Jpn.ca An open-access journal
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
jpn.ca
An open-access journal
March 2018 Volume 43 Number 2
Adolescent THC exposure in female rats leads to cognitive
deficits through a mechanism involving chromatin
modifications in the prefrontal cortex
Arterial stiffness is associated with depression
in middle-aged men — the Maastricht Study
Publications Mail Agreement no. 41387051
She knows
the pain.
Novartis Pharmaceuticals Canada Inc. © 2018 Novartis Pharmaceuticals Canada Inc. For additional information, please contact Novartis med info:
Dorval, Quebec H9S 1A9 Medical Information Email: medinfo.canada@novartis.com
www.novartis.ca NPR/AMG/0001E Medical Information Toll-free Number: 1-800-363-8883
T 514 631-6775 F 514 631-1867
We know
the science.
We are committed to advancing the science
of migraines.
Today, a growing understanding of CGRP*
brings new insights to the science behind
the migraine experience.1
*CGRP, calcitonin gene-related peptide
Reference: 1. Headache Classification Committee of the International Headache Society. The International
Classification of Headache Disorders, 3rd edition (beta version); 2013 Cephalalgia 33(9) 629–808.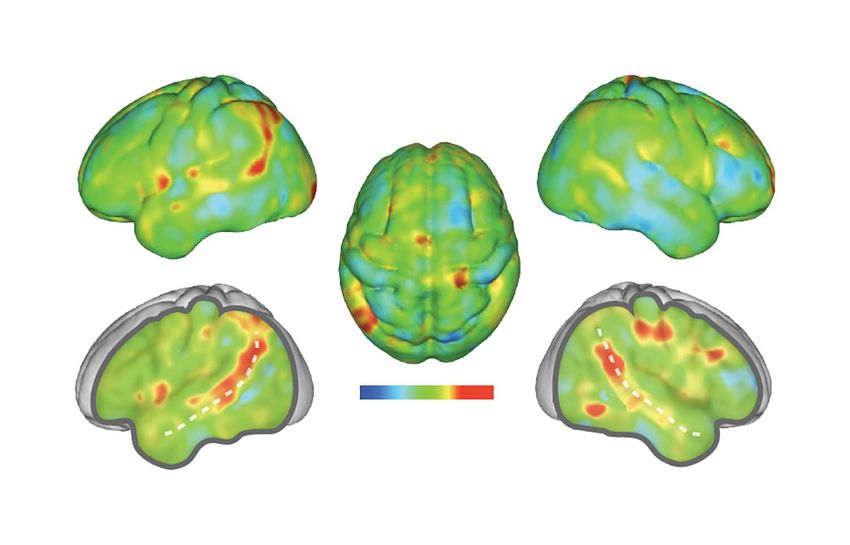
Editors-in-Chief
P. Boksa, PhD
R. Joober, MD, PhD
Editor Emeritus
Y.D. Lapierre, MD
Associate Editors Official Journal of the Canadian College of Neuropsychopharmacology
P. Albert, PhD
M. Alda, MD
March 2018 Vol. 43, No. 2 jpn.ca
H. Anisman, PhD
M. Leyton, PhD
G.M. MacQueen, MD, PhD
Editorial
Associate Editors (Statistics)
A. Labbe, PhD
76 Is poststroke depression the same as major depression?
N. Schmitz, PhD P.R. Albert
Editorial Board competing interest statements
are available at jpn.ca
Research Papers
Editorial Advisory Board
G. Agam, PhD, Israel 79 Grey matter correlates of autistic traits in women
S.L. Andersen, PhD, USA with anorexia nervosa
M. Bourin, MD, France M. Björnsdotter, M. Davidovic, L. Karjalainen, G. Starck, H. Olausson,
S. Chattarji, PhD, India
E. Wentz
K.P. Ebmeier, MD, United Kingdom
S. Floresco, PhD, Canada
T.S. Frodl, MD, Ireland
K.A. Hawkins, PsyD, USA 87 Adolescent THC exposure in female rats leads to cognitive deficits
S. Kanba, MD, PhD, Japan
through a mechanism involving chromatin modifications in the
F. Kapczinski, MD, PhD, Brazil
T. Kato, MD, PhD, Japan prefrontal cortex
J. Mendlewicz, MD, Belgium P. Prini, F. Rusconi, E. Zamberletti, M. Gabaglio, F. Penna, M. Fasano,
S.A. Montgomery, MD, United Kingdom E. Battaglioli, D. Parolaro, T. Rubino
B. Müller-Oerlinghausen, MD, Germany
I. Nalepa, PhD, DSc, Poland
P. Ohrmann, MD, Germany
M. Pollack, MD, USA 102 A postmortem analysis of NMDA ionotropic and group 1
G.J. Sarwer-Foner, MD, USA metabotropic glutamate receptors in the nucleus accumbens in
P. Seeman, MD, PhD, Canada schizophrenia
A. Serretti, MD, Italy J.S. Lum, S.J. Millard, X.-F. Huang, L. Ooi, K.A. Newell
D.J. Stein, MD, South Africa
K.G. Todd, PhD, Canada
V.K. Yeragani, MD, India
111 Arterial stiffness is associated with depression in middle-aged
Submit your manuscript at men — the Maastricht Study
http://mc.manuscriptcentral.com/jpn V. Onete, R.M. Henry, S.J.S. Sep, A. Koster, C.J. van der Kallen,
P.C. Dagnelie, N. Schaper, S. Köhler, K. Reesink, C.D.A. Stehouwer,
© 2018 Joule Inc. M.T. Schram
ISSN 1180-4882
120 Greater body mass index is associated with reduced frontal
cortical volumes among adolescents with bipolar disorder
A.H. Islam, A.W.S. Metcalfe, B.J. MacIntosh, D.J. Korczak,
B.I. Goldstein
Publications Mail Agreement no. 41387051. 131 Association between structural and functional brain alterations
in drug-free patients with schizophrenia: a multimodal
Printed by The Lowe-Martin Group, meta-analysis
Ottawa, Ont.
Appears in January, March, May, July, X. Gao, W. Zhang, L. Yao, Y. Xiao, L. Liu, J. Liu, S. Li, B. Tao, C. Shah,
September and November. Q. Gong, J.A. Sweeney, S. Lui
74 J Psychiatry Neurosci 2018;43(2)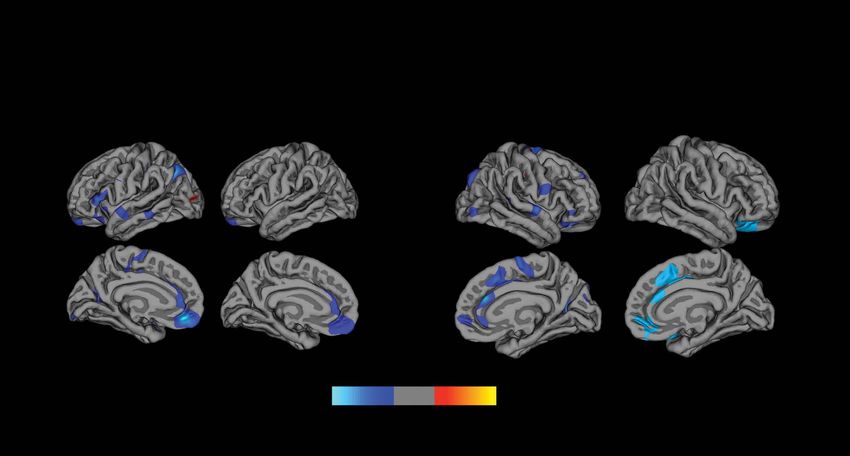
Editorial Staff Psychopharmacology for the Clinician
Managing Editor
Wendy Carroll 143 Covert dysphagia and recurrent pneumonia related to
wendy.carroll@cma.ca antipsychotic treatment
tel 800 663-7336 x8419
J.T. Stewart
Editorial Coordinator
Holly Clark
holly.clark@cma.ca
tel 800 663-7336 x8424
IBC Service Information
Production Staff
Manager, Production & Graphic Design
Jennifer Pershick
Production Designers
Carole Lalonde, Sarah O’Neill, Clara Walker
Online Publishing
James Manship The Journal of Psychiatry & Neuroscience publishes papers at the intersection of psychiatry
and neuroscience that advance our understanding of the etiology, pathophysiology and
treatment of psychiatric disorders. This includes studies on patients with psychiatric
CMAJ Group Staff disorders, healthy humans, and experimental animals as well as studies in vitro. Original
research articles, including clinical trials, and review papers will be considered.
Editor in Chief, Interim
Diane Kelsall
Publisher, Interim
Holly Bodger
Advertising All editorial matter in the Journal of Psychiatry & Neuroscience represents the opinions of
the authors and not necessarily those of the publisher. We assume no responsibility or
Classified Advertising liability for damages arising from any error or omission, or from use of any information
Laurie McLeod, Susan Ritchie or advice contained in the Journal of Psychiatry & Neuroscience, including articles, editorials,
613 731-8610 x8460/8475 reviews, abstracts, letters and advertisements.
advertising@cma.ca
Display Advertising Sales
Trish Sullivan
cell 905 330-8770; trish.sullivan@cma.ca
All prescription drug advertisements have been
cleared by the Pharmaceutical Advertising Online manuscript
Advisory Board. submission and peer review
Published by Joule Inc., a wholly owned subsidiary
AVAILABLE at
of the Canadian Medical Association.
http://mc.manuscriptcentral.com/jpn
Visit JPN’s archives
Full-text PDFs going back to 1991 are available at
pubmedcentral.com
J Psychiatry Neurosci 2018;43(2) 75
Editorial
The views expressed in this editorial are those of the author(s) and do not necessarily reflect the position of the Canadian Medical Association or its subsidiaries,
the journal’s editorial board or the Canadian College of Neuropsychopharmacology.
Is poststroke depression the same as major depression?
Paul R. Albert, PhD
What causes PSD versus major depression? Thus, an emerging concept that remains to be tested is that
strokes leading to PSD may disrupt the anxiety or depression
In the United States, it is estimated that 11 million strokes oc- circuitry at several locations.14
curred within 1 year (1998).1,2 Poststroke depression (PSD) is a
common outcome following stroke, with 30% of patients post- Detecting PSD and vascular depression
stroke having comorbid major depression and 80% of patients
having milder forms of depression.3,4 Patients with PSD show Poststroke depression is a form of vascular depression related
increased likelihood of recurrent stroke and depression, and to large vessel occlusion.14 Covert (or “silent”) strokes include
increased mortality compared with nondepressed patients.5 small brain infarcts or microbleeds (lacunae or white matter
Major depression is a chronic disorder that is often comorbid infarctions) that do not result in obvious sensorimotor impair-
with anxiety.6 Environmental stressors, including having a ments. Covert strokes are five-fold more frequent forms of
stroke, contribute to predisposition and can trigger episodes stroke, with one stroke every nine minutes (62 000/yr) and one
of major depression.6 Both PSD and major depression are covert stroke each two minutes in Canada.2,15 Recently, vascu-
diagnosed according to the same set of criteria that combine lar depression has been associated with the presence of covert
diverse and sometimes opposite symptoms, which contrib- strokes.11 Thus, the prevalence of vascular depression is poten-
utes to the heterogeneous nature of major depression.7 One of tially five-fold higher than that of PSD.16 On the other hand the
the goals of psychiatry today is to move toward precision incidence of covert stroke in depressed patients is 46%,2 consis-
medicine by elucidating biomarkers for better characteriza- tent with a strong bidirectional connection between the two.17
tion of mental illness and its treatment.8 Identifying the However, the “silence” of covert stroke presents a challenge in
underlying molecular, cellular or circuit changes leading to detecting vascular versus major depression. Presently, covert
behavioural phenotypes can be used to target therapeutic stroke is often detected only once a more severe condition
interventions to specific mechanisms driving mental illness. arises requiring imaging, at which time the presence of lacunae
This raises the question of whether PSD and major depression or white matter hyperintensities may be evident. Typically, pa-
should be considered the same or separate mental illnesses. tients presenting with depression are not referred for imaging,
Poststroke depression appears to be triggered by or linked but the need for imaging may be important, particularly in
to the ischemic event, as depression occurs within three patients with risk factors for cerebrovascular disease (e.g., car-
months of a stroke.3 How stroke triggers depression is un- diovascular disease, hypertension, diabetes).2,17 Recently, im
clear. The sudden physical handicap and loss of personal in- aging has been applied with repetitive transcranial magnetic
dependence following stroke may trigger a chronic state of stimulation (rTMS), which is recommended as second-line
depression. However, there is evidence that lesions associated treatment for major depression in patients who do not respond
with stroke or vascular ischemic events, particularly in cases to antidepressant treatment.18 It remains unclear what propor-
of covert stroke where no evident impairment presents, can tion of patients with major depression show stroke pathology
lead to depression. The size, number of ischemic lesions, and that may suggest vascular depression. Based on the prevalence
whether the lesions disrupt the midbrain, limbic and medial of covert stroke, this proportion may be substantial.
prefrontal cortical (mPFC) circuitry are implicated in depres-
sion.9 In particular, white matter lesions are associated with Does PSD/vascular depression respond to
metabolic alterations in this circuitry10 and are correlated with antidepressant treatment?
major depression.11 Several independent studies have indi-
cated that in patients with ischemic stroke, lesions in the left Assuming we can distinguish PSD and vascular depression
frontal cortex, left basal ganglia or brainstem are correlated from major depression, how does this impact treatment? It
with affective and apathetic symptoms of depression.12,13 remains unclear. Like major depression, PSD is mainly
Correspondence to: P. Albert, UOttawa Brain and Mind Research Institute, Ottawa Hospital Research Institute, 451 Smyth Road, Ottawa, ON
K1H 8M5; paul.Albert@uottawa.ca
DOI: 10.1503/jpn.180015
© 2018 Joule Inc. or its licensors
76 J Psychiatry Neurosci 2018;43(2)
Is poststroke depression the same as major depression?
treated with antidepressants, such as selective serotonin umans.31 It has been suggested that neuroinflammatory pro-
h
reuptake inhibitors (SSRIs).14 There is evidence that in addi- cesses involving cytokine and microglial mobilization underlie
tion to improving anxiety and depression symptoms, SSRIs some forms of depression,29,32 and inflammatory processes
also enhance poststroke cognitive ability and recovery.9,14,19 may be important in the pathology of PSD and vascular de-
However, most antidepressants require chronic treatment pression.33,34 Therefore, vascular depression may fall into a
(3–4 weeks) to produce improvement.20 For major depres- “neuroinflammatory” depression phenotype.14
sion, the STAR*D study found that although about 50% of Hence the question remains: how much of major depres-
patients responded to SSRIs, remission occurred in only sion is really undiagnosed PSD? It can be argued that in-
30%.21 It remains unclear whether the same can be said for creased effort to diagnose both systemic inflammation and
PSD or vascular depression; notably, chronic SSRI treatment small-vessel disease in depressed individuals is warranted,
increases the risk of hemorrhage.22,23 However, to examine since many of the risk factors leading to stroke (e.g., diabetes,
treatment outcomes for vascular depression, it will be neces- atherosclerosis, stroke, heart failure) are also tied to depres-
sary to first detect it using imaging, as mentioned earlier. sion.2,16,35 The good news is that these risk factors, if recog-
What can preclinical studies tell us about treatment for nized early enough, can be controlled to prevent or reverse
PSD? Most rodent models of PSD have used middle cerebral the depression phenotype.36
artery occlusion, which produces a large and variable lesion,
leading to sensorimotor impairments and altered behaviour.24 Acknowledgements: The author thanks Drs. Faranak Vahid-Ansari,
Antoine M. Hakim, and the members of the JPN Editorial Board for
The sensorimotor impairments may confound behavioural their insightful comments and suggestions. P. Albert is supported by
tests that are often based on intact sensorimotor function. grants from the Canadian Institutes of Health Research and the HSF
Thus, in order to obtain a robust depression phenotype, mid- Canadian Partnership for Stroke Recovery.
dle cerebral artery occlusion has been combined with chronic Affiliation: From the UOttawa Brain and Mind Research Insitute,
stress, which itself induces depression-like behaviour. Al- Ottawa Hospital Research Institute, University of Ottawa, Ottawa,
though chronic SSRI treatment is effective, this raises the Ont., Canada.
question of whether stroke- or stress-induced depression is Competing interests: None declared.
being studied. One recent study used photothrombosis to
elicit an anterior cortical stroke and waited until sensorimotor
References
function recovered before testing behaviour.25 The researchers
showed that chronic SSRI treatment is effective to reverse the 1. Leary MC, Saver JL. Annual incidence of first silent stroke in the
United States: a preliminary estimate. Cerebrovasc Dis 2003;16:280-5.
anxiety- and depression-like phenotypes, involving increase 2. Vermeer SE, Longstreth WT Jr, Koudstaal PJ. Silent brain infarcts:
in hippocampal brain-derived neurotrophic factor.25 Another a systematic review. Lancet Neurol 2007;6:611-9.
model used endothelin-1 microinjection to induce a small 3. Paolucci S, Gandolfo C, Provinciali L, et al. The Italian multicenter
lesion of the left medial prefrontal cortex, resulting in anxiety- observational study on post-stroke depression (DESTRO). J Neurol
2006;253:556-62.
and depression-like behaviour, as well as cognitive impair- 4. Hackett ML, Pickles K. Part I: frequency of depression after stroke:
ment, with no sensorimotor impairment.26,27 In this model, an updated systematic review and meta-analysis of observational
chronic SSRI treatment, but not free running wheel exercise, studies. Int J Stroke 2014;9:1017-25.
5. Ayerbe L, Ayis S, Crichton S, et al. The natural history of depres-
reversed the behavioural and cognitive phenotypes. Interest- sion up to 15 years after stroke: the South London Stroke Register.
ingly, the small lesion became refilled with neurons, which Stroke 2013;44:1105-10.
may be recruited by SSRI treatment. These findings suggest 6. Hyman S. Mental illness: genetically complex disorders of neural
that chronic SSRI treatment is effective to reverse PSD, in part circuitry and neural communication. Neuron 2000;28:321-3.
7. Krishnan V, Nestler EJ. The molecular neurobiology of depression.
through growth factor induction. In this regard, chronic SSRI Nature 2008;455:894-902.
treatment may trigger neuroplasticity to promote recovery 8. Insel TR, Cuthbert BN. Medicine. Brain disorders? Precisely. Science
from depression, including PSD. However, clinical studies of 2015;348:499-500.
9. Flaster M, Sharma A, Rao M, et al. Poststroke depression: a review
the effectiveness of SSRI treatment in human PSD or vascular emphasizing the role of prophylactic treatment and synergy with
depression need to be done and will require a dedicated treatment for motor recovery. Top Stroke Rehabil 2013;20:139-50.
pretreatment imaging screen to detect vascular lesions in 10. Capizzano AA, Jorge RE, Robinson RG. Limbic metabolic abnor-
malities in remote traumatic brain injury and correlation with
drug-naive, depressed patients. psychiatric morbidity and social functioning. J Neuropsychiatry Clin
Neurosci 2010;22:370-7.
Etiology of PSD and depression: inflammation 11. Taylor WD, Aizenstein HJ, Alexopoulos GS. The vascular depression
link? hypothesis: mechanisms linking vascular disease with depres-
sion. Mol Psychiatry 2013;18:963-74.
12. Terroni L, Amaro E, Iosifescu DV, et al. Stroke lesion in cortical
The pathology underlying PSD and major depression differs. neural circuits and post-stroke incidence of major depressive epi-
Stroke leads to neuronal and glial cell death due to hypoxic sode: a 4-month prospective study. World J Biol Psychiatry 2011;
12:539-48.
lesion, whereas major depression is not always associated with 13. Murakami T1, Hama S, Yamashita H, et al. Neuroanatomic path-
detectable cell death. However, postmortem studies of brains ways associated with poststroke affective and apathetic depression.
from depressed individuals who committed suicide show loss Am J Geriatr Psychiatry 2013;21:840-7.
of glia and neurons.28,29 Chronic stress is known to induce 14. Robinson RG, Jorge RE. Post-stroke depression: a review. Am J
Psychiatry 2016;173:221-31.
neuronal atrophy,30 particularly in the hippocampus, and re- 15. Black S, Butcher K, Chambers LW, et al. Mind the connection. Preventing
ductions in hippocampal volume can be seen in depressed stroke and dementia. 2016 stroke report. Ottawa (ON): Heart and Stroke
J Psychiatry Neurosci 2018;43(2) 77
Albert
Foundation of Canada; 2016. Available: www.strokebestpractices.ca/ 25. Jin HJ, Pei L, Li YN, et al. Alleviative effects of fluoxetine on depressive-
wp-content/uploads/2016/06/HSF_StrokeReport2016_EN-Rev-1.pdf like behaviors by epigenetic regulation of BDNF gene transcription
(accessed 2018 Jan. 31). in mouse model of post-stroke depression. Sci Rep 2017;7:14926.
16. Brookes RL, Herbert V, Lawrence AJ, et al. Depression in small- 26. Vahid-Ansari F, Albert PR. Chronic fluoxetine induces activity
vessel disease relates to white matter ultrastructural damage, not changes in recovery from poststroke anxiety, depression, and cogni-
disability. Neurology 2014;83:1417-23. tive impairment. Neurotherapeutics 2017.
17. Hakim AM. Depression, strokes and dementia: new biological in- 27. Vahid-Ansari F, Albert PR et al. Persistent post-stroke depression
sights into an unfortunate pathway. Cardiovasc psychiatry neurol in mice following unilateral medial prefrontal cortical stroke. Transl
2011;2011:649629. Psychiatry 2016;6:e863.
18. Milev RV, Giacobbe P, Kennedy SH, et al. Canadian Network for 28. Rajkowska G, Miguel-Hidalgo JJ, Wei J, et al. Morphometric evidence
Mood and Anxiety Treatments (CANMAT) 2016 clinical guide- for neuronal and glial prefrontal cell pathology in major depression.
lines for the management of adults with major depressive disor- Biol Psychiatry 1999;45:1085-98.
der: section 4. Neurostimulation treatments. Can J Psychiatry 2016; 29. Mechawar N, Savitz J. Neuropathology of mood disorders: Do we
61:561-75. see the stigmata of inflammation? Transl Psychiatry 2016;6:e946.
19. Chollet F, Tardy J, Albucher JF, et al. Fluoxetine for motor recov- 30. McEwen BS. Stress and hippocampal plasticity. Annu Rev Neurosci
ery after acute ischaemic stroke (FLAME): a randomised placebo- 1999;22:105-22.
controlled trial. Lancet Neurol 2011;10:123-30. 31. MacQueen GM, Campbell S, McEwen BS, et al. Course of illness,
20. Mead GE, Hsieh CF, Lee R, et al. Selective serotonin reuptake in- hippocampal function, and hippocampal volume in major depres-
hibitors (SSRIs) for stroke recovery. Cochrane Database Syst Rev sion. Proc Natl Acad Sci U S A 2003;100:1387-92.
2012;11:Cd009286. 32. Anisman H. Cascading effects of stressors and inflammatory im-
21. Rush AJ, Warden D, Wisniewski SR, et al. STAR*D: revising con- mune system activation: implications for major depressive disorder.
ventional wisdom. CNS Drugs 2009;23:627-47. J Psychiatry Neurosci 2009;34:4-20.
22. Mortensen JK, Larsson H, Johnsen SP, et al. Impact of prestroke 33. Anrather J, Iadecola C. et al. Inflammation and stroke: an overview.
selective serotonin reuptake inhibitor treatment on stroke severity Neurotherapeutics 2016;13:661-70.
and mortality. Stroke 2014;45:2121-3. 34. Dinan TG. Inflammatory markers in depression. Curr Opin Psychiatry
23. Scheitz JF, Turc G, Kujala L, et al. Intracerebral hemorrhage and 2009;22:32-6.
outcome after thrombolysis in stroke patients using selective 35. Evans DL, Charney DS, Lewis L et al. Mood disorders in the med
serotonin-reuptake inhibitors. Stroke 2017;48:3239-44. ically ill: scientific review and recommendations. Biol Psychiatry 2005;
24. Kronenberg G, Gertz K, Heinz A, et al. Of mice and men: model- 58:175-89.
ling post-stroke depression experimentally. Br J Pharmacol 2014; 36. Hakim AM. Perspective: silent, but preventable, perils. Nature
171:4673-89. 2014;510:S12.
Reprint-half-horizontal.pdf 1 2018-02-14 3:30 PM
REPRINTS HOMELESS PEOPLE
WITH MENTAL ILLNESS
from the CMAJ Group
Cost of services for
homeless people with
mental illness in
5 Canadian cities
Going to a conference?
Teaching a course?
Need extra copies?
Contact Sheridan Press
1-800-635-7181 ext. 8065
marcus.glover@sheridan.com
www.sheridan.com/cma/eoc
20170006
78 J Psychiatry Neurosci 2018;43(2)
Research Paper
Grey matter correlates of autistic traits in women
with anorexia nervosa
Malin Björnsdotter, MSc, PhD;* Monika Davidovic, MSc, MD, PhD;*
Louise Karjalainen, MSc, PhD; Göran Starck, MSc, PhD; Håkan Olausson, MD, PhD;
Elisabet Wentz, MD, PhD
Background: Patients with anorexia nervosa exhibit higher levels of behaviours typically associated with autism-spectrum disorder
(ASD), but the neural basis is unclear. We sought to determine whether elevated autistic traits in women with anorexia nervosa may be
reflected in cortical morphology. Methods: We used voxel-based morphometry (VBM) to examine regional grey matter volumes in
high-resolution MRI structural brain scans in women with anorexia nervosa and matched healthy controls. The Autism-spectrum Quo-
tient (AQ) scale was used to assess autistic traits. Results: Women with anorexia nervosa (n = 25) had higher AQ scores and lower bi-
lateral superior temporal sulcus (STS) grey matter volumes than the control group (n = 25). The AQ scores correlated negatively with
average left STS grey matter volume in women with anorexia nervosa. Limitations: We did not control for cognitive ability and exam-
ined only women with ongoing anorexia nervosa. Conclusion: Elevated autistic traits in women with anorexia nervosa are associated
with morphometric alterations of brain areas linked to social cognition. This finding provides neurobiological support for the behavioural
link between anorexia nervosa and ASD and emphasizes the importance of recognizing autistic traits in preventing and treating
anorexia nervosa.
Introduction with anorexia nervosa also meet the criteria for ASD,11,15 and
the prevalence of ASD is higher in populations affected by
Anorexia nervosa is a severe psychiatric disorder that pre- eating disorders.16
dominantly affects young women.1 Although the diagnosis is Despite the large and growing body of research showing
defined by restricted eating and disturbed body perception,2 behavioural and cognitive ASD-like traits in women with
converging research links anorexia nervosa to a wide range anorexia nervosa, the neural correlates of elevated autistic
of poorly understood behavioural alterations.3 Specifically, traits in women with anorexia nervosa are poorly under-
behavioural risk factors typically associated with autism- stood. However, recent research links anorexia nervosa to
spectrum disorder (ASD) are consistently found in patients specific alterations in social cognition typically associated
with anorexia nervosa.4 For instance, affected women typ with ASD, such as impaired understanding of other people’s
ically exhibit perfectionism, particularly regarding symmetry mental states, or theory of mind (ToM).17–21 Although only a
and exactness,5 obsessive–compulsiveness, low cooperative- handful of studies have examined the neural basis of altered
ness, low novelty-seeking, impaired social cognition6,7 and sociocognitive function in patients with anorexia nervosa,22–25
set-shifting difficulties.8 Moreover, a large number of studies studies specifically targeting ToM processes have identified
have found persistently elevated levels of autistic traits in pa- reduced activity in brain circuits associated with social cogni-
tients with anorexia nervosa,4,7,9–13 and autistic traits and eat- tion,26 including the superior temporal cortex25 and temporo-
ing disorder behaviours are correlated in typically develop- parietal junction (TPJ).22,23 Consistently, a relatively large
ing children.14 In fact, a relatively high proportion of women number of studies have identified grey matter reductions of
Correspondence to: M. Björnsdotter, Department of Clinical Neuroscience, Karolinska Institutet, Nobels Väg 9, 171 77 Stockholm, Sweden;
malin.bjornsdotter@gmail.com
*These authors contributed equally to this work.
Submitted Apr. 7, 2017; Revised June 27, 2017; Accepted July 11, 2017; Online first Dec. 7, 2017
DOI: 10.1503/jpn.170072
© 2018 Joule Inc. or its licensors
J Psychiatry Neurosci 2018;43(2) 79
Björnsdotter et al.
the temporal lobe in patients with anorexia nervosa.27–29 Data processing
These findings echo findings of temporal cortex alterations in
patients with ASD,30 including alterations of the superior Structural brain images were processed using the VBM8 pack-
temporal sulcus (STS) and the TPJ.31–33 age in SPM8 (Wellcome Trust Centre for Neuroimaging, Insti-
In the present study, we sought to determine whether ele- tute of Neurology, www.fil.ion.uncl.ac.uk/spm) including the
vated autistic traits in women with anorexia nervosa may be VBM8 toolbox (http://dbm.neuro.uni-jena.de/vbm/) in
reflected in morphometric brain alterations. Specifically, we MATLAB 2014a (The MathWorks). Processing involved spa-
examined focal alterations in cortical grey matter volume tial normalization into Montreal Neurological Institute (MNI)
through voxel-based morphometry (VBM) analyses of struc- template space using the high-dimensional diffeomorphic
tural brain scans. As deficit ToM is a classical symptom of anatomic registration through exponentiated lie algebra
ASD30 and because brain regions linked to ToM are altered in (DARTEL) method with a final voxel size of 1.5 × 1.5 ×
patients with anorexia nervosa22–25 and those with ASD,31–33 1.5 mm3; segmentation into grey matter, white matter and
we hypothesized that autistic traits in women with anorexia cerebrospinal fluid; and modulation by the nonlinear com
nervosa would correlate with grey matter volume of regions ponent only for volume changes during spatial normalization
associated with ToM. to identify regional differences in grey matter volume cor-
rected for individual brain size. The spatially normalized and
Methods modulated grey matter partitions were smoothed with an iso-
tropic 8 mm full-width at half-maximum (FWHM) Gaussian
Participants kernel. Finally, we computed an average of all participants’
normalized structural scans for visualization of the results.
Patients with anorexia nervosa aged 16–25 years were re-
cruited consecutively from the in- and outpatient specialist Theory of mind region of interest analyses
Anorexia-Bulimia unit at the Queen Silvia Children’s Uni-
versity Hospital in Gothenburg, Sweden. At first assess- To specifically test the hypothesis that autistic traits in
ment by a psychiatrist, all patients received a diagnosis of women with anorexia nervosa correlate with grey matter vol-
anorexia nervosa according to DSM-IV. Patients with any ume of regions associated with ToM, we defined a set of in-
neurologic disorder were excluded. All healthy partici- dependent ToM regions of interest (ROIs). Here, we used
pants were asked to report neurologic disorders, ongoing Neurosynth software (neurosynth.org) to conduct a reverse
diseases and medications using a written questionnaire, inference meta-analysis of previously published studies with
and ongoing eating disorders were assessed using the the predefined search term “theory mind.” This process iden-
Structured Clinical Interview (SCID-I) for DSM-IV. Inclu- tified all studies indexed by the software that mentioned the
sion criteria for matched control participants were no search term “theory mind” at least once in the abstract, as per
ongoing eating disorders, no neurologic disorders, no on- the default procedure. All voxels of the reverse inference
going diseases and no medication. Depressive symptoms map passing the default threshold of a false-discovery rate
were assessed in all patients using the Beck Depression In- (FDR) of 0.01 were included in the set of ROIs.
ventory (BDI). The Regional Ethical Review Board at the
University of Gothenburg approved the study (registration Group difference analyses
number 007–14), and all participants gave written informed
consent. We conducted a voxel-wise general linear model (GLM)
analysis to identify brain regions exhibiting group differences
Assessment of autistic traits between women with anorexia nervosa and healthy control
participants. Because brain regions linked to social cognition,
We assessed the level of autistic traits in all participants including temporal cortex areas such as the TPJ, mature dur-
by administering the Autism-spectrum Quotient (AQ) ing adolescence,35 we included age as a covariate. The results
questionnaire.34 were assessed using nonparametric permutation testing clus-
terwise inference as implemented in the Statistical Non
Magnetic resonance imaging Parametric Mapping toolbox (http://warwick.ac.uk/snpm),
with a cluster-forming threshold of 0.005 and a family-wise
Structural brain scans were collected using a Philips error (FWE) of 0.05. Given our a priori hypothesis, we as-
Gyroscan 3 T Achieva scanner, software release 3.2. The sessed the results within the predefined ROIs.
scanner’s 2-channel parallel transmit was used for improved
signal homogeneity over the field of view, and the partici- Correlation analyses
pant’s head was firmly supported with cushions in the head
coil (32-channel SENSE, Philips). The T1-weighted scan (3D To assess associations between autistic traits and grey matter
T1–turbo field echo [TFE]) was obtained using the following volume in women with anorexia nervosa, we extracted indi-
parameters: flip angle 8º, echo time (TE) 4.0 ms, repetition vidual average grey matter volumes from areas exhibiting
time (TR) 8.4 ms, SENSE factor 2.7, TFE factor 240, 170 sagit- significant group differences using the MarsBaR toolbox
tal slices with a scan resolution of 1.0 × 1.0 × 1.0 mm3. (http://marsbar.sourceforge.net/) and computed the Pearson
80 J Psychiatry Neurosci 2018;43(2)Neural correlates of autistic traits in anorexia
linear correlation coefficient between grey matter volumes participants. No participant reported substance abuse, and
and AQ scores while controlling for age. no healthy participant reported any neurologic disorder, on-
going disease (including eating disorder) or medication use.
Control analyses
Assessment of autistic traits
We conducted a number of control analyses to examine
whether any observed effects may have been due to general Women with anorexia nervosa had significantly higher levels
grey matter loss in women with anorexia nervosa rather of autistic traits than control participants (AQ score group
than to social cognition processes. First, we examined total mean 16.60 ± 6.73 v. 11.64 ± 6.82, p = 0.010). There was a strong
grey matter across the entire brain volume and assessed positive association between AQ and BDI scores in women
group differences as well as associations with AQ. Second, with anorexia nervosa (r = 0.53, p = 0.006), but not in control
we replicated the analyses described previously within re- participants (r = 0.24, p = 0.24). The AQ score did not correlate
gions reliably associated with grey matter loss in patients with BMI in patients (r = 0.24, p = 0.25) or control participants
with anorexia nervosa, as reported in a recent meta- (r = –0.01, p = 0.95), and there was no association between AQ
analysis:29 namely, the hypothalamus, the left inferior pari- and duration of illness in patients (r = –0.09, p = 0.67).
etal lobule, the right putamen and the right caudate. These
regions were anatomically identified using the Automated Theory of mind region of interest definition
Anatomic Labelling (AAL) system in the WFU pickatlas
(www.nitrc.org/projects/wfu_pickatlas/). Since the hypo- The Neurosynth search yielded 140 studies (Appendix 1,
thalamus is not defined in AAL, we constructed an ROI as a Table S1, available at jpn.ca/170072-a1). The resulting reverse
10 mm sphere centred on the coordinates reported in the inference meta-analysis map revealed a set of ROIs consis-
meta-analysis,29 converted from Talairach to MNI space tently associated with ToM processes (pFDR < 0.01), including
using GingerAle (www.brainmap.org/ale/; resulting MNI the bilateral superior temporal cortex extending into the TPJ,
coordinates: x, y, z = –1, –3, –16). and medial frontal areas (Appendix 1, Fig. S1 and Table S2).
Whole brain analyses Theory of mind region of interest analyses
We conducted 2 exploratory whole brain analyses. First, we The ToM ROI analysis revealed 2 regions with significantly
searched for group differences between women with anorexia reduced grey matter volume in women with anorexia ner-
nervosa and healthy control participants. Second, we exam- vosa relative to control participants (p < 0.005, k ≥ 293): the
ined correlations between grey matter volume and AQ scores left (MNI coordinates: x, y, z = –60.00, –55.50, 12.00; t = 3.66,
only in women with anorexia nervosa. Again, the analysis in- 706 voxels) and right STS (MNI coordinates: x, y, z = 46.50,
cluded age as a covariate and the results were assessed on the –43.50, 19.50; t = 3.99, 503 voxels), extending into the TPJ
basis of nonparametric cluster-wise inference, with a cluster- (Fig. 1A). No region exhibited increased grey matter volume
forming threshold of 0.005 and cluster-based correction for in patients relative to control participants.
multiple comparisons such that pFWE < 0.05. In addition, we re- We found a negative association between AQ score and
ported any results passing the cluster-forming threshold of average grey matter volume extracted from the left (r =
p < 0.005 located near any of the ToM or control ROIs. –0.41, p = 0.045), but not the right (r = –0.03, p = 0.90), STS
region in women with anorexia nervosa (Fig. 1B). Post hoc
Results analyses showed that grey matter volumes did not correlate
with BMI (all p > 0.25); however, when controlling for BMI,
Demographic characteristics the strength of the association between AQ score and left
STS grey matter was reduced (r = –0.38, p = 0.08) whereas
A total of 37 patients were asked to participate, and 25 pa- the right hemisphere correlation was marginally strength-
tients accepted. Thus, the final sample consisted of 50 female ened (r = –0.07, p = 0.76)
participants aged 16–25 years: 25 with anorexia nervosa and
25 healthy controls (Table 1). All patients with anorexia ner-
vosa had a body mass index (BMI) of 17.5 kg/m2 or lower, as Table 1: Demographic and clinical characteristics of study participants
measured at the unit. All patients with anorexia nervosa Group; mean ± SD
were medically stable at the time of scanning, and 1 patient
was admitted to a psychiatric ward. Twelve patients were Anorexia nervosa, Control,
Characteristic n = 25 n = 25 p value
not medicated, and the rest used the following psychoactive
Age, yr 20.32 ± 2.23 21.28 ± 2.11 0.12
medications: fluoxetine (n = 6), sertraline (n = 4), olanzapine
(n = 2), quetiapine (n = 1), venflaxine (n = 1), propiomazine (n BMI 16.28 ± 0.93 21.13 ± 2.27 < 0.001
= 4), lamotrigine (n = 1) and lisdexametafine (n = 1). Four pa- BDI 26.88 ± 13.06 7.76 ± 7.33 < 0.001
tients had the binge-eating/purging type of anorexia nervosa Duration of 4.14 ± 3.54 — —
illness, yr
and the rest had the restrictive type. Patients had signifi-
BDI = Beck Depression Inventory; BMI = body mass index; SD = standard deviation.
cantly lower BMI and higher depression scores than control
J Psychiatry Neurosci 2018;43(2) 81Björnsdotter et al.
Whole brain analyses els). In the left inferior parietal lobule, 2 clusters passed the
cluster-forming threshold of p < 0.005, but these were too
The group difference analysis did not reveal any additional small to pass the cluster threshold of k ≥ 145 (x, y, z = –25.5,
significantly altered regions on the whole brain level (p < –66, 42; t = 3.08, 29 voxels, and x, y, z = –37.5, –63, 51; t = 3.45,
0.005, k ≥ 2464; Fig. 2). 88 voxels). In the caudate, 2 clusters passed the cluster-
The whole brain search for correlations with AQ score did forming threshold, but none were near the cluster threshold
not yield any significant results at the predetermined statis of k ≥ 44 voxels (x, y, z = 4.5, 6, –6; t = 2.84, 2 voxels, and x, y,
tical threshold (p < 0.005, k ≥ 2484). However, we found z = 6, 21, –1.5; t = 2.72, 2 voxels).
2 clusters of voxels located near the predetermined ROIs that Average grey matter extracted from these clusters did not
passed the uncorrected threshold of p < 0.005 in the left and correlate with AQ score in patients with anorexia nervosa
right TPJ (left: x, y, z = –45.00, –63.00, 30.00; peak uncorrected (putamen: r = 0.26, p = 0.23; hypothalamus: r = 0.01, p = 0.98;
p = 0.003, t = –3.03, 6 voxels; right: x, y, z = 45.00, –54.00, 28.50; inferior parietal cortex: r = –0.03, p = 0.88; caudate: r = –0.03,
peak uncorrected p = 0.003, t = –3.05, 7 voxels; Fig. 3). p = 0.90), and the whole brain voxel-wise search for correla-
tions with AQ score did not identify any voxels that passed
Control analyses the uncorrected threshold of p < 0.005 within or near any of
these ROIs (p < 0.005, k ≥ 2484).
The control analysis showed that total grey matter volume did
not differ significantly between women with anorexia nervosa Discussion
and control participants (p = 0.38) and did not correlate with
AQ score in women with anorexia nervosa (p = 0.48). We searched for neuromorphometric correlates of autistic
Also, the control analyses revealed significantly reduced traits in women with anorexia nervosa and hypothesized that
grey matter of the right putamen (p < 0.005, k ≥ 46; x, y, z = these would be found in brain regions associated with social
33.00, 3.00, 1.50; t = 3.21, 240 voxels) and the hypothalamus cognition and ToM. The results confirmed our hypothesis:
(p < 0.005, k ≥ 27; x, y, z = –3.00, 3.00, –9.00; t = 3.38, 82 vox- grey matter volume of the STS was reduced bilaterally in
A R 0.75 Controls
Average grey matter
Anorexia nervosa
0.70
0.65
–50 48
20
0.60
Left Right
B 0.75
Average grey matter volume
0.65
0.55
r = –0.41 r = –0.03
p = 0.045 p = 0.902
0.45
5 10 15 20 25 30 35 5 10 15 20 25 30 35
Autism-spectrum quotient Autism-spectrum quotient
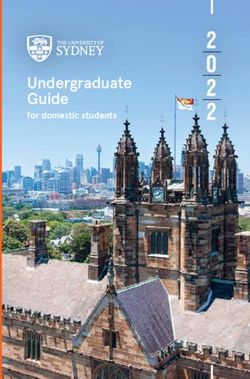
Fig. 1: Grey matter correlates of autistic traits in women with anorexia nervosa. (A) Significant grey matter reductions within
theory of mind regions of interest in women affected by anorexia nervosa compared with healthy control participants (cluster-
level corrected p < 0.05). (B) Inverse association between autistic traits in women with anorexia nervosa and left, but not right,
superior temporal grey matter volumes extracted from the group contrast. Coordinates refer to the Montreal Neurological Institute
(MNI) atlas space, the results are displayed in neurologic convention on a group average brain, error bars indicate standard error,
and the dotted lines indicate the 95% confidence bounds.
82 J Psychiatry Neurosci 2018;43(2)Neural correlates of autistic traits in anorexia
women with anorexia nervosa, and average left STS grey mat- ticipants adds to the growing body of studies observing be-
ter showed a weak but significant negative correlation with havioural overlaps between anorexia nervosa and ASD.4,7,10,13–15
AQ scores. In addition, we found a trend toward a correlation Our results are also consistent with the extensive literature
between TPJ grey matter volume and autistic traits bilaterally. on structural brain alterations in anorexia nervosa.27,29,36–45
The finding that patients with anorexia nervosa exhibited Specifically, previous structural brain studies found grey
significantly higher levels of autistic traits than control par matter reductions of the temporal lobe in patients with
R
–6 T 6
–48 48
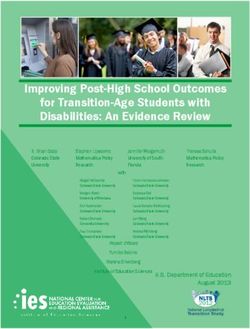
Fig. 2: Whole brain grey matter reductions in women with anorexia nervosa compared with healthy control participants. The un-
thresholded group difference T-map is overlaid on a group average brain. Positive values indicate voxels where control partici-
pants show increased grey matter compared with women with anorexia nervosa, and vice versa for negative values. Coordinates
indicate X axis cuts to reveal deeper structures, shown in Montreal Neurological Institute (MNI) atlas space. The dotted line indi-
cates the superior temporal sulcus. R = right hemisphere.
Left TPJ Right TPJ
0.90
Grey matter volume
0.70
0.50
0.30
–45 +45
5 10 15 20 25 30 35 5 10 15 20 25 30 35
Autism-spectrum quotient Autism-spectrum quotient
Fig. 3: Association between autistic traits and temporoparietal grey matter volume. Inverse association between autistic traits in
women with anorexia nervosa and temporoparietal junction (TPJ) grey matter volume identified in the whole brain search (at un-
corrected p < 0.005; note that these clusters did not meet the family-wise error–corrected cluster-forming threshold of k ≥ 2484).
The data indicate the cluster mean grey matter volumes, coordinates refer to the Montreal Neurological Institute (MNI) atlas
space, and the dotted lines indicate the 95% confidence bounds.
J Psychiatry Neurosci 2018;43(2) 83Björnsdotter et al. anorexia nervosa,27,28 and a recent activation likelihood esti- patients with ASD.51,53 Indeed, the results from the meta- mation (ALE) meta-analysis showed that the temporal lobe analysis revealed largely symmetric bilateral regions, but with consistently exhibits reduced regional grey matter in patients a larger right (3540 voxels) than left (2530 voxels) STS area. with anorexia nervosa.29 Our results are further supported by However, the lateralization of ToM processing is mixed. For functional MRI studies that found reduced activations of instance, a study of adults with brain damage suggests that brain regions linked to social cognition, including the super the left TPJ is critical for functional ToM processes.54 Also, cor- ior temporal cortex25 and TPJ,22,23 in patients with anorexia tical TPJ thinning during adolescence is localized to the left nervosa. Additionally, increased functional connectivity in hemisphere.35 Nevertheless, we observed bilateral STS grey the left angular gyrus, located near the TPJ, has been noted in matter reductions in women with anorexia nervosa and found patients with ongoing anorexia nervosa.46 Finally, the control trends toward associations between TPJ grey matter volume analyses showed that the women with anorexia nervosa had and autistic traits bilaterally. Any lateralization should there- significantly reduced grey matter of the putamen and the hy- fore be interpreted with caution, and further studies in larger pothalamus, replicating findings of robust grey matter altera- samples are required to confirm such effects. tions in patients with anorexia nervosa.29 Corroborating studies showing a link between autistic Morphological brain alterations are largely ubiquitous in traits and depression,12 the AQ measure was strongly associ- patients with anorexia nervosa,4,7,10,13–15 leaving the possibility ated with BDI scores in patients with anorexia nervosa. This that the observed association between autistic traits and grey finding highlights the question of whether depression may matter volume may be a generalized effect of grey matter loss influence autistic traits or vice versa12 and emphasizes the due to the illness. However, the whole brain search for asso- need for future research into the nature of the association be- ciations with AQ scores did not reveal any additional areas tween the 2 measurements. The finding also raises the possi- showing a similar effect, and grey matter volume in regions bility that depression could contribute to the observed mor- known to be affected in patients with anorexia nervosa did phological alterations. Indeed, subclinical depression is not correlate with AQ score. Moreover, AQ score was not as- associated with altered grey matter volume of the temporal sociated with whole brain grey matter volume. Taken to- cortex;55 however, the opposite pattern of increased grey mat- gether, these control analyses therefore suggest that the iden- ter with higher depression scores was found, speaking tified association between autistic traits and grey matter against a confounding effect of depression on the results of volume of social cognition areas does not reflect general loss the present study. of grey matter in women with anorexia nervosa. Instead, the results suggest that autistic traits may be specifically linked Limitations to temporal lobe grey matter morphology. Although the literature on grey matter alterations in A limitation of this work is that we did not control for cogni- patients with ASD is highly inconsistent,47–49 superior tem- tive ability in women with anorexia nervosa; however, cogni- poral grey matter decreases have been observed in high- tive ability is not generally affected in patients with this dis- functioning individuals with ASD.50 This suggests the pos- order56 and is unlikely to have had any substantial impact on sibility that elevated autistic traits in patients with anorexia the results. An additional limitation is that we examined only nervosa may share similarities with high-functioning pa- patients with ongoing anorexia nervosa; hence, low body tients with ASD. However, the majority of ASD studies weight and associated factors may have contributed to the have been conducted mainly with male participants, and observed grey matter alterations. Indeed, we found that con- recent findings highlight puzzling sex differences in brain trolling for BMI reduced the association between grey matter structure and function in patients with ASD. Specifically, in the left STS and AQ scores, suggesting that body weight STS responses to social cues are altered in male but not in may play a role. Also, the broad structural grey matter abnor- female patients with ASD,51 and bilateral superior temporal malities found in patients with acute anorexia nervosa gener- cortex volume is greater in female than in male patients ally normalizes as patients recover.57 However, 2 studies re- with ASD and in typically developing participants.52 Nota- ported remaining grey matter reductions of the left angular bly, healthy girls exhibit a higher rate of cortical thinning of gyrus, part of the TPJ, after weight recovery,58,59 raising the social brain regions during adolescence than boys, includ- possibility that the observed alterations may be persistent. ing thinning of the right temporal cortex and the left TPJ.35 Further studies in weight-recovered women are required to Our findings raise the possibility that adolescent onset of establish whether this is the case. As socioemotional impair- anorexia nervosa may be linked to such cortical develop- ments may be perpetuated by the illness — for instance, ments. However, further studies directly comparing boys chronic anorexia nervosa can lead to ASD-like symp- and girls with anorexia nervosa are required to character- toms60,61 — such studies are particularly important. ize shared and distinct alterations; this is a particularly dif- ficult challenge given the low prevalence of anorexia ner- Conclusion vosa in boys. We found correlations with AQ score primarily in the left With its limitations in mind, this study shows that elevated hemisphere. Alterations in social perception processes, in- autistic traits in women with anorexia nervosa are associ- cluding processing of stimuli such as biological motion, are ated with morphometric alterations of brain areas linked to primarily associated with right hemisphere STS alterations in social cognition. This finding provides neurobiological 84 J Psychiatry Neurosci 2018;43(2)
Neural correlates of autistic traits in anorexia
s upport for the behavioural link between anorexia nervosa 6. Cassin SE, von Ranson KM. Personality and eating disorders: a
ecade in review. Clin Psychol Rev 2005;25:895-916.
d
and ASD4,7,9–13 and raises the possibility that neurobiological 7. Zucker NL, Losh M, Bulik CM, et al. Anorexia nervosa and autism
risk factors linked to autistic traits may contribute to an- spectrum disorders: guided investigation of social cognitive endo-
orexia nervosa in adolescent girls. Critically, further re- phenotypes. Psychol Bull 2007;133:976-1006.
search is required to disentangle predisposing and perpetu- 8. Westwood H, Stahl D, Mandy W, et al. The set-shifting profiles of an-
orexia nervosa and autism spectrum disorder using the Wisconsin
ating features of any such effect. Finally, our results have Card Sorting Test: a systematic review and meta-analysis. Psychol Med
important clinical implications: the observation that ele- 2016;46:1809-27.
vated autistic traits may be rooted in structural brain altera- 9. Baron-Cohen S, Jaffa T, Davies S, et al. Do girls with anorexia ner-
vosa have elevated autistic traits? Mol Autism 2013;4:24.
tions similar to those observed in patients with ASD sup- 10. Gillberg C, Råstam M. Do some cases of anorexia nervosa reflect
ports the notion that patients with anorexia nervosa may underlying autistic-like conditions? Behav Neurol 1992;5:27-32.
benefit from treatment schemes explicitly acknowledging 11. Mandy W, Tchanturia K. Do women with eating disorders who
ASD-like difficulties. For instance, treatment approaches have social and flexibility difficulties really have autism? A case
series. Mol Autism 2015;6:6.
used in patients with ASD, such as highly structured and 12. Tchanturia K, Smith E, Weineck F, et al. Exploring autistic traits in
concrete pedagogic methods or experimental pharmaco anorexia: a clinical study. Mol Autism 2013;4:44.
logical procedures such as oxytocin administration,62 may 13. Wentz E, Gillberg IC, Anckarsäter H, et al. Adolescent-onset an-
orexia nervosa: 18-year outcome. Br J Psychiatry 2009;194:168-74.
accelerate recovery in patients with anorexia nervosa who 14. Coombs E, Brosnan M, Bryant-Waugh R, et al. An investigation
exhibit high levels of autistic traits. into the relationship between eating disorder psychopathology and
autistic symptomatology in a non-clinical sample. Br J Clin Psychol
2011;50:326-38.
Acknowledgements: The authors thank the participants for making
15. Anckarsäter H, Hofvander B, Billstedt E, et al. The sociocommuni-
this study possible. They also thank the staff at the Anorexia-Bulimia cative deficit subgroup in anorexia nervosa: autism spectrum dis-
Unit, Queen Silvia Children’s Hospital for their continuous support. orders and neurocognition in a community-based, longitudinal
M. Björnsdotter was supported by the European Union Seventh study. Psychol Med 2012;42:1957-67.
Framework Program (FP7/2007-2013) under grant agreement PIOF- 16. Huke V, Turk J, Saeidi S, et al. Autism spectrum disorders in eat-
GA-2012-302896, The Söderström König Foundation, Linnea and ing disorder populations: a systematic review. Eur Eat Disord Rev
Joself Carlsson’s Foundation, the Fredrik och Ingrid Thuring Foun- 2013;21:345-51.
dation and O. E. och Edla Johanssons’ Foundation. L. Karjalainen 17. Gillberg IC, Billstedt E, Wentz E, et al. Attention, executive func-
was supported by the Wilhelm och Martina Lundgren Foundation. tions, and mentalizing in anorexia nervosa eighteen years after on-
The study was supported by ALF-Västra Götaland. set of eating disorder. J Clin Exp Neuropsychol 2010;32:358-65.
18. Jewell T, Collyer H, Gardner T, et al. Attachment and mentaliza-
Affiliations: From the Department of Clinical Neuroscience, Karolin- tion and their association with child and adolescent eating pathol-
ska Institutet, Stockholm, Sweden (Björnsdotter); the Centre for So- ogy: a systematic review. Int J Eat Disord 2016;49:354-73.
cial and Affective Neuroscience, Linköping University, Linköping, 19. Russell TA, Schmidt U, Doherty L, et al. Aspects of social cogni-
Sweden (Björnsdotter, Olausson); the Institute of Neuroscience and tion in anorexia nervosa: affective and cognitive theory of mind.
Physiology, University of Gothenburg, Gothenburg, Sweden Psychiatry Res 2009;168:181-5.
(Davidovic, Olausson); the Gillberg Neuropsychiatry Centre, Insti- 20. Tapajóz P, de Sampaio F, Soneira S, et al. Theory of mind and cen-
tute of Neuroscience and Physiology, University of Gothenburg, Go- tral coherence in eating disorders: two sides of the same coin?
thenburg, Sweden (Karjalainen, Wentz); the Department of Radiation Psychiatry Res 2013;210:1116-22.
Physics at the Institute of Clinical Sciences, University of Gothen- 21. Tapajóz Pereira de Sampaio F, Soneira S, Aulicino A, et al. Theory
burg, Gothenburg, Sweden (Starck); and the Department of Medical of mind in eating disorders and their relationship to clinical pro-
Physics and Biomedical Engineering, Sahlgrenska University Hospi- file. Eur Eat Disord Rev 2013;21:479-87.
tal, Gothenburg, Sweden (Starck). 22. McAdams CJ, Lohrenz T, Montague PR. Neural responses to kind-
ness and malevolence differ in illness and recovery in women with
Competing interests: None declared. anorexia nervosa. Hum Brain Mapp 2015;36:5207-19.
23. McAdams CJ, Krawczyk DC. Impaired neural processing of social
Contributors: M. Davidovic, G. Starck, H. Olausson and E. Wentz de- attribution in anorexia nervosa. Psychiatry Res 2011;194:54-63.
signed the study. M. Davidovic and L. Karjalainen acquired the data, 24. McAdams CJ, Krawczyk DC. Who am I? How do I look? Neural dif-
which M. Björnsdotter and M. Davidovic analyzed. M. Björnsdotter ferences in self-identity in anorexia nervosa. Soc Cogn Affect Neurosci
wrote the article, which all authors critically reviewed. All authors 2014;9:12-21.
approved the final version to be published and can certify that no 25. Schulte-Rüther M, Mainz V, Fink GR, et al. Theory of mind and
other individuals not listed as authors have made substantial contri- the brain in anorexia nervosa: relation to treatment outcome. J Am
butions to the paper. Acad Child Adolesc Psychiatry 2012;51:832-41.e11.
26. Gallagher HL, Frith CD. Functional imaging of “theory of mind.”
Trends Cogn Sci 2003;7:77-83.
References 27. Boghi A, Sterpone S, Sales S, et al. In vivo evidence of global and
focal brain alterations in anorexia nervosa. Psychiatry Res
1. Bulik CM, Sullivan PF, Tozzi F, et al. Prevalence, heritability, and Neuroimaging 2011;192:154-9.
prospective risk factors for anorexia nervosa. Arch Gen Psychiatry 28. Suchan B, Busch M, Schulte D, et al. Reduction of gray matter den-
2006;63:305-12. sity in the extrastriate body area in women with anorexia nervosa.
2. American Psychiatric Association. Diagnostic and Statistical Manual Behav Brain Res 2010;206:63-7.
of Mental Disorders (DSM-5®). Lake St. Louis (MO): American 29. Titova OE, Hjorth OC, Schiöth HB, et al. Anorexia nervosa is
Psychiatric Association; 2013. p. 1629. linked to reduced brain structure in reward and somatosensory re-
3. Kaye WH, Fudge JL, Paulus M. New insights into symptoms and gions: a meta-analysis of VBM studies. BMC Psychiatry 2013;13:110.
neurocircuit function of anorexia nervosa. Nat Rev Neurosci 2009; 30. Lai M-C, Lombardo MV, Baron-Cohen S. Autism. Lancet 2014;383:
10:573-84. 896-910.
4. Oldershaw A, Treasure J, Hambrook D, et al. Is anorexia nervosa a ver- 31. Dichter GS. Functional magnetic resonance imaging of autism
sion of autism spectrum disorders? Eur Eat Disord Rev 2011;19:462-74. spectrum disorders. Dialogues Clin Neurosci 2012;14:319-51.
5. Srinivasagam NM, Kaye WH, Plotnicov KH, et al. Persistent per- 32. Pelphrey KA, Shultz S, Hudac CM, et al. Research review: Con-
fectionism, symmetry, and exactness after long-term recovery straining heterogeneity: the social brain and its development in
from anorexia nervosa. Am J Psychiatry 1995;152:1630-4. autism spectrum disorder. J Child Psychol Psychiatry 2011;52:631-44.
J Psychiatry Neurosci 2018;43(2) 85You can also read