La gastroparesi vista dal diabetologo: quali problematiche e quali domande? - Dr.ssa Carla Greco
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
La gastroparesi vista dal
diabetologo:
quali problematiche e quali
domande?
Dr.ssa Carla Greco
Università di Modena e Reggio Emilia
Disclosure Statement La dr.ssa Carla Greco dichiara di NON aver ricevuto negli ultimi due anni compensi o finanziamenti da Aziende Farmaceutiche e/o Diagnostiche. Dichiara altresì il proprio impegno ad astenersi, nell’ambito dell’evento, dal nominare, in qualsivoglia modo o forma, aziende farmaceutiche e/o denominazione commerciale e di non fare pubblicità di qualsiasi tipo relativamente a specifici prodotti di interesse sanitario (farmaci, strumenti, dispositivi medico-chirurgici, ecc).
Agenda • Definition and epiemiology of diabetic gastroparesis • Phatophysiology of gastric motor functions • Diagnostic procedure of gastroparesis in diabetic patient • Behavioral and pharmacological therapeutic approach
X-rays: gastric studies after ingestion of the x-ray meal consisting of 4 ounces of barium sulphate and water.
Kassander P. Ann Intern Med 1958; 48(4):797-812.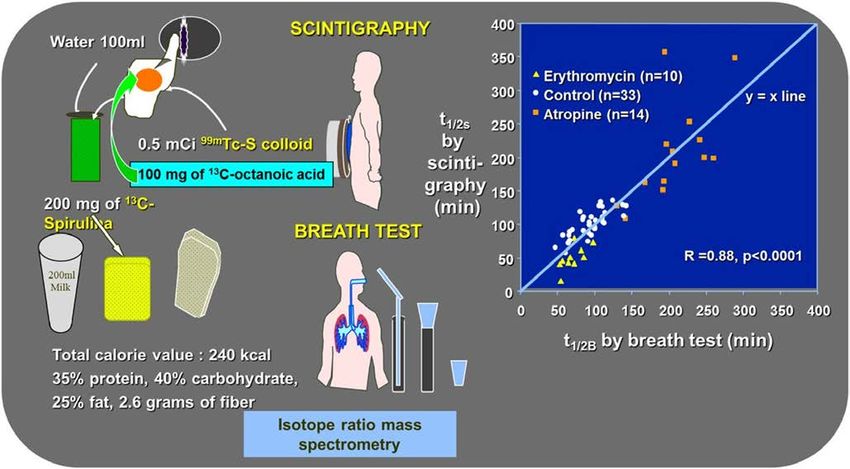
X-rays: gastric studies after ingestion of the x-ray meal consisting of 4 ounces of barium sulphate and water.
Kassander P. Ann Intern Med 1958; 48(4):797-812.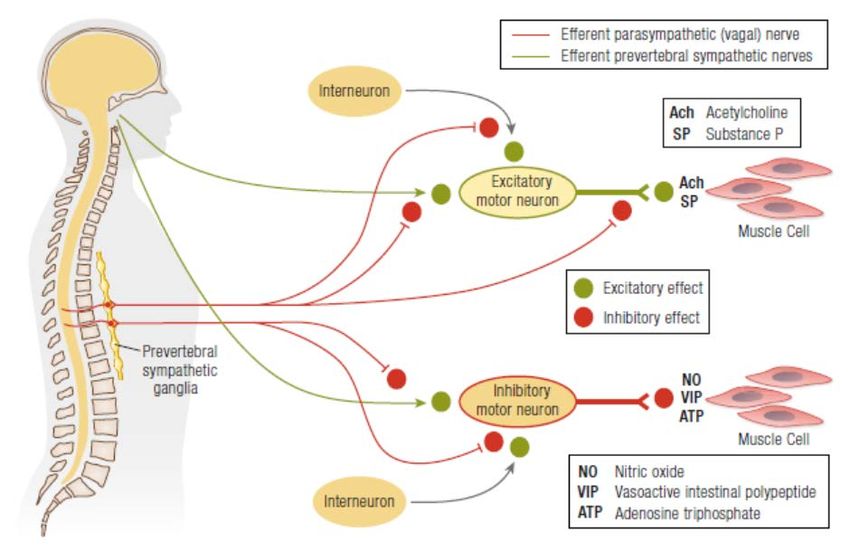
Diabetic gastroparesis: definition
*
Clinical syndrome characterized by delayed gastric emptying
in the absence of mechanical obstruction of the stomach in
diabetic patient.
Parkman HP et al. Gastroenterology 2004; 127:1589–91.
Camilleri M et al. Am J Gastroenterol 2013; 108:18–37.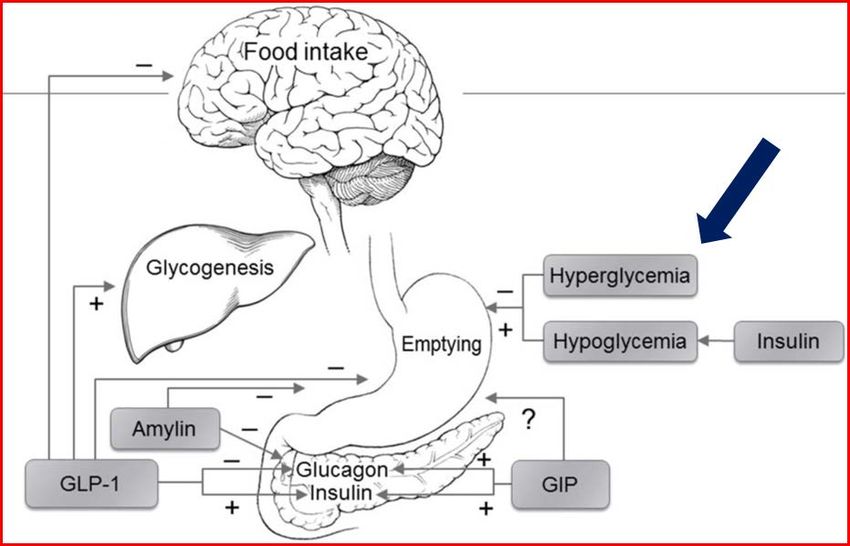
Community-Based Epidemiologic Studies
of GI Symptoms in DM
Study Population Upper GI Symptoms
Dyck et al, 1993 Residents of Rochester, MN Gastroparesis:
DM1 and DM2 0% DM1, 1% DM2
Janatuinen et al, 1993 Residents in a hospital district Symptoms of nausea and vomiting were
(481 DM2, 89 DM1 and 635 controls) not different between cases with DM
and controls
Maleki et al, 2000 Samples of Olmsted County residents No difference in stomach
(217 DM2, 138 DM1 and 388 controls) symptoms between DM and controls;
less heartburn reported by DM1 patients
Bytzer et al, 2001 Sample of people in Sydney, Australia Vomiting 1.7% vs 11% (OR 2.71)
Hammer et al, 2003 (402 DM2, 21 DM1 and 8132 controls) Upper gut dysmotility (when evaluated)
18.2% vs 15.3% (OR 1.75)
Choung et al, 2012 Follow up of samples of Olmsted County During 10 years, gastroparesis developed
residents, MN in 5.2% DM1, 1% DM2 and 0.2%
(409 DM2, 269 DM1 and 735 controls) controls.
HR 4.4; 95% CI, 1.1- 17 in DM1 than DM2
Aleppo et al, 2017 Multisite study of 7107 patients Clinical diagnosis of gastroparesis: 4.8%
(>26 years old with DM1 for >2 years) (women 5.8% vs men 3.5%)
All surveys, with the exception of Aleppo et al., used a mailed questionnaire. Modifyed by Bharucha AE et al. Endocr Rev 2019; 40(5):1318-1352.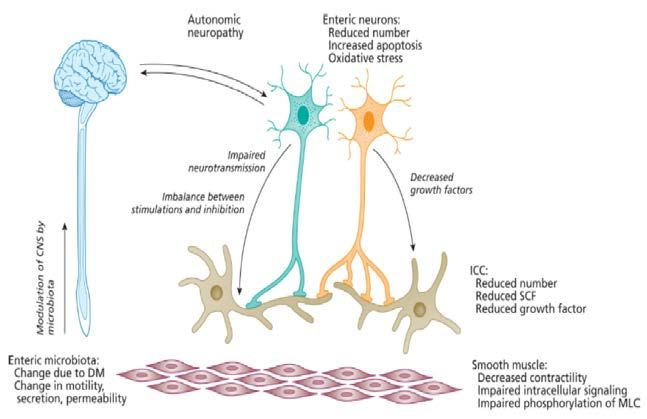
Definite Gastroparesis
Delayed gastric emptying by scintigraphy 3604 potential cases
and typical symptoms of gastroparesis
Probable Gastroparesis
Symptoms as above plus food retention 222
on endoscopy or an upper GI study 83 126
(not scintigraphy) definite
definite definite
plus
gastroparesis plus
Possible Gastroparesis probable/
Typical symptoms alone or delayed probable (43)
gastric emptying by scintigraphy in the 25.3% diabetes possible (96)
gastroparesis
absence of GI symptoms. 82% female gastroparesis
Incidence Gastroparesis in Olmsted County, 1996–2006 Prevalence Gastroparesis in Olmsted County, 1996–2006
Definite Definite & Definite & probable Definite Definite & Definite & probable
gastroparesis probable & possible gastroparesis probable & possible
gastroparesis gastroparesis gastroparesis gastroparesis
Female 9.8 14.2 22.3 Female 37.8 48.9 70.6
(95% CI) (7.5-12.1) (11.4-17) (18.7-25.9) (95% CI) (23.3-52.4) (32.2-65.7) (50.6-90.7)
Males 2.4 5.0 11.8 Males 9.6 15.3 27.9
(95% CI) (1.2-3.8) (3.2-6.9) (9-14.7) (95% CI) (1.8-17.4) (5.7-24.9) (14.4-41.4)
Total 6.3 9.8 17.2 Total 24.2 33.4 50.5
(95%) (4.9-7.7) (8.1-11.6) (14.9-19.5) (95%) (15.7-32.6) (23.3-43.4) (38.1-62.8)
Jung HK et al. Gastroenterology 2009; 136(4):1225-33.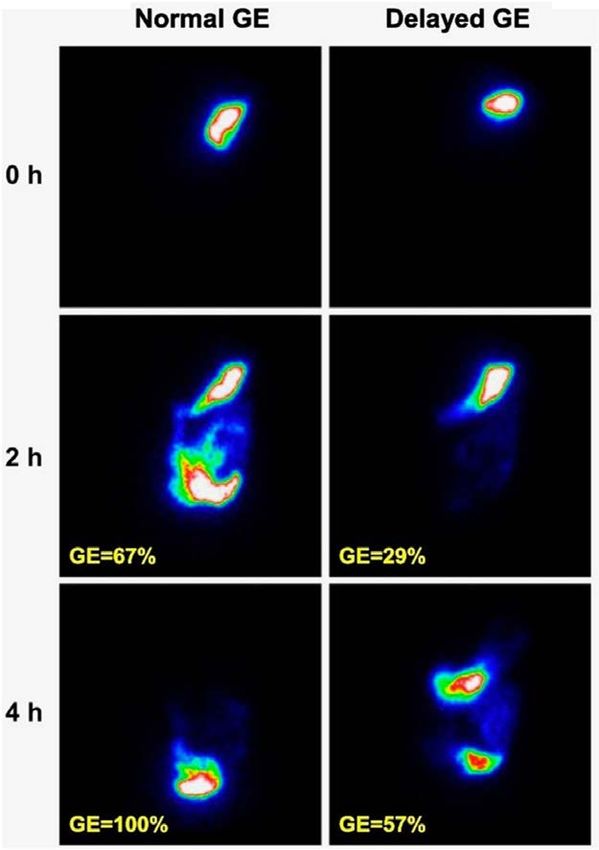
The cumulative proportions developing gastroparesis over a 10-year time period were
5.2% in type 1 DM, 1.0% in type 2 DM, and 0.2% in controls.
The age- and gender-adjusted hazard ratios (HR) for gastroparesis (relative to controls) was 33
(95% CI: 4.0–274) in type 1 DM and 7.5 (95% CI: 0.8–68) in type 2 DM.
The risk of gastroparesis in type 1 DM was significantly greater than in type 2 DM (HR: 4.4 [1.1,
17]).
Choung RS et al. Am J Gastroenterol 2012; 107(1):82-8.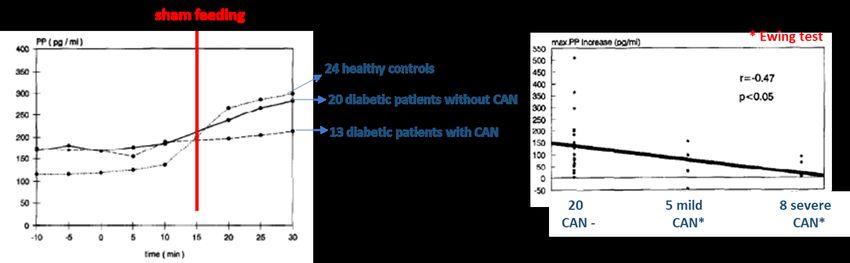
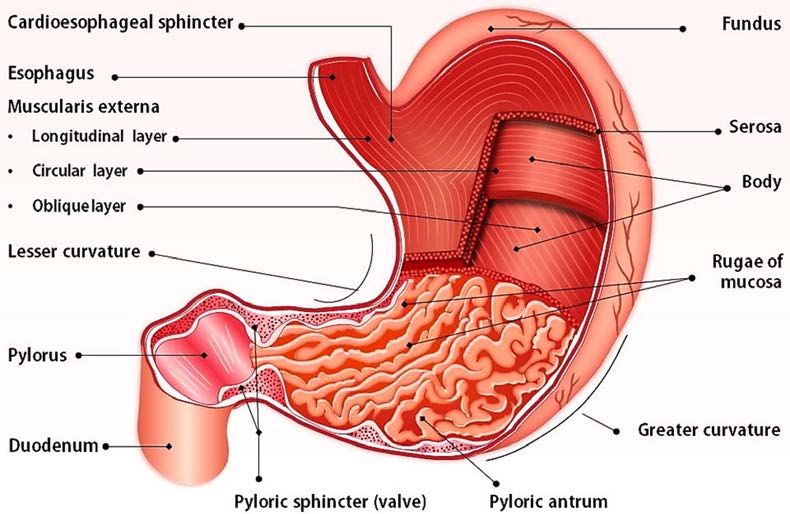
Physiology of gastric motor functions
Schematic representation of enteric and extrinsic mechanisms that control GI motility
Antegrade peristalsis proximal contraction mediated by excitatory neurotransmitters,
coordinated with distal relaxation mediated by inhibitory neurotransmitters
The sympathetic neural input can tonically inhibit antegrade peristalsis in the viscus and
stimulates tonic contraction of the sphincters
Bharucha AE et al. Endocr Rev 2019; 40(5):1318-1352.Physiology of gastric motor functions
Autonomic Nervous System (ANS)
Sympathetic nervous system
Parasympathetic nervous system (vagus)
Enteric Nervous System (ENS)
GASTRIC PACEMAKER Colinergic neurons of myenteric plexus
Interstitial cells of Cajal (ICCs) of Auerbach
Adrenergic neurons of myenteric plexus of
Auerbach and submucosal plexus of
Meissner
Interstitial cells of Cajal (ICCs)
Gastric pacemakerPhatophysiology of gastric motor functions
Damage to gastric neurons and ICCs in gastric biopsies in diabetic patients.
Faussone-Pellegrini MS et al. J Cell Mol Med 2012; 16:1573–81.
Alterations neurons and ICCs lack of fundus relaxation and reduced gastric capacity,
potentially responsible for dyspeptic symptoms He CL et al. Gastroenterology 2001; 121: 427–34.
Damage to ICCs tachyarrhythmia aberrant progression corpus-antrum
O’Grady G et al. Gastroenterology 2012; 143:589–98.
Yarandi SS et al. Neurogastroenterol Motil 2014; 26(5):611-24 .
Greco C. Published online. Giornale Italiano di Diabete e Metabolismo, 2019.
Modify by Koch KL et al. Gastroenterol Clin North Am 2015; 44(1):39-57.Autonomic dysfunction and GI motility disorder
Mayo Clinic, Rochester, MN, USA. Distribution of gastrointestinal motility scores.
January 1988 - July 1991
Pneumohydraulic perfusion manometry.
Supine and standing BP sympathetic adrenergic
function.
113 patients with HR and BP responses to the Valsalva manoeuvre
suspected GI sympathetic adrenergic function and vagal innervation.
motility disorders Sudomotor axon reflex test cholinergic sympathetic Distribution of autonomic function.
function.
HR responses to deep breathing vagal cholinergic
function.
Significant (pGastrointestinal vagal dysfunction
A subnormal plasma pancreatic polypeptide response during sham
feeding is associated with cardiovascular vagal dysfunction.
Glasbrenner B et al. Diabetes Res ClinPract 1995; 30(2):117–123.
Krishnasamy S et al. Diabetes Ther 2018; 9:1-42.Hyperglycemia and gastric emptying
Effect of hyperglycemia on plasma motilin concentration
Effect of hyperglycemia on antral phase III activity.
Acute hyperglycemia delays gastric emptying.
In contrast, insulin-induced hypoglycaemia accelerates gastric emptying even in diabetic
patients with gastroparesis.
Conflicting relationship between HbA1cand gastric symptoms among diabetic people.
Halland M et al. Clin Gastroenterol Hepatol 2016; 14(7):929-36.
Barnett JL et al. Gastroenterology 1988; 95(1):262.
Bharucha AE et al. Endocr Rev. 2019; 40(5):1318-1352.Glycemia and gastric emptying
42 T1DM patients without chronic complications and 31 controls evaluated by 13C-octanoate breath test.
T1DM patients showed a significantly slower GE T1/2 T1DM patients with delayed GE time showed a mean time-
value (113+34 min) than controls (89+17 min; P < 0.001). to-peak glucose significantly longer than that in patients
36% T1DM showed a delayed GE (T1/2>120 min), whereas with normal GE time (108+19 min in T1DM T1/2 > 120 min
all controls showed a normal GE (T1/2 < 120 min). vs 81+36 min in T1DM T1/2 > 120 min; P = 0.004).
Time-to-peak glucose directly related to the GE T1/2 (r = 0.424; P = 0.009).
After adjustment, GE T1/2 independent predictor of time-to-peak glucose (β = 0.329; P = 0.025), and GE T1/2
> 120 minutes independently associated with time-to-peak glucose > 120 minutes (OR 5.33; 95% CI, 1.16-
24.5; P = 0.031).
In the ROC analysis, time-to-peak glucose > 120 minutes identified 73% of patients with GE T1/2 > 120 min.
Lupoli R et al. JCEM 2018; 103:2269-2276.Clinical evaluation of gastric symptoms
When to start screening?...
Characteristic symptoms nausea/vomiting
gastric fullness and early satiety
bloating
Hypoglycemia-hyperglycemia blood glucose oscillations due to
incoordination between the
absorption of sugars and exogenous
insulin action or other antidiabetic
KetoacidosisClinical evaluation of gastric symptoms
Gastroparesis Cardinal Symptom Index (GCSI)
3 sub-scales:
• post-prandial fullness/early satiety (4 items)
• nausea/vomiting (3 items)
• bloating (2 items).
Revicki DA et al. Aliment Pharmacol Ther 2003; 18(1):141-50.
Revicki DA et al. Qual Life Res 2004; 13(4):833-44.Clinical evaluation of gastric symptoms
6 domains (31 items):
• Orthostatic intolerance Nell’ultimo anno ha notato dei cambiamenti nella comparsa del senso
di sazietà (sentirsi pieno) quando consuma un pasto?
• Vasomotor
Nell’ultimo anno le è capitato di sentirsi troppo pieno o pieno più a
• Secretomotor lungo (sensazione di gonfiore) dopo un pasto?
• Gastrointestinal Nell’ultimo anno le è capitato di vomitare dopo un pasto?
• Bladder
Nell’ultimo anno le è capitato di avere un dolore addominale come un
• Pupillomotor crampo o una colica?
Italian version
(six domain scores and a total score (range 0–100)
after appropriate weighting)
Sletten DM et al. Mayo Clin Proc 2012; 87: 1196–1201.
Pierangeli G et al. Neurol Sci 2015; 36(10):1897-902.
Greco C et al. Diabet Med 2017; 34(6):834-838.Evaluation of gastroparesis
Proposal diagnostic procedure of gastroparesis in diabetic patient
Clinical suspicion Characteristic symptoms
Hypoglycemia-hyperglycemia
Evaluation autonomic neuropathy Cardiovascolar tests
Exclude mechanical obstruction EGDS
Ex adiuvantibus therapy Prokinetic drugs for 4 weeks
Evaluation Gastric scintigraphy
Electrogastrography
Wireless capsule
13C-octanoic and –spirulina breath test
Modify by Greco C. Published online. Giornale Italiano di Diabete e Metabolismo, 2019.Instrumental evaluation
Gastric scintigraphy
99m Tc-radiolabeled EggBeaters (meal
with jam, toast and water) to perform
solid-phase.
Labeling of solid and liquid phases may
also be performed.
Gastric emptying is considered
delayed if there is greater than 60%
retention at 2 h or 10% retention at 4 h.
Camilleri M et al. Am J Gastroenterol 2013; 108:18–37.
Shin AS et al. Diabetes 2013; 62:2667–73.
Krishnasamy S et al. Diabetes Ther 2018; 9:1-42.Instrumental evaluation
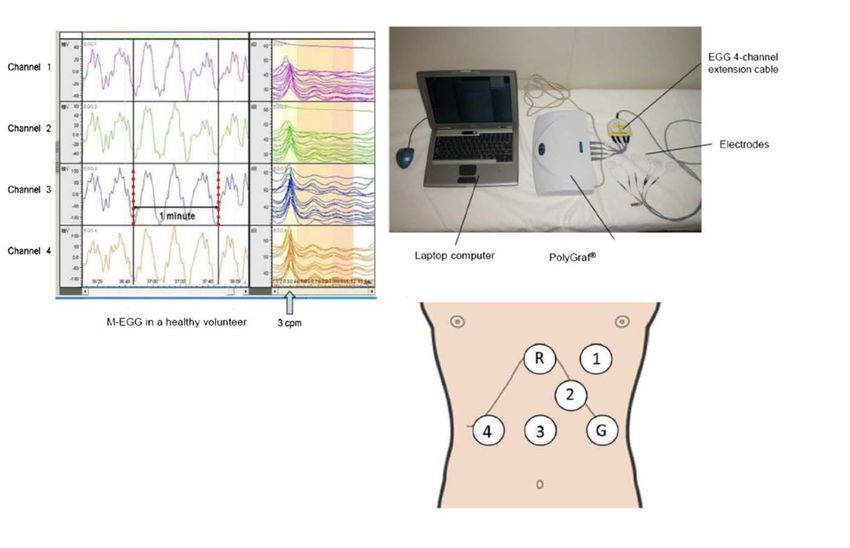
Electrogastrography (EGG)
High-resolution electrogastrogram is a
research tool that reveals abnormal
initiation and/or propagation of gastric
electrical activity.
Murakami H et al. J Smooth Muscle Res 2013; 49:78-88.Instrumental evaluation
13C-Octanoic breath test 13C-Spirulina breath test
Methods for GE assessment by breath test (T1/2B) and scintigraphy (T1/2S), and
corresponding correlation of T1/2 in erythromycin, control and atropine groups
showing a significant correlation between estimates (r = 0.88, P < 0.0001) based on
the multiple linear regression model.
Ziegler D et al. Diabetologia 1996; 39: 823–830.
Viramontes BE et al. Neurogastroenterol Motil 2001; 13(6):567-74.
Szarka LA et al. Clin Gastroenterol Hepatol 2008; 6:635-643.
GEBT, Gastric Emptying Breath Test Shin AS et al. Diabetes 2013; 62:2667–73.Instrumental evaluation
Wireless Motility Capsule (WMC)
Ingestion of non-digestible capsule capable
of measuring temperature, pH and the
pressure of its immediate surroundings
allows for the measurement of gastric,
small bowel, and colonic transit times in an
ambulatory setting.
WMC is a useful clinical tool in assessment
and management of diabetic patient with
motility impairment.
Saad RJ. Curr Gastroenterol Rep 2016; 18(3):14.
Rouphael C et al. Neurogastroenterol Motil 2017; 29(9).Therapeutic approach
What therapeutic approach?...
improving glycemic control GLP-1 analogs delay gastric emptying
DPP-IV inhibitors do not delay
CSII
diet and nutritional support small meals that are low in fat and fiber
small particle size diet
multivitamin support
enteral/parenteral nutrition
behavioral approach reduce carbonated beverages
avoide alcohol and tobacco smoking
ex adiuvantibus therapy …
Camilleri M et al. Am J Gastroenterol 2013; 108:18–37.
Olausson EA et al. Am J Gastroenterol 2014; 109(3):375-85.Ex adiuvantibus therapy
Classe Meccanismo d’azione Molecola Posologia Principali eventi avversi
Farmacologica
Procinetici Antagonista D2 e Metoclopramide 10-20 mg x 4 Sintomi extrapriramidali
agonista 5-HT3/5-HT4 Iperprolattinemia
Tachifiassi
Procinetici Antagonista D2 Domperidone 10-20 mg x 4 Iperprolattinemia
Antibiotici macrolidi Agonista motilina Eritromicina 40-250 mg x 3 Dolori addominali
Allungamento QT
Antibiotici macrolidi Agonista motilina Azitromicina 500 mg Allungamento QT
Procinetici Antagonista D2 Levosulpiride 25 mg x 3 Iperprolattinemia
Antiemetici Agonista 5-HT4 Allungamento QT
Antiemetici Antagonista 5-HT3 Ondansetron 4-8 mxg x 2 Allungamento QT
Granisetron 1-3 mg
Antidepressivi Antagonista 5-HT3 Mirtazapina 30 mg Vertigini
noradrenergici Ipotensione ortostatica
serotoninergici
Greco C. Published online. Giornale Italiano di Diabete e Metabolismo, 2019.Conclusion
…Grazie per l’attenzione
You can also read