Modeling the Impact of Demography on COVID-19 Dynamics in Hubei and Lombardy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Modeling the Impact of Demography on
COVID-19 Dynamics in Hubei and Lombardy
The Harvard community has made this
article openly available. Please share how
this access benefits you. Your story matters
Citation Wilder, Bryan, Marie Charpignon, Jackson A. Killian, Han-Ching Ou,
Aditya Mate, et al. Modeling the Impact of Demography on COVID-19
Dynamics in Hubei and Lombardy (2020)
Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:42659940
Terms of Use This article was downloaded from Harvard University’s DASH
repository, and is made available under the terms and conditions
applicable to Other Posted Material, as set forth at http://
nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-
use#LAAModeling the Impact of Demography on COVID-19
Dynamics in Hubei and Lombardy
Age, household structure, and comorbidity distributions
influence outbreak dynamics and evaluation of policy interventions.
Bryan Wilder1∗ , Marie Charpignon2 , Jackson A. Killian1 , Han-Ching Ou1 ,
Aditya Mate1 , Shahin Jabbari1 , Andrew Perrault1 , Angel N. Desai3 ,
Milind Tambe1∗ , Maimuna S. Majumder4,5∗
1 School of Engineering and Applied Sciences, Harvard University, Cambridge, MA, USA
2 MIT Institute for Data, Systems, and Society, Cambridge, MA, USA
3 International Society for Infectious Diseases, Brookline, MA, USA
4 Department of Pediatrics, Harvard Medical School, Boston, MA, USA
5 Computational Health Informatics Program, Boston Children’s Hospital, Boston, MA, USA
*Corresponding author. Email: bwilder@g.harvard.edu (B.W.); milind tambe@harvard.edu (M.T.);
Maimuna.Majumder@childrens.harvard.edu (M.S.M.)
As the COVID-19 pandemic accelerates, understanding its dynamics will be
crucial to formulating regional and national policy interventions. We develop
an individual-level model for SARS-CoV2 transmission that accounts for location-
dependent distributions of age, household structure, and comorbidities ap-
plied to Hubei, China and Lombardy, Italy. Using these distributions together
with age-stratified contact matrices for each country, our model estimates that
the epidemic in Lombardy is both more transmissible and more deadly than
1in Hubei, while rates of disease documentation in both locations may be lower
than previously established. Evaluation of potential policies in Lombardy sug-
gests that targeted “salutary sheltering” by 50% of a single age group may
have a substantial impact when combined with the adoption of physical dis-
tancing measures by the rest of the population.
Since December 2019, the COVID-19 pandemic – caused by the the novel coronavirus
SARS-CoV2 – has resulted in significant morbidity and mortality (1). As of March 28, 2020,
an estimated 664,000 individuals have been infected, with over 30,000 fatalities worldwide (2).
Key factors such as existing comorbidities and age have appeared to play a role in an increased
risk of mortality (3). Epidemiological studies have provided significant insights into the disease
to date; however, as the pandemic continues to accelerate around the world, understanding
the transmission dynamics of SARS-CoV2 will be critical to mitigating its spread (4–7). As
national and regional governments begin to implement broad-reaching policies in response to
rising case counts and stressed healthcare systems, estimating the impact of these policies while
accounting for how population-specific demography impacts outbreak dynamics will be vital.
This study employs mathematical modeling to evaluate the impact of the distribution of age,
comorbidities, and household contacts on COVID-19 dynamics using existing data from Hubei,
China, and Lombardy, Italy, together with age-stratified contact matrices for each location.
We then describe how these findings may affect the utility of potential non-pharmaceutical
interventions at a country-level.
Model
We develop a stochastic agent-based model for SARS-CoV2 transmission which accounts for
distributions of age, household types, comorbidities, and contact between different age groups
in a given population. The model follows a susceptible-exposed-infectious-removed (SEIR)
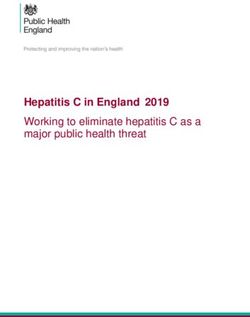
2template (8, 9) and proceeds in discrete time steps corresponding to days. Fig. 1 shows the
progression of individuals through the model compartments. Each individual’s probability of
progressing to severe disease states is determined by their age and comorbidities. We strat-
ify age into ten-year intervals and incorporate hypertension and diabetes as comorbidities due
to their worldwide prevalence (10) and association with higher risk of in-hospital death for
COVID-19 patients (3). However, our model can be expanded to include other comorbidities of
interest in the future.
The disease is transmitted over a contact structure, which is divided into in-household and
out-of-household groups. Each individual’s household is simulated using census data. Individ-
uals infect members of their households at a higher rate than out-of-household individuals. We
model out-of-household transmission using country-specific estimated contact matrices (11).
These matrices state the mean number of daily contacts an individual of a particular age stratum
has with individuals in other age strata.
Validation and Inferred Parameters
This section instantiates the model for two specific locations: Hubei, China (where the disease
originated) and Lombardy, Italy (one of the most heavily-impacted areas thus far, along with
Hubei). We show how our model is able to reproduce observed patterns in the number of
reported deaths, examine how a range of possible underlying parameters are consistent with
the data, and propose plausible ranges for r0 in Hubei and Lombardy and for the rate at which
infected individuals are documented.
There are three parameters for which values are not precisely estimated in the literature and
are varied in-simulation. First is pinf , the probability of infection given contact with an infected
individual. This determines the level of transmissibility of the disease. Second is t0 , the start
time of the infection, which is not precisely characterized in most locations and has an impact
3Infectious
Susceptible Exposed Asymptomatic
Removed
Mild
Recovered
Contact Household
matrix structure
Severe
Deceased
Critical
1 − !!→# (#$ , %$ )
Mild
!!→# (#$ , %$ ) ) ∼ Exp(.!→% )
Recovered
) ∼ Exp(.!→# )
Severe
Fig. 1: We use a modified SEIR model, where the infectious states are subdivided into levels
of disease severity. The transitions are probabilistic and there is a time lag for transitioning
between states. For example, the magnified section shows the details of transitions between
mild, recovered, and severe states. Each arrow consists of the probability of transition (e.g.,
pm→s (ai , ci ) denotes the probability of progressing from mild to severe) as well as the associated
time lag (e.g., the time t for progression from mild to severe is drawn from an exponential
distribution with mean λm→s ). ai and ci denote the age and set of comorbidities of the infected
individual i.
4due to rapid doubling times. Third is a parameter dmult , which accounts for differences in the rate
of mortality between locations that are not captured by demographic factors in the model (e.g.,
the impact of limited ICU capacity in Lombardy). dmult is a multiplier applied to the baseline
mortality rate estimated from China CDC data.
Hubei, China
We simulate the epidemic from a starting time t0 (varied around November 17 for the first iden-
tified patient in Wuhan (12)) through March 21, with lockdown on January 23. Details of the
modeled scenario can be found in the supplementary text. Validating the simulated results is
complex because infections are likely underdocumented (13). Because deaths are believed to
be better documented than infections, we evaluate our model by using the number of deaths
on the simulation end date while considering the possibility of both underreporting and overre-
porting (14, 15). Tables S2 and S3 show a sensitivity analysis of our estimates for hypothetical
underreporting or overreporting of deaths. The results of this analysis do not alter our main
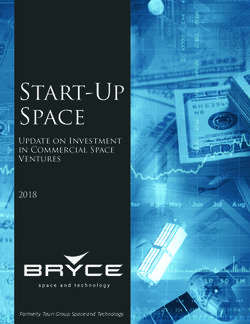
conclusions. While we fit using only the final total of deaths, Fig. 2 shows that our simulations
closely match the entire trajectory, thus guarding against overfitting. In addition, Figs. S1 and
S2 show out-of-sample validation against reported deaths in the week after the model was cal-
ibrated. All results, here and in the remainder of the paper, use 1000 independent runs of the
simulation.
There are several parameters that fit the data well. Fig. 3 shows two simulation outputs
across the entire parameter range, with heatmap saturation representing the goodness of fit
between the simulated and true number of reported deaths. We measure goodness of fit by
evaluating whether the true number of reported deaths is well-contained within the simulated
distribution. Specifically, if p is the percentile of the true number of reported deaths in the
distribution of the simulation runs, the color of the cell reflects p(1 − p). A value of 0 represents
510000 10000
Total deaths
Total deaths
7500 7500
5000 5000
2500 2500
0 0
15
10
4
29
23
21
1/
2
1
1
1
2
2
1
/
/
1/
2/
3/
2
2/
1
2
3/
1
2
11
12
1/
2/
2/
3/
3/
Date Date
Fig. 2: Simulated trajectories of the number of deaths over time in Hubei (left, pinf = 0.019,
t0 = November 15) and Lombardy (right, pinf = 0.029, t0 = January 22, dmult = 4) compared
to the true number of reported deaths. Light blue lines are individual trajectories, green is the
median, and the black dots are the number of reported deaths. The red dashed line represents
the lockdown in each location. The true number of reported deaths is contained within the
simulated distribution and lies close to the median (Pearson r = 0.998 and 0.992 respectively).
that the real number of deaths is either greater or smaller than all simulation runs, and a value
of 0.25 (the maximum possible) represents that the real number of deaths is exactly at the 50th
percentile of the simulated distribution. Assessing fit via the mean squared error yields a similar
parameter order but is more difficult to interpret.
The dark cells along the diagonal have p(1−p) close to 0.25, indicating that the true number
of reported deaths is well-contained within the simulated distribution across a range of param-
eter settings. We examine the implications of this range of possible parameter settings for two
quantities of interest: the basic reproduction number r0 and the documentation rate for symp-
tomatic infections.
The left side of Fig. 3 shows the inferred pre-lockdown r0 given by each set of parameters.
The values are consistent with existing estimates, which largely fall in the range 2–3 (16).
We calculate a single plausible range for our results, which includes all values for parameter
settings where the percentile p of the true number of reported deaths in the simulated distribution
satisfies p(1 − p) ≥ 0.2. For r0 , the plausible range is 2.06–2.28.
6dmult = 1 dmult = 1
0.00 0.05 0.10 0.15 0.20 0.25 0.00 0.05 0.10 0.15 0.20 0.25
0.016 1.858 1.892 1.876 1.889 1.892 1.875 1.911 0.016 0.561 0.651 0.858 - - - -
0.017 1.954 1.991 1.997 1.968 1.964 1.980 1.973 0.017 0.260 0.326 0.423 0.525 0.659 0.813 -
0.018 2.072 2.066 2.082 2.086 2.066 2.059 2.088 0.018 0.130 0.165 0.215 0.248 0.313 0.440 0.579
0.019 2.169 2.171 2.171 2.177 2.181 2.157 2.182 0.019 0.068 0.084 0.109 0.132 0.170 0.243 0.325
pinf
pinf
0.019 2.214 2.214 2.217 2.225 2.223 2.223 2.222 0.019 0.050 0.063 0.078 0.100 0.129 0.185 0.252
0.020 2.273 2.268 2.259 2.272 2.271 2.273 2.276 0.020 0.037 0.048 0.061 0.071 0.097 0.130 0.171
0.021 2.363 2.360 2.358 2.347 2.350 2.364 2.360 0.021 0.023 0.029 0.037 0.041 0.054 0.076 0.101
0.022 2.443 2.455 2.455 2.469 2.448 2.463 2.464 0.022 0.016 0.019 0.024 0.026 0.036 0.044 0.060
/8
0
2
3
5
7
9
/8
0
2
3
5
7
9
/1
/1
/1
/1
/1
/1
/1
/1
/1
/1
/1
/1
11
11
11
11
11
11
11
11
11
11
11
11
11
11
t0 t0
Fig. 3: Fit of parameters for Hubei. Left: median r0 as a function of pinf (y-axis) and t0 (x-axis).
Right: median fraction of symptomatic infections documented. Colors indicate the goodness
of fit, where darker colors suggest better fit. A large set of parameter settings (the dark green
diagonal entries) are consistent with the data, leading to a range of possible values for r0 and
the rate of documentation.
7The right side of Fig. 3 shows the inferred rate of documentation of symptomatic infections
given each set of parameters. We calculate this by dividing the actual number of confirmed
cases in Hubei on the simulation end date by the total number of symptomatic infections in
the simulation. The plausible range is 10.9–21.5%, lower than the range 28–33% estimated by
Russell et al. (13). One explanation is that earlier studies assumed an age-homogeneous attack
rate (13, 17); however, Fig. S3 shows that attack rates in our simulation are substantially higher
for younger groups, attributable to their larger number of daily contacts (11, 18). Since younger
individuals also have lower risk of fatality (19, 20), and because we use the total number of
deaths to calibrate the model, a larger number of undocumented infections is expected. This il-
lustrates how age-dependent behavioral patterns may impact estimates of important parameters,
motivating the inclusion of demographic information in COVID-19 modeling.
Lombardy, Italy
For Lombardy, we simulate the epidemic from January 22 through March 22, with a lockdown
on March 8. We vary the two parameters pinf and t0 that we examined for Hubei, but now also
consider the impact of dmult . Recall that dmult is a multiplier to the fatality rate across all ages and
comorbidities, which captures location-dependent variation in fatalities in excess of differences
due to demographic factors.
Fig. 4 shows goodness of fit for a wide range of parameters, along with the associated
estimates for r0 and the rate of infection documentation. Within each figure, each heatmap
corresponds to a different value of dmult , the multiplier for fatality rates relative to Hubei. It is
possible that fatality rates in Lombardy are higher than in Hubei (e.g., by a factor of 3-5), or
that r0 is higher in Lombardy than in Hubei. Together, the simulations suggest that both factors
likely contribute. We find broad support for the hypothesis that Lombardy has experienced a
more transmissible and more deadly outbreak than Hubei (21, 22).
8dmult = 1 dmult = 3 dmult = 5
0.00 0.05 0.10 0.15 0.20 0.25 0.00 0.05 0.10 0.15 0.20 0.25 0.00 0.05 0.10 0.15 0.20 0.25
0.020 0.170 0.282 0.510 0.804 - - 0.020 0.178 0.285 0.468 0.796 - - 0.020 0.177 0.303 0.513 0.820 - -
0.021 0.101 0.181 0.287 0.512 0.876 - 0.021 0.106 0.179 0.296 0.526 0.857 - 0.021 0.109 0.176 0.312 0.515 0.877 -
0.022 0.060 0.110 0.186 0.339 0.562 - 0.022 0.063 0.109 0.199 0.328 0.599 0.992 0.022 0.063 0.112 0.191 0.325 0.583 0.994
0.023 0.038 0.065 0.119 0.218 0.377 0.691 0.023 0.038 0.065 0.118 0.214 0.379 0.678 0.023 0.038 0.064 0.121 0.219 0.388 0.702
0.024 0.024 0.043 0.075 0.129 0.257 0.481 0.024 0.025 0.044 0.079 0.141 0.247 0.468 0.024 0.025 0.043 0.074 0.142 0.266 0.485
0.025 0.016 0.028 0.050 0.098 0.182 0.320 0.025 0.017 0.028 0.050 0.092 0.169 0.360 0.025 0.016 0.029 0.049 0.093 0.177 0.340
pinf
pinf
pinf
0.026 0.011 0.019 0.034 0.061 0.116 0.230 0.026 0.011 0.018 0.033 0.061 0.119 0.228 0.026 0.011 0.019 0.033 0.061 0.117 0.234
0.027 0.008 0.013 0.023 0.044 0.083 0.160 0.027 0.008 0.013 0.022 0.041 0.083 0.157 0.027 0.008 0.013 0.022 0.043 0.083 0.162
0.028 0.006 0.009 0.016 0.029 0.057 0.113 0.028 0.007 0.009 0.016 0.030 0.057 0.112 0.028 0.007 0.010 0.016 0.028 0.056 0.116
0.029 0.005 0.007 0.012 0.020 0.040 0.081 0.029 0.005 0.007 0.012 0.021 0.040 0.081 0.029 0.005 0.007 0.012 0.021 0.040 0.082
0.030 0.005 0.006 0.009 0.015 0.029 0.057 0.030 0.005 0.006 0.009 0.015 0.029 0.056 0.030 0.005 0.006 0.009 0.015 0.029 0.058
0.031 0.004 0.005 0.007 0.011 0.020 0.043 0.031 0.004 0.005 0.007 0.011 0.022 0.043 0.031 0.004 0.005 0.007 0.011 0.021 0.041
10
13
16
19
22
25
10
13
16
19
22
25
10
13
16
19
22
25
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
t0 t0 t0
dmult = 1 dmult = 3 dmult = 5
0.00 0.05 0.10 0.15 0.20 0.25 0.00 0.05 0.10 0.15 0.20 0.25 0.00 0.05 0.10 0.15 0.20 0.25
0.020 2.313 2.314 2.305 2.322 2.309 2.320 0.020 2.327 2.316 2.318 2.311 2.322 2.311 0.020 2.308 2.309 2.310 2.308 2.316 2.321
0.021 2.408 2.416 2.419 2.415 2.420 2.410 0.021 2.403 2.410 2.410 2.410 2.419 2.417 0.021 2.414 2.407 2.410 2.408 2.408 2.413
0.022 2.514 2.512 2.518 2.513 2.520 2.496 0.022 2.500 2.511 2.506 2.509 2.500 2.500 0.022 2.502 2.510 2.503 2.517 2.504 2.507
0.023 2.598 2.610 2.613 2.604 2.600 2.605 0.023 2.604 2.616 2.602 2.602 2.607 2.614 0.023 2.600 2.604 2.600 2.606 2.596 2.598
0.024 2.702 2.700 2.703 2.707 2.696 2.708 0.024 2.699 2.708 2.697 2.706 2.711 2.700 0.024 2.703 2.699 2.706 2.695 2.695 2.689
0.025 2.794 2.809 2.800 2.801 2.788 2.810 0.025 2.794 2.802 2.806 2.797 2.801 2.786 0.025 2.806 2.790 2.794 2.796 2.790 2.787
pinf
pinf
pinf
0.026 2.901 2.900 2.901 2.906 2.897 2.888 0.026 2.893 2.896 2.890 2.894 2.889 2.884 0.026 2.888 2.892 2.895 2.886 2.895 2.884
0.027 2.993 2.998 2.995 2.989 2.990 2.991 0.027 2.988 2.996 2.987 2.985 2.984 2.977 0.027 2.990 2.986 2.987 2.981 2.979 2.983
0.028 3.095 3.083 3.089 3.087 3.085 3.076 0.028 3.080 3.079 3.094 3.077 3.077 3.073 0.028 3.081 3.089 3.075 3.077 3.087 3.068
0.029 3.180 3.187 3.182 3.181 3.174 3.179 0.029 3.171 3.180 3.177 3.179 3.173 3.163 0.029 3.174 3.173 3.175 3.171 3.174 3.171
0.030 3.274 3.283 3.283 3.280 3.271 3.269 0.030 3.276 3.272 3.277 3.281 3.265 3.269 0.030 3.277 3.267 3.276 3.275 3.275 3.263
0.031 3.367 3.369 3.379 3.365 3.376 3.363 0.031 3.367 3.369 3.365 3.373 3.366 3.355 0.031 3.368 3.362 3.367 3.367 3.363 3.360
10
13
16
19
22
25
10
13
16
19
22
25
10
13
16
19
22
25
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
1/
t0 t0 t0
Fig. 4: Top row: fraction of symptomatic infections that become documented in Lombardy as
a function of pinf (y axis) and t0 (x axis). Bottom row: r0 during the pre-lockdown phase. From
left to right: a mortality multiplier dmult relative to China of 1, 3, 5. Colors indicate goodness
of fit of the parameter settings to the true number of reported deaths on March 21 in Lombardy,
with darker cells indicating a better fit. We again find a wide range of possible parameterizations
given the observed data, with a plausible range of 1.14-6.68% for the documentation rate and
of 2.50-3.37 for r0 .
9Documentation rates are lower under most well-fitting parameter settings than previously
reported for Italy overall. Russell et al. (13) reported a 95% confidence interval of 4.6–5.9%,
while our model yields a plausible range of 1.14–6.68%. Our plausible ranges broadly agree
with (13) in that documentation rates are lower in Lombardy than in China; however, our range
contains substantially lower values. By accounting for demographic factors, greater disease
prevalence in Lombardy is possible. For r0 , we obtain the plausible range 2.50–3.37, which is
disjointed with (and higher than) the corresponding plausible range for Hubei.
Containment Policies in Lombardy: Salutary Sheltering and
Physical Distancing
Various interventions – from complete lockdown to physical distancing recommendations –
have been implemented worldwide in response to COVID-19. Within these are a range of al-
ternatives. For example, a government could encourage some percentage of a given age group
to remain sheltered in place, while the rest of the population could continue in-person work
and social activities. Age-specific policies are particularly relevant because they have already
been employed in some countries (e.g., US CDC recommendations that people above 65 years
old shelter in place (23)) and because older age groups are more likely to be able to telecom-
mute (24, 25).
Here, we investigate to what extent the epidemic in Lombardy can be mitigated by encour-
aging a single age group to engage in “salutary sheltering” – a term we coin here to describe
individuals who shelter in place irrespective of their exposure or infectious state – or whether
the entire population must also be asked to adopt physical distancing. Accordingly, we compare
two scenarios. First, we simulate salutary sheltering for a fraction of a single age cohort while
leaving the rest of the population’s behavior unaltered. Second, we simulate salutary sheltering
for a fraction of a single age cohort and physical distancing measures among the rest of the
10population. We model physical distancing as reducing daily contacts by a factor of two for all
individuals (who are not sheltering). The supplementary text discusses concrete suggestions to
implement such physical distancing in various settings along with details of the experiments
described. While this case study applies to Lombardy, it could be extended to other locations
using population-specific demographic data.
Fig. 5 shows the first policy scenario, where a portion of a single age group engages in salu-
tary sheltering but the rest of the population in Lombardy does not adopt physical distancing.
The left plots (Figs. 5(a) and 5(c)) show salutary sheltering of 50% of a single age group, while
the right plots (Figs. 5(b) and 5(d)) show salutary sheltering of 100% of a single age group.
We evaluate these interventions in Lombardy according to two metrics: the percentage of the
population infected (top row) and the total number of deaths (bottom row). Each colored line
shows the impact of salutary sheltering of a single given age group. Additionally, we consider
three baseline policies: the gray dotted curve reflects a baseline scenario with no intervention
(no salutary sheltering, no physical distancing) and the blue and pink dotted curves correspond
to baselines where 50% and 100% of the entire population engages in salutary sheltering, re-
spectively (with no additional physical distancing).
For Lombardy, we observe that even complete sheltering in place of any single age group
leaves at least 60% of the population infected (Fig. 5b), and nearly 70-80% in the more realistic
scenario where only half the group engages in sheltering (Fig. 5a). Notably, the only policies
that limit the percentage of infected, or the total number of deaths, would require sheltering
50% ((a) and (c)) to 100% ((b) and (d)) of the population in Lombardy. Except for these
two scenarios, illustrated by the blue and pink dotted curves respectively, the total number of
deaths as projected by our model in Lombardy is correspondingly large (above 200 thousand)
in the absence of any level of physical distancing and can only be significantly ameliorated by
completely sheltering the entire population of 70 years and older (Fig. 5d).
11100 100
Percentage of infected
Percentage of infected
Absence of Absence of
intervention intervention
80 Ages 0-14 80 Ages 0-14
Ages 15-29 Ages 15-29
Ages 30-49 Ages 30-49
60 Ages 50-69 60 Ages 50-69
Ages 70+ Ages 70+
40 All ages 40 All ages
50% sheltered 50% sheltered
All ages All ages
100% sheltered 100% sheltered
20 20
0 0
0 20 40 60 80 100 120 0 20 40 60 80 100 120
Days since patient zero Days since patient zero
(a) (b)
400 400
Total deaths (thousands)
Total deaths (thousands)
Absence of Absence of
350 intervention 350 intervention
Ages 0-14 Ages 0-14
300 Ages 15-29 300 Ages 15-29
250 Ages 30-49 250 Ages 30-49
Ages 50-69 Ages 50-69
200 Ages 70+ 200 Ages 70+
All ages All ages
150 50% sheltered 150 50% sheltered
All ages All ages
100 100% sheltered 100 100% sheltered
50 50
0 0
0 20 40 60 80 100 120 0 20 40 60 80 100 120
Days since patient zero Days since patient zero
(c) (d)
Fig. 5: Effect of salutary sheltering for a fraction of each age group on infections in Lombardy
(top row, (a) and (b)) and deaths (bottom row, (c) and (d)), without physical distancing by
others. Left-hand side, (a) and (c): salutary sheltering of 50% of a single age group. Right-hand
side, (b) and (d): salutary sheltering of 100% of a single age group. The red vertical dashed line
indicates the start of the intervention. Each solid colored curve represents sheltering a specific
age cohort, the gray dotted curve presents the “no intervention” scenario, and the blue and
pink dotted curves correspond to baselines where 50% and 100% of the population is sheltered,
respectively.
12100 100
Percentage of infected
Percentage of infected
Absence of Absence of
intervention intervention
80 Ages 0-14 80 Ages 0-14
Ages 15-29 Ages 15-29
Ages 30-49 Ages 30-49
60 Ages 50-69 60 Ages 50-69
Ages 70+ Ages 70+
40 All ages 40 All ages
50% sheltered 50% sheltered
All ages All ages
100% sheltered 100% sheltered
20 20
0 0
0 20 40 60 80 100 120 0 20 40 60 80 100 120
Days since patient zero Days since patient zero
(a) (b)
400 400
Total deaths (thousands)
Total deaths (thousands)
Absence of Absence of
350 intervention 350 intervention
Ages 0-14 Ages 0-14
300 Ages 15-29 300 Ages 15-29
250 Ages 30-49 250 Ages 30-49
Ages 50-69 Ages 50-69
200 Ages 70+ 200 Ages 70+
All ages All ages
150 50% sheltered 150 50% sheltered
All ages All ages
100 100% sheltered 100 100% sheltered
50 50
0 0
0 20 40 60 80 100 120 0 20 40 60 80 100 120
Days since patient zero Days since patient zero
(c) (d)
Fig. 6: Effect of salutary sheltering for a fraction of each age group on infections in Lombardy
(top row, (a) and (b)) and deaths (bottom row, (c) and(d)), when combined with physical dis-
tancing by the rest of the population. Left-hand side, (a) and (c): salutary sheltering of 50% of
a single age group. Right-hand side, (b) and (d): salutary sheltering of 100% of a single age
group. The red vertical dashed line indicates the start of the intervention. Each solid colored
curve represents sheltering a specific age cohort, the gray dotted curve presents the “no inter-
vention” scenario, and the blue and pink dotted curves correspond to baselines where 50% and
100% of the population is sheltered, respectively.
13However, combining partial salutary sheltering of a single age group with physical distanc-
ing by the rest of the population has a substantially greater impact for Lombardy, as shown in
Fig. 6. The fraction of the population infected drops to 50% or below (depending on which age
group and what percentage is sheltered) four months following the beginning of the outbreak.
The total number of deaths projected for this time horizon decreases even more substantially,
to the range of 100–150 thousand (as compared to 275–360 thousand for the previous scenario
with 50% sheltering by a single age group and no population-wide physical distancing). In a
scenario where physical distancing is adopted by everyone in Lombardy, there is only a small
benefit to sheltering 100% of an age group (as opposed to 50%), particularly with respect to
total deaths (6b and 6d), instead of 50% (6a and 6c). The age group sheltered need not be 70+
either; in fact, 50% salutary sheltering of the 30–49 age group in Lombardy has a somewhat
larger impact. Differences in the effectiveness of sheltering different age groups in a particular
location stem from the interplay of contact patterns (the 30–49 group has many daily phys-
ical interactions in Italy (11)), risk of mortality from the disease (older groups are at higher
risk (3, 23)), and the size of the age group (the 30–49 group is the second largest generation in
Italy (26)). However, they are not reducible to any single factor. Figs. S4–S7 show a sensitivity
analysis incorporating changes in model parameters due to potential underreporting or overre-
porting of deaths. Our main conclusions for Lombardy remain unaltered even after accounting
for reporting discrepancies.
Building upon Lombardy, our model suggests that hybrid policies that combine targeted
salutary sheltering by one part of the population and physical distancing by the rest could be
as effective at limiting the final outbreak size as salutary sheltering of an entire sub-population,
while preserving social ties and avoiding complete disruption of the economy. Our analysis can
be readily extended to other locations by parameterizing our model for a new population using
existing demographic data and age-stratified contact patterns.
14Discussion and Future Work
In this study, we developed a model of SARS-CoV2 transmission that incorporates household
structure, age distributions, comorbidities, and age-stratified contact patterns in Hubei, China,
and Lombardy, Italy, and created simulations using available demographic information from
these two locations. Our findings suggest that population-wide sheltering in place may not be
necessary to mitigate the spread of COVID-19. Instead, targeted salutary sheltering of specific
age groups combined with adherence to physical distancing by the rest of the population may
be sufficient to thwart a substantial fraction of infections and deaths. Physical distancing could
be achieved by engaging in activities such as staggered work schedules, increasing spacing in
restaurants, and prescribing times to use the gym or grocery store. Specific mechanisms and
considerations for implementing physical distancing are documented in the supplementary text.
Moreover, we note that depending on the demography and contact structure of the population,
the groups targeted for salutary sheltering need not be the oldest in the population to be effective.
From a pragmatic perspective, targeted salutary sheltering may not be realistic for all pop-
ulations. Its feasibility relies on access to safe shelter, which does not reflect reality for all
individuals. In addition, sociopolitical realities may render this recommendation more feasi-
ble in some populations than in others. Concerns for personal liberty, discrimination against
sub-segments of the population, and societal acceptability may prevent the adoption of targeted
salutary sheltering in some regions of the world. Allowing salutary sheltering to operate on a
voluntary basis using a shift system (rather than for indefinite time periods) may address some
of these issues. Future work should formulate targeted recommendations about salutary shelter-
ing and physical distancing by age group or other stratification adapted to a specific country’s
workforce.
Existing modeling work of COVID-19 has largely focused on simpler compartmental or
15branching process models which do not allow for the simulation of targeted policies as de-
scribed above. While these models have played an important role in estimating key parameters
such as r0 (5, 7) or the rate at which infections are documented (27), and in the evaluation
of prospective non-pharmaceutical interventions (28, 29), they do not characterize how differ-
ences in demography impact the course of an epidemic in a particular location. Our focus on
population-specific demography allows for further refinement of current mortality estimates and
is a strength of this study. r0 estimates in this study are generally comparable to other estimates
in the literature (30), although our model yields higher estimates for Lombardy than Hubei –
possibly due to differential mask-wearing practices (31) or adoption of behavioral interventions
such as hand hygiene (32). Similarly, our model suggests a higher mortality rate in Lombardy
than Hubei for reasons beyond demography. Possible explanations include variability in ICU
capacity (33), coordination challenges in Lombardy (33), documented prevalence of antibiotic
resistance in secondary bacterial infections (34), and perhaps greater background population
exposure to other novel coronaviruses in China (35). Reporting rates estimated in this study
were generally lower than those in prior studies (13). This is likely due the fact that our simula-
tions produce infection rates that are not homogeneous across age groups, attributable to higher
reported contacts for younger groups (11, 18). These differences highlight the potential impact
of demography on COVID-19 dynamics, a key feature of our model.
Another advantage of our framework is its flexibility. The model is modifiable to test differ-
ent policies or simulate additional features with greater fidelity across a variety of populations.
Examples of future work that can be accommodated include analysis of contact tracing and
testing policies, health system capacity, and multiple waves of infection after lifting physical
distancing restrictions. Our model includes the necessary features to simulate these scenarios
while remaining otherwise parsimonious, a desirable feature given uncertainties in data report-
ing.
16This study has several limitations. While several comorbidities associated with mortality
in COVID-19 were accounted for, the availability of existing data limited the incorporation of
all relevant comorbidities. Most notably, chronic pulmonary disease was not included although
it has been associated with mortality in COVID-19 (19), nor was smoking, despite its preva-
lence in both China and Italy (36, 37). Gender-mediated differences were also excluded, which
may be important for both behavioral reasons (e.g., adoption of hand-washing (38, 39)) and
biological reasons (e.g, the potential protective role of estrogen in SARS-CoV infections (40)).
Nevertheless, these factors can all be incorporated into the model as additional data becomes
available.
It is also worth noting that we have not yet attempted to model super-spreader events in
our existing framework. Such events may have been especially consequential in South Korea
(41), and future work could attempt to more closely model the epidemic there by incorporating
a dispersion parameter into the contact distribution, a method which has been used in other
models (5).
Despite these limitations, this study demonstrates the importance of considering population
and household demographics when attempting to better define outbreak dynamics for COVID-
19. Furthermore, this model highlights potential policy implications for non-pharmaceutical
interventions that account for population-specific demographic features and may provide alter-
native strategies for national and regional governments moving forward.
References and Notes
1. D. Baud, et al., The Lancet (2020).
2. Center for Systems Science and Engineering at Johns Hopkins University, Coronavirus
COVID-19 Global Cases (2020). https://coronavirus.jhu.edu/map.html.
173. F. Zhou, et al., The Lancet (2020).
4. B. Xu, et al., Scientific Data 7 (2020).
5. J. Riou, C. Althaus, Eurosurveillance 25 (2020).
6. R. Li, et al., Science (2020).
7. A. Kucharski, et al., The Lancet Infectious Diseases (2020).
8. P. Van den Driessche, M. Li, J. Muldowney, Canadian Applied Mathematics Quarterly 7,
409 (1999).
9. F. Ball, E. Knock, P. O’Neill, Mathematical Biosciences 266, 23 (2015).
10. G. Roth, et al., The Lancet 392, 1736 (2018).
11. K. Prem, A. Cook, M. Jit, PLoS Computational Biology 13, e1005697 (2017).
12. South China Morning Post, Coronavirus: China’s first confirmed
COVID-19 case traced back to November 17 (2020). https://
www.scmp.com/news/china/society/article/3074991/
coronavirus-chinas-first-confirmed-covid-19-case-traced-back.
13. T. Russell, et al., Using a delay-adjusted case fatality ratio to estimate under-reporting
(2020). https://cmmid.github.io/topics/covid19/severity/global_
cfr_estimates.html. Accessed 03-26-20.
14. H. Bai, et al., Radiology (2020).
15. G. Onder, G. Rezza, S. Brusaferro, The Journal of the American Medical Association
(2020).
1816. M. S. Majumder, K. D. Mandl, The Lancet Global Health .
17. R. Verity, et al., medRxiv (2020).
18. J. Mossong, et al., PLoS medicine 5 (2008).
19. C. C. for Disease Control, Prevention, China CDC Weekly 2,
113 (2020). http://weekly.chinacdc.cn//article/id/
e53946e2-c6c4-41e9-9a9b-fea8db1a8f51.
20. W. H. O. China, Report of the WHO-China Joint Mis-
sion on Coronavirus Disease 2019 (COVID-19) (2020). https:
//www.who.int/docs/default-source/coronaviruse/
who-china-joint-mission-on-covid-19-final-report.pdf.
21. J. Horowitz, E. Bubola, E. Polvedo, The New York Times (2020).
https://www.nytimes.com/2020/03/21/world/europe/
italy-coronavirus-center-lessons.html.
22. V. Di Donato, S. McKenzie, L. Borghese, CNN
(2020). https://www.cnn.com/2020/03/28/europe/
italy-coronavirus-cases-surpass-china-intl/index.html.
23. C. for Disease Control, Prevention, People who are at higher risk for se-
vere illness (2020). https://www.cdc.gov/coronavirus/2019-ncov/
need-extra-precautions/people-at-higher-risk.html.
24. P. Mateyka, M. Rapino, L. C. Landivar, Home-based workers in the United States (2012).
https://www.census.gov/prod/2012pubs/p70-132.pdf.
1925. U. B. of Labor Statistics, Labor force statistics from the current population survey (2019).
https://www.bls.gov/cps/cpsaat08.htm.
26. United Nations (2019). https://population.un.org/wpp/.
27. P. De Salazar, R. Niehus, A. Taylor, C. Buckee, M. Lipsitch, medRxiv (2020).
28. S. Kissler, C. Tedijanto, M. Lipsitch, Y. Grad, medRxiv (2020).
29. J. Hellewell, et al., The Lancet Global Health (2020).
30. M. Majumder, K. Mandl, SSRN (2020).
31. S. Feng, et al., The Lancet Respiratory Medicine (2020).
32. G. Di Giuseppe, R. Abbate, L. Albano, P. Marinelli, I. Angelillo, BMC Infectious Diseases
8, 36 (2008).
33. G. Grasselli, A. Pesenti, M. Cecconi, The Journal of the American Medical Association
(2020).
34. A. Cassini, et al., ECDC country visit to Italy to discuss antimicrobial resis-
tance issues (2017). https://www.ecdc.europa.eu/sites/default/files/
documents/AMR-country-visit-Italy.pdf.
35. V. Cheng, S. Lau, P. Woo, K. Y. Yuen, Clinical Microbiology Reviews 20, 660 (2007).
36. M. Parascandola, L. Xiao, Translational Lung Cancer Research 8, S21 (2019).
37. A. Lugo, et al., Tumori Journal 103, 353 (2017).
38. M. Guinan, M. McGuckin-Guinan, A. Sevareid, American Journal of Infection Control 25,
424 (1997).
2039. D. Johnson, D. Sholcosky, K. Gabello, R. Ragni, N. Ogonosky, Perceptual and Motor Skills
97, 805 (2003).
40. R. Channappanavar, et al., The Journal of Immunology 198, 4046 (2017).
41. British Broadcasting Corporation, Coronavirus: South Korea emergency measures as infec-
tions increase (2020). https://www.bbc.com/news/world-asia-51582186.
42. Y. Bai, et al., The Journal of the American Medical Association (2020).
43. C. Rothe, et al., New England Journal of Medicine (2020).
44. Z. Du, et al., Emerging Infectious Diseases (2020).
45. P. Allison, Survival analysis using SAS: a practical guide (SAS Institute, 2010).
46. D. Collett, Modelling survival data in medical research (CRC Press, 2015).
47. S. Lauer, et al., Annals of Internal Medicine (2020).
48. Y. Liu, R. Eggo, A. Kucharski, The Lancet (2020).
49. Z. Hu, X. Peng, The Journal of Chinese Sociology 2, 9 (2015).
50. D. He, X. Zhang, Z. Wang, Y. Jiang, China Population and Development Studies 2, 430
(2019).
51. Statista, Household structures in Italy in 2018 (2018). https://www.statista.
com/statistics/730604/family-structures-italy/, Last Accessed:
2020-03-28.
52. Statista, Number of single-person households in Italy from 2012 to
2018 (2018). https://www.statista.com/statistics/728061/
21number-of-single-person-households-italy/, Last Accessed: 2020-
03-28.
53. Statista, Number of couples with children in Italy from 2012 to 2018, by num-
ber of children (2018). https://www.statista.com/statistics/570106/
number-of-couples-with-children-italy/, Last Accessed: 2020-03-28.
54. Statista, Biennial average number of household members in Italy from 2012
to 2018 (2018). https://www.statista.com/statistics/671945/
biennial-average-number-of-families-with-children-italy/,
Last Accessed: 2020-03-28.
55. Statista, Number of single parents in Italy from 2011 to 2018, by number of
children (2018). https://www.statista.com/statistics/570234/
number-of-single-parents-with-children-in-italy-by-number-of-children/,
Last Accessed: 2020-03-28.
56. E. Carrà, M. Lanz, S. Tagliabue, Journal of Comparative Family Studies 45, 235 (2014).
57. Y. Xu, et al., The Journal of the American Medical Association 310, 948 (2013).
58. Z. Wang, et al., Circulation 137, 2344 (2018).
59. P. Modesti, et al., International Journal of Hypertension (2017).
60. Y. Tatsumi, T. Ohkubo, Hypertension Research 40, 795 (2017).
61. C. C.-. R. Team, Severe outcomes among patients with coronavirus disease 2019 (COVID-
19)—United States, February 12–March 16, 2020 (2020). https://www.cdc.gov/
mmwr/volumes/69/wr/mm6912e2.htm.
2262. X. Peng, Science 333, 581 (2011).
63. New York Times, China tightens Wuhan lockdown in wartime battle with coron-
avirus (2020). https://www.nytimes.com/2020/02/06/world/asia/
coronavirus-china-wuhan-quarantine.html.
64. J. Zhang, et al., medRxiv (2020).
65. Italian National Institute of Statistics, Median age in Lombardy (2019). https:
//www4.istat.it/it/lombardia/dati?qt=gettable&dataset=DCIS_
INDDEMOG1&dim=21,0,0, Last Accessed: 2020-03-28.
66. C. W. Factbook, Field listing: median age (2020). https://www.cia.gov/
library/publications/the-world-factbook/fields/343.html, Last
Accessed: 2020-03-28.
67. L. Tondo, The Guardian (2020). https://www.theguardian.com/world/
2020/mar/18/italy-charges-more-than-40000-people-violating-lockdown-coro
68. Wikipedia, 2020 coronavirus pandemic in italy (2020). https://en.wikipedia.
org/wiki/2020_coronavirus_pandemic_in_Italy, Last Accessed: 2020-03-
29.
69. Wikipedia, Timeline of the 2019–20 coronavirus pandemic in November 2019 – Jan-
uary 2020 (2020). https://en.wikipedia.org/wiki/Timeline_of_the_
2019-20_coronavirus_pandemic_in_November_2019_-_January_
2020, Last Accessed: 2020-03-28.
70. F. Carinci, British Medical Journal (2020).
71. J. Miller, Bulletin of Mathematical Biology 74, 2125 (2012).
2372. A. Remuzzi, G. Remuzzi, The Lancet (2020).
73. J. Lourenco, et al., medRxiv (2020).
74. T. I. C. C.-. R. Team, Report 12: The global impact of COVID-19
and strategies for mitigation and suppression (2020). https://www.
imperial.ac.uk/mrc-global-infectious-disease-analysis/
news--wuhan-coronavirus/.
75. U.S. Bureau of Labor Statistics, American time use survey (2018). https://www.bls.
gov/tus/.
76. N. Qualls, et al., CDC MMWR Recommendations and Reports 66, 1 (2017).
77. Oklahoma County Department of Health, Social distancing fact sheet (2019).
https://www.occhd.org/application/files/3715/7013/9751/
Social_Distancing.pdf, Last Accessed: 2020-04-05.
78. F. Ahmed, N. Zviedrite, A. Uzicanin, BMC Public Health 18, 518 (2018).
79. P. Totterdell, Handbook of work stress, J. Barling, E. K. Kelloway, M. R. Frone, eds. (Sage
publications, 2004), chap. 3.
80. L. DeRigne, P. Stoddard-Dare, L. Quinn, Health Affairs 35, 520 (2016).
81. M. W. Fong, et al., Emerging Infectious Diseases 26 (2020).
82. F. Aimone, Public Health Reports 125, 71 (2010).
83. L. Ecola, T. Light, RAND Corporation pp. 1–45 (2009).
2484. NBC News, Walmart will limit customers and create one-way traffic in-
side its stores (2020). https://www.nbcnews.com/news/us-news/
walmart-will-limit-customers-create-one-way-traffic-inside-its-n1176461
85. NBC Connecticut, New social distancing measures take effect at stores across
Connecticut (2020). https://www.nbcconnecticut.com/news/local/
new-social-distancing-measures-enacted-at-stores-across-connecticut/
2249937/.
86. A. Selyukh, Supermarkets add ’senior hours’ for vulnera-
ble shoppers (2020). https://www.npr.org/sections/
coronavirus-live-updates/2020/03/19/818488098/
supermarkets-add-senior-hours-for-vulnerable-shoppers.
87. Centers for Disease Control and Prevention (2007).
88. WGNTV, This student created a network of ‘shopping angels’ to help the elderly
get groceries during the COVID-19 pandemic (2020). https://wgntv.com/news/
this-student-created-a-network-of-shopping-angels-to-help-the-elderly-g
89. American Broadcasting Company, Santa Monica volunteers protect se-
niors with new grocery delivery service (2020). https://abc7.com/
coronavirus-seniors-covid-19-groceries/6045815/.
90. K. Gardner, K. Lister, 2017 state of telecommuting in the U.S. employee workforce (2017).
https://www.flexjobs.com/2017-State-of-Telecommuting-US/.
91. T. Noah, ‘it makes me very angry’: Coronavirus damage ripples across the
workforce (2020). https://www.politico.com/news/2020/03/09/
america-workers-outbreak-uncertainty-124191.
2592. Drew Desilver, As coronavirus spreads, which U.S. work-
ers have paid sick leave – and which don’t? (2020).
https://www.pewresearch.org/fact-tank/2020/03/12/
as-coronavirus-spreads-which-u-s-workers-have-paid-sick-leave-and-which
93. D. Card, Carnegie-Rochester Conference Series on Public Policy (Elsevier, 1990), vol. 33,
pp. 137–168.
94. C. for Disease Control, Prevention, Interim pre-pandemic planning guidance: Commu-
nity strategy for pandemic influenza mitigation in the united states— early, targeted, lay-
ered use of nonpharmaceutical interventions (2007). https://www.cdc.gov/flu/
pandemic-resources/pdf/community_mitigation-sm.pdf.
95. Q. Li, et al., New England Journal of Medicine (2020).
Acknowledgments
Funding: This work was supported in part by the Army Research Office by grant MURI
W911NF1810208 and in part by grant T32HD040128 from the Eunice Kennedy Shriver Na-
tional Institute of Child Health and Human Development, National Institutes of Health. Killian
was supported by the National Science Foundation Graduate Research Fellowship under Grant
No. DGE1745303. Perrault and Jabbari were supported by the Harvard Center for Research on
Computation and Society. The funders had no role in study design, data collection and analysis,
decision to publish, or preparation of the manuscript.
Author contributions: In accordance with the ICMJE authorship guidelines, BW, MC, JAK,
HCO, AM, SJ, and AP acquired, analyzed, and interpreted data for the work. BW, MC, SJ, and
AP also drafted the work. AND, MT, and MSM made substantial contributions to the concep-
tion or design of the work and revised the work critically for important intellectual content.
26Competing interests: All authors declare no competing interests.
Data and materials availability: All code and data are available at https://github.
com/bwilder0/COVID19-Demography.
Supplementary Materials
Materials and Methods
Supplementary Text
Figs. S1 to S7
Tables S1 to S3
References (41-95)
27Supplementary Materials for
Modeling the Impact of Demography on COVID-19 Dynamics
in Hubei and Lombardy
Bryan Wilder1∗ , Marie Charpignon2 , Jackson A. Killian1 , Han-Ching Ou1 ,
Aditya Mate1 , Shahin Jabbari1 , Andrew Perrault1 , Angel N. Desai3 ,
Milind Tambe1∗ , Maimuna S. Majumder4,5∗
1
School of Engineering and Applied Sciences, Harvard University, Cambridge, MA, USA
2
MIT Institute for Data, Systems, and Society, Cambridge, MA, USA
3
International Society for Infectious Diseases, Brookline, MA, USA
4
Department of Pediatrics, Harvard Medical School, Boston, MA, USA
5
Computational Health Informatics Program, Boston Children’s Hospital, Boston, MA, USA
*Corresponding author. Email: bwilder@g.harvard.edu (B.W.); milind_tambe@harvard.edu (M.T.);
Maimuna.Majumder@childrens.harvard.edu (M.S.M.)
This PDF file includes:
Materials and Methods
Supplementary Text
Figs. S1 to S7
Tables S1 to S3
1Materials and Methods
Model description
We develop an agent-based model for COVID-19 spread which accounts for the distributions of age, household types,
comorbidities, and contact between different age groups in a given population. The model follows a susceptible-exposed-
infectious-removed (SEIR) template [8, 9]. Specifically, we simulate a population of n agents (or individuals), each with
an age ai , a set of comorbidities ci , and a household (a set of other agents). We stratify age into ten-year intervals and
incorporate hypertension and diabetes as comorbidities. These comorbidities are common worldwide [10] and have
been associated with a higher risk of in-hospital death for COVID-19 patients [3]. However, our model can be expanded
to include other comorbidities of interest in the future. The specific procedure we use to sample agents from the joint
distribution of age, household structures, and comorbidities is described below.
The simulation tracks two states for each individual: the infection state and the isolation state. The infection state
is divided into {susceptible, exposed, infectious, removed}. Susceptible individuals are those who have never been
contacted by an infectious individual. Exposed individuals are those who have had contact with an infectious individual,
though not all exposed individuals become infectious. If an exposed individual contracts the disease, they proceed
to the infectious state.1 Infectious is further subdivided into severity levels {asymptomatic, mild, severe, critical}.
We interpret mild severity as symptomatic (but not requiring hospitalization), severe as requiring hospitalization, and
critical as eligible for intensive care unit (ICU) care. The removed state is further subdivided into {recovered, deceased}.
Individuals in all severity levels can transmit the disease, but those in the asymptomatic state do so at a rate α < 1 times
that of symptomatic cases. The decision to incorporate reduced transmission for asymptomatic individuals is based on
the fact that, though infection by asymptomatic individuals has been observed in case clusters and in examinations of
serial intervals [42, 43, 44], available evidence suggests that individuals with no or limited symptoms are less infectious
than those with severe symptoms [6]. Currently, our simulation incorporates two levels of infectiousness (before and
after the onset of symptoms), but it can be adjusted as better information on how viral shedding increases with severity
of illness becomes available. We acknowledge that our assumptions surrounding transmissibility and disease severity –
as derived from existing literature – may serve as a limitation of our model, as many of these factors are evolving over
time.
Each individual has a separate isolation state {isolated, not isolated}. If isolated, the individual is unable to infect
others. We assume that (1) asymptomatic individuals are never isolated, (2) mild individuals become isolated over
a mean time of λisolate days (see Table 1) after the onset of symptoms, and (3) all severe and critical individuals are
isolated. However, our simulation framework can easily accommodate different sets of assumptions about isolation (for
example, preemptively isolating exposed individuals if they are known to have had contact with an infectious agent).
The disease is transmitted over a contact structure, which is divided into in-household and out-of-household groups.
Each agent has a household consisting of a set of other agents. Individuals infect members of their households at a
higher rate than out-of-household agents. We model out-of-household transmission using country-specific estimated
contact matrices [11]. These matrices state the mean number of daily contacts an individual of a particular age strata has
with individuals from each of the other age strata. We assume demographics (including age and household distribution)
in Hubei and Lombardy are well-approximated by country-level data.
The model iterates over a series of discrete time steps, each representing a single day, from a starting time t0 to an
end time T . There are two main components to each time step: disease progression and new infections. The progression
component is modeled by drawing two random variables for each individual each time they change severity levels (e.g.
on entering the mild state). The first random variable is Bernoulli and indicates whether the individual will recover
or progress to the next severity level. The second variable represents the amount of time until progression to the next
severity level. We use exponential distributions for almost all time-to-event distributions, a common choice in the
absence of specific distributional information [45, 46]. The exception is the incubation time between asymptomatic and
2
mild states, where more specific information is available; here, we use a log-normal distribution (see µe→m and σe→m
in Table 1) based on estimates by [47]. Table 1 summarizes all distributions and their parameters.
In the new infections component, individuals in the susceptible state may enter the exposed state. Infected
individuals infect each of their household members with probability ph at each time step. ph is calibrated so that the
total probability of infecting a household member before either isolation or recovery matches the estimated secondary
attack rate for household members of COVID-19 patients (i.e., the average fraction of household members infected) [48].
Infected individuals draw outside-of-household contacts from the general population using the country-specific contact
matrix. For an infected individual of age group i, we sample wij ∼ Poisson(Mij ) contacts for each age group j,
1
Currently, our simulation implementation does not separately track individuals who are exposed but do not become infected, and
instead groups them with the susceptible population. This is because we assume that, if exposed again, they will become infected
with the same probability as an individual who has never been exposed. However, the implementation can be modified to support
either differing probabilities of contracting the disease after first exposure or policies that treat exposed and susceptible individuals
differently.
2where M is the country-specific contact matrix. Poisson distributions are a standard choice for modeling contact
distributions [11]. Then, we sample wij contacts of age j uniformly with replacement, and each contact is infected with
the probability pinf , the probability of infection given contact. This probability is an unknown; our experiments test a
range of values, and we report which values give results consistent with observations from Lombardy and Hubei.
Sampling agents
Our process for sampling agents follows three steps that successively sample households, individual agents within
households, and comorbidities for each agent. Because the full joint distributions over all of these quantities are not
known, we implement a sampling procedure that respects the marginal distributions of household structure and age, as
well as the marginal distribution for the occurrence of comorbidities within each age group.
First, we use information on the distribution of household structures to draw a type of household (e.g., single person,
couple, nuclear family, or multigenerational family). Second, we sample the ages of the individual agents according to
their role in the household (e.g., parent, child, or grandparent) combined with information about the age distribution of
the population and the intergenerational interval. For China, we use household distributions from the 2010 Chinese
census [49], intergenerational intervals from [50], and the age distribution provided by UN population statistics [26].
For Italy, we use demographic statistics from Statista online portal about the following: household structure distribution
[51], single-person households [52], couples with children [53] and corresponding family size [54], and single parents
with children [55]. Furthermore, we assume that children could stay within the family until the age of 30 and that
couples without children were aged 30+, to account for societal patterns reported in familial studies which may have
affected household distribution metrics [56]. Third, we sample comorbidities from the corresponding country- and
age-specific distributions. For China, we use estimates on age-specific prevalence of diabetes [57] and hypertension [58].
For Italy, we use estimates from the Global Burden of Disease study on diabetes [10] and a recent study of age-stratified
hypertension prevalence [59]. We ensure that diabetes and hypertension are appropriately correlated using a single
global estimate for the probability of hypertension in individuals with diabetes [60].
Estimating disease progression from age and comorbidities
Many of the parameters for this model are assigned values based on estimates in the literature, shown in Table 1.
However, we currently lack a detailed understanding of the joint impact of age and comorbidities on disease progression
and mortality. Currently, case fatality rates (CFRs) are available either by age or by individual comorbidity, but not
for each specific combination of age and comorbidities. To obtain these estimates, we model the CFR with a logistic
regression fit to CFRs from the Chinese Center for Disease Control and Prevention (China CDC) [19], discussed in the
next section. This model yields pm→d (ai , ci ), the country-independent probability that an individual i of age ai and
comborbidity status ci will die if infected with SARS-CoV-2. Corrections for country-specific differences in mortality
are handled via the parameter dmult .
The simulation also requires specific values for the probabilities of transitioning between the disease states mild,
severe, critical, and death. However, there is currently insufficient information available to infer the probabilities of these
individual transitions for each combination of age and comorbidity. We assume that while the absolute values of these
probabilities may vary based on age and comorbidity, the ratios between them do not exhibit such strong dependency. In
particular, we assume that there are coefficients γs→c (ai ) and γc→d such that ps→c (ai , ci ) = γs→c (ai )pm→s (ai , ci ) and
pc→d (ai ) = γc→d pm→s (ai , ci ). We allow γs→c (ai ) to be age-specific while assuming that γc→d is age-homogeneous
because of the information currently available to estimate them; namely, we estimate γs→c (ai ) based on the relative
probabilities of hospitalization and ICU admission by age group in the US [61] and γc→d based on the probability of
death for all critical patients in China [19]. Note that we assume both coefficients to be independent of the comorbodities
ci . Then, we can solve for pm→s (ai , ci ) such that
pm→s (ai , ci ) · γs→c (ai )pm→s (ai , ci ) · γc→d pm→s (ai , ci ) = pm→d (ai , ci ),
and set ps→c (ai , ci ) and pc→d (ai , ci ) accordingly. Future work can relax the assumptions in this process as more
information becomes available about how age and comorbidity impact the progression between disease states.
Estimating mortality from age and comorbidities
We require a model of pm→d (ai , ci ), however existing data sources only specify pm→d (ai ) and pm→d (ci ). To infer the
joint distribution, we assume a linear (logistic) interaction between age bracket, diabetes status, and hypertension status.
Specifically, we assume
pm→d (ai , ci ) = σ βage (ai ) + βdiabetes 1 [diabetes ∈ ci ] + βhypertension 1 [hypertension ∈ ci ] ,
3You can also read