock
levels as needed. Once the UK government has completed its work looking at new
entry points into the UK avoiding Dover we are ready to quickly change to these
entry points as well to ensure our products enter the UK smoothly and without
any unnecessary delays if required.”
Sunni Patel, Allergan’s Director, Eyecare UK and Ireland told us:
“Allergan’s priority is to maintain supply of our medications to people with
glaucoma and healthcare professionals across the UK. We have been carefully and
consistently evaluating the impact of the differing Brexit scenarios to ensure that
patients will continue to have access to the products they need.
“Allergan is actively stockpiling medicines to ensure products are available to
patients with glaucoma. We have set up a specialist team to plan for the differing
Brexit scenarios and have already put several actions into place to alleviate any
potential supply issues. These include:
• Working with the relevant authorities to ensure we can utilise all “fast-track”
options regarding customs arrangements.
News Spring 2019 3
News
• Working with our distribution networks to assess if we need to make
amendments to accommodate possible changes to current customs
arrangements.
“Our top priority is to ensure that all people with glaucoma receive the
medications that they need, across our EU markets. We do not anticipate Brexit
having an impact on product availability in EU markets.
“Allergan is following the guidance issued by The Department for Health and Social
Care. This has involved an analysis of our supply chains as well as the stockpiling of
medicines above and beyond our usual supply levels to offset any potential delays
that may arise in the short term. If people living with glaucoma have any concerns
about the availability of their medications, our advice would be to direct them to
speak with their healthcare practitioner.”
Dr Matthew Olsen, Marketing Manager at Thea Pharmaceuticals Ltd said:
“It has been well covered in the press that the government has requested
pharmaceutical companies increase their stock holding of medicines in the UK
by six weeks of ‘stock cover’ to help reduce any risk of stock outs. We have
agreed to that and put it in place.
“At this time we would anticipate that there will be minimal impact of Brexit on
availability of our eye drops. We have been working hard to minimise the risk of
stock out, and will continue to do everything we can to ensure this is the case.”
Lauren at Pfizer’s UK Press Office told us:
“We aim to have sufficient medicine and vaccine reserves at all times to ensure
continuity of supply for patients. We have undertaken work to ensure we can
continue to supply in the EU and the UK in all Brexit outcome scenarios and
are taking into account the recent UK Department of Health guidance on
medicine and vaccine supplies in preparation for the UK leaving the EU under a
“no deal” scenario.
“To protect patient safety and public health, we support a comprehensive and
pragmatic agreement between the EU27 and UK to minimise any potential
disruption in medicines and vaccines.”
4 News Spring 2019
News And finally Novartis pointed us to their website where a statement from January 2019 included these comments: “It is vital that Government makes minimising disruption to the medicines supply the highest priority as it prepares for a potential hard or disorderly Brexit and ensures cooperation over medicines regulation in this event. Given the complex nature of the supply chain, Government needs to implement a comprehensive continuity plan rapidly that includes relevant departments beyond the Department of Health and Social Care and the NHS, to ensure medicines can reach patients in the event of a no-deal Brexit. This includes clarity over customs arrangements, both to and from Europe, and to minimise disruption at our borders. It is also imperative that NHS trusts and pharmacists adhere to the Government’s advice not to stockpile medicines so supply can be managed centrally, minimising the risk of medicine shortages across the UK.” So what is our advice? IGA Chair of Trustees, Professor Philip Bloom gave some reassurance: "We are aware how unsettling it is for patients and carers when eye drops are changed. Usually this is done to improve the pressure-lowering effect or the tolerability of the medicine, but sometimes for other reasons such as available supply or cost. “I can reassure our members there are suitable, effective alternatives to almost all medicines. There are two-four different drugs in each of the four-five classes of medication, in addition to combination and preservative-free products. Furthermore, in addition to proprietary drops (which carry the manufacturer’s trade name as well as the drug’s chemical name), there are now a range of generic alternatives to most drops. “The net result is great choice of drops available to eye care professionals, and much flexibility for drop combinations. It is of course always best to be organised and to plan ahead for new supplies so drops do not run out, and this also gives your pharmacist time to suggest alternatives in the event of supply issues, often after discussion with your local eye department. “If you have any queries or concerns, please consider ringing Sightline to talk to one of our empathetic and knowledgeable staff." News Spring 2019 5
News
Driving improvements at the DVLA
One of the biggest fears associated with being diagnosed with glaucoma is the impact it
has on quality of life, including the ability to drive. This makes the IGA’s relationship with
the DVLA one of our most important. We work closely with the agency to ensure if you
are diagnosed with glaucoma, the process of having your vision tested and the subsequent
decision about your driving licence is managed clearly and fairly. The UK has one of the
best road safety records in the world, which the DVLA is keen to maintain, while ensuring
the individual’s experience of reporting a medical condition is as pain-free as possible.
The DVLA hosts a charities’ forum every six months, where medical charities can learn
about the DVLA’s work on medical conditions and discuss how to improve people’s
experiences. At the last forum in January 2019, three topics were up for discussion: the
DVLA’s online portal, the Honorary Medical Advisory Panels and the DVLA’s statistics on
medical conditions.
If you are diagnosed with a medical condition that may affect your ability to drive, you are
legally obliged to notify the DVLA. You only need to inform the DVLA if you have
glaucoma in both eyes. However, if you are a commercial driver, you need to notify the
DVLA even if you only have glaucoma in one eye.
To make this easier, the
Contact the DVLA: DVLA have an online
portal: www.gov.uk/
Drivers ’ Medical Enquiries report-driving-medical-
DVLA Swansea SA99 1TU condition
glaucomaqueries@dvla.gov.uk
Licence Group One call: 0300 79 06 806 This can be used either to
LGV and PVC Group Two call: 0300 79 06 807 notify the DVLA of a new
diagnosis, or for a review of
an existing condition,
usually every one to three years. If you prefer, you can continue to contact the DVLA via
phone, email or post.
The DVLA also runs six Honorary Medical Advisory Panels, with members appointed by
the Secretary of State for Transport. One of these is for visual disorders. The
membership of this panel includes doctors, DVLA staff and lay members. The role of this
panel is to assist in the management or development of medical standards and policies
and to help with decisions for individual cases. Lay members are recruited every six
6 News Spring 2019
News
months; their role is to offer constructive challenge to the panel and to provide the
patient voice. If you are interested in becoming a lay member of this panel, keep an eye
on the Civil Service Jobs website.
The DVLA are keen to share the statistics they hold on medical conditions and licencing
decisions. They are in the process of developing dashboards of key facts associated with
different medical conditions. These will include:
• Typical customer pathways upon notification of a medical decision
• Time taken for decisions to be made, including for complex conditions
• The age groups and genders of individuals notifying the DVLA of conditions
• The geographic distribution of individuals notifying the DVLA
As soon as we receive the data on glaucoma we will share it with you. Hopefully this
will help you understand the process and manage your expectations, for example how
long it may take for the DVLA to make a decision. The data will also help us identify
where we might need to work more closely with the DVLA to make the process
smoother or clearer.
In 2018 the DVLA’s online portal received
• 35,000 notifications of new medical conditions
• 34,500 reviews of existing medical conditions
News Spring 2019 7
News
We understand a number of a members have had difficult experiences with the DVLA.
However, we left the forum feeling the DVLA are trying really hard to get it right and get
the correct balance between road safety and an individual’s wish to drive. Please continue
to provide us and the DVLA with any feedback on your experiences, so we can work
’
together to improve the process as much as possible.
Idi d n t
t ha t !
kn o w
700,000 of licencing decisions made by the DVLA each year
4.1% of licence holders have a medical condition
6% annual revocation rate for individuals with glaucoma
34 days DVLA’s average decision time following an
individual’s notification of a medical condition
150 vision conditions monitored by the DVLA
Recent campaigns by DVLA:
#winterdriving
#wearyourglasses #eye735t
8 News Spring 2019News MIGS 2019: what’s happening in the world of glaucoma? In January, the Sightline team attended the 11th Moorfields International Glaucoma Symposium (not to be confused with Minimally Invasive Glaucoma Surgery, aka MIGS!) held at the Royal College of Physicians in London. Well-respected glaucoma surgeons from around the globe attend and give talks on all aspects of glaucoma and related eye conditions and the different treatment options. They do not always agree but this allows for colourful discussions into the best way to treat their patients. Talks ranged from landmark trials and what we are learning from them, through discussions of the best treatment options, to new research for the future which will improve patients’ experiences and outcomes. One of the talks by Professor Jonathan Crowston looked at the impact of exercise on the health of retinal ganglion cells (RGCs). An RGC is a type of neuron located near the inner surface - the ganglion cell layer - of the retina. It receives visual information from photoreceptors via intermediate nerve cells and passes the information on to the brain. Studies on mice have shown that if exposed to high pressure, these RGCs can be damaged, but recovery is better in younger mice than older ones. But if the older mice exercise, this strengthens RGCs. This effect is also seen in humans – the progression of glaucoma in a person who runs more than six km a day tends to be slower than in someone more sedentary. When Sightline receives calls from people asking about a healthy lifestyle we always encourage them to exercise, even if it’s just to walk for half an hour every day (you don’t need to commit to running a marathon!). Exercise can also stimulate the cognitive function of the brain which helps concentration and learning. There are so many things going on in the world of glaucoma at the moment: investigating better treatment pathways, new surgical techniques and improved understanding of how glaucoma affects individuals differently. Very exciting times ahead! News Spring 2019 9
News
Campaign News #1
W
World Glaucoma Week
10 - 16 March 2019
We are delighted to have teamed up Worried about your vision?
with pharma company Santen to The answer’s clear
launch an engaging digital quiz for
World Glaucoma Week and beyond.
The quiz uses manipulated images to
show how glaucoma damage affects
sight, and the call to action is to have
a regular eye health check.
Our Development Managers
delivered patient talks, exhibitions
Image courtesy of R&J Moore Opticians, Sandwich
and events in Scotland, Wales and Glaucoma steals sight and can blind
England, and the week ended with Book an eye test today
our Annual Lectures in
London on 15 March. See our
For support and advice call our glaucoma helpline
01233 64 81 70
website or social media for details of
www.iga.org.uk
the quiz and other activities.
Charity registered in England and Wales No 274681 and in Scotland No SC041550
Visit www.worldglaucomaweek.org
10 News Spring 2019News
Campaign News #2
Don’t stop your drops this Ramadan
saving sight with the Muslim Council of Britain
Throughout the month of Ramadan, Muslims fast during daylight hours abstaining
from eating or drinking between sunrise and sunset. Many Muslims with glaucoma are
concerned taking eye drops constitutes a breaking of the fast, in particular due to the
draining of excess medication through the tear duct and down the back of the throat.
Anecdotal evidence indicates some people then stop using the drops completely when
they don’t perceive any change to their sight. However, significant and permanent loss
of vision can occur very quickly if an individual stops using their drops.
Last year for the first time, we engaged with the Muslim Council of Britain (MCB)
to advise Muslims with glaucoma to continue taking their drops throughout the month.
The message was very straightforward:
1. Do not stop eye drops during Ramadan
- all Islamic Schools of Thought support this
2. If in doubt, use morning drops at Suhoor (before sunrise)
and evening drops at Iftar (after night fall)
3. Try practising punctual occlusion following instillation of drops
This campaign was so successful it caught us by surprise, with an estimated audience of
over 600 million! (Mostly courtesy of an article on the BBC News website.) The support
of the MCB was crucial in providing us with the religious credibility we needed for the
message to resonate in Muslim communities.
News Spring 2019 11News
This year we’re planning on going bigger and better…
with a campaign during the lead-up to Ramadan and throughout the month, which starts
on May 6. We plan to use a number of different voices, for example an ophthalmologist,
an Imam and a Muslim glaucoma patient. Each will have a different story to tell about the
importance of taking glaucoma eye drops throughout Ramadan, although the key message
is staying the same. We hope the MCB will help us reach out to wide audiences by
sending our materials in the languages most commonly spoken by British Muslims, to a
large proportion of the mosques and other Muslim organisations in the UK.
As most Muslims in the UK are of South Asian or African origin, they are at a higher risk
of sight loss due to glaucoma. The prevalence of angle-closure glaucoma is higher in
Indian, Pakistani and Bangladeshi populations.
Glaucoma patients of African origin tend to develop open-angle glaucoma at a younger
age, and progression tends to be more rapid. Therefore, adherence to eye drops is
especially important amongst these groups.
We would like to thank the MCB and other partners, in particular Professor
Ejaz Ansari, Consultant Ophthalmic Surgeon at Maidstone and Tunbridge
Wells NHS Trust, for their help with this important work.
In 2018 the Academy of Medical Royal Colleges took up the issue of
reported cases of individuals being denied insurance cover or charged
higher premiums for travel insurance because of their participation in
a clinical trial. The AMRC wrote to the Association of British Insurers
(ABI) and met with them in January, and we’re pleased to say that the
ABI agreed a statement making clear that people should not be
refused cover or charged increased premiums solely for participation
in a trial although a pre-existing condition may affect the premium.
At the IGA we are not aware of any cases of this happening, but if
you do come across instances where an individual is refused cover
or charged more simply because of participation in a trial (as opposed
to the originating condition) do please let us know and we will raise it
with the ABI.
12 News Spring 2019News Campaign News #3 Glaucoma Awareness Week 17 - 23 June 2019 With summer firmly in mind one of our key themes for this year will be how to manage the challenges of travelling with eye drops over the holiday season. We’ll build on the work done in Ramadan and raise awareness of how to keep drops cool, when to take your eye drops in different time zones, and the importance of sticking with your treatment while away. As usual we’ll be sending out hundreds of free awareness raising resource packs to eye clinics and eye health professionals across the UK. If you would like to receive Awareness Week materials please just email marketing@iga.org.uk or call us on 01233 64 81 64. See the light: Improving capacity in NHS eye care in England All-Party Parliamentary Group on Eye Health and Visual Impairment. The IGA’s patient representative to the APPG, Chris Wall, brings us news of progress to date: “In September 2017, I joined the Expert Advisory Group for an All Party Parliamentary Group (APPG) as a patient rep, examining ways to improve capacity in NHS eye care in England, including the impact of appointment delays on patients’ sight. In January 2018 I joined three other patients, two ophthalmologists and a hospital optometrist in giving evidence to the Parliamentary Group – a similar event had taken place earlier with other patients and professionals. The importance of, and the case for improving NHS eye care, could not have been more clearly set out by all speakers. In June 2018 the Report was launched at a Parliamentary reception, and received favourable coverage in the press. “Since then, despite the attempts of several members of the Expert Advisory Group and the RNIB secretariat, including meetings with NHS England and Department of Health and Social Care (DHSC) civil servants, the impact of the Report has been disappointingly hard to detect. No doubt this is in some part owing to the dominance of Brexit-related matters across the political scene, but it is also likely to relate to the low profile of eye care, ophthalmology and the prevention of avoidable blindness at all levels in the NHS hierarchy. News Spring 2019 13
News “For those of us who recognise the value of even a minimal amount of sight, it is hard to understand how 20 people a month losing their sight for lack of NHS capacity does not cause sleepless nights for NHS managers and indeed MPs, but seemingly it does not. “There has been some recognition that the new ophthalmology tariffs, which are a crude instrument at the best of times, may have affected clinical prioritisation but there is still a conviction that patients are not being discharged appropriately and the tariff is an antidote to that. The NHS Long-Term Plan which came out in January has signalled a move towards Integrated Care Systems and less differentiated budgets, so it remains to be seen what will happen to the ophthalmology tariff in the interim. “While the Plan has raised important issues such as the need to improve maternity care, mental health services and eye care for people with learning disabilities, what is clear is that eye health in general is not one of the priorities. There is mention of maintaining short waits for cataract which is clearly important and which we welcome. However it is not clear what this might mean for other eye conditions which are not so easily treatable and for which, unlike cataract, sight cannot be restored once lost. “Apparently in spring 2019 there is a planned reunion for those who gave evidence to the APPG, at which DHSC and NHS England’s draft response will be shared, prior to an official response being published in May or June 2019. There is clearly still much for which to fight.” Chris Wall In February the IGA responded to another NHS consultation on tariffs, this one asking for views on reductions to tariffs for some implants and for procedures such as cataract plus valve surgery, or cataract plus tube. Here is our response: “The proposed tariff changes will impact upon all glaucoma implant surgery, and have the potential to impact most on patients with very complex high risk disease (such as those having Baerveldt and Ahmed valves implanted) in whom conventional surgery is high risk or likely to fail. This would impact negatively on patient quality of life, and there may also be indirect long term drug costs because patients may need to continue on a larger number of drops with potential risk of side effects… “… Current clinical practice is supported by NICE guidance and any changes which make combined cataract and glaucoma procedures less viable for hospital trusts will impact negatively on the patient experience. Eye surgery can be challenging and sometimes traumatic for patients, and facing two separate procedures rather than one will not be welcome. The changes are also likely to impact badly on capacity in eye clinics that are already seriously overcrowded, and it will make the implementation of improvement programmes even harder.” 14 News Spring 2019
News Spring 2019 15
News
UK Ophthalmology Alliance
The IGA is a member of the UK Ophthalmology Alliance (UKOA), established in 2017
as a membership group of UK NHS ophthalmology providers and stakeholders including
professional colleges, NHS programmes and eye care charities. Its ambition is to
“promote national standardisation and shared learning to deliver best practice in clinical
outcomes, patient standards and cost efficiency.” In plain English, that means working
together to make sure wherever you’re treated in the country, eye care services are
well run and you get the best possible quality of care.
One of their current initiatives - in which we are involved - is the development of
glaucoma patient standards. The aim of this project is to provide every single hospital eye
department with a document which provides recommendations on how best to manage:
• Co-ordinated care pathways, including referrals, monitoring and discharge, and
information sharing between health care professionals
• Understanding and supporting patients, including adaptations for individuals with
particular needs and how to provide the right information on the condition,
treatment and management
• Shared decision making between different professionals and the patient
• Active participation of patients in their own care, including managing compliance
and side effects
The guidance is only advisory, but we hope nonetheless hospitals will pick it up.
We contributed some excellent feedback from our readers’ panel and in particular
flagged the importance of patient education and support, which we judged had initially
been underrepresented. We also provided suggestions on the referral journey and
supporting patients with multiple eye conditions.
We hope this initiative will help relieve pressure on some ophthalmology departments,
while ensuring patients are provided with the information and guidance they need to
manage their condition.
Other projects being run within the UKOA include recommendations for a common
competency framework for eye care professionals, better use of data, e.g. use of virtual
clinics, and improved management of patient lists for clinic or surgery. For more
information on the UKOA, visit www.uk-oa.co.uk
16 News Spring 2019Research
IGA Research funding roundup
Our £25,000 2018 optometry research grant was awarded to Dr Tamsin Callaghan,
a dispensing optician and optometrist prior to completing her PhD at Cardiff University,
and now a lecturer at City, University of London. Tamsin’s research is entitled Tapping
into the 5,000 hours – how feasible is home monitoring of visual fields? and
she told us more about the study:
“People with glaucoma and those at risk of glaucoma require lifelong hospital review to
monitor their condition. This includes regular visual field (VF) tests in outpatient clinics
which is time-consuming, expensive and can be unpopular with patients.
“More effective management of these patients may delay disease progression and reduce
the economic burden of this disease. However this is challenging within the current
system and alternatives to monitoring need investigation.
“Patients spend only a few hours each year in
eye clinics but spend more than 5,000 waking
hours each year doing everything else. We
wondered whether glaucoma patients could
self-monitor their visual field at home between
clinic visits, and it’s this question that is
explored in this study, the first to investigate
the monitoring of VFs in the home.
“Home monitoring is increasingly popular
in healthcare, and it’s already commonly
used for blood pressure and diabetes
monitoring. Advances in portable technology allow vision testing in unconventional
settings and our new method of assessing VFs - the Eyecatcher visual field test - uses an
inexpensive tablet device to allow people to carry out VFs in their own homes. It is the
first home-monitoring programme to use eye and head movement, designed to assess
and encourage steady eye positioning when patients are not being supervised in a
hospital or research setting.
“20 people with moderate glaucoma in at least one eye will be first assessed at City,
University of London, using the standard visual field test: the Humphrey Field Analyser
test. All participants will receive instructions on how to use the Eyecatcher test and half
of the group will also have an additional training session. All participants will then be
issued with the Eyecatcher tablet and asked to monitor their VFs on both eyes at home
once a month for six months.
News Spring 2019 17Research
“Using the front facing camera of the device, participants’ faces will be photographed at
set times during each field test, with the data used to assess the Eyecatcher’s reliability
and participants’ movements.
“When home-monitoring is finished, participants will return for a final assessment at
City University, and carry out a final Humphrey Field Analyser test. The Eyecatcher VF
results will be compared to the Humphrey results.”
We asked what level of technical ability the participants would need in order to take
part – would the trial be limited to those people who are confident using computers
and tablets? “Hopefully no, although it’ll be interesting to test this. It’s very easy; it’s a
case of turning it on and pressing a button then following the instructions. So you don’t
need a huge degree of digital literacy to do it, but we understand this may be a perceived
barrier, and it’ll be interesting to see if that’s the case. Most of our patients are
increasingly using tablets and iPads at home so they are maybe more used to the
technology than we realise.
“This trial will use just one type of device and participants will be given a simple tablet to
do the tests on, but the eventual aim is to develop a model that can be used on many
different types of device, the sort of thing patients might have at home.”
We know from IGA member
feedback that many of you have
struggled taking VF tests
in optician and hospital premises
because of distractions like noise
and interruption, and we
wondered whether the trial had
ways of accounting for any
unexpected variables in peoples’
home environment that might
affect the results. “If for example
someone didn’t perform the test well because they were interrupted by the phone
ringing, the extra data and photos provided by the Eyecatcher should help the
researchers understand that. And because we’re doing a series of tests we can average
the results, so if there are four good measures and two not so good this would be
interesting too. Patients normally take just one Humphrey test a year, and there’s always
chance factors like tiredness and background distractions could affect that annual test."
We asked whether there was a chance people might become ‘hooked’ and do the test
more often, introducing a learning effect which could improve performance? “A previous
18 News Spring 2019Research literature review of research on home testing in diabetes and blood pressure didn’t reveal any information to suggest this happened, and discussions with glaucoma patients led researchers to think this wouldn’t be a major factor, but they appreciate it is a possibility. Feedback will be collected from participants on their home-monitoring experience to identify any difficulties, potential improvements, and to compare the home VF test experience with the Humphrey. The effect of the training support package on participants’ compliance will be studied and all feedback will be analysed to identify any trends or themes.” If home VF monitoring for glaucoma is feasible, this could have significant, far-reaching impact for those with glaucoma and clinicians. Hospital glaucoma clinics would benefit from shorter eye clinic appointments, reducing costs and waiting lists and allowing at-risk patients to be seen more quickly. Most importantly, people with glaucoma would benefit from increased VF monitoring, potentially detecting VF progression at an earlier stage. Tamsin and her colleagues would be keen to hear from any IGA members who might be interested in joining the trial. Contact details: Dr Tamsin Callaghan: tamsin.callaghan@city.ac.uk Tel 0207 04 08 345 Dr Peter Campbell: peter.campbell@city.ac.uk Tel 0207 04 03 339 News Spring 2019 19
Research grants
Ophthalmology Research Grants
In the last edition of IGA News we reported that Prof Colin Willoughby from
Ulster University had been awarded our 2018 ophthalmology research grant, worth
£99,600. Although the IGA funds the whole of these annual grants, we work in
partnership with The Royal College of Ophthalmologists to promote and
administer the funding.
It’s an extremely beneficial partnership, and we are grateful to our colleagues at the
College for their permission to use this recent Q&A interview with Colin, which also
appeared in the January edition of their membership magazine, College News.
Can you very briefly outline the scope of your research?
The proposal looks at primary open angle glaucoma and raised intraocular pressure,
specifically, the influence of the protein NOX4 on fibrosis and scarring in the trabecular
meshwork and Tenon fibroblasts, and how this can be regulated. With further
investigation, the findings could have implications for the medical and surgical
treatment of glaucoma.
It’s still very early days, but how do you see the initial six-12 months
and beyond of the project unfolding?
The proposal supports a three-year PhD studentship. The project is based on cell
samples from normal and glaucoma patients which will be examined in a laboratory and
at this stage the study is purely pre-clinical. The data generated in the initial three-year
period could however ultimately be developed into a therapy which could be used in a
patient focused trial.
The IGA are very much interested in
patient outreach and advocacy so we This is important research
imagine there will be interest from the in an exciting area, but it is
glaucoma patient community. Interest still early days and there is
from the scientific community will most much more work required
likely come later, and there is certainly to translate laboratory
potential for high impact at a later date.
findings into new treatments
News Spring 2019 21Research grants
What do you think the importance
It is important the of the IGA award being offered in
partnership with The Royal College
Royal College promotes
of Ophthalmologists is?
and nurtures academic
ophthalmology through these At the moment securing research funding is
challenging in the UK. Some of the funding
awards for future generations comes from government agencies and
of ophthalmologists research councils, however, a significant
amount of the funding for entry-level
projects comes from research charities.
The IGA is a significant funder of research into glaucoma and their support enables
early-entry innovative research, which might not necessarily attract larger research
council funding, to get off the ground. They are a vital link between this initial research
and the later transition to larger scale trials. The IGA is also a specifically patient
focused charity and as such involves patients directly, ensuring the research is
relevant.
They also perform a great deal of advocacy in terms of the profile of glaucoma in visual
health in general, beyond just ophthalmology. They deserve the support and collaboration
of the ophthalmic community.
As a fairly large project are there any contributors or collaborators
you would like to mention?
One of the people who helped me to establish this research is Dr Neeru Vallabh,
who is an ophthalmic trainee in Liverpool. She was in fact partly funded by the IGA
among others to undertake her PhD research into mitochondrial dysfunction in
glaucoma, and was instrumental in patient recruitment, sample collection and providing
a direct link with patients.
My research group at Ulster University includes Dr Karen Lester, a research associate,
who has been key in developing and supporting glaucoma related research. I also have
some key co-workers in Ulster University including Dr Andrew Nesbit, a scientist
with an interest in molecular biology, and Dr Declan McKenna who works on
microRNA biology. I have another long-term collaborator at Queen’s University Belfast,
Dr David Simpson, whose expertise in gene sequencing has been vital to a number of
glaucoma-related studies.
22 News Spring 2019Research grants
Do you have any advice for anyone
considering applying for the next round
of IGA and RCOphth funding? I know
the scale of the grant and application
process can seem daunting and put
off some potential candidates.
It is difficult for junior ophthalmologists to
get involved in academic research, and
some of these awards could facilitate
junior ophthalmologists who have an
interest in research.
These grants by their very nature are
applicable to individuals wanting to develop
Professor Colin Willoughby a research career or experience, especially
if partnered with a more experienced or
senior individual; they have quite a broad portfolio in terms of what they fund, and it is
not purely laboratory-based research.
The value of these awards is that they offer opportunities to develop research skills and a
portfolio. They are flexible, multidisciplinary, and multi-faceted in terms of the projects
they fund, and that is the beauty of them.
Any other thoughts you’d like to add?
This is important research in an exciting area, but it is still early days and there is much
more work required to translate laboratory findings into new treatments. It is important
the Royal College promotes and nurtures academic ophthalmology through these awards
for future generations of ophthalmologists. These sorts of projects are vital for the
ophthalmic research community.
News Spring 2019 23Research grants UK & Éire Glaucoma Society Research Award 2018 Our final research awards of 2018 were made in partnership with the UK & Éire Glaucoma Society, or UKÉGS. £60,000 was available, with £50,000 coming from the IGA and £10,000 contributed by UKÉGS from the profits made by last December’s successful conference, organised by the IGA. Two grants were announced at the meeting in London in early December, the first for £30,300 went to Colin Willoughby, for ‘The role of transforming growth factor beta-1 in glaucoma: therapeutic opportunities?’ Colin told us “This project will provide significant insight into the molecular changes in the trabecular meshwork that cause glaucoma and drive the development of new therapeutic approaches for glaucoma. Pilot work has identified small, naturally occurring regulatory genes called microRNAs that can be manipulated therapeutically. Basically, the levels of ‘good’ microRNAs will be increased, and the levels of ‘bad’ microRNAs will be reduced in order to develop a new potential treatment for fibrosis in glaucoma. “The data from the project will allow the development of a new class of disease-modifying therapeutics that will have direct translation benefits to the clinical treatment of patients.” The second grant – of £30,000 - was awarded to Professor Colm O’Brien from Mater Misericordiae University Hospital in Dublin for a study ‘Investigating the Role of the Proto-Oncogene c-Met and the PI3K/mTOR Signalling Pathway in Lamina Cribrosa Fibrosis in Glaucoma.’ Professor O’Brien summarised the study “Glaucoma patients are prescribed eye drops to lower the eye pressure in the eye that causes damage to the optic nerve. This damage then leads to loss of vision. Eye drops are effective, but unfortunately, many patients continue to lose sight. Therefore there’s an urgent need to identify new treatments to stop the ongoing optic nerve damage. This research will be looking at molecules that have been found to stop glaucoma progressing. Through these molecules, a therapeutic approach will be developed to stop damage to the optic nerve and protect further sight loss.” 24 News Spring 2019
Talking glaucoma Talking Glaucoma #1 EyeWatch glaucoma implants – the world’s first adjustable drainage device Dr Emma Linton (EyeWatch Co-investigator) and Mr Leon Au (EyeWatch Principal Investigator) share news of this current study. Glaucoma is a disease that damages the optic nerve in the back of the eye which can cause loss of vision. Early on in the disease patients may not have any symptoms, so the diagnosis is often made by an optician or an eye doctor. Often, glaucoma is associated with a raised pressure inside the eye. Current treatments aim to reduce eye pressure to slow down damage to the optic nerve and stabilize vision. In the many years of glaucoma drainage surgery, we have never had a device that allows flow adjustment – until now. Treatment to reduce pressure inside the eye may include eye drops, laser or surgery. Initially, when the condition is mild, eye drops are often sufficient in controlling the pressure. When drops fail we often turn to laser treatment or some of the new News Spring 2019 25
Talking glaucoma
minimally-invasive glaucoma implants. Most of
In the many years of these procedures aim to restore the natural
glaucoma drainage surgery, drainage in the eye. However when the
condition is more advanced, or the pressure
we have never had a device
remains uncontrolled, a bypass drainage
that allows flow adjustment operation is often required. Trabeculectomy
– until now has been the gold-standard drainage operation
for 50 years. It aims to create a new drainage
outlet on the top of the eye and significantly
lower eye pressure. Although the success of trabeculectomy is high, some will
unfortunately fail. This is often due to an excessive amount of scarring on the eye,
blocking the trabeculectomy from draining. There are also other types of secondary
glaucoma where trabeculectomies are thought to be unsuitable. In these difficult cases,
we often turn to glaucoma tube surgery.
Glaucoma tube surgery has been shown clinically and in research trials to be effective in
controlling pressure in the eyes where previous trabeculectomy has failed. Although
there are different types of glaucoma tubes, most involve inserting a silicone tube into the
water chamber of the eye. Fluid is then drained along this tube and eventually exits near
the back of the eye. The design of the glaucoma tube enables it to combat scarring better
so it is often used in more complicated cases or secondary glaucoma.
One of the major criticisms of our current glaucoma drainage device is the “one size fit
all” concept. The design of the device allows sufficient drainage in the majority of patients
but not in everyone. In some cases the drainage may not be sufficient. More importantly
it can drain too much, causing low eye pressure, which can be damaging to the eyesight.
In the many years of glaucoma drainage surgery, we have never had a device that allows
flow adjustment - until now.
The EyeWatch drainage implant is a new surgical device manufactured by Rheon Medical,
Switzerland. It is the first ever surgical option for glaucoma that allows flow from the eye
to be adjusted in clinic following the operation. The EyeWatch is a very small device
buried in the white coat of the eye and cannot be seen. It diverts fluid out of the eye via
a small tube surrounded by a magnetic compressive wheel with ruby bearings (much like
the inside of a Swiss watch). With a small, specialized EyeWatch pen held over the
magnet the wheel can be turned and the flow through the tube can be increased or
decreased, much like turning a tap on and off.
26 News Spring 2019Talking glaucoma This can be repeated where necessary until the pressure stabilizes at the desired amount. This can save patients from having to undergo multiple operations or uncomfortable procedures in the clinic to optimize their eye pressure. More importantly it promises individual tailored drainage for each patient, potentially eliminating the complication of low eye pressure. If the pressure goes too low, one justs “turn the tap down” a bit in clinic by manipulating the EyeWatch with a magnet. Although the adjustability is the key difference to our current glaucoma tube, there are other improvements made too. For example the material used in the EyeWatch is more flexible which should be more bio-compatible to the eye, causing less discomfort. The size of the EyeWatch tube is also a bit smaller and angled slightly to better suit the shape of the eye. This, so far, has been shown to cause less wear and tear on the surrounding structures of the eye. Currently EyeWatch is undergoing clinical trial only in Switzerland, Greece and the UK. The trial started in the UK over six months ago and is only performed in Manchester Royal Eye Hospital and St Thomas’ Hospital in London. We are only including patients who have had previous failed drainage operations in the study, and there are many other inclusion and exclusion criteria too. The safety and efficacy of such a new device needs to be carefully evaluated before commercial licensing can occur. So far, nearly 20 patients in the UK and over 50 patients worldwide with advanced glaucoma have had the EyeWatch device implanted. The study recruitment is due to end in the middle of 2019 with an 18-month follow-up. Results so far are promising but we are still very early on in this exciting journey. The EyeWatch, for us, has been a giant step forward in the field of glaucoma drainage surgery. Are we likely to see more adjustable glaucoma drainage device in the years to come? You bet. Will the EyeWatch be THE ultimate glaucoma surgery? I doubt it. There is always room for improvement and technology is moving fast. We as glaucoma specialists are so excited to see the current high level of financial and research investment in this field and this can only lead to better patient care for the future. News Spring 2019 27
Talking glaucoma
Talking Glaucoma #2
Aye, eye: Modernising glaucoma care in Scotland
Health care in Scotland is a devolved issue, meaning the Scottish government is
responsible for funding and managing services. As a result, things happen differently
North of the Border.
In 2008, free eye examinations were introduced in
Scotland. A decade later, a Scottish Community
Eye-care Review is considering the impact of an
ageing population, improved treatment options and Every two years:
moving some eye services from a hospital to a Everyone in
community setting. This has included a number of Scotland is entitled
running focus groups for service users (including to at least one
some of our own IGA members) to provide their free eye test,
experiences of eye care services in Scotland. The every two years
review highlighted good practice across different
health boards and recommended schemes to help
reduce geographical differences in services.
A number of changes have taken place for glaucoma patients over the last
10 years, including:
• Optometrists refining their referrals through supplementary eye examinations,
meaning only those patients who need to be seen in the hospital are referred
• Hospitals have been actively discharging patients, e.g. those without glaucoma
• Innovative delivery models including virtual clinics, offering high standards of
hospital-based assessment and monitoring while increasing throughput of patients
• Accreditation of community optometrists for stable glaucoma patients. This provides
patients with the reassurance regarding the quality of care, while reducing hospital
visits and providing more capacity in hospitals for higher-risk patients.
28 News Spring 2019Talking glaucoma
Additionally, changes to the General Ophthalmic
Services in October 2018 have granted
optometrists more freedom to make decisions
based on individual patient need.
2.2 million:
the number of eye
These decisions must be made based on SIGN examinations
(the Scottish equivalent of NICE) evidence-based performed by
guidance regarding referral and safe discharge. Scotland-based
Most notably, patients with stable glaucoma, a optometrists
family history of glaucoma or with ocular in 2017/18
hypertension only need to be reviewed every two
years instead of annually.
Patients who are judged to be of greater risk can be seen more frequently. This initiative
is supported by new requirements for optometrists in Scotland undertaking annual
mandatory training with NHS Education for Scotland.
Wider initiatives in Scottish health will also
impact eye care services, including the
3rd: procurement of a nationwide ophthalmology
glaucoma was the Electronic Patient Record (EPR).
third most common
The record will provide clinicians with all a
issue that resulted patient’s results, images and plots in an easily
in a risk of sight loss accessible format. Access within the
or blindness in community and hospitals will enable patients
Scotland in 2015 to be treated, monitored and assessed more
efficiently, as important healthcare information
like glaucoma treatment history will be
available to all relevant professionals.
With prevalence of glaucoma across the UK expected to increase by 44 per cent over
the next 20 years, we hope the changes being initiated now will help make Scotland’s
eye care services fit for the future.
News Spring 2019 29Talking glaucoma
Pachymeters, used to
measure the thickness
Image courtesy of Carleton Optical Ltd
of the cornea accurately,
were provided by the
Scottish government
to every optometry
practice in
Scotland in 2016
30 News Spring 2019Experience Charles Bonnet Syndrome Charles Bonnet Syndrome (CBS) is a condition affecting people with significant sight loss due to glaucoma and other eye conditions. Judith Potts, founder of the CBS support charity Esme’s Umbrella, told us how she came to set up the charity, and how it helps people with sight loss. My mother – Esme - was an independent 92 year-old, living on her own and coping admirably. Following a late diagnosis of glaucoma, she was given an incredibly complex schedule of different eye drops but her sight gradually deteriorated. She adapted and adjusted in the most remarkable way, still completing the Telegraph cryptic crossword every day. However, something else was lurking – the vivid, silent, visual hallucinations that make up Charles Bonnet Syndrome. It took many months of anguish before Esme, a proud, independent lady, confided in me about the faceless people sitting on her sofa, the gargoyle-like creature who jumped from table to chair and the tear-stained Victorian street-child who followed her everywhere – and how this left her disoriented, frightened and distressed. I could not imagine what was wrong with her. Her mind seemed as focused and active as ever, but she was clearly tormented by what she was seeing. With a huge piece of luck, at around that time I read a tiny piece in the health pages of a newspaper which could have been written by my mother. Here was the answer – the hallucinations were called Charles Bonnet Syndrome and they were caused by her loss of sight. Feeling greatly relieved this was not a mental health issue, I rang Esme’s ophthalmologist. To my great surprise he refused to discuss Charles Bonnet Syndrome. I tried the GP and the optometrist, but News Spring 2019 31
Experience
neither had heard of the condition. Eventually, I found Dr Dominic Ffytche at King’s
College Hospital, London, who is the globally-acknowledged expert in CBS, and now
my medical adviser. Dominic explained that as sight diminishes, the messages that travel
from the retina to the visual cortex in the brain slow or stop entirely. But the brain does
not. It fires up and creates its own images. The visual hallucinations of Charles Bonnet
Syndrome are entirely silent and no other sense is involved. What is seen depends on
which part of the brain is firing at that moment.
CBS can occur in anyone of any age who has lost over 60 per cent of their sight. The
loss can come through glaucoma or any of the other eye diseases, or through stroke,
cancer, diabetes or any other health condition or accident that damages the optic
nerve. There are no specialists and no reliable, side-effect-free medication to alleviate
the hallucinations.
Realising there was a need to raise awareness of this condition which so negatively affects
lives, I launched Esme’s Umbrella in November 2015 at the House of Commons. My aim
was – and still is – to persuade ophthalmologists it is crucial for patients to be warned
about the condition. Only 17 per cent of patients with significant visual loss receive a
warning from their ophthalmologist, and this is shocking. Forewarned is forearmed: if a
medieval army marches
through the garden, if the
bedroom morphs into a
fast-flowing river or is
invaded by a weary-looking
second world war pilot or a
snarling tiger, it makes it
marginally easier to cope if
CBS has been mentioned by
the ophthalmologist.
CBS can cause severe distress. People with multiple hallucinations find it
impossible to distinguish what is real and what is not and can become
housebound. Others, repulsed by the worms and slugs they see on their food
or in their drink, stop eating and drinking. A few, who find the hallucinations
so terrifying or inappropriate, consider suicide. Young professionals tell me
their hallucinations disrupt their concentration at meetings and turn already
difficult journeys on public transport into a real nightmare.
At any age, bones can be broken trying to avoid the unexpected appearance of furniture,
fire or strange animals.
32 News Spring 2019Experience
Misdiagnosis through lack of awareness of CBS can follow and - as happens all too often -
people in an older age group can find themselves ushered down the mental health route,
sometimes on a one-way ticket with the word ‘dementia’ hanging in the air.
We have no data on the prevalence of CBS. This is partly because many people living
with the condition are too frightened the hallucinations are due to a mental health issue
or too embarrassed about what they are seeing, to confide in anyone. However, Dominic
estimates there are one million people living with CBS in the UK.
Thanks to the support of the charity sector, Esme’s Umbrella now has a researcher –
Dr Greg Elder - at Newcastle University, who is comparing the brains of people with
sight loss and CBS with those of people with sight loss who do not develop the
condition. If we can identify the difference, it may lead to a non-medication,
non-invasive treatment.
One of the glaucoma consultants at Moorfields is going to do some grass roots research
for me about how many of his patients have CBS. Data is lacking, and we need that if
we are going to persuade anyone to fund more research.
Last November, to coincide with Charles Bonnet Syndrome Awareness Day, I hosted
the world’s first CBS Patient Day at Moorfields Eye Hospital. Supported by the IGA
and other national eye charities, the audience heard from patients, researchers, me and
a consultant ophthalmologist. The event resulted in a call for specialist CBS nurses to
whom patients can be referred; a tick box to be added to the CVI form to show that
the ophthalmologist has warned the patient about CBS; a further programme of support
groups; and the creation of a proper pathway for diagnosis, treatment and support.
I watched powerlessly as glaucoma sight loss and the torment of CBS took its toll on
Esme. Her life was dramatically and negatively altered by what Charles Bonnet described
as the ‘theatre of the mind.’ If you have glaucoma and are seeing things which should not
be there, please confide in someone.”
For help
• call Sightline on 01233 64 81 70
• go to www.charlesbonnetsyndrome.uk
• Call Judith’s Esme’s Umbrella helpline
(answered on her behalf by the eye health team at the RNIB) on 0207 39 13 299
• Or email Judith at esmesumbrella@gmail.com
News Spring 2019 33You can also read

















































