Meningococcal Meningitis - Serogroups A, C, Y, W-135 and Serogroup B - Winnipeg Regional Health Authority
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Meningococcal Meningitis - Serogroups A, C, Y, W-135 and Serogroup B
The disease, meningococcal meningitis, is a serious, sometimes fatal bacterial infection that occurs sporadically worldwide and in focal
epidemics. It is transmitted by person-to-person close contact with respiratory secretions or saliva of an infected person. Children and
young adults are most at risk for the disease. Meningococcal meningitis is characterized by a short incubation period followed by sudden
onset of symptoms. Meningococcal septicemia, in which bacteria rapidly disseminate through the bloodstream, is a less common form of
meningococcal disease, but has been responsible for the high case fatality rate in outbreaks of group C disease in Canada.
The five major serogroups most commonly associated with invasive disease are A, B, C, Y & W-135. Serogroups B & C are the most
frequent causes of sporadic cases and outbreaks in Europe & the Americas, followed by Y. Although serogroup A used to be the main
cause of epidemic disease, mainly in Africa and Asia, ssince 2010, 22 of the 26 countries in the African meningitis belt have introduced a
meningococcal A conjugate vaccine (MACV), and the decrease in the incidence of Neisseria meningitidis (N.m) A has been confirmed and
sustained. Serogroups Y and W-135 are relatively uncommon, but may be on the rise; during the past years, serogroup Y has emerged as
a cause of disease in Canada and the USA, and serogroup W-135 has been associated with meningococcal disease epidemics in Saudi
Arabia and Burkina Faso. Serogroup B is the most common source of meningococcal disease world-wide.
Epidemics most often occur during the winter-spring in temperate regions and in the dry season (which varies by country, but typically
between Nov & June) in tropical regions. The exact timing of the season varies from year to year and from country to country (occurring
earlier in the east and later in the west) (See Map 7-7). Vaccines against serogroups A, B, C, Y and W-135 are available in Canada.
The “meningitis belt” in Africa (see Map 7-8) is considered hyper-endemic for meningococcal meningitis. The disease is present all the time,
with epidemic rates (occurring between epidemics) often exceeding those in other countries. Epidemics in the belt occur in cycles that can last
2-3 years and tend to recur every 8-12 years. Since the 1980’s the intervals between epidemics have become shorter and more irregular.
During the dry season, the incidence rate of meningococcal disease can reach as high as 1,000 cases per 100,000 population. In non-
epidemic periods, the rate of meningococcal disease is roughly 5 - 10 cases per 100,000 population. The fatality rate is about 5 to 10%.
Since the mid-1990’s epidemics have become more frequent, and have spread beyond the usual boundaries. Outside the meningitis belt, there
is no evidence of a cyclical pattern of epidemics.
To identify travellers at higher risk and who should also receive vaccine (See Section II, Table 4 Meningococcal Meningitis):
• Countries in the meningitis belt (endemic), noted with the year of most recent activity - children and adolescents are at increased risk
• Countries that are outside of the meningitis belt that have experienced meningococcal meningitis activity (epidemic) within the last 2 -3
years - rates rise in older children and young adults
Refer to the MHSAL Eligibility Criteria and to the Canadian Immunization Guide (CIG), Table 1 for individuals with underlying
medical conditions who meet the criteria for publicly funded meningococcal vaccines.
Revised July 7, 2020E -Vaccination for Serogroups A, C, Y, W-135 is Recommended for the following individuals, depending on
degree of exposure: In general, the following travellers do not need to receive serogroup B vaccine unless there is evidence of a
hyperendemic strain or an outbreak that is known to be caused by serogroup B that can be prevented by the vaccine:
(The decision to recommend vaccination should be based on a careful assessment of risk, taking into account the destination, epidemiology of
disease, nature of exposure, and the health of the traveller).
• All persons 2 months of age and older, travelling to an area of current epidemic disease (*within the last year) regardless of
duration of exposure (Refer to Table 4, bolded countries).
• Persons travelling to the meningitis belt or to African countries outside the usual boundaries of the meningitis belt, where there is not
current activity but where epidemics have occurred within the past 2 – 3 years who will also be:
o Living or working there
o In close contact with the local population i.e.; through school, accommodations, or public transport.
*Note: When making your assessment, risk in these areas is highest in the dry season (which varies between countries from
Dec to June).
• Persons travelling to areas (including developed countries) where sporadic epidemics (including meningococcal C) have been
reported in the last 6 months (check Public Health Agency of Canada Advisories or WHO web sites). *Note: In developed countries,
travellers should follow the meningococcal immunization recommendations of the destination country.
• Travellers to Saudi Arabia for the purpose of “Umrah” or the Hajj pilgrimage, or for seasonal work. Saudi Arabia requires
evidence of vaccination (certificate of vaccination clearly documented with the name and type) against serogroups A, C, Y, W-135 for
adults and children aged two years and older, administered no less than 10 days before arrival in Saudi Arabia. The vaccine name and
type must be clearly indicated on the immunization certificate. For entry purposes:
o Visitors from all countries: Visitors arriving for the purpose of Umrah or pilgrimage (Hajj) or for seasonal work are
required to submit a certificate of vaccination with the quadrivalent (ACYW 135) vaccine against meningitis, proving the
vaccine was administered in the past 3 years with a polysaccharide vaccine (no longer available in Canada) or 5 years
with a conjugate vaccine and no less than 10 days before arrival in Saudi Arabia. The responsible authorities in the
visitor’s country of origin should ensure that adults and children aged over 2 years are given 1 dose of the quadrivalent
(ACYW135) vaccine and state clearly the type of the vaccine used on the vaccination card. If the vaccine type is not
indicated on the certificate, the certificate will only be valid for 3 years.
o Interior pilgrims and the Hajj workers: Vaccination with quadrivalent (ACYW135) vaccine is required for those who
have not been vaccinated in the past 3 years with a polysaccharide vaccine (no longer available in Canada) or 5 years
with a conjugate vaccine:
all citizens and residents of Medina and Mecca
all citizens and residents undertaking the Hajj (ie; domestic pilgrims)
all Hajj workers including individual working at entry points or those in direct contact with pilgrims, such as
personnel in healthcare settings
Revised July 7, 2020E -Vaccination for Serogroups A, C, Y, W-135 is Recommended for the following individuals, depending on
degree of exposure, in addition to consideration of serogroup B meningococcal vaccine:
• Travellers staying in schools, colleges & other places where large numbers of adolescents and your adults congregate
• Travellers engaging in research, industrial and/or clinical laboratory settings as well as military personnel may be at increased risk
of disease or exposure to N. Meningitis
• Travellers with asplenia, functional or anatomic (including sickle cell disease); congenital complement deficiency; properdin; factor
D or primary antibody deficiencies; acquired complement deficiency due to receipt of the terminal complement inhibitor
eculizumab (Soliris™); HIV infection, especially if congenitally acquired and those with cochlear implants are at higher risk of
complications from invasive meningococcal meningitis and should be provided vaccination with the conjugate quadrivalent vaccine
regardless of potential for travel. (*Note: These individuals with underlying medical conditions meet the criteria for publicly funded
vaccine according to Manitoba Health Seniors & Healthy Living).
Vaccine Usage:
• Travellers who have previously received meningococcal conjugate vaccine against serogroup C (at 1 year of age and/or with the
school based program) will not be protected against other serogroups and will therefore still require the quadrivalent conjugate
vaccine, if indicated for their travel. Independent of travel, Conjugate C vaccine should be up-to-date for age, according to the
provincial immunization schedule.
• There are three conjugate quadrivalent vaccines (containing Groups A, C, Y, W-135) currently licensed in Canada; Menomune™ (a
polysaccharide vaccine) has been discontinued in Canada:
®
o Menactra , Menveo™ & Nimenrix™ are the vaccines of choice for travellers, as they are known to have significant
advantages over the polysaccharide vaccine:
• Better immune memory
• Longer duration of efficacy
• Lack of hypo-responsiveness with booster doses
• Possible reduction of bacterial carriage rate
• There are two meningococcal serogroup B vaccines currently licensed in Canada: Bexsero® and Trumenba™
Respected Timeframes Between Meningococcal Vaccines:
If a meningococcal conjugate vaccine is given, wait at least 1 month before administering another meningococcal conjugate vaccine.
Meningococcal serogroup B vaccines can be given concomitantly with quadrivalent meningococcal serogroup A, C, Y, W conjugate
vaccines or other vaccines
Interchangeability of Meningococcal Vaccines:
There are no published data regarding the interchangeability of Men-C-C vaccines, but the vaccines have been safely interchanged
without a noticeable decrease in efficacy.
Revised July 7, 2020 When possible, an infant series should be completed with the same vaccine. Either Men-C-ACYW vaccine may be used for re-
vaccination, regardless of which meningococcal vaccine was used for initial vaccination.
If providers are challenged with having to consider alternate use of conjugate quadrivalent vaccines to ensure travellers are provided some
protection prior to departure (ie; during times of vaccine shortages etc.), the following principles should be used in your decision making:
o For individuals 2 to 23 months of age:
Menveo™ should be the first-line recommendation (CIG recommendation)
Nimenrix® should be the alternative option, if Menveo™ is not available (product monograph indication)
If neither Menveo™ or Nimenrix® are available, Menactra® should be considered as a last option
(*off-label recommendation)
• Ensure parents are informed of this usage, and note that although adequate protection or efficacy may be assumed to
be similar, it cannot be guaranteed.
• Any prescriber who is recommending or administering this vaccine should be aware of the contents of the product
monograph and/or similarly approved standards or instructions for use. The manufacturer has received approval for
use of their product based on evidence as to the safety and efficacy of their product only when used in accordance
with the product monograph or similarly approved standard or instruction for use. This recommendation for use
may differ from that set out in the product monograph or other similarly approved standards or instructions for use
by the licensed manufacturer. Such recommendations may be endorsed by NACI, CIG or CATMAT, based on the
best available evidence.
The two serogroup B meningococcal vaccines (MenB-fHBP and 4CMenB) are not interchangeable; the vaccine products contain different
antigens and there are no published studies on the immunogenicity resulting from a vaccination series combining the two products.
Therefore, the same vaccine product should be used for all doses in a vaccination series. If, in a person with an incomplete vaccination
series, it is unknown what vaccine product they initially received, the initial dose(s) should be discounted and the vaccination series
repeated using the same vaccine product for all doses in the new, repeated series.
Sources:
CIG: Meningococcal Vaccine;
Trumenba Product Monograph, May 24, 2019
Bexsero Product Monograph, June 12, 2020
Menveo Product Monograph, June 3, 2020
Nimenrix Product Monograph, Dec 19, 2018
Menactra Product Monograph, Nov 28, 2017
CATMAT Statement on Meningococcal Disease and the International Travel, May 7, 2015
Health Requirements and Recommendations for Travellers to Saudi Arabia for Hajj and Umrah; June 9, 2019
Weekly Epidemiological Record; 5 APRIL 2019, Nos. 14/15, 2019, 94, 179–188
NACI Update on Quadrivalent Meningococcal Vaccines available in Canada, April 2015
The Use of Bivalent Factor H Binding Protein Meningococcal Serogroup B (MenB-fHBP) Vaccine for the Prevention of Meningococcal B Disease, NACI, Jan
29, 2020
Advice for the Use of the Multicomponent Meningococcal Serogroup B (4CMenB) Vaccine, NACI, April 2014
Revised July 7, 2020Recommended Quadrivalent Conjugate Meningococcal Vaccines (Men-C-ACYW-135*1) &
Serogroup B Meningococcal Vaccine *2 Schedules for Travellers
Recommended Booster Doses
Age Schedule
vaccine(s)
2 to 11 months Menveo™*3 2 or 3 doses *4 given 8 weeks apart*5 (with another Men-C-ACYW-135:
of age and/or Bexsero® dose between 12-23 months of age that is at least 8 • If vaccinated at 6 years of age or younger:
weeks from the previous dose) *5 every 3 to 5 years
12 to 23 Menveo™ *3 2 doses at least 8 weeks apart*5 • If vaccinated at 7 years of age & older:
months of age and/or Bexsero® every 5 years
• Travellers to the Hajj should check
24 months to 9 Men-C-ACYW-135*1 1 dose of Men-C-ACYW-135*1 recommendations for re-vaccination, as they
years of age 2 doses of Bexsero® (4CMenB), given at least 8 may require booster vaccination no more than
and/or Bexsero® weeks apart 3 years and no less than 10 days before
arrival in Saudi Arabia.
10 years of age Men-C-ACYW-135*1 1 dose of Men-C-ACYW-135*1 Serogroup B:
and older*6 and/or 2 doses of Bexsero®, at least 4 weeks apart or • The need for a booster dose is yet to be
Bexsero® or determined
Trumenba™ 2 doses of Trumenba™, at least 6 months apart or
3 doses of Trumenba™, at least 4 weeks apart, with
another dose at least 4 months after dose two)
*1: Men-C-ACYW-135: Menactra® (Men-C-ACYW-DT), Menveo™ (Men-C-ACYW-CRM) or Nimenrix™ (Men-C-ACYW-TT)
*2: Serogroup B Meningococcal Vaccines: Bexsero® (4CMenB) - Multicomponent Meningococcal Serogroup B OR Trumenba™ (MenB-fHBP) - Bivalent
Meningococcal Serogroup B
*3: Men-C-ACYW-CRM (Menveo™) is authorized for use in children 2 months of age and older. Based on available published data in this age group,
Menveo™ should be used because it has been found to be safe and immunogenic.The schedules in this table are based on those used in published clinical
trials and the recommendation that a dose of meningococcal conjugate vaccine be given in the second year of life (12 to 23 months) for children vaccinated at less
than 1 year of age.
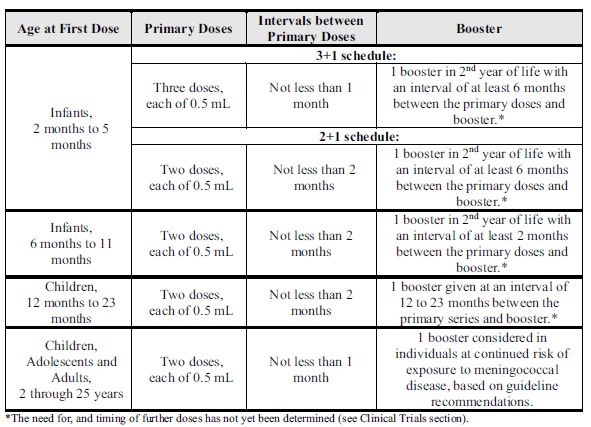
*4: For Bexsero® (4CmenB), depending on the age at which immunization is initiated, the manufacturer recommends two or three primary doses and a booster
(2 + 1 schedule or 3 + 1 schedule) when the first dose is received between the ages of 2 and 5 months, and two primary doses and a booster (2 + 1 schedule) when
the first dose is received between ages of 6 and 11 months. The booster dose should be administered in the second year of life.*See Biological page for schedule
*5: Men-C-ACYW-135 vaccines may be given a minimum of 4 weeks apart if accelerated immunization is needed.
*6: Serogroup B Meningococcal vaccines are not authorized for use in those 26 years of age and older and Men-C-ACYW-135 vaccines are not
authorized for use in those 56 years of age and older; however, based on limited evidence and expert opinion their use is considered appropriate above
these authorized ages (*CIG).
*Refer to section above on Interchangeability
Revised July 7, 2020Initial Series Reinforcements Specific Contraindications Expected Reactions
Meningococcal Dosage: If vaccinated at 6 years 1. Known hypersensitivity to any Common Local Reactions:
Meningitis 1 Dose of age or younger: component of the vaccine: Sodium 2 to 10 year olds:
Conjugate 0.5 ml IM (deltoid every 3 to 5 years Chloride, Sodium Phosphate, - Pain at the injection site (40 – 48%)
preferred site or Anhydrous, *Syringes & vial Adolescents and adults:
Menactra® anterolateral part of If vaccinated at 7 years stopper latex-free - Pain at the injection site (52 - 64%)
A, C, Y, W-135 the thigh in those of age & older: 2. Anaphylactic reaction to a Common Systemic Reactions:
(Men-C-ACYW-DT) 12 to 23 months of every 5 years previous dose. 2 to 10 year olds
age) 3. Previous history of Guillain-Barré - Drowsiness (10 – 26%)
Sanofi Pasteur Syndrome - Irritability (11 – 35%)
*Travellers to Saudi - Diarrhea (12 –16%)
*Authorized in Protection is Arabia for the purpose Caution: Adolescents and adults:
Canada for ages 9 established 8 – 28 of Umrah and Hajj Menactra® has not been studied - Headache (37 – 41%)
months to 55 years days after require the vaccine with pregnant women; use only if the - Fatigue (30 – 34%)
vaccination. within past 5 years with benefits outweigh the risks. May be Very Rare:
a conjugate vaccine administered to women who are - Guillain Barré Syndrome
and no less than 10 breastfeeding. - Thrombocytopenia
days before arrival. - Urticaria
Biological Initial Series Reinforcements Specific Contraindications Expected Reactions
Meningococcal Dosage: If vaccinated at 6 years 1. Known hypersensitivity to any Very common (greater than 1 in 10):
Meningitis 1 Dose of age or younger: component of the vaccine: Sucrose, Loss of appetite, irritability,
Conjugate 0.5 ml IM (deltoid every 3 to 5 years Trometamol. Sodium chloride drowsiness, headache, fever, swelling,
preferred site or 2. Anaphylactic reaction to a pain & redness at the injection site,
Nimenrix™ anterolateral part of If vaccinated at 7 years previous dose. fatigue
A, C, Y, W-135 the thigh in those 6 of age & older: 3. Previous history of Guillain-Barré Common (greater than 1 in 100):
(Men-C-ACYW-TT) to 23 months of every 5 years Syndrome Diarrhea, vomiting, nausea, injection
age) site hematoma
Pfizer Canada Protection is Uncommon (greater than 1 in 1,000):
established 8 – 28 Caution: Insomnia, crying, dizziness, decreased
*Requires days after NIMENRIX® should be used during feeling or sensitivity especially in the
reconstitution vaccination. pregnancy only when clearly needed skin, itching, rash, aching muscles,
and the possible advantages pain in extremity (pain in the limb),
*Authorized in Note: Although outweigh the potential risks for the generally feeling unwell, and injection
Canada for ages 6 NIMENRIX® *Travellers to Saudi fetus. May be administered to site reaction (such as a hard lump at
weeks to 55 years contains tetanus Arabia for the purpose women who are breastfeeding. the injection site, itching warmth and
toxoid, this vaccine of Umrah and Hajj loss of feeling)
does not substitute require the vaccine Rare (up to 1 in 1,000):
for tetanus within past 5 years with Large swelling of the vaccinated limb
immunization a conjugate vaccine associated with redness
and no less than 10
days before arrival.
Revised July 7, 2020Biological Initial Series Reinforcements Specific Contraindications Expected Reactions
Meningococcal Dosage: If vaccinated at 6 years 1. Known hypersensitivity to any Common (greater than 10%):
Meningitis 1 Dose of age or younger: component of the vaccine: Swelling, redness and soreness at
Conjugate 0.5 ml IM (deltoid every 3 to 5 years CRM197 or other diphtheria- injection site headache, diarrhea,
preferred site or containing vaccines; feeling tired or achy
Menveo™ anterolateral part of If vaccinated at 7 years Potassium dihydrogen phosphate, Not Common (1 – 10%):
A, C, Y, W-135 the thigh in those of age & older: sucrose, sodium chloride, sodium Fever, vomiting, rash
(Men-C-ACYW-CRM) 12 to 23 months of every 5 years dihydrogen phosphate monohydrate, Very Rare:
age) di-sodium hydrogen phosphate Anaphylaxis (itchy hives, swelling of
GlaxoSmithKline bihydrate; *Latex Free and T-Free the lips, face, tongue, legs and arms)
Protection is 2. Anaphylactic reaction to a
*Requires established 8 – 28 previous dose.
reconstitution days after *Travellers to Saudi 3. Previous history of Guillain-Barré
vaccination. Arabia for the purpose Syndrome
*Authorized in of Umrah and Hajj
Canada for ages 2 require the vaccine Caution:
months to 55 years within past 5 years with Menveo™ should be given during
a conjugate vaccine pregnancy only if the benefits of
and no less than 10 vaccination clearly outweigh the
days before arrival. risks. May be administered to
women who are breastfeeding.
Revised July 7, 2020Biological Initial Series Reinforcements Specific Contraindications Expected Reactions
Bivalent Standard Dosage The need for a booster 1.Known hypersensitivity to any Very Common (more than 1 in 10)
Meningococcal B for Routine dose following primary component of the vaccine: aluminum Headache, nausea, diarrhea, muscle
Vaccine Immunization: immunization series has phosphate, histidine, polysorbate 80, pain, joint pain, redness, swelling and
not been established. & sodium chloride pain at the injection site, chills and
2 doses 2. Anaphylactic reaction to a fatigue
Trumenba™ 0.5ml IM*from a previous dose
(MenB-fHBP) prefilled syringe at This vaccine is Common (more than 1 in 100
Recombinant 0 & 6 months immunogenic, although *syringes & plunger latex free Vomiting, fever
its effectiveness, impact The tip cap and rubber plunger of the
Dosage strength of syringe are not made with natural
60 mcg of subfamily Dosage for on carriage and herd
Individuals at immunity, and its duration rubber latex
A and 60 mcg of
subfamily B rLP2086 Increased Risk of of protection remain
Invasive unknown. Caution:
(120 mcg total There are no data from the use of
protein) per 0.5 mL Meningococcal
Disease (IMD): Trumenba™ in immunocompromised
dose. individuals or in pregnant women. It
Pfizer Canada 3 doses is unknown if Trumenba™ is
0.5ml IM* from a excreted in human milk. Only use in
prefilled syringe these circumstances, if the potential
with the first 2 benefits clearly outweighs the
Notes: potential risks.
Shake vigorously doses at least 1
before use to ensure month apart, Give with caution to individuals with
a homogeneous followed by a third thrombocytopenia or any coagulation
white suspension is dose at least 4 disorder or to those receiving
obtained. months after the anticoagulant therapy, unless
2nd dose the potential benefit clearly
Do not use the outweighs the risk of administration.
vaccine if it cannot be
re-suspended or if *Deltoid preferred
particulate matter or site
discolouration is
found. Note:
Due to lack of
Syringes should be data,
stored in the meningococcal
refrigerator group B vaccines
horizontally (laying are not
flat on the shelf) to interchangeable.
minimize
the re-dispersion
time.
*Authorized in
Canada for ages 10
through 25 years
Revised July 7, 2020Biological Initial Series Reinforcements Specific Contraindications Expected Reactions
Dosage: The need for a booster 1. Known hypersensitivity to any Local Reactions:
Multicomponent 0.5 ml IM dose is yet to be component of the vaccine: Tenderness and redness at the
Meningococcal determined. Kanamycin, Sodium Chloride, injection site; induration.
Vaccine *See chart below Histidine, Sucrose, Aluminum
for Schedule: Hydroxide, Natural Rubber Latex Systemic Reactions:
Bexsero® (tip cap of the syringe) Adults: Headache, malaise, myalgia,
(4CMenB) 2. Anaphylactic reaction to a
Recombinant, previous dose Infants & children:
Fever, irritability, unusual crying,
adsorbed Caution: sleepiness
- Not expected to provide protection Uncommon (≥ 1/1,000 to < 1/100):
GlaxoSmithKline against all circulating meningococcal Fever ≥40°C, nervous system
serogroup B strains or other invasive disorders, seizures (including febrile
meningococcal disease (IMD). seizures), skin & subcutaneous tissue
- In immunocompromised disorders, eczema, urticaria, vascular
individuals, vaccination may not disorders, pallor (rare after booster)
result in a protective antibody Rare (≥ 1/10,000 to < 1/1,000):
response. Kawasaki syndrome
- Should only be given during
pregnancy or when breastfeeding if
the benefits of vaccination clearly
outweigh the risks, as there are no
studies.
White opalescent
liquid suspension in a
prefilled syringe. A
fine off-white deposit
may form when the
product stands for a
long period. Shake
the vaccine well
before use.
*Authorized in
Canada for ages 2
months to 25 years
Revised July 7, 2020You can also read