Osteopathia Striata With Cranial Sclerosis: Clinical, Radiological, and Bone Histological Findings in an Adolescent Girl
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
American Journal of Medical Genetics 129A:8 – 12 (2004)
Osteopathia Striata With Cranial Sclerosis:
Clinical, Radiological, and Bone Histological Findings
in an Adolescent Girl
L.M. Ward,1,2* F. Rauch,2 R. Travers,2 M. Roy,3 J. Montes,4 G. Chabot,2,3 and F.H. Glorieux2,4
1
Department of Pediatrics, Children’s Hospital of Eastern Ontario, University of Ottawa, Ottawa, Canada
2
Genetics Unit, Shriners Hospital, McGill University, Montréal, Québec, Canada
3
Département de Pédiatrie, Hôpital Ste. Justine, Université de Montréal, Québec, Canada
4
Departments of Surgery and Pediatrics, McGill University, Montréal, Québec, Canada
Osteopathia striata with cranial sclerosis (OS– INTRODUCTION
CS) is a rare skeletal dysplasia characterized by
Osteopathia striata with cranial sclerosis (OS–CS; MIM#
linear striations of the long bones, osteosclerosis
166500) is a rare skeletal dysplasia characterized by long-
of the cranium, and extra-skeletal anomalies. We
itudinal striations of the long bone diametaphyses and
provide a comprehensive description of the ske-
sclerosis of the cranial vault and base. Striated metaphyses
letal phenotype in a French-Canadian girl with a
were first described by the Dutch radiologist Voorhoeve [1924],
moderate to severe form of sporadic OS–CS.
and their association with cranial sclerosis was subsequently
Multiple medical problems, including anal steno-
reported by Hurt [1953]. OS–CS can occur in isolation, or may
sis and the Pierre–Robin sequence, were evident
be part of a syndrome together with heart defects, malrotation
in the first few years of life. At 14 years, she was
of the abdominal organs, omphalocele, partial agenesis of the
fully mobile, with normal intellect and stature.
corpus callosum, and the Pierre–Robin sequence [Winter et al.,
She suffered chronic lower extremity pain in the
1980; Pellegrino et al., 1997]. Over 100 cases of OS–CS have
absence of fractures, as well as severe headaches,
been described to date [Savarirayan et al., 1997; Bueno et al.,
unilateral facial paralysis, and bilateral mixed
1998; Lazar et al., 1999; Behninger and Rott, 2000; Viot et al.,
hearing loss. Biochemical indices of bone and
2002]. About one third of cases are sporadic, while the
mineral metabolism were within normal limits.
remainder show familial clustering. Reports of familial OS–
Bone densitometry showed increased areal bone
CS clearly point to dominant heritability [Horan and Beighton,
mineral density in the skull, trunk, and pelvis, but
1978], but whether the trait is transmitted in an autosomal or
not in the upper and lower extremities. An iliac
X-linked dominant fashion remains unsettled [Behninger and
bone biopsy specimen revealed an increased
Rott, 2000; Viot et al., 2002].
amount of trabecular bone. Trabeculae were
The linear striations of the long bones typically first appear
abnormally thick, but there was no evidence of
between 5 months and 6 years of age [Viot et al., 2002] and
disturbed bone remodeling. In a cranial bone
usually are of little clinical significance. However, the cranial
specimen, multiple layers of periosteal bone were
sclerosis is frequently disabling, as it may lead to hearing loss
found that covered a compact cortical compart-
and nerve palsies [Behninger and Rott, 2000], and macro-
ment containing tightly packed haversian canals.
cephaly is often present [Viot et al., 2002]. The histological
Bone lamellation was normal in both the iliac and
basis of the long bone striations and the skull sclerosis is not
skull samples. Osteoclast differentiation studies
entirely clear. Increased trabecular thickness was described in
showed that peripheral blood osteoclast precur-
the femur of a newborn, as well as in the ilium and rib of two
sors from this patient formed functional osteo-
middle-aged men [Hurt, 1953; Winter et al., 1980; Nakamura
clasts in vitro. Thus, studies of bone metabolism
et al., 1998]. The normal lamellar pattern of mature bone was
did not explain why bone mass is increased in
reported to be absent in one case [Nakamura et al., 1998]. In the
most skeletal areas of this patient. Cranial histol-
present report, we provide a detailed analysis of the skeletal
ogy points to exuberant periosteal bone formation
phenotype in an adolescent girl with moderately severe,
as a potential cause of the cranial sclerosis.
sporadic OS–CS.
ß 2004 Wiley-Liss, Inc.
KEY WORDS: osteopathia striata; cranial sclero-
sis; osteosclerosis; histology MATERIALS AND METHODS
Serum and urine biochemistry was performed using meth-
odology described previously [Ward et al., 2002]. Total body
bone densitometry in the antero-posterior direction was per-
formed using a Hologic 4500A device (Hologic, Inc., Waltham,
MA). Areal bone mineral density (aBMD) results were
transformed to age-specific z-scores using published reference
data [Bailey et al., 1996].
Grant sponsor: Shriners of North America. An iliac bone biopsy was obtained after tetracycline labeling
*Correspondence to: L.M. Ward, M.D., Department of and was processed as previously described [Glorieux et al.,
Pediatrics, University of Ottawa, Children’s Hospital of Eastern 2000]. Quantitative histomorphometric results were compared
Ont., 401 Smyth Road, Ottawa, Ontario, Canada K1H 8L1. with previously published reference material [Glorieux et al.,
E-mail: ward_l@cheo.on.ca 2000]. A full-thickness trans-parietal bone biopsy sample was
Received 18 September 2003; Accepted 16 December 2003 taken at the time of intracranial pressure monitoring. This
DOI 10.1002/ajmg.a.30107 specimen was compared to that of an 8-year-old boy undergoing
ß 2004 Wiley-Liss, Inc.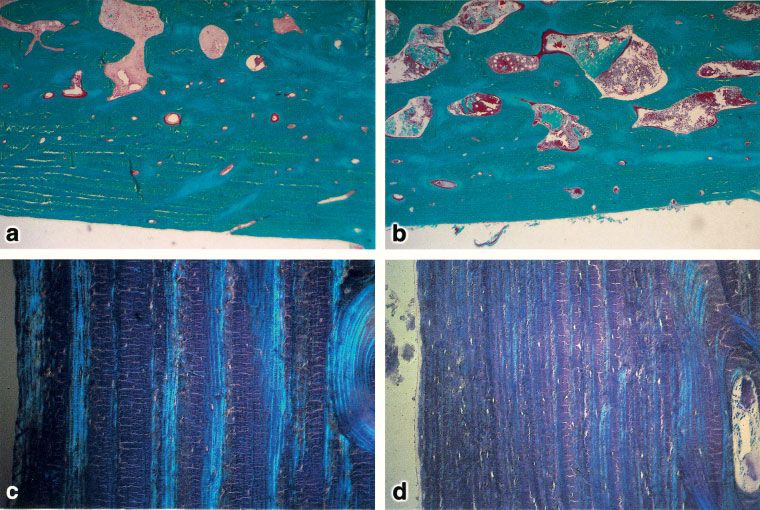
Bone Histology in Osteopathia Striata 9
Fig. 1. a: Anterior–posterior view of the lower extremities showing striated diametaphyses in the patient (13.8 years) with osteopathia striata with
cranial sclerosis (OS–CS). b: Lateral view of the cranium showing severe sclerosis in the 14.8 year old girl with OS–CS.
brain surgery for astrocytoma, who had no evidence of a
skeletal disorder.
Functional osteoclast studies were performed following
isolation of peripheral blood mononuclear cells as previously
described [Shalhoub et al., 2000]. Patient and control cells were
plated on bone slices in triplicate. Cultures were fed every
other day with colony-stimulating factor-1 (30 ng/ml) plus
osteoprotegerin ligand (100 ng/ml), or colony-stimulating
factor-1 (30 ng/ml) alone, for 24 days. The ability of monocyte
precursors in this conditioned media to form tartrate-resistant
acid phosphatase (TRAP) positive multi-nucleated osteoclasts
that produced resorption lacunae in bone was evaluated.
CLINICAL REPORT
The proposita is of French-Canadian descent, the youngest
of three daughters born to healthy, non-consanguineous
parents. The extended family history was negative for skeletal
disorders, miscarriages, or neonatal deaths. Delivery was
spontaneous at 43 weeks’ gestation, following an uneventful
pregnancy. Birth weight was 4.8 kg, length 55 cm, and occipital
frontal circumference 40 cm, all of which were significantly
greater than the 95th centile. Abnormalities noted shortly
after birth included the Pierre–Robin sequence (hypoplastic
mandible and midline cleft palate), laryngotracheomalacia,
and anal stenosis. The clinical course in the first year of life was
complicated by laryngotracheal stenosis and gastroesophageal
reflux with a hiatal hernia, necessitating surgical interven-
tion. Hearing aids were prescribed at 4 (right) and 6 (left) years
of age for bilateral, mixed hearing loss that was predominantly
conductive. A skeletal survey obtained at the age of 4 years
showed linear striations in the metaphyseal and diaphyseal
areas of long bones (Fig. 1a) as well as sclerosis of the cranial
base (Fig. 1b). These findings led to the diagnosis of OS–CS. In
retrospect, striations of the proximal humeri had already been
visible on chest X-rays that had been taken at 7 months of age.
The striations had not been clearly visible at 2 and 4 months of
age, however (Fig. 2). At 12 years of age, complete left facial
paralysis occurred, but improved following treatment with a
Fig. 2. a–d: Radiographs performed to assess the patient’s respiratory
non-steroidal anti-inflammatory agent. The patient com- status at various intervals, showing absence of visible abnormality of the
plained of chronic lower extremity pain, especially of the hips humerus at 2 months (a). At 4 months (b), minimal, non-specific sclerosis is
and the knees, but had never sustained any fractures. evident. Definite linear striations are seen at 7 months (c) and 3.6 years (d).10 Ward et al.
At her most recent clinical evaluation (age 14.5 years), the TABLE I. Anthropometry and Bone Densitometry Results
patient was fully mobile with normal intellectual development.
The height and weight are presented in Table I. The head Parameter Result Z score
circumference was 62.5 cm (5 cm above the 98th centile). There Height (cm) 147.7 2.65
was turricephaly with bifrontal bossing. The ears were small Weight (kg) 40.6 1.26
and low-set. Bilateral pre-auricular sinuses were present. aBMD (g/cm2)
Mild, left-sided facial paralysis was still evident. The palate Total body 1.249 3.99
was high-arched with significant dental crowding. The Head 2.930 7.65
laryngotracheomalacia of childhood had resolved, and pub- Upper limbs 0.690 0.49
ertal development was normal (Tanner stage 3). Her most Trunk 0.741 1.35
significant complaint was headaches, which were only par- Pelvis 1.283 1.53
tially responsive to anti-inflammatory medication. Because of Lower limbs 1.008 0.28
the persistent headaches, the patient underwent intracranial
aBMD, areal bone mineral density.
pressure monitoring, which showed no abnormality. At 14.5
years of age, a series of investigations were undertaken in
order to fully characterize her skeletal phenotype and to striations were evident in the ilial wings. Mild curvatures of
investigate her chronic limb pain and headaches. the thoracic (dextroconvex 118) and lumbar (levoconvex 158)
spine were present. There was marked craniofacial sclerosis,
particularly at the skull base (Fig. 1b), which was evident at
RESULTS
seven weeks of age. Cerebral computed tomography showed no
A biochemical evaluation of bone and mineral metabolism evidence of cranial nerve entrapment despite the marked
including serum levels of total calcium, inorganic phosphate, cranial sclerosis.
alkaline phosphatase, tartrate-resistant acid phosphatase Bone densitometry demonstrated an elevated aBMD of the
(TRAP), osteocalcin, parathyroid hormone, 1,25-dihydroxy- total body (Table I). However, aBMD varied considerably
vitamin D and 25-hydroxyvitamin D levels as well as urinary between skeletal regions. There was marked elevation of skull
excretion of calcium, cyclic adenosine-monophosphate and N- aBMD. Results for the trunk and pelvis were also elevated
terminal telopeptide of collagen type I did not reveal any considering the short stature of the patient, while upper and
abnormality. lower limb aBMD appeared to be adequate (Table I).
Longitudinal striations were visible in the metaphyseal and Qualitative evaluation of the iliac bone biopsy specimen
diaphyseal regions of long bones (Fig. 1a) and fan-like revealed increased trabecular thickness (Fig. 3a,b) and a
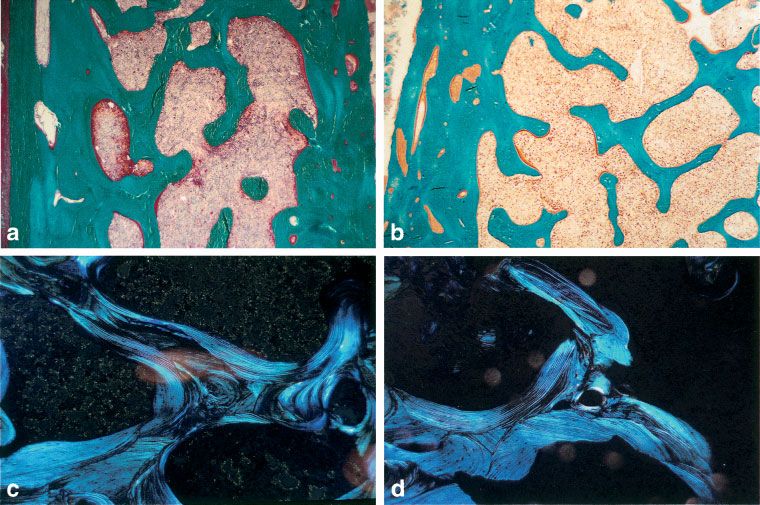
Fig. 3. a, b: Qualitative histomorphometry at the iliac crest showing increased trabecular thickness in the patient (a) compared to an age-matched
control (b). c, d: Iliac crest specimen showing a preserved pattern of lamellation under birefringent light in the proposita (c), similar to the age-matched
control (d).Bone Histology in Osteopathia Striata 11
TABLE II. Iliac Bone Histomorphometry
Parameter Patient Reference rangesa
Structural parameters
Cortical width (mm) 1,002 897 331
Bone volume/tissue volume (%) 40.0 24.4 4.3
Trabecular thickness (mm) 225 148 23
Trabecular Number (/mm) 1.8 1.7 0.2
Formation parameters
Osteoid thickness (mm) 7.2 6.7 1.8
Osteoid surface/bone surface (%) 12.9 22.1 7.8
Mineralizing surface/bone surface (%) 15.8 11.7 5.0
Mineral apposition rate (mm/day) 0.81 0.87 0.09
Bone formation rate/bone surface (mm3/mm2/year) 46.9 37.3 16.7
Resorption parameters
Eroded surface/bone surface (%) 22.3 14.9 5.6
Osteoclast surface/bone surface (%) 1.29 0.94 0.38
a
Values are means and SD, according to normative data by Glorieux et al. [2000].
normal pattern of birefringence under polarized light compartment with tightly packed haversian canals. The
(Fig. 3c,d). Tetracycline labels were distinctly visible (not periosteal bone layers were much more evident in the proposita
shown). Quantitative histomorphometry (Table II) showed than in a control sample (Fig. 4c,d). There was no evidence of
normal cortical width. However, trabecular bone volume was woven bone in the skull bone sample.
markedly elevated, due to increased trabecular thickness. Given the osteosclerosis in this patient, we evaluated
Histomorphometric parameters of bone formation and resorp- osteoclast differentiation and function in vitro. Patient and
tion were within normal limits. control peripheral blood mononuclear cells were similarly able
Qualitative evaluation of the cranial biopsy (Fig. 4a,b) to form TRAP-positive multi-nucleated osteoclasts that pro-
showed layers of periosteal bone covering a compact cortical duced resorption lacunae over the bone surface.
Fig. 4. a, b: Cranial specimen showing compact cortical bone in the proposita with tightly packed Haversian canals (a) compared to an 8-year-old boy with
a normal metabolic bone status (b). c, d: Cranial specimen showing successive layering of periosteal apposition (c) that is more evident compared to the control
specimen (d).12 Ward et al.
DISCUSSION and figures, Guy Charette for processing of the bone histology
specimens, and Josée Depot for the biochemical studies and
The girl described here had typical features of OS–CS
histomorphometric analyses.
associated with multiple developmental anomalies. Most
features of her disease have been previously associated with
this skeletal dysplasia [Winter et al., 1980; Konig et al., 1996].
However, the anal stenosis found in our patient appears to be REFERENCES
rarely associated with OS–CS, as only one similar case has Bailey DA, Faulkner RA, McKay HA. 1996. Growth, physical activity, and
been published [Savarirayan et al., 1997]. Also, unusual bone mineral acquisition. Exerc Sport Sci Rev 24:233–266.
macrosomia was noted in our patient at birth, which did not Behninger C, Rott HD. 2000. Osteopathia striata with cranial sclerosis:
persist post-natally. A similar growth pattern has been Literature reappraisal argues for X-linked inheritance. Genet Couns 11:
previously described in a girl with sporadic OS–CS [Kondoh 157–167.
et al., 2001]. Our patient’s most troubling clinical feature was Bueno AL, Ramos FJ, Bueno O, Olivares JL, Bello ML, Bueno M. 1998.
cranial stenosis, which has led to unilateral facial nerve Severe malformations in males from families with osteopathia striata
paralysis and headaches. Medical imaging and intracranial with cranial sclerosis. Clin Genet 54:400–405.
monitoring have ruled out cranial nerve entrapment and Glorieux FH, Travers R, Taylor A, Bowen JR, Rauch F, Norman M,
hydrocephalus as causative factors. It is possible, however, Parfitt AM. 2000. Normative data for iliac bone histomorphometry in
growing children. Bone 26:103–109.
that vascular entrapment is at play.
As to the skeletal phenotype, bone densitometry confirmed Horan FT, Beighton PH. 1978. Osteopathia striata with cranial sclerosis. An
autosomal dominant entity. Clin Genet 13:201–206.
the presence of marked cranial osteosclerosis in our patient.
Elevated bone density was also found in the pelvis and trunk, Hurt RL. 1953. Osteopathia striata-Voorhoeve’s disease: Report of a case
presenting the features of osteopathia striata and osteopetrosis. J Bone
but not in the upper and lower extremities. As such, there was Joint Surg Am 35B:89–96.
evidence of variability in the bone density distribution.
Kondoh T, Yoshinaga M, Matsumoto T, Takayanagi T, Uetani M,
Organization of the bone matrix appeared to be normal, since Kubota T, Nishimura G, Moriuchi H. 2001. Severe cervical kyphosis in
the normal lamellar pattern was preserved in both iliac and osteopathia striata with cranial sclerosis: Case report. Pediatr Radiol
cranial bone. Thus, in contrast to the report of Nakamura et al. 31:659–662.
[1998], there was no evidence of woven bone. The cranial Konig R, Dukiet C, Dorries A, Zabel B, Fuchs S. 1996. Osteopathia striata
specimen, however, showed a large number of periosteal bone with cranial sclerosis: Variable expressivity in a four generation
layers that covered a compact cortical compartment, suggest- pedigree. Am J Med Genet 63:68–73.
ing that the marked cranial sclerosis may have resulted from Lazar CM, Braunstein EM, Econs MJ. 1999. Clinical vignette: Osteopathia
the periosteal apposition of successive bone layers. striata with cranial sclerosis. J Bone Miner Res 14:152–153.
Quantitative analyses of the iliac sample revealed an Nakamura K, Nakada Y, Nakada D. 1998. Unclassified sclerosing bone
increased amount of trabecular bone, which is in accordance dysplasia with osteopathia striata, cranial sclerosis, metaphyseal
with the elevated bone density reading and confirms previous undermodeling, and bone fragility. Am J Med Genet 76:389–394.
histological reports [Hurt, 1953; Winter et al., 1980; Nakamura Parfitt AM, Travers R, Rauch F, Glorieux FH. 2000. Structural and cellular
et al., 1998]. Nevertheless, histomorphometric indicators of changes during bone growth in healthy children. Bone 27:487–494.
bone metabolism were within normal limits. Biochemical Pellegrino JE, McDonald-McGinn DM, Schneider A, Markowitz RI,
studies also revealed a normal profile for parameters of bone Zackai EH. 1997. Further clinical delineation and increased morbidity
in males with osteopathia striata with cranial sclerosis: An X-linked
and mineral metabolism, similar to previous reports [Whyte disorder? Am J Med Genet 70:159–165.
et al., 1978]. Finally, our osteoclast differentiation studies
Savarirayan R, Nance J, Morris L, Haan E, Couper R. 1997. Osteopathia
showed that peripheral blood osteoclast precursors of this striata with cranial sclerosis: Highly variable phenotypic expression
patient formed functional osteoclasts in vitro. Thus, neither within a family. Clin Genet 52:199–205.
clinical nor in vitro studies of bone metabolism provide a clue as Shalhoub V, Elliott G, Chiu L, Manoukian R, Kelley M, Hawkins N, Davy E,
to why bone mass is increased in most skeletal areas of our Shimamoto G, Beck J, Kaufman SA, Van G, Scully S, Qi M, Gristanti M,
patient. However, it must be acknowledged that small changes Dunstan C, Boyle WJ, Lacey DL. 2000. Characterization of osteoclast
in bone remodeling balance can lead to large changes in bone precursors in human blood. Br J Haematol 111:501–512.
mass [Parfitt et al., 2000]. Subtle alterations in bone metabo- Viot GDL, David A, Mathieu M, de Broca A, Faivre L, Gigarel N, Munnich A,
lism may not have been detectable with the methods used. Lyonnet S, Le Merrer M, Cormier-Daire V. 2002. Osteopathia striata
This adolescent girl with sporadic OS–CS had generalized cranial sclerosis: Non-random X-inactivation suggestive of X-linked
dominant inheritance. Am J Med Genet 107:1–4.
osteosclerosis with relative sparing of the limbs. Biochemical,
histomorphometric, and in vitro osteoclast assays did not Voorhoeve N. 1924. L’image radiologique non encore decrite d’une anomalie
du squelette: Ses rapports avec la dyschondroplasie et l’osteopathia
reveal any abnormality that could explain the osteosclerosis.
condensans disseminata. Acta Radiol 3:407–427.
Cranial histology points to exuberant periosteal bone forma-
Ward LM, Rauch F, Travers R, Chabot G, Azouz EM, Lalic L, Roughley PJ,
tion as a potential cause of the cranial sclerosis.
Glorieux FH. 2002. Osteogenesis imperfecta type VII: An autosomal
recessive form of brittle bone disease. Bone 31:12–18.
ACKNOWLEDGMENTS Whyte MP, Murphy WA, Siegel BA. 1978. 99mTc-pyrophosphate bone
imaging in osteopoikilosis, osteopathia striata, and melorheostosis.
We thank Victoria Shalhoub (Amgen, California, USA) for Radiology 127:439–443.
performing the in vitro osteoclast studies, and the following Winter RM, D’A CM, Meire HB, Mitchell N. 1980. Osteopathia striata with
individuals at the Shriners Hospital for Children, Montréal, cranial sclerosis: Highly variable expression within a family including
Québec, Canada: Mark Lepik and Guylain Bedard for artwork cleft palate in two neonatal cases. Clin Genet 18:462–474.You can also read

















































