Malihe akbarpour Assistant professor Guilan university of medical science 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Malihe akbarpour
Assistant professor
Guilan university of medical science 2021
balance
Interaction of visual , vestibular and
proprioceptive input that CNS integrates as
motion and spatial orientation.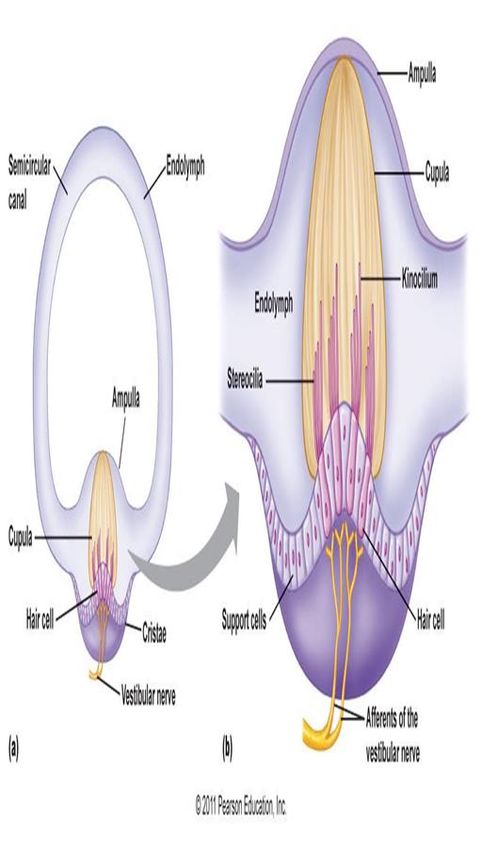
vestibular system
The peripheral vestibular
system is an integral part of the
labyrinth that lies in the otic
capsule in the petrous portion
of the temporal bone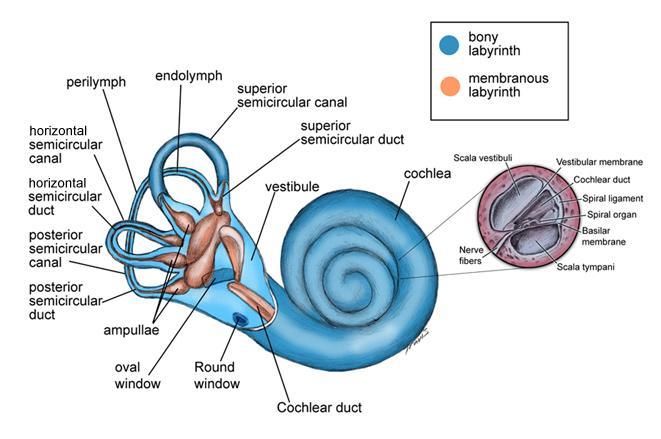
vestibular system
The vestibular system, which is the system of
balance, consists of 5 distinct end organs: 3 SCC
that are sensitive to angular accelerations and 2
otolith organs that are sensitive to linear (or
straight-line) accelerations
Each canal forms two thirds of a circle with a
diameter of about 6.5 mm / luminal cross-sectional
diameter of 0.4 mm .
Vestibular system development : 6w….25w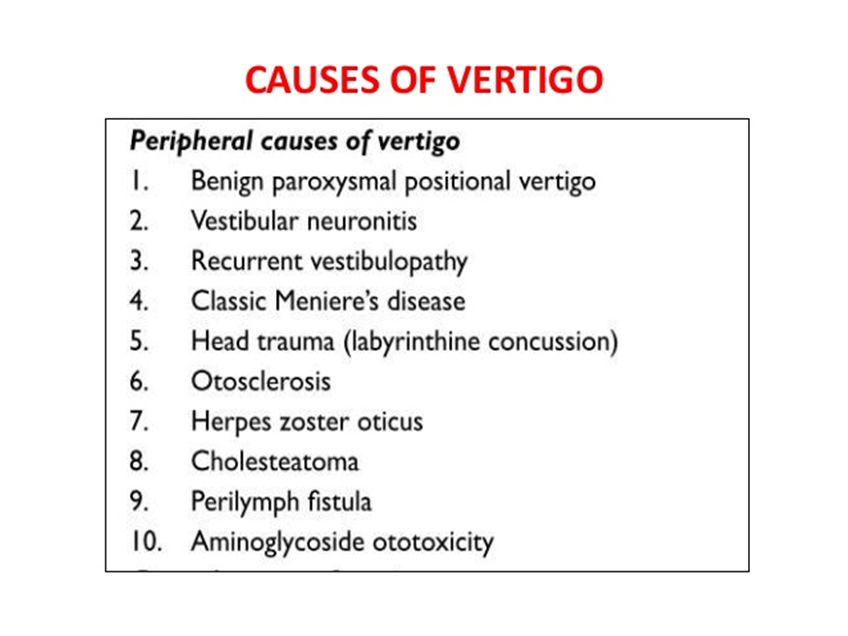
vestibular system
Semicircular canals
lateral or horizontal, superior or anterior, and posterior or
inferior.
They are oriented at right angles to each other and are
situated so that the superior and posterior canals are at 45°
angles to the sagittal plane and the horizontal canal is 30° to
the axial plane.
responsive to angular motion
paired with a canal on the contralateral side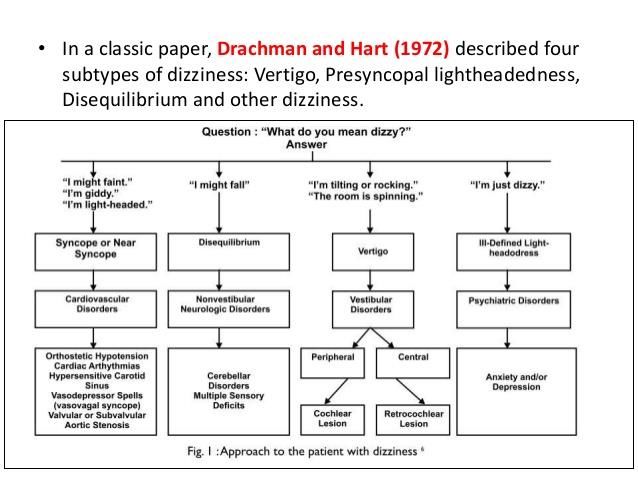
vestibular system
One end of each canal is dilated to form the ampulla, which
contains a saddle-shaped ridge termed the crista ampullaris;
the sensory epithelium lies on the crista ampullaris. The
nonampulated ends of the superior and posterior canal form the crus
commune or common crus.
All canals merge into the utricle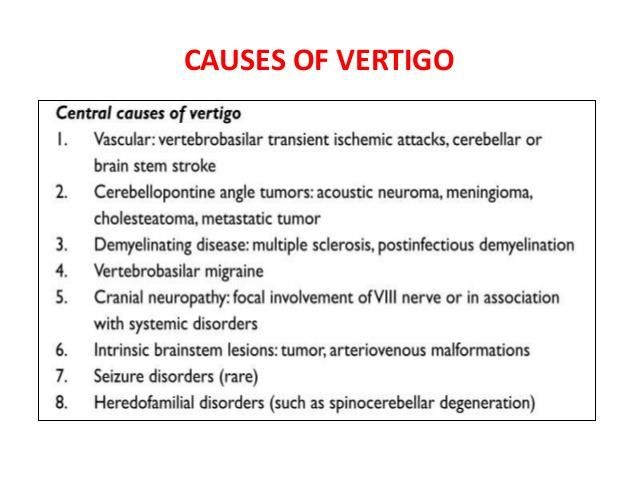
vestibular system
The otolith organs include the utricle and the saccule.
The utricle senses motion in the horizontal plane (eg,
forward-backward movement, left-right movement, or a
combination thereof).
The saccule senses motions in the sagittal plane (eg, up-
down movement)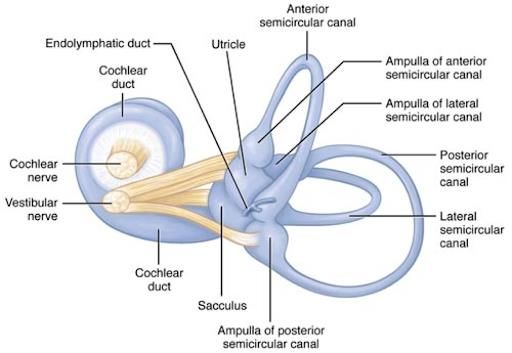
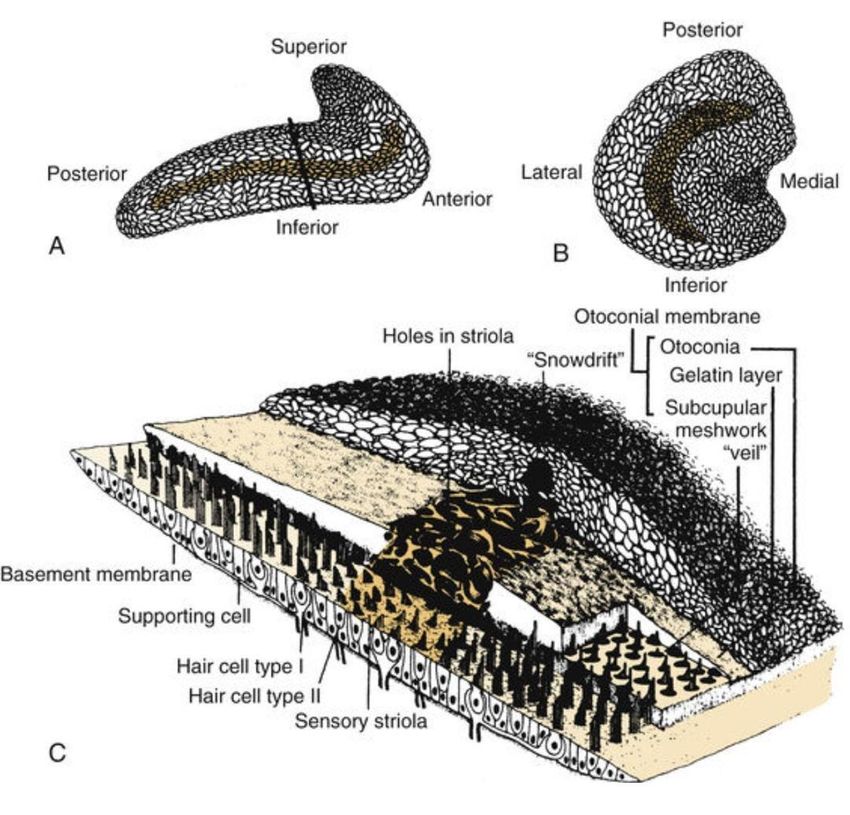
vestibular sensory epithelium
The vestibular sensory epithelium is located on the maculae of the saccule and
utricle and the cristae of the semicircular canals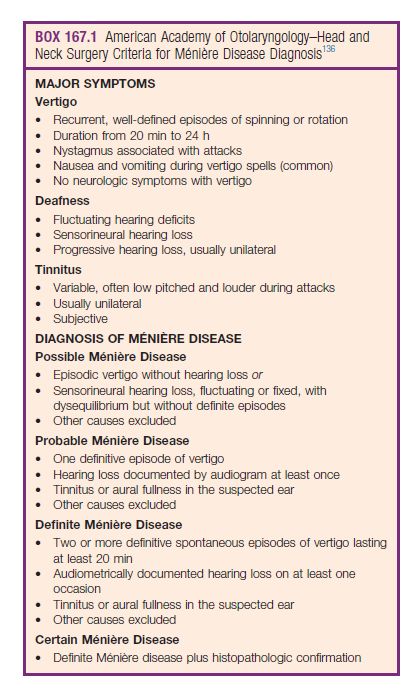
Blood suply
Central Vestibular Connections
Vestibular nuclei
The central processes of the primary afferent vestibular neurons divide into an ascending and descending
branch after entering the brainstem at the inner aspect of the restiform body.
Some primary vestibular neurons pass directly to the cerebellum, in particular the flocculonodular lobe
and the vermis. No primary vestibular afferent neurons cross the midline.
In the vestibular nuclei, 4 major groups of cell bodies (the second-order vestibular neurons) may be
identified: (1) superior vestibular nucleus (SVN) of Bechterew, (2) lateral vestibular nucleus (LVN) of
Dieter, (3) medial vestibular nucleus (MVN) of Schwalbe, and (4) descending vestibular nucleus (DVN).vertigo
Dizziness and vertigo are among the most common symptoms causing patients to visit a
physician (as common as back pain and headaches).
The overall incidence of dizziness, vertigo, and imbalance is 5-10%, and it reaches 30-40% in
patients older than 40 years. The incidence of falling is 25% in subjects older than 65 years.
1–3% of presentations to the emergency department (ED)
incidence of cerebrovascular disease in patients presenting to the ED with these
complaints ranges from 3 to 5%
previous studies have shown that about 10% of patients with cerebellar stroke may at
least initially present with symptoms that mimic vestibular neuritis “pseudovestibular
neuritis”vertigo
Vertigo is an illusion of movement caused by asymmetric input to the vestibular
system.
Subjective or Objective
Peripheral or centralEvaluation of the patient with dizziness :
Dizziness includes light-headedness, unsteadiness, motion intolerance, imbalance,
floating, or a tilting sensation.
It is essential to distinguish vertigo, which is a subtype of dizziness defined as an
illusion of movement caused by asymmetric input to the vestibular system, from
other types of dizziness.
This dichotomy is helpful because true vertigo is often due to inner-ear disease, whereas
other symptoms of dizziness may be due to central nervous system (CNS ),
cardiovascular, or systemic diseases.Evaluation of the patient with dizziness :
careful history taking
complete neuro-otologic physical examination
nature of the symptoms,
the duration,
triggering or alleviating factors.Evaluation of Patient with dizziness
Determine if the patient has a sense of being pushed down or pushed to 1 side . sense of movement of
objects viewed when the patient moves is termed oscillopsia.
Ascertain whether the symptoms are related to an anxiety episode; patients with agoraphobia may describe
their symptoms as dizziness.
Determine if the sensation is continuous or episodic; if episodic, find out if the sensation is fleeting or
prolonged.
Ascertain whether the onset and progression of symptoms were slow and insidious or acute.
Ask the patient about head trauma and other illnesses to determine the setting of the initial symptoms.Evaluation of Patient with dizziness
Determine if the episodes are associated with turning the head, lying supine, or sitting upright.
Determine if symptoms of an upper respiratory infection or flu-like illness preceded the onset of vertigo.
Inquire about associated symptoms such as hearing loss or tinnitus (ringing in the ears), aural fullness,
diaphoresis, nausea, or emesis.
Determine if the patient has an aura or warning before the symptoms start.
If hearing loss is evident, find out if hearing fluctuates.
Determine if the patient has a headache or visual symptoms such as scintillating scotoma.
Ask the patient about brainstem symptoms such as diplopia, dysarthria, facial paresthesia, or extremity
numbness or weakness.Evaluation of Patient with dizziness
Medical history
Determine if the patient has conditions such as diabetes (which can cause visual and
proprioceptive problems), hypertension, cardiovascular or cerebrovascular disease, migraine, or
neurologic disease (eg, multiple sclerosis).
Determine if the patient has any family history of cardiovascular disease, peripheral vascular
disease, or migraine. Labyrinthine causes of vertigo usually are not inherited; however, rare
exceptions (eg, Usher syndrome) are reported. Some clinical researchers believe that Ménière
disease may have a hereditary predilection.
Inquire about the patient's medications. The list of medications that can cause dizziness is long;
the most common culprits are antihypertensive agents. Ask if the onset of the patient's symptoms
was associated with starting a new medication or a change in the dose or frequency of a
medication.Evaluation of Patient with dizziness
Determine if the patient has had ear surgery. Although surgery for chronic ear disease only
occasionally results in permanent vestibular injury, patients with a history of surgery for
cholesteatoma may have an iatrogenic or acquired labyrinthine fistula. Patients who have
undergone stapes surgery for otosclerosis or tympanosclerosis may develop vestibular symptoms
because of perilymphatic fistula, adhesions between the oval window and saccule, or an overly
long prosthesisThe time course of vertigo is important:
1. Vertigo lasting seconds and is associated with head or body position changes is probably due to benign
paroxysmal positional vertigo (BPPV)
2. Vertigo lasting minutes to hours : a. Ménière disease b. Migraine associated vertigo c. Otic syphilis d.
Cogan disease
3. Vertigo lasting days to weeks with nausea and no other ear or CNS symptoms (vestibular neuritis)
4. Vertigo of variable duration a. Inner ear fistula b. Labyrinthine concussion c. Blast trauma d.
Barotrauma e. Superior semicircular canal dehiscence syndrome f. Bilateral vestibular hypofunction
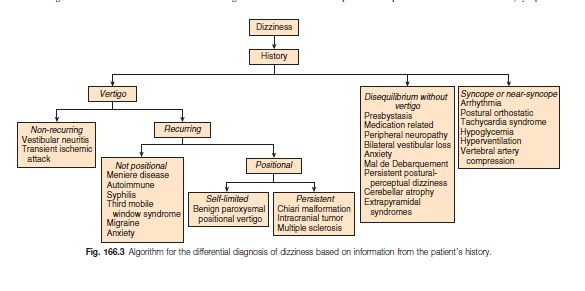
5. Constant vertigo : a. Suggests a central etiologyDizziness has been sub-classified into :
vertigo – a false sensation of movement of self or environment,
presyncope – sensations of light-headedness and impending fainting,
disequilibrium – a sensation of imbalance and/or postural instability,
"other types of dizziness“ – a vague and floating sensation often accompanied
by somatic symptoms
DDX
The most common causes of peripheral vertigo include BPPV, vestibular neuronitis, Ménière disease, and immune-mediated inner-ear disease. The most common cause of central dizziness is migraine, frequently referred to as vestibular migraine or migraine-associated dizziness. Other central causes include demyelination, acoustic tumors, and brainstem or cerebellar vascular lesions
BPPV
Benign paroxysmal positional vertigo (BPPV), a disorder of the inner ear characterized by
sudden, repeated episodes of positional vertigo, is the most common : 17-20% of peripheral
vertigo. It has a favorable prognosis for recovery, with approximately 50% of cases resolving
spontaneously within 3 months, and is rarely associated with any serious underlying CNS
disorder.
50 to 70 years and mostly in female
DX : Dix–Hallpike test
RX: Epley Manoeuvrevestibular neuronitis
classically presents with vertigo, nausea, and gait imbalance It is considered a benign, self-limited
condition that typically lasts several days
The data is lacking regarding the incidence of acute vestibular neuritis, is known to be the third most
common cause of peripheral vertigo following BPPV and Meniere disease.
no gender preference / usually affects middle ages
inflammatory disorder selectively affecting the vestibular portion(superior division of the vestibular
nerve) of the 8th cranial nerve.
cause is presumed to be of viral origin (e.g., the reactivation of latent HSV infection), but other causes
of vascular etiologyMénière disease
Definite MD: Two or more spontaneous attacks of vertigo, each
lasting 20 minutes to 12 hours
Audiometrically documented fluctuating low- to
midfrequency sensorineural hearing loss (SNHL) in
the affected ear on at least 1 occasion before,
during, or after 1 of the episodes of vertigo
Fluctuating aural symptoms (hearing loss, tinnitus,
or fullness) in the affected ear
ther causes excluded by other tests
Probable MD: At least 2 episodes of vertigo or dizziness lasting
20 minutes to 24 hours
Fluctuating aural symptoms (hearing loss, tinnitus,
or fullness) in the affected ear
Other causes excluded by other testsNystagmus
Nystagmus may be defined as a periodic rhythmic ocular oscillation of the eyes. The
oscillations may be sinusoidal and of approximately equal amplitude and velocity
(pendular nystagmus) or, more commonly, with a slow initiating phase and a fast
corrective phase (jerk nystagmus).
unilateral or bilateral.
congenital ( may be associated with afferent visual pathway abnormalities (sensory
nystagmus) or acquiredThree mechanisms are involved in maintaining foveal
centration of an object of interest:
Fixation in the primary position involves the visual system's ability to detect drift of a foveating
image and signal an appropriate corrective eye movement to refoveate the image of regard. The
vestibular system is intimately and complexly involved with the oculomotor system.
The vestibulo-ocular reflex is neural interconnections that maintains foveation of an object
during changes in head position.
neural integrator. When the eye is turned in an extreme position in the orbit, the fascia and
ligaments that suspend the eye exert an elastic force to return toward the primary position. To
overcome this force, a tonic contraction of the extraocular muscles is required. A gaze-holding
network called the neural integrator generates the signal. The cerebellum, ascending
vestibular pathways, and oculomotor nuclei are important components of the neural
integrator.Vestibular nystagmus
central or peripheral.
peripheral nystagmus is unidirectional with the fast phase opposite the lesion;
central nystagmus may be unidirectional or bidirectional; purely vertical or torsional nystagmus suggests a
central location;
central vestibular nystagmus is not dampened or inhibited by visual fixation; tinnitus or deafness often is
present in peripheral vestibular nystagmus, but it usually is absent in central vestibular nystagmus.
You can also read