Improving tuberculosis prevention in South Africa - deNovo ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Leader in digital CPD
Earn 3
for Southern African
free CEUs Respiratory
healthcare professionals
Improving tuberculosis
prevention in South Africa
Learning objectives
You will learn:
Dr Jeremy Nel • The South African burden of TB infection and who is at risk for developing active TB disease
Head of Infectious Diseases
Helen Joseph Hospital and • The evidence and guidelines for initiating isoniazid as TB preventive therapy
Wits University • The evidence and guidelines for the use of cotrimoxazole in advanced HIV disease
• The advantages of a fixed-dose combination of therapies for preventing TB and other
opportunistic infections in people living with HIV.
Introduction
South Africa has high prevalence of Mycobacterium tuberculosis infection (TBI),
one of the highest in the world in terms of real numbers and rates of infection.
A TBI prevalence of 89% in gold miners has previously been demonstrated. Young
children, adolescents, household contacts of cases of active TB disease, people living
with HIV, and health care workers are also particularly at high risk of TB infection.
Dr Francesca Conradie The prevalence and annual risk of TBI is high in South African urban populations
Clinical HIV Research Unit (34.3% and 3.1% respectively), especially in men, but independent of HIV infection.1,2
University of the
Witwatersrand
Johannesburg
Professor Mahomed Yunus
Suleman Moosa
Associate Professor
Chief Specialist
Head of Infectious Diseases
Unit
University of KwaZulu-Natal
This report was made possible
© shutterstock/1506001223
by an unrestricted educational
grant from Cipla. The content
of the report is independent of
the sponsor.
© 2021 deNovo Medica JANUARY 2021 I 1
Improving tuberculosis prevention in South Africa
The World Health Organization’s (WHO) Global Tuberculosis Report 2020 demonstrates, in
2019, a total TB incidence of 360 000 South Africans with 209 000 also being co-infected
with HIV.3 HIV infection increases the risk of TB infection by 80- to 500-fold; the lifetime risk
of TB infection is 50% if HIV-positive as compared to a 10% lifetime risk in the HIV-negative
population. TB mortality is higher in the HIV-positive population (62 per 100 000) as compared
to those who are HIV-negative (38 per 100 000).3
TB preventive treatment (TPT) is a community wide intervention in the South African context.
There is an individual benefit of preventing TB infection or progression to active TB disease,
with the additional potential for community benefit through reducing TB transmission. In
2019, TPT was initiated in 69% of HIV-positive people newly enrolled in care and 56% of
children aged younger than five years with household contacts of active TB disease. While
these figures represent great improvements in access to TPT over recent years, South Africa
must do better. The prevention of TB and other opportunistic infections, in the case of people
While these living with advanced HIV infection, saves lives.2,3
figures
represent great
improvements Isoniazid for the prevention of TB infection
in access to
TPT over recent
years, South What is the evidence for the use of isoniazid as TPT?
Africa must Isoniazid TPT helps to prevent progression The TEMPRANO trial randomised HIV-
do better. The to active TB disease irrespective of HIV positive patients initiating ART at any
infection status. A 2010 Cochrane review of CD4 count to isoniazid TPT or no TPT for
prevention of isoniazid TPT in HIV-infected persons found six months. The primary end point was a
TB and other a lower incidence of active TB (RR 0.68, 95% composite of death from any cause, AIDS-
opportunistic CI 0.54 to 0.85). This benefit was more pro- defining disease, non–AIDS-defining cancer,
infections, in the nounced in individuals with a positive tuber- or non–AIDS-defining invasive bacterial
case of people culin skin test (TST) (RR 0.38, 95% CI 0.25 disease. After adjusting for ART strategy,
to 0.57) than in those who had a negative test baseline CD4 count and other key character-
living with (RR 0.89, 95% CI 0.64 to 1.24). Furthermore, istics, hazard ratio of death in patients who
advanced HIV a reduction in mortality with isoniazid mono- had isoniazid TPT as compared to no TPT
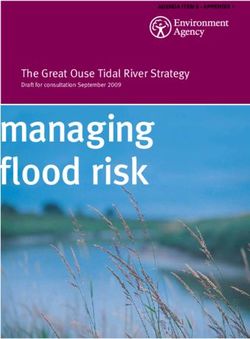
infection, saves therapy as compared to placebo was evident was 0.61 (CI 0.39-0.94) (Figure 1).5
lives among individuals with a positive TST (RR
0.74, 95% CI 0.55 to 1.00).4
15 No IPT 6.9% (95% CI 5.1–9.2)
IPT 4.1% (95% CI 2.9–5.7)
Cumulative probability of death (%)
Log rank p=0.039
10
5
0
0 1 2 3 4 5 6
Number at risk
No IPT 1 026 997 981 836 672 474 188
IPT 1 030 1 018 1 007 859 692 492 185
Figure 1. TEMPRANO isoniazid TPT vs placebo: Kaplan–Meier curves of 6-year probability of death5
2 I JANUARY 2021
Improving tuberculosis prevention in South Africa
What are the National Department of Health (NDoH) guidelines for TPT?
The South African state sector guidelines • Pregnant women with CD4 ≤350cell/mm3
recommend TPT of isoniazid 300mg daily, where active TB has been excluded (defer
together with pyridoxine 25mg daily, for 12 until after delivery in pregnant women
months for: with CD4 >350cell/mm3, due to a small
• All HIV-positive patients irrespective of risk of adverse pregnancy outcomes).
CD4 count and antiretroviral therapy • Children younger than five years of age,
(ART) status, but excluding those with: regardless of HIV status, who are contacts
» Confirmed or suspected active TB of active TB cases and those between
disease five and 15 years of age living with HIV
» Liver disease should receive and complete TPT for a
Remember that » Painful peripheral neuropathy duration of six months, as per the NDoH
HIV infection is » Alcohol abusers guidelines.
» Previous MDR- or XDR-TB.
an independent
risk factor for Why is pyridoxine recommended with isoniazid TPT?
the development Pyridoxine (vitamin B6) prevents isoniazid- infection is an independent risk factor for the
of peripheral induced neurological toxicities such as development of peripheral neuropathy.6
neuropathy peripheral neuropathy. Remember that HIV
What are the clinical considerations prior to initiating TPT in somebody
with TBI?
Most importantly, rule out TB disease. Take treatment for TB disease. If previously treated
a history (Box 1).7 Although TB is predomi- for TB disease, was the TB drug-sensitive or
nantly a lung disease, it can also present as drug-resistant? This will make a difference to
extrapulmonary TB and the easiest way to the recommended TPT in the patient, as there
find this is by physical examination, pay- are drugs other than isoniazid that can be
ing attention to lymph nodes in the neck used. Determine current and previous drug
and axilla (Table 1). If necessary, do a chest therapy. Assess risks and benefits of initiating
X-ray; sometimes TB changes can be seen on TPT in the patient.8
the X-ray even prior to the development of
Most symptoms (Table 2).8 If the TB screening is negative, initiate ART
importantly, rule and TPT at the same time and if needed,
out TB disease Find out if the patient has previously had cotrimoxazole.
Box 1. Patient history to exclude TB disease7
For each health care visit for all people living with HIV, ask:
1. Are you coughing?
In the patient with HIV, a cough of even one day’s duration should be investigated
2. Are you sweating at night?
Drenching night sweats
3. Are you losing weight?
EARN FREE Weight loss that cannot be explained by diet or lifestyle change
CPD POINTS 4. Do you have a fever?
Join our CPD community at What is the value of asking these four questions? Meta-analysis of observational studies has indicated that
absence of all of current cough, fever, night sweats, and weight loss can identify a subset of people living
www.denovomedica.com
with HIV who have a very low probability of having TB disease.7 These four symptoms represent a simple,
and start to earn today! standardised TB screening rule for resource-constrained settings that will adequately separate patients into
two groups:
• TB is reliably excluded, and TPT and ART can be initiated
• Further investigation for TB disease is required.
JANUARY 2021 I 3Improving tuberculosis prevention in South Africa
Table 1. Common forms of Table 2. Radiological manifestations of
extrapulmonary TB TB in HIV infection
• Lymph node disease • Early HIV disease
– Peripheral: cervical > axillary > inguinal – Predominantly upper lobe involvement
– Central: mediastinal > hilar, intra-abdominal – Breakdown and cavitations
• Disseminated disease – Pleural effusion
• Serosal: pleural, pericardial, peritoneal • Advanced HIV disease
• CNS: meningitis, tuberculoma – Intrathoracic lymphadenopathy
• Bone and joint – Predominantly lower/middle lobe infiltrates
• Genitourinary. – Vague nodular infiltrates
– Pleural/pericardial involvement.
What are the current recommendations regarding testing for TB infection?
Testing for TBI prior to initiating TPT is appropriate medicines, making the patient
largely falling away. The Mantoux TST is less likely to be linked to care. Interferon-
often out of stock, requires two visits to gamma release assays (IGRA) are expensive
the clinic, and often delays the initiation of and not available in the state sector.
Doctor Conradie
emphasises Who is at risk for developing TB disease?
the need in the Those at high risk for developing TB disease
coming months fall into two categories, those who have an Table 3. Increased risk of progression
increased likelihood of exposure to persons from TBI to TB disease9
to pay specific
with TB disease and those with clinical condi-
attention to • HIV-infected persons: 19 times more likely
tions that increase their risk of progressing
children under from TBI to TB disease (Table 3).9 • Those with a history of prior untreated TB or
the age of five fibrotic lesions on chest radiograph
years, as with Doctor Conradie emphasises the need in the • Children ≤5 years with a positive TST
• Underweight or malnourished persons
the COVID- coming months to pay specific attention to
• Substance abusers (such as smoking, alcohol
children under the age of five years, as with
19 lockdown abusers, or injection drug use)
the COVID-19 lockdown many will have had
many will have increased exposure to family or carers with
• Those with certain medical conditions such as:
had increased – Silicosis
TB disease. She also warns that the economic – Diabetes mellitus
exposure to effects of lockdown will see an increase in – Chronic renal failure or on haemodialysis
family or carers underweight and malnourished people, with a – Solid organ transplantation (e.g., heart,
consequential increased risk of progression to
with TB disease kidney)
TB disease.8 – Carcinoma of head or neck
– Gastrectomy or jejunoileal bypass.
Is the use of TPT a risk for the development of resistant TB?
If active TB is misdiagnosed during the 1951 and 2005 concluded that it was not
screening process and the bacterial load is associated with an increased risk of isonia-
significant, treatment with monotherapy zid resistance and that isoniazid resistance is
theoretically has the potential to generate much more likely to result from inadequate
drug resistance. Concern over potential drug treatment of active disease. Studies in South
resistance is one of the primary factors driv- African and Botswana have similarly shown
ing clinical inertia towards initiating TPT in no increased risk of isoniazid resistance when
high-risk individuals. A systematic review of used for TPT.10-13
studies of isoniazid TPT conducted between
4 I JANUARY 2021Improving tuberculosis prevention in South Africa
Cotrimoxazole for the prevention of opportunistic
infections
Cotrimoxazole (sulfamethoxazole/trimetho- cotrimoxazole prophylaxis should be initiated
prim) preventive therapy is a feasible, well and continued regardless of CD4 count or
tolerated and inexpensive intervention for WHO clinical stage.14
people living with HIV to reduce HIV-related
morbidity and mortality.13 The NDoH guidelines indicate cotrimox-
azole 160mg/800mg daily for use in WHO
The WHO 2016 guidelines recommend co- clinical stages 2, 3, and 4 and for those with
trimoxazole prophylaxis for adults (including CD4 200cells/
pregnant women) with: mm3, as measured at the routine CD4 count
• Severe or advanced HIV clinical disease performed at one year on ART, discontinue
(WHO stage 3 or 4) and/or prophylaxis. If the CD4 count was >200cells/
• CD4 count 14kg) Meta-analysis of randomised controlled malaria, isosporiasis, Toxoplasma gondii and
without signs trials and observational studies including other bacterial and non-viral opportunistic
of active TB cotrimoxazole prophylaxis and a comparator infections in HIV-infected patients with CD4
disease group in HIV-infected adults showed reduced 14kg) without signs of active TB disease,
EARN FREE cotrimoxazole prophylaxis. Benefits were using one tablet once daily for 12 months in
CPD POINTS maintained through 48 weeks (24% lower
rate), with a number-needed-to-treat of 29
adults and children ≥25kg, or half a tablet
once daily in younger children weighing 14kg
Join our CPD community at to prevent one death. Patients who received to 24.9kg. This co-formulation supports
www.denovomedica.com enhanced prophylaxis also had a significantly patient adherence to treatment by reducing
lower rate of hospitalisation, WHO stage 3 or pill burden and improving the quality of life
and start to earn today! 4 events, IRIS-compatible events, tuberculo- of people living with HIV. Improved adher-
sis, and cryptococcal and candida infections. ence reduces mortality and delays/prevents
There was no evidence of increased toxicity, the development of microbial resistance.
JANUARY 2021 I 5Improving tuberculosis prevention in South Africa
Key learnings
• South Africa has a high burden of TBI
• HIV infection increases the risk of TBI and progression to TB disease
• South African guidelines recommend 12 months of isoniazid TPT for all HIV-positive patients and for
childrenYou can also read