Update - CPD Accredited Sponsored in the interest of continued medical education - Medical Practice Consulting
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Infectious Diseases
Volume 7 No 3 September 2018
Update
CPD Accredited
Sponsored in the interest of continued medical education

Editorial board Editorial
Professor Charles Feldman Professor Charles Feldman MBBCh DSc PhD FRCP FCP (SA)
(Editor-in-chief) Professor of Pulmonology and Chief Physician
Professor of Pulmonology and Chief Physician Charlotte Maxeke Johannesburg Academic Hospital and Faculty of Health
Charlotte Maxeke Johannesburg Sciences
Academic Hospital and Faculty of Health University of the Witwatersrand, Johannesburg
Sciences
University of the Witwatersrand
Johannesburg his third edition of the journal for 2018 contains three interesting and
topical articles, the first relating to antibiotic susceptibility, the second
Professor Lucille Blumberg about acute pneumonia in children, and the third dealing with post-
Deputy Director at the National Institute for
Communicable Diseases, Johannesburg exposure prophylaxis for infectious diseases.
Associate Professor, University of the
Stellenbosch, Western Cape The first article is by Dr Chanel Kingsburgh, a consultant clinical microbiologist at
Ampath Laboratories in Centurion, and she discusses what antibiotic susceptibility
Dr Jennifer Coetzee testing is, how it’s done and what it means for the treating clinician. She ends the
Microbiologist
article by reminding us that the friendly microbiologist is always only a phone
National Reference Laboratory, Ampath
Pretoria call away for advice.
Dr Raymond Friedman The second article is by Prof Robin Green from the Department of Paediatrics
Ear, Nose and Throat Surgeon and Child Health of the University of Pretoria. He deals comprehensively with
Sandton Clinic, Johannesburg
the topic of acute pneumonia in children.
Professor Robin Green
Professor of Paediatrics The last article is by Dr Michelle Venter, an Infectious Diseases specialist from the
Dept of Paediatrics and Child Health Charlotte Maxeke Johannesburg Academic Hospital, who deals with the subject
University of Pretoria, Pretoria of post-exposure prophylaxis in infectious diseases.
Professor Shabir Madhi
Professor of Vaccinology As always, the journal would welcome any correspondence on any of the topics
University of the Witwatersrand covered, as well as suggestions for topics to be carried in future editions of the
Director, MRC Respiratory and Meningeal Journal.
Pathogens Research Unit
Chair in Vaccine Preventable Diseases,
DST/NRF SARChI
Professor Bruce Sparks
Department of Family Medicine
University of the Witwatersrand
Johannesburg
Professor Anton Stoltz
Subspecialist Adult Infectious Diseases
Division of Adult Infectious Diseases
University of Pretoria
In this issue:
Professor Francois Venter
Deputy Executive Director, Wits Reproductive Editorial Prof Charles Feldman 3
Health and HIV Institute (WRHI)
Associate Professor in the Department of Antibiotic susceptibility testing in the micro
Dr Chanel Kingsburgh 4
Medicine, University of the Witwatersrand lab “S, R or l”: What does it mean?
Head of Infectious Diseases, Charlotte
Maxeke Johannesburg Academic Hospital Acute pneumonia in children Prof Robin Green 7
Ex-president of the Southern African HIV
Clinicians Society Postexposure Prophylaxis in Infectious
Dr Michelle Venter 10
Diseases
Disclaimer.
The content contained in this publication contains medical or health sciences information and is intended for professional
use within the medical field. No suggested test or procedure should be carried out unless, in the reader’s judgement,
its risk is justified. Because of rapid advances in the medical sciences, we recommend that the independent verification
Production Editors: Ann Lake Publications of diagnoses and drug dosages should be made. Discussions views, and recommendations as to medical procedures,
Ann Lake & Helen Gonçalves products, choice of drugs, and drug dosages are the views of the authors. The views expressed by the editor or
Design: Jane Gouveia authors in this newsletter do not necessarily reflect those of the sponsors or publishers. The sponsors, publishers and
Sponsors: Sandoz editor will not be liable for any damages or injuries of any kind arising from the use or misuse of information provided
in this publication and do not support the use of products for off label indications.
Enquiries: lakeann@mweb.co.za
Volume 7 No 3 September 2018 3
Antibiotic susceptibility testing in the micro
lab “S, R or l”: What does it mean?
Dr Chanel Kingsburgh
Consultant Clinical Microbiologist, Department of Clinical Microbiology and Molecular Biology
Ampath National Reference Laboratory
Centurion
linicians rely on clinical microbiology laboratories the specific antibiotic being tested. This is performed under
to identify and do susceptibility testing of patho- standardised conditions following international guidelines.
gens isolated from clinical samples. In an era of
increasing multi-drug resistant and pan-drug re- There are two broad categories of susceptibility testing, namely
sistant organisms, determining which antibiotics dilution tests and diffusion tests. A comparison of the two is
the pathogen is susceptible to is crucial for the eradication of made in Table 1.
infection and preventing morbidity and mortality in the patient.
What then is susceptibility testing and how is it performed? These tests are usually performed manually as described
What does the “S, R, or I” mean on a laboratory report? above. Various automated systems have been developed and
are increasingly being used by laboratories across the world.
What is antibiotic susceptibility testing? Some of the benefits of using automated systems include,
Antibiotic susceptibility testing is laboratory-based testing among others, a decreased demand on human labour, some
performed on a bacterial isolate to determine which antibiotics instruments provide assistance in the interpretation of results
it is susceptible to. and results are available sooner because of the greater
sensitivity of the instrument’s optical systems in detecting
How is it done? subtle increases in microbial growth.
Antibiotic susceptibility testing is done by measuring the growth
of the isolate in the presence of a predetermined amount of
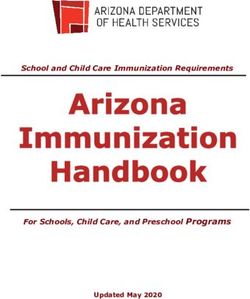
Table 1. Comparison of antibiotic susceptibility testing methods
Dilution tests Diffusion tests
Set amount of bacterial inoculum incubated in either
broth or solid medium containing a predetermined Agar plate is swabbed with a set bacterial inoculum
amount of antibiotic. The tubes or plates contain to which an antibiotic impregnated disk or strip is
Description serial dilutions of antibiotic. The minimum applied and incubated. The next day the zone size
inhibitory concentration (MIC) is read as the lowest is measured (disk) or MIC measured as point where
concentration of antibiotic that inhibits visible growth bacterial growth touches the strip.
of the organism.
Output data MIC MIC (strip) or zone size (disk)
Broth dilution Etest strip
Examples
Agar dilution Disk diffusion
4 Volume 7 No 3 September 2018
Most of the current automated instruments use the principle schedules and/or that demonstrate zone diameters that fall in
of turbidimetric detection of bacterial growth in a well using the range where specific microbial resistance mechanisms are
a photometer. An alternative means of growth detection is by likely. Clinical failure is therefore highly likely.
the detection of hydrolysis of a fluorogenic growth substrate
incorporated into a special test medium. If an organism is Clinical breakpoints make the
resistant to a specific concentration of antibiotic present in a
well, it will grow, consuming fluorophore-labelled substrates interpretation of MIC values and
present in the well. This leads to emission of a fluorescent zone diameters possible and are
signal which can be measured by a fluorometer. One example
of an automated antibiotic susceptibility testing instrument
published by international guidelines
is the Vitek® 2 system (bioMérieux). It is a highly automated to assist laboratories to release
system that uses complex plastic reagent cards that contain simple but meaningful information to
microliter quantities of antibiotics in a 64-well format. The
instrument uses repetitive turbidimetric monitoring of bacterial clinicians.
growth during an abbreviated incubation period. This allows it
to give a susceptibility result for the common, rapidly growing
gram-positive, and gram-negative aerobic bacteria, as well as How are these clinical breakpoints derived?
Streptococcus pneumoniae within 4 to 6 hours. Clinical breakpoints make the interpretation of MIC values
and zone diameters possible. These clinical breakpoints are
published by international guidelines to assist laboratories to
release simple but meaningful information to clinicians. How
are these breakpoints derived? First of all, a large number
of the bacterial isolate has to be collected, their MIC values
determined, and based on this, a wild type MIC is defined for the
organism. Secondly, the epidemiological cut-of value (ECOFF)
for the organism is calculated. An ECOFF is the MIC threshold
value that allows discrimination of wild type-strains (strains
that have no resistance mechanisms) from non-wild type strains
(strains with accumulated resistance mechanisms). Thirdly,
When should antibiotic susceptibility testing Pk/Pd data is collected, population pharmacokinetic models
be performed? are developed, and the Pk/Pd parameter that would result in
Antibiotic susceptibility testing should be performed on a the optimal outcome is determined (i.e. T> MIC, or AUC/MIC,
bacterial isolate from a clinical specimen when it is considered or Cmax/MIC). Next, Monte Carlo statistical simulations are
to be a pathogen and when the susceptibility to a specific performed and the Pk/Pd breakpoints are calculated based on
antibiotic cannot be reliably predicted. conventional dosing regimens. Clinical data is then collected
correlating the MIC of the organism, dosage, administration and
What does “S, R or I” stand for? last but not least, the clinical outcomes of patients. This then
“S, R, or I” stand for susceptible, resistant or intermediate allows tentative clinical breakpoints to be drawn up and sent
respectively. These are clinical breakpoints which have been to steering committees for comments. Once there is consensus
developed to indicate those clinical isolates that are likely regarding the clinical breakpoints, they are published by the
to respond to treatment with a given antimicrobial agent international guiding societies.
administered at the approved dosing regimen for that agent.
A susceptible isolate is one that is inhibited by the usually
achievable concentration of antibiotic when the recommended ECOFFs
dosage is used for the site of infection. It means that the
antibiotic is likely to have clinical efficacy when used at the
approved dosing regimen for an approved site of infection.
Intermediate applies to an isolate with a MIC or zone diameter Monte Clinical PK/PD data
that approaches the usually attainable blood and tissue levels. Carlo breakpoints collected
simulation derived
Here the response rate may be lower than for susceptible
isolates. However, in body sites where the drug is physiologically
concentrated or when higher than normal dosages of the
antibiotic can be safely used, you will probably have clinical
efficacy. Clinical
response data
collected
A resistant isolate is one that is not inhibited by the usually
achievable concentration of the agent with normal dosage
Volume 7 No 3 September 2018 5
How should “S”, “I”, or “R” be interpreted?
Can one safely conclude that “susceptible” means clinical Key messages
success and "resistant" clinical failure? Are these clinical
breakpoints 100% fool-proof? Unfortunately not. One cannot • Antibiotic susceptibility testing is crucial to guide antibiotic
with 100% confidence predict the clinical efficacy of an antibiotic therapy in an era of increasing multi-drug resistant organisms
based solely on the clinical breakpoints. Additional factors such • There are various antibiotic susceptibility testing modalities,
as host immunity/response, site of infection, the presence or all with their own strengths and weaknesses
absence of biofilm, etc. can all influence to response to the • One cannot, with 100% confidence, predict the clinical
antibiotic. There is a phenomenon that is referred to as the efficacy of an antibiotic based solely on its susceptibility
“90-60” rule that states that “susceptible” infections respond • Always consider host factors, site of infection, the possibility
to appropriate therapy approximately 90% of the time and of the presence of biofilm, etc. when judging the chances of
“resistant” infections respond only 60% of the time. clinical success
• “Susceptible” infections respond to appropriate antibiotic
Is there any use, then, in performing antibiotic therapy about 90% of the time and “resistant” infections
respond about 60% of the time
susceptibility testing?
• Never hesitate to phone your local microbiologist for
Definitely. Although antibiotic susceptibility testing is an
treatment advise
imperfect science, it is the best we currently have available to
us and is still very useful if interpreted whilst keeping in mind
the three crucial role players in any infection: The bug, the drug,
and the patient.
Feeling a bit confused?
If this has left you feeling a bit confused and overwhelmed,
always remember:
Your friendly microbiologist is always a phone-
call away!
References
1. Reller LB, Weinstein M, Jorgensen JH, Ferraro MJ.
Antimicrobial Susceptibility Testing: A Review of General
Principles and Contemporary Practices. Clin Infect Dis. 2009;
48(11).
2. Clinical and Laboratory Standards Institute (CLSI).
Performance Standards for Antimicrobial Susceptibility
Testing. 28th ed. CLSI supplement M100. 2018.
Images sources
1. www.basicmedicalkey.com
1. https://steemit.com
6 Volume 7 No 3 September 2018
Acute pneumonia in children
Professor Robin Green
Department of Paediatrics and Child Health, University of Pretoria
PhD,DSc
oughing is common in children and is usually due the commonest cause of bacterial pneumonia but vaccination
to a viral ‘cold’. Unfortunately antibiotic use is against pneumococcus is starting to reduce the incidence
largely unnecessary for coughing children and of pneumococcal pneumonia. Other bacterial causes acute
only contributes to antimicrobial resistance of in- pneumonia include Staphyloccocus aureus and Haemophilus
fectious organisms, especially bacteria. The World influenzae (both type b (Hib) and non-typeable disease).
Health Organization (WHO) has defined ‘pneumonia’ as a condi- Immunisation of young children against Hib has decreased the
tion that only occurs in children who have ‘fast breathing or incidence of pneumonia due to this bacterium, although non-
chest wall indrawing’.1 That would clearly separate a ‘cold’ of typeable strains are still responsible for a significant proportion
the upper respiratory tract from a lower respiratory tract infec- of pneumonia.
tion. However, in addition to pneumonia another important en-
tity exists in the lower respiratory tract that is almost always vi- Table 1. Common causes of AP in infants and
ral in origin. This condition is acute viral bronchiolitis. Therefore, children
whilst certain clinical phenotypes do not require antibiotics, Viruses
acute pneumonia is always treated with an antibiotic.
• Respiratory syncytial virus
• Rhinovirus
Acute pneumonia and acute viral bronchiolitis are responsible
• Influenza A and B
for significant illness-events annually in higher socio-economic • Parainfluenza virus types 1 and 3
countries, whilst pneumonia is the leading cause of death in • Adenovirus
children, under 5 years of age, in developing countries.2-6 The • Human metapneumovirus
HIV epidemic has contributed enormously to more severe • Bocavirus
pneumonia and increased mortality from this common • Corona virus
condition.4,6 Acute lower respiratory tract infections (ALRTI) • Measles virus
account for roughly 35% of hospital admissions, with associated • Cytomegalovirus
case fatality rates of between 15% and 28% in developing Bacteria
countries but death is less common in the developed world.7,8
• Streptococcus pneumoniae
Pneumonia still accounts for nearly one-fifth of childhood
• Haemophilus influenzae
deaths worldwide. • Staphylococcus aureus
• Mycobacterium tuberculosis
What bugs cause acute pneumonia in • Moraxella catarrhalis
children? • Bordetella pertussis
Atypical bacteria
Acute pneumonia (AP) is caused mostly by viruses and bacteria.
• Mycoplasma pneumoniae
Not only is it clinically impossible to distinguish viral from
• Chlamydia trachomatis
bacterial pneumonia, new evidence suggests that most cases of • Chlamydophila pneumoniae
AP in children have a mixture of micro-organisms in the airway
and that both bacteria and viruses occur in combination.9 In
addition, finding an organism on the common tests employed (of
airway secretions) does not prove that organism is causing the In addition pathogens vary by age and in neonates and children
lower airway infection. In addition, the problem is compounded younger than 2 months of age, Gram-negative bacteria, Group
by the fact that many healthy children harbor both viruses B streptococcus, S. aureus, and C. trachomatis, are important
and bacteria in their airways.9 These findings suggest that the causes. Atypical bacteria are more common in children 5 years
management of a ALRTI in children requires choosing therapies of age and older.
based on clinical findings rather than on special investigations.
The common causes of AP in children are listed in Table 1. Mycobacterium tuberculosis (TB) has been recognised as an
important cause of AP in both HIV-infected and HIV-uninfected
Bacteria are the important organisms causing mortality and children.10 In Uganda 20% of children with severe AP had
the reason for routine antibiotics when acute pneumonia clinically suspicious TB and 10% had a culture-confirmed
meets the clinical definition.1,3,4 Streptococcus pneumoniae is diagnosis.11
Volume 7 No 3 September 2018 7
Respiratory syncytial virus (RSV) is the commonest viral cause of The choice of antibiotic is clear in the WHO guideline – amoxicillin
AP, especially in young infants. RSV causes significant morbidity, (Figure 1). Addition of clavulanic acid may be useful in areas
especially in children born prematurely and who have other with high numbers of beta-lactamase producing Haemophilus
risk factors such as chronic lung disease and congenital cardiac influenzae.
disorders. HIV-infected children with RSV are more likely to
develop pneumonia rather than bronchiolitis as compared to In older children the addition of a macrolide is often advocated
HIV-uninfected children. Other important respiratory viruses and treatment for Staphylococcus aureus should be considered
include rhinovirus, influenza A and B, parainfluenza virus types in children with a pleural effusion, lung abscess, pneumatocoeles
1 and 3, adenovirus, human metapneumovirus, bocavirus, or who fail to respond to first line therapy.
coronavirus and measles virus.
Because we live in an era of resistant pneumococcal infections,
However, pneumonia resulting from opportunistic pathogens the dose of amoxicillin is 90mg/kg/day in two divided doses.
should also be considered in HIV-infected children. Of these, The new duration of therapy is ‘short course’, usually 3-5 days.1
Pneumocystis jiroveci and cytomegalovirus (CMV) are the
most common and serious infection among infants, occurring Oral therapy works just as well as intravenous therapy in all
commonly at 6 weeks - 4 months of age. children except those who cannot take medication orally.
How should we diagnose acute pneumonia? Beside an antibiotic the next most important therapeutic
strategy is to decide if the child requires oxygen. Peripheral
Pneumonia should be diagnosed clinically. The pattern of
12 oxygen saturations below 90-92% indicate a need for nasal
cough with fast breathing is the WHO definition for pneumonia prong oxygen.
and is appropriate for all levels of care.1
Ancillary therapies of nebulisation, oral steroids, cough
Special testing to decide on the presence of pneumonia such as mixtures and mucolytics have absolutely no role. In addition,
a CXR are not mandatory but may be useful if complications are physiotherapy for simple pneumonia is contra-indicated.
suspected.13,14
Children with measles should get two daily doses of 200 000IU
Haematological testing for C-reactive protein, erythrocyte of Vitamin A.17
sedimentation rate and white cell count are unnecessary and
blood culture is seldom positive.15,16 HIV-infected infants with severe hypoxic pneumonia should
be managed for Pneumocystis jirovecii.18 This usually involves
And then treating acute pneumonia ventilation with lung protective strategies as for acute
respiratory distress syndrome (often with high PEEP), Bactrim
The clinical pattern of cough and fast breathing without features and steroids, ganciclovir as well as fluid restriction.18
of bronchiolitis necessitates antibiotic therapy.
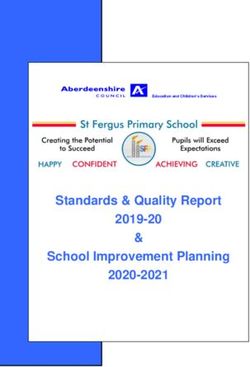
Comparison of previous and revised classification and treatment of childhood pneumonia at health facility
Revised classification and treatment
Previous classification and treatment Availability of for childhood pneumonia
of childhood pneumonia new evidence at health facility
Cough and cold: Home care
no pneumonia advice
Home care
Oral cotri- Cough and cold:
advice
moxazole no pneumonia
Fast breathing:
and home
pneumonia
care advice
Child Child
Oral
age 2-59 age 2-59 Fast breathing amoxicillin
months months and/or chest and home
with cough Chest indrawing: with cough indrawing: care advice
and/or severe First dose and/or pneumonia
difficult pneumonia antibiotic difficult
breathing and referral breathing
First dose
to facility for General danger antibiotic
injectable signs:F severe and referral
General danger antibiotic/ pneumonia or to facility for
signs:F severe supportive very severe injectable
pneumonia or therapy disease antibiotic/
very severe supportive
disease therapy
Figure 1. Reproduced with kind permission of 1.1
8 Volume 7 No 3 September 2018
Making sure parents know what is going on 4. Liu L, Oza S, Hogan D, et al. Global, regional, and national
causes of child mortality in 2000-13, with projections to
Children who are treated at home or go home after inform post-2015 priorities: an updated systematic analysis.
hospitalisation require their parents to know what is happening. Lancet 2015;385(9966):430-40.
Parent education is our most important tool (Table 2). 5. Mulholland K. Magnitude of the problem of childhood
pneumonia. Lancet 1999;534: 590-592.
6. Zwi KJ, Pettifor JM, Soderlund N. Paediatric hospital
Table 2. Key elements of an educational message for
admissions at a South African urban regional hospital: the
parents of children with AP12
impact of HIV, 1992-1997. Ann Trop Paediatr 1999;19: 135-
• The condition may start as an upper respiratory tract 142.
infection with low-grade fever 7. Leowski J. Mortality from acute respiratory infections in
• Symptoms are cough and often, fast breathing children under 5 years of age: Global estimates. World
• When a child has fast breathing, additional medical
Health Statistics Quarterly 1986;39:138–44.
help should be sought
• Bronchiolitis is caused by a virus; antibiotics are not
8. Levels and Trends in Child Mortality: Report 2014. United
needed Nations Inter Agency Group for Child Mortality Estimation.
• Bronchiolitis is usually self-limiting, although symptoms UNICEF, WHO, The World Bank, United Nations Population
may occur for up to 4 weeks in some children Division. New York, 2014.
• AP requires antibiotic treatment but the dose and 9. Annamalay AA, Abbbott S, Sikazwe, C, et al. Respiratory
duration are important viruses in young South African children with acute lower
• All over-the-counter medicines should be avoided respiratory infections and interactions with HIV. J Clin Virol
except for 'safe' fever medicines 2016;81:58-63
10. Bates M, Mudenda V, Mwaba P, Zumla A. Deaths due to
respiratory tract infections in Africa: a review of autopsy
studies. Curr Opin Pulm Med 2013;19:229-37.
11. Nantongo JM, Wobudeya E, Mupere E, et al. High incidence
Key messages of pulmonary tuberculosis in children admitted with severe
pneumonia in Uganda. BMC Pediatr 2013;13:16.
• Acute pneumonia in children may be caused by bacteria and 12. Green RJ, Zar HJ, White D, Madhi SA. Viral lower respiratory
viruses and they are indistinguishable clinically or by special tract infections. In: Viral infections in children. Green RJ
testing. (Editor). Austria, Springer Publications, 2017
• Therefore therapy is directed at the clinical picture of cough 13. Swingler GH. Radiologic differentiation between bacterial
and fast breathing and absence of wheeze or hyperinflation. and viral lower respiratory infection in children: A systematic
• Special tests are unnecessary. literature review. Clin Pediatr 2000;39:627-633.
• The best antibiotic is amoxicillin at 90mg/kg/day for 3-5 14. Swingler GH, Hussey GD, Zwarenstein M. Randomised
days. controlled trial of clinical outcome after chest radiograph
• Oxygen administered via nasal prongs in hospital is required in ambulatory acute lower-respiratory infection in children.
for hypoxic children. Lancet 1998;351:404-408.
• Do not use cough mixtures, nebulised drugs, oral steroids or 15. Nohynek H, Valkeila E, Leinonen M, et al. Erythrocyte
physiotherapy for children with pneumonia. sedimentation rate, white blood cell count and serum
C-reactive protein in assessing etiologic diagnosis of acute
lower respiratory infections in children. Pediatr Infect Dis J
1995;14:484-490.
References 16. Toikka P, Irjala K, Juven T, et al. Serum procalcitonin,
1. World Health Organization. Revised WHO classification C-reactive protein and interleukin-6 for distinguishing
and treatment of childhood pneumonia at health facilities. bacterial and viral pneumonia in children. Pediatr Infect Dis
World Health Organization 2014. http://apps.who.int/iris/ J 2000;19:598-602.
bitstream/10665/137319/1/9789241507813_eng.pdf 17. Hussey GD, Klein M. A randomized, controlled trial of
2. Wardlaw T, You D, Newby H, Anthony D, Chopra M. vitamin A in children with severe measles. N Engl J Med
Child survival: a message of hope but a call for renewed 1990;323(3):160-4.
commitment in UNICEF report. Reprod Health 2013;10:64. 18. Kitchin OP, Becker P, Masekela R, Green RJ. Outcome of
3. Guerrera G. Neonatal and pediatric healthcare HIV exposed and infected children admitted to a pediatric
worldwide: A report from UNICEF. Clin Chim Acta 2015;pii intensive care unit for respiratory failure. Pediatr Crit Care
:S0009-8981(15)00136-9. Med 2012;13:516-519.
Volume 7 No 3 September 2018 9
Postexposure Prophylaxis in Infectious
Diseases
Dr Michelle Venter MBBCh (Wits), FCP (SA), MMed (Int Med), Dip HIV Man (SA), Cert ID (Phys) SA
Infectious Diseases Department
Charlotte Maxeke Johannesburg Academic Hospital
Johannesburg
xposure to communicable diseases via exposure to blood, tissues, or body fluids (semen, cerebrospinal, pleural, perito-
neal, pericardial, synovial and amniotic fluid) occurs in both occupational and non-occupational settings. Communicable
diseases may be transmitted via bloodborne, airborne and other routes (mucosal contact).
The role of postexposure prophylaxis (PEP) in the setting of infectious diseases is twofold: To prevent incipient illness in the
exposed individual after exposure, and to reduce the onward spread of these pathogens to other susceptible individuals.
Postexposure prophylaxis (PEP) refers to the comprehensive management package prescribed to minimise the risk of infection
following an exposure to potentially infectious pathogens. Strategies used as part of a PEP bundle may include vaccination,
immunoglobulins, antibiotics and antiviral medication, depending on the specific pathogen encountered. These strategies may
also be combined in the setting of PEP. The requirement for PEP depends on pathogen, disease and patient-related factors. These
factors are weighed up by the treating clinician in the decision as to whether PEP is required or not.
Steps in Determining if PEP is Warranted 3. Determine if the Source Patient is Infectious at
the Time of Exposure
1. Assess the Nature and Source of the Exposure If possible, the source patient should be asked about the date
A detailed source history is helpful, but not always available. of onset of illness and the last day of symptoms. This helps in
Ideally, a source history, examination and any relevant laboratory determining the infectious period for the specific pathogen.
investigations should be documented. In the exposed individual,
relevant history includes preceding background illness, 4. Determine the Type and Characteristics of the
medications taken and prior vaccination status. It is also important Exposure
to obtain a detailed exposure history - what the nature of the A significant exposure to an infectious disease is defined as
exposure was, when it happened, circumstances surrounding the one in which the risk of transmitting microorganisms is high.
exposure and precautions taken to avoid infection.
• For bloodborne pathogens, the average risk of infection
Key information that should be after percutaneous exposure to blood from a patient
documented after an exposure: infected with HIV is approximately 0.3% (Ippolito, Puro et
al 1993)
• Name and exposure-relevant information of the
source, if available. • For hepatitis B virus, 6% (if the hepatitis B e antigen is
• Time and date of exposure. negative) to 31% (if the hepatitis B e antigen is positive)
• Nature of exposure (non-intact skin, mucosal, or (Werner and Grady 1982)
percutaneous exposure). • For hepatitis C virus, 1.8% (Puro, Petrosillo et al 1995).
• Body site exposed and contact time. • For airborne spread, prolonged or close contact to a person
• Infective status of the source if known. with active disease without appropriate infection control
• For percutaneous injuries: a description of the practices constitutes a risk.
injury (depth of wound, solid versus hollow
needle) as well as measures taken after the
injury (irrigation, washing with soap and water). Table 1. Exposure - type and characteristics
• Circumstances under which the exposure Mode Examples
incident occurred. Airborne Measles, tuberculosis, varicella zoster virus
• Previous testing and immune status of the Bites Rabies, tetanus
exposed individual if known.
Hepatitis B virus, hepatitis C virus, human
Bloodborne
immunodeficiency virus (HIV)
2. Determine if the Source Patient is Infected Contact Varicella zoster virus
with a Communicable Disease Diphtheria, influenza, invasive
For certain infections (human immunodeficiency virus (HIV), Droplet
meningococcal disease, pertussis
hepatitis A, hepatitis B) the diagnosis in the source patient may Faeco-oral Hepatitis A virus
be determined by laboratory investigations.
10 Volume 7 No 3 September 20185. Determine if the Exposed Individual is −− 6 weeks: HIV test (rapid test plus 4th generation ELISA),
Susceptible syphilis serology (RPR or TPAb)
A vaccination history should be sought from the exposed individu- * Comment on Hepatitis C virus testing: if the source individual is
al. If the history is uncertain, serological testing may be considered. an intravenous drug user, MSM, haemophiliac or from a high HCV
prevalence setting, or where the source is unknown. In such cases,
the source should be tested for HCV Ab. If the source is HCV-negative,
6. Determine the Proper Management for the the exposed individual should be tested at baseline to assess their
Exposure, Including the Correct PEP Regimen own HCV status, and no further HCV testing will be necessary in
Guidelines for exposures requiring PEP have been published, further follow-up. However, where the source is HCV-positive, and
and it is advisable to familiarise oneself with them. Should the the exposed individual is HCV-negative at baseline, HCV PCR testing
situation require it, consultation with an infectious diseases should be performed at 6 weeks.
specialist may be warranted.
Hepatitis B Virus
7. Appropriate Baseline and Follow-up
Investigations Source disease status
Persons exposed to an infectious source should be assessed • HBsAg-negative: If exposed individual is not vaccinated or
at baseline and at subsequent intervals while they are at risk does not know their vaccination or antibody status, refer to
of developing the disease of concern, as well as for any side- a local facility for testing and vaccination.
effects of the PEP regimen. • HBsAg-positive or unknown source: Management depends
on the status of the exposed person as follows
8. Appropriate Counselling
Inadvertent exposure to a potentially infectious pathogen may Table 2. Management of Hepatitis B
result in anxiety in the exposed individual concerning potential
Vaccinated HBIG
disease acquisition and onward transmission. Psychological
status of HBsAb HBV vaccine (0.06 mL/
support and counselling may be required. exposed kg)
Counselling for these patients should include issues around Previous
confidentiality, rational quantification of the potential risk of vaccination;
Not done None None
known
infection, the rationale behind either administering or withholding
responder
PEP, possible adverse reactions related to PEP and counselling
pertaining to the prevention of transmission to others. If HBsAb >
10 IU/mL
(natural None None
PEP for Specific Pathogens immunity to
hepatitis B)
Not vacci-
Bloodborne Pathogens nated If HBsAb
1st dose stat and
Give stat
proceed to accel-
< 10 IU/mL HBIG
Human Immunodeficiency Virus (HIV) erated vaccina-
(no natural and
tion schedule
immunity to repeat at
(0, 1 and 6
Status of the exposed person hepatitis B) 1 month
months)
• Baseline investigations: HIV test (rapid test plus 4th generation
ELISA), hepatitis B surface antigen (HBsAg), hepatitis C
Complete
antibodies (HCV)*, syphilis serology (rapid plasma reagin-RPR Incomplete depending on
or treponema pallidum antibodies-TPAb) and serum creatinine. Single
vaccination - documentation or
dose stat
or unsure restart 0, 1 and 6
Regimen (adults and adolescents ≥ 35 kg) months
• HIV PEP regimens should contain three drugs.
−− Preferred PEP backbone regimen is tenofovir (TDF) +
lamivudine/emtricitabine (3TC/FTC).
−− Raltegravir (RAL) recommended as the preferred third Vaccinated;
drug (except in pregnant women, where atazanavir/ Single
unknown - Single booster stat
dose stat
ritonavir-ATV/r is the recommended third drug). response
−− Alternative third drugs include ATV/r, lopinivir/ritonavir-
LPV/r, darunavir-ritonavir DRV/r or efavirenz (EFV).
• Full one-month course of antiretroviral drugs should be 1st dose stat
provided at initial assessment; starter packs are discouraged. Give stat
and proceed
Non- HBIG
• Exposed individual should be seen at 2 weeks, 6 weeks and 3 to accelerated
responder HBsAb and
months after exposure: vaccination
to prior < 10 IU/mL repeat at
−− 2 weeks: Creatinine if TDF forms part of the backbone of schedule
vaccination 1 month
treatment (0, 1 and 6
months)
−− 6 weeks: HIV test (rapid test plus 4th generation ELISA),
HCV PCR* * Comment: HBIG and HBV vaccine can be administered
concomitantly at different sites
Volume 7 No 3 September 2018 11Airborne Pathogens contacts within 21 days of onset of cough in the index case.
Antibiotics only prevent pertussis disease if given prior to
Influenza Virus symptom onset (during the incubation period).
Spread via respiratory droplets that are generated by coughing, • Vaccinate close and vulnerable contacts appropriately.
sneezing and talking. Human-to-human transmission of • Monitor contacts for at least 21 days for signs and symptoms
influenza viruses occurs either directly or indirectly through of pertussis
close, unprotected contact with large respiratory droplets.
A person with flu is contagious from 1 day before and for 3-7 Diphtheria
days after the onset of symptoms. Diphtheria is a contagious and potentially life-threatening
bacterial infection caused by infection with a toxin-producing
Exposed individuals who are at particularly high risk of strain of Corynebacterium diphtheriae which spreads from
complications of influenza include: Pregnant women (including person to person through contact with respiratory droplets
the 2-week period after delivery), young children (under the or hand-to-mouth contact with secretions from an infected
age of 2 years), the elderly (over 65 years of age), people with person’s mouth, nose and throat.
existing chronic diseases (heart, lung, kidney, endocrine), Following exposure to a case of diphtheria, contacts (persons
immunosuppression, morbid obesity (BMI ≥40/BMI≥35 with sharing meals or living in the same house, persons caring
obesity-related health conditions). for infected children, or HCWs who have conducted CPR, or
procedures involving contact with respiratory secretions) should
Antiviral chemoprophylaxis is currently not recommended. have a nasopharyngeal and oropharyngeal swab to determine
However, WHO guidelines recommend that individuals at high carriage status, followed by chemoprophylaxis which eliminates
risk of severe disease who have been exposed to a patient with asymptomatic carriage and treats incubating disease.
confirmed influenza may benefit from presumptive treatment
with a full twice-daily 5-day course of antivirals, even if they do Appropriate vaccination depends on current vaccination
not show signs and symptoms of infection. Alternatively, such status, with all contacts requiring at least one dose of vaccine.
patients can be monitored closely for early signs of possible All contacts should be educated about the symptoms of
influenza infection, and given antiviral treatment if they occur. diphtheria and monitored for 10 days for the development
of symptoms of diphtheria. Follow-up swabs should be
Pertussis (whooping cough) collected from contacts that were culture or PCR positive for
Pertussis is a highly contagious, vaccine-preventable respiratory toxigenic C. diphtheriae on primary culture, after completion
tract disease, caused by the bacterium Bordetella pertussis. of chemoprophylaxis. Chemoprophylaxis should be repeated if
It can affect people of all ages. Young unimmunised/ partially contacts remain C. diphtheriae positive.
immunised infants are the most vulnerable group with the
highest rates of complications and death. Table 4. Recommended Chemoprophy-
laxis for close Contacts (diptheria)
Spread occurs from person-to-person by respiratory droplets • Children < 6 years: Single dose: 600
from infected individuals who are most contagious during the 000 units IM
early catarrhal stage. Those with pertussis are infectious from Benzylpenicillin • Children > 6 years: Single dose: 1.2
the beginning of the catarrhal stage to the third week after the million units IM
onset of paroxysms or until 5 days after the start of effective • Adults: Single dose: 1.2 million units IM
antimicrobial treatment. • Children: oral 10 mg/kg per day on
day one, then 5 mg/kg per day for
Azithromycin four days
Table 3. Recommended Pertussis • Adult: oral 500 mg on day one, then
250 mg daily for four days
Vaccination Schedule for Close Contacts
Children 32 containing vaccine if they vaccination in the exposed individual, as well as for the
weeks’ gestation) have not been vaccinated notification of the condition in the source patient to the relevant
in the last five years) medical authorities, if it is a notifiable condition.
Although it is not currently legally mandated in health-
Management of contacts should be undertaken in all confirmed
care workers, annual immunisation against influenza and
and suspected pertussis cases:
immunisation for hepatitis B are advised due to both a high risk
• Identify close and vulnerable (at-risk of severe disease)
of exposure in the occupational setting as well as the risk of
contacts including health care workers (HCWs).
onward transmission to at-risk patients.
• Take nasopharyngeal swabs from symptomatic contacts.
• Give targeted chemoprophylaxis to close and vulnerable
12 Volume 7 No 3 September 2018Useful Resources References
• South African HIV Clinicians Society: www.sahivsoc.org 1. (2010). WHO Guidelines for Pharmacological Management
• National Institute for Communicable Diseases (NICD): of Pandemic Influenza A(H1N1) 2009 and Other Influenza
www.nicd.ac.za Viruses. Geneva.
• Centers for Disease Control and Prevention (CDC): 2. Ippolito, G., V. Puro and G. De Carli (1993). "The risk of
www.cdc.gov occupational human immunodeficiency virus infection in
• Online notification of notifiable conditions: health care workers. Italian Multicenter Study. The Italian
www.nicd.ac.za/index.php/nmc Study Group on Occupational Risk of HIV infection." Arch
Intern Med 153(12): 1451-1458.
3. Puro, V., N. Petrosillo, G. Ippolito, M. S. Aloisi, E. Boumis
Key messages and L. Rava (1995). "Occupational hepatitis C virus infection
in Italian health care workers. Italian Study Group on
• PEP is routinely recommended following exposure to a wide Occupational Risk of Bloodborne Infections." Am J Public
spectrum of viral and bacterial diseases. Thus, physicians Health 85(9): 1272-1275.
should be familiar with established, locally relevant PEP 4. Werner, B. G. and G. F. Grady (1982). "Accidental hepatitis-
protocols. B-surface-antigen-positive inoculations. Use of e antigen to
• Selecting appropriate patients to receive PEP should be estimate infectivity." Ann Intern Med 97(3): 367-369.
based on the assessment of the type of exposure, the status
of the source patient, and the status of the exposed person.
• PEP should be given as soon as possible following a high-risk
exposure.
• Locally-applicable guidelines are available for commonly-
encountered entities that require PEP and may be accessed
at the resources listed below.
Congresses 2018/2019
Event/Congress Date Venue Contact
Pan African Travel
Southern Sun, Cape Sun, www.sastm.org.za/TMC/
Medicine Congress 12-15 September
Cape Town Details/18
2018
34th World Congress Cape Town International
of Internal Medicine 18-21 October Convention Centre, Cape www.wcim2018.com
(WCIM 2018) Town
ALLPAEDS 2018 (SAPA 29 August - 2 Century City Conference
www.allpaeds2018.co.za/
& ALLSA) September Centre, Cape Town
South African HIV
Gallagher Convention
Clinicans Society 24-27 October www.sahivsoc2018.co.za/
Centre, Johannesburg
Sahivsoc2018
21st International
Conference on
Tuberculosis: Clinics, 12-13 January waset.org/conference/2019/01/
Cape Town
Diagnostics, Therapy, 2019 durban/ICTCDTE
and Epidemiology
ICTCDTE 2019
Volume 7 No 3 September 2018 1314 Volume 7 No 3 September 2018
You can also read