Myofibrillar myopathy with desmin accumulation in a young Australian Shepherd dog
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Neuromuscular Disorders 14 (2004) 399–404
www.elsevier.com/locate/nmd
Myofibrillar myopathy with desmin accumulation
in a young Australian Shepherd dog
G. Diane Sheltona,*, Veronique Sammutb, Saschiko Hommac,
Shinichi Takayamac, Andrew P. Mizisina
a
Department of Pathology, University of California San Diego, La Jolla, CA 92093-0709, USA
b
Veterinary Medical Referral Service, Buffalo Grove, IL, USA
c
The Burnham Institute, La Jolla, CA, USA
Received 18 December 2003; received in revised form 26 March 2004; accepted 31 March 2004
Abstract
A 1-year-old male neutered Australian Shepherd dog was referred to a veterinary specialist for evaluation of chronic lameness,
contractures, and exercise intolerance. Serum creatine kinase was elevated, and electromyography showed complex repetitive discharges.
Cardiomyopathy was clinically identified. Muscle biopsies evaluated by light and electron microscopy, and immunohistochemistry revealed
the presence of a myofibrillar myopathy with accumulation of desmin and other proteins. These observations represent the first report of
myofibrillar myopathy in the dog.
q 2004 Elsevier B.V. All rights reserved.
Keywords: Canine; Myopathy; Myofibrillar; Desmin
1. Introduction 2. Case report
In humans, myofibrillar myopathy, consisting of focal 2.1. Clinical history
myofibrillar dissolution and accumulation of the products of
this degradative process, has been described [1,2]. Charac- A 1-year-old male neutered Australian Shepherd dog was
referred to a veterinary orthopedist for evaluation of
teristic pathological changes are evident in muscle cryostat
lameness of both thoracic limbs. The dog was adopted
sections and include abnormal variability in fiber size, and
from a shelter at 8 months of age and an abnormal gait was
fibers containing small particles, hyaline structures, small
reported at that time. Physical examination revealed
vacuoles rimmed by membranous material, and deposits of
bilateral contractures of the carpal flexor muscles. Radio-
amorphous, granular or hyaline material [1]. With the
graphs of the thoracic limbs were unremarkable. Following
exception of canine X-linked muscular dystrophy, very few
a 2-month course of therapy with prednisone (5 mg daily),
congenital or chronic non-inflammatory myopathies have splints, and physical therapy, the dog was referred to a
been described in the dog [3]. Here we describe a 1-year-old veterinary neurologist. The dog was ambulatory but very
dog with a history of chronic generalized weakness and reluctant to walk, advancing only a few steps before it
muscle atrophy. Morphological and immunohistochemical would stop and sit down. There was generalized weakness
evaluation of muscle biopsies revealed pathological changes characterized by tremors of the limbs when standing,
that are consistent with myofibrillar myopathy and similar marked ventroflexion of the neck, and moderate generalized
to those described in humans. To our knowledge, this is muscle atrophy. Cranial nerve examination was normal with
the first description of myofibrillar myopathy occurring in the exception of a weak palpebral reflex. Spinal reflexes
a dog. were reduced. The neuroanatomical localization suggested a
generalized lower motor neuron disorder.
* Corresponding author. Tel.: þ 1-858-534-1537; fax: þ1-858-534-0391. Esophageal dilatation was present on thoracic radio-
E-mail address: gshelton@ucsd.edu (G.D. Shelton). graphs. The serum creatine kinase concentration was
0960-8966/$ - see front matter q 2004 Elsevier B.V. All rights reserved.
doi:10.1016/j.nmd.2004.03.010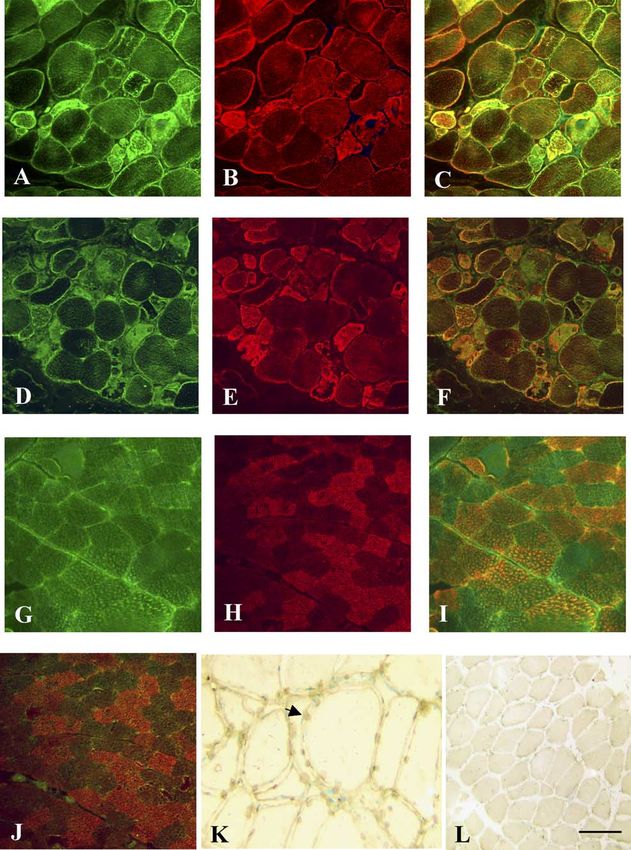
400 G.D. Shelton et al. / Neuromuscular Disorders 14 (2004) 399–404
elevated at 4,127 IU/l (canine reference 10 – 200). An muscle fibers (Fig. 2C and F). Fibers that were not
edrophonium chloride challenge was performed that overtly abnormal did not stain for caspases. Of interest is
resulted in no improvement in muscle strength and an the absence of BAG3 staining in several fibers. For
acetylcholine receptor antibody titer was negative, render- comparison, similar stainings were performed in normal
ing a diagnosis of acquired myasthenia gravis unlikely. dog muscle (Fig. 2G – I). BAG3 staining co-localized with
Electromyography revealed complex repetitive discharges desmin in normal muscle in a speckled pattern demon-
and sparse fibrillation potentials in all muscles evaluated. strating Z-disk localization. As expected, labeling for
Muscle and peripheral nerve biopsies were collected. activated caspases was not observed in the normal dog
muscle (Fig. 2J). For TUNEL assays, apoptotic nuclei
2.2. Histopathology and immunohistochemistry were detected using the ApopTag in situ oligo ligation
(ISOL) kit, using oligo B, according to the manufacturer’s
Specimens were collected from the biceps femoris instructions (Intergen). Numerous fibers with brown
muscle and peroneal nerve by an open biopsy procedure staining TUNEL-positive nuclei (arrow) were present in
under general inhalation anesthesia. Muscle biopsies were the myopathic muscle (Fig. 2K), while none were detected
flash frozen in isopentane pre-cooled in liquid nitrogen or in the normal dog muscle (Fig. 2L).
immersed in 10% buffered formalin. Cryostat sections
(8 mm) were processed by standard histological and 2.3. Electron microscopy
histochemical methods. There was an abnormal variability
in myofiber size with atrophic fibers occurring singularly Formalin-fixed muscle and nerve specimens were
and in small groups (Fig. 1A and C). A few of the atrophic washed in 0.1 M phosphate buffer, immersed in 2.5%
fibers arose by fiber splitting. Some fibers contained glutaraldehyde, and post-fixed in 1% aqueous osmium
irregularly shaped hyaline structures and amorphous tetroxide prior to dehydration and embedding in araldite
material (Fig. 1B). Trichrome-stained sections showed resin. Thick sections (1 mm) were stained with toluidine
multiple small blue or blue-red particles in some myofibers blue-basic fuchsin prior to light microscopic examinations,
(Fig. 1D). The succinic dehydrogenase reaction showed while thin sections (60 –90 nm) were stained with uranyl
areas of reduced oxidative activity in several muscle fibers acetate and lead citrate prior to examination in a Zeiss 10
(result not shown). electron microscope. Foci of myofibrillar disruption were
Desmin, alpha-actinin, and dystrophin distributions were evident (Fig. 3A and B) with replacement of myofibrils by a
analyzed by an indirect immunoperoxidase method. Incu- matrix composed of fragments of thick and thin filaments,
bation with primary monoclonal antibodies (desmin 1:100, remnants of Z disks, vacuoles containing cytoplasmic
Sigma clone DE-U-10; alpha-actinin 1:50, NCL-alpha- degradation products, spheroid-like structures, and scattered
ACT, Novocastra; and dystrophin rod domain 1:50 DYS1, glycogen granules. Accumulations of Z-disk material were
Novocastra) was followed by incubation with a biotinylated evident as small dense structures (Fig. 3C) and larger dense
second antibody and a peroxidase-strepavidin reagent bodies (Fig. 3D). Filaments within the dense bodies had a
(Vectastain ABC kit, Vector Laboratories, Burlingame, diameter of 14 –15 nm. No abnormalities were identified
CA). Abnormal staining for desmin (Fig. 1E and F) and within the peripheral nerve biopsy.
alpha-actinin (Fig. 1G) was found in regions of amorphous
or granular deposits. In addition to the normal sarcolemmal
staining pattern, diffuse localization of dystrophin (Fig. 1H) 3. Discussion
was identified in several fibers.
BAG3, a co-chaperone of Hsp 70 [4 –6], and active To our knowledge, this is the first report of myofibrillar
caspase were localized by immunofluorescence. Muscle myopathy occurring in the dog. The clinical presentation of
sections were incubated with affinity-purified polyclonal slowly progressive muscle weakness and atrophy is similar
antibodies against recombinant human BAG3 (1:50) or to that described in a group of 10 human patients with
CM1 (1:100, BD PharMingen, anti-active caspase-3 and 7 myofibrillar myopathy [2]. As in this dog, weakness
polyclonal antibody) followed by incubations with green- involved the limb and truncal muscles with sparing of
fluorescent Alexa Fluor 488 goat anti-rabbit IgG (1:200; muscles innervated by cranial nerves. Following the
Molecular Probes Inc). For double staining, sections were diagnosis in this dog, an echocardiogram was performed
incubated with a desmin monoclonal antibody (1:100; documenting a reduced shortening fraction consistent with
Sigma clone DE-U-10) followed by incubation with red- cardiac involvement.
fluorescent Alexa Fluor 594 chicken anti-mouse IgG Patterns of pathological alterations at both light and
(1:200; Molecular Probes Inc). The specimens were electron microscopic levels support this diagnosis. Similar to
imaged by confocal microscopy (Bio-Rad MRC 1024 human patients, the main abnormalities included myofibril-
microscope). Areas of abnormal positivity for BAG3 lar destruction (Fig. 3A) and accumulation of the products of
(Fig. 2A), CM1 (Fig. 2D), and desmin (Fig. 2B and E) myofibrillar degradation (Fig. 3B). There were foci of
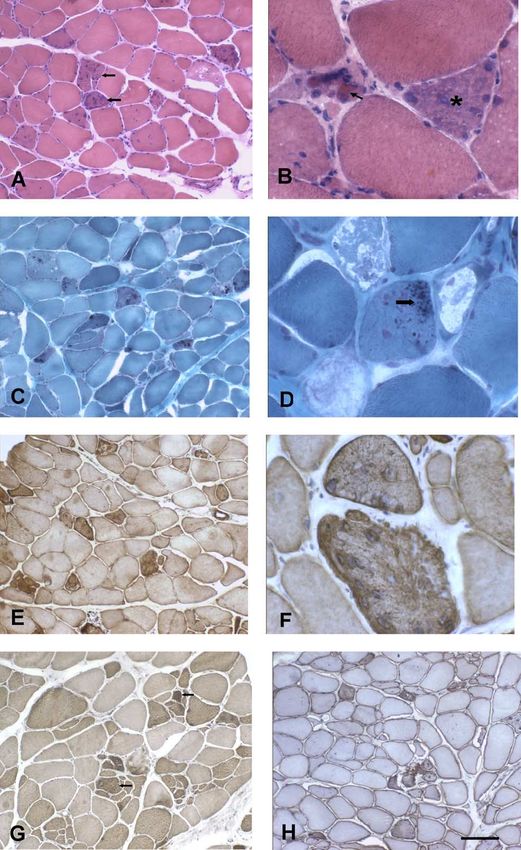
partially co-localized in several abnormal appearing disrupted myofibrillar architecture containing filamentousG.D. Shelton et al. / Neuromuscular Disorders 14 (2004) 399–404 401 Fig. 1. Cryostat sections from a dog with myofibrillar myopathy were evaluated histologically, histochemically, and for desmin, alpha-actinin and dystrophin immunostaining. (A) Low-power H and E stain showed variability in myofiber size and sarcoplasmic inclusions (arrows) in several muscle fibers. (B) Irregularly shaped hyaline inclusions (arrow) and amorphous material (asterisk) are evident at higher power with H and E staining. (C) Low-power modified Gomori trichrome stain shows multiple small blue or blue-red particles in several fibers. (D) Small particles (arrow) and patchy loss of staining in some fibers are highlighted with the trichrome stain at higher power. (E) Abnormal desmin positivity was found in regions of amorphous or granular deposits. (F) Irregular areas of desmin positivity are more evident at high power. (G) Staining for alpha-actinin showing abnormal accumulations in some muscle fibers (arrows). (H) Abnormal diffuse dystrophin positivity was identified in several fibers in addition to the normal sarcolemmal pattern. (Original magnification £ 100 for (A), (C), (E), (G), and (H) and £ 400 for (B), (D), and (F). Bar, 100 mm for (A), (C), (E), (G), and (H) and 25 mm for (B), (D), and (F).)
402 G.D. Shelton et al. / Neuromuscular Disorders 14 (2004) 399–404 Fig. 2. Frozen sections from the biceps femoris muscle of a dog with myofibrillar myopathy (A –F) and a normal dog (G– J) were labeled for BAG3 (A, G), CM1 (D), and desmin (B, E, H). Doubling labeling is shown for BAG3/desmin (C, I) and CM1/desmin (F, J). In the dog with myofibrillar myopathy, areas of BAG3 (A) and desmin (B) staining were patchy in some fibers and absent in others. Stainings co-localized in some of the fibers (C; yellow staining). In the dog with myofibrillar myopathy, several fibers stained positively for both activated caspases (D) and desmin (E), although co-localization (F) was not as apparent as for BAG3/desmin. In normal dog muscle, BAG3 staining (G) was speckled throughout the muscle fibers and desmin staining (H) was more prominent in some fibers than others. Double staining (I) showed co-localization of BAG3 and desmin in a similar speckled pattern. As expected, staining for activated caspases was not found within normal dog muscle fibers (J), which shows desmin staining (red) but not CM1 (green) staining. TUNEL staining was performed on muscle from the dog with myofibrillar myopathy (K) and the control dog (L). Brown-staining TUNEL positive nuclei (arrow) were present in the myopathic muscle but not observed in nuclei from normal dog muscle (L). In these micrographs, normal nuclei are stained green. (Original magnification £ 200 for (A)– (J) and (L), and £ 400 for (K); Bar, 50 mm for (A)–(J) and (L), and 25 mm for (K).) material and dense accumulations of Z-disk material Abnormal accumulation of material immunoreactive (Figs. 2G and 3C) or Z-bodies (Fig. 3D). In human patients, for desmin is a common feature of this myopathy, it was noted that each destructive alteration was associated although there is also accumulation of several other with an anomaly of the Z disk, suggesting an important role proteins [2,3]. Abnormal accumulations of alpha-actinin for this organelle in myofibrillar myopathy [2]. (Fig. 1G) and dystrophin (Fig. 1H) were also found in this
G.D. Shelton et al. / Neuromuscular Disorders 14 (2004) 399–404 403 Fig. 3. Myofibrillar destruction and accumulation of degradation products were evident by electron microscopy. (A) A focus of disrupted myofibrils containing filamentous material, small and large dense structures, and membranous debris is evident in a myofiber adjacent to a normal appearing fiber at the upper right. (B) Numerous vacuoles containing cytoplasmic degradation products surround a large dense structure, possibly a nucleus, surrounded by autophagic vacuolar material. A putative spheroid body (asterisk and see insert) is also present. (C) In the myofibers, multiple small dense structures are in the vicinity of Z-disks. (D) Large dense structures subjacent to the sarcolemma are shown with remnants of disrupted sarcomeres. (Original magnifications 11,600 for (A), 15,500 for (B), 12,200 for (C), and 30,500 for (D); Bar, 0.87 mm for (A), 0.65 mm for (B), 0.83 mm for (C), and 0.33 mm for (D).) dog. The abnormal alpha-actinin localization confirm the present. Further, staining for the activated caspases 3 or 7 presence of Z-disk material. Since it was recently provides evidence for activity in the apoptotic pathway. demonstrated that BAG3 partially co-localizes with TUNEL staining, which detects fragmented DNA in the desmin at the Z-disk of skeletal muscle and in nuclei of cells [7], confirmed apoptosis. As an anti- differentiated C2C12 cells (Takayama, unpublished obser- apoptotic role for BAG3 has been postulated, abnormal- vation), immunostaining for BAG3 localization was ities of BAG3 may play a key role in initiation of performed. As shown in Fig. 2C, there was partial co- myofibrillar myopathies. Further investigations into the localization of staining in abnormal fibers. Some fibers role of BAG3 in spontaneous animal models such as the appeared unstained suggesting that BAG3 was no longer dog or in the recently engineered BAG3 KO mouse
404 G.D. Shelton et al. / Neuromuscular Disorders 14 (2004) 399–404
(Takayama, unpublished) may provide new investigations and electron microscopy of 10 cases. J Neuropath Exp Neurol 1996;55:
into what initiates the degradation in this myofibrillar 549– 62.
[2] De Bleecker JL, Engel AG, Ertl BB. Myofibrillar myopathy with
myopathy. abnormal foci of desmin positivity. II. Immunocytochemical analysis
reveals accumulation of multiple other proteins. J Neuropath Exp
Neurol 1996;55:563–77.
Acknowledgements [3] Shelton GD, Engvall E. Muscular dystrophies and other inherited
myopathies. Vet Clin North Am: Small Anim Pract 2002;32:
103– 24.
The authors would like to thank Norma Prades for [4] Takayama S, Xie Z, Reed J. An evolutionarily conserved family of
excellent technical assistance and Dr Eva Engvall for Hsp70/Hsc70 molecular chaperone regulators. J Biol Chem 1999;274:
helpful suggestions. This work was partially supported by a 781– 6.
grant from the Muscular Dystrophy Association. [5] Takayama S, Reed JC. Molecular chaperone targeting and regulation
by BAG family proteins. Nat Cell Biol 2001;3:E237– 41.
[6] Takayama S, Reed JC, Homma S. Heat shock proteins as regulators of
apoptosis. Oncogene 2003;22:9041–7.
References [7] Thomas LB, Gates DJ, Richfield EK, O’Brien TF, Schweitzer JB,
Steindler DA. DNA end labeling (TUNEL) in Huntington’s disease
[1] Nakano S, Engel AG, Waclawik AJ, Emslie-Smith AM, Busis NA. and other neuropathological conditions. Exp Neurol 1995;133:
Myofibrillar myopathy with abnormal foci of desmin positivity. 1. Light 265– 72.You can also read

















































