PEPFAR Civil Society Update - AMB Deborah L. Birx, MD November 26, 2018 - Global Faith Initiative
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

PEPFAR Civil Society Update
AMB Deborah L. Birx, MD
November 26, 2018
The PEPFAR Program: a unique approach to foreign assistance
Critical objectives for 2019 and 2020
• Determine what things cost not what we are spending for MoF negotiations
• ABC costing initiative in Kenya and Tanzania
• FBO and NGO funding and differential model of investment
• Movement to indigenous partners (parastatal or private sector)
• Realignment of HQ and “concentrated epidemics” resources for maximal
impact
• Critical review of all elements of program at the site level. What are we
buying and what impact is it having and how long we need to buy each
specific item.
• Positioning for long-term success at the site, district, National level
• Scaling index and self-testing.
• Filling the testing and treatment gaps quarter after quarter
• Comprehensive re-evaluation of West and West-Central investments
unless policy change occurs
• Ensuring all ages and risk groups have the same equitable access to
prevention and treatment services
2
PEPFAR’s Evolution
PEPFAR I (2001-2009) PEPFAR II (2009-2014) PEPFAR III (2014-present)
• Emergency response • Shared responsibility & • Data, quality, oversight,
• AIDS- a security issue country-driven programs transparency &
• Rapid delivering • Ensuring an AIDS Free accountability for impact
prevention, care, and generation • Accelerating core
treatment services • Building & strengthening interventions for epidemic
• Focus on individuals health systems to deliver control
with late stage AIDS HIV services • Ensure treatment of all
defining illness • Scaling up of prevention, HIV positive individuals
care, and treatment for their own health and
services for people stop transmissions
without AIDS defining • Sustainability agenda
illness based on data, actual
costs and indigenous
partners
3
Main Messages
• Epidemic control is possible and achievable
• We know more than ever about programmatic
performance and what we need to improve
• Epidemic control is essential for long-term national
fiscal health –infections are increasing in the youth
– women 15-24 and men 25-35 which will have the
longest investment tail
• The demographics of SSA show this is the most
rapidly expanding age group
• Highest risk + largest age cohort = social and
health risk and future instability
4
Political Will Matters
POLICIES Matter
Data matters as it allows us to
see past perceptions and assumptions to
see who we need to reach and creates
the space for an equity based response
rather than an “equal response”
5
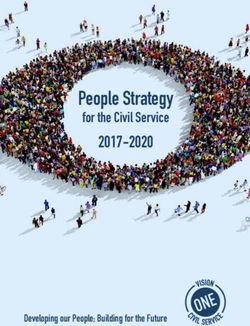
Political Will matters: countries must address the epidemic they have versus want they want to have
New Infections in Russia vs Ukraine 2000-2017
140,000
120,000
Russia
Number of new HIV infections
100,000
80,000
60,000
40,000
20,000
0
40,000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
35,000
Number of new HIV infections
30,000 Ukraine
25,000
20,000
15,000
10,000
5,000
0
7
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Data matters as it allows us to see past perceptions and assumptions to see who we need to reach and creates the space for an equity based response rather than an “equal response
Using granular data We have identified the key gaps in the program execution and together we are tailoring our response to the gaps : testing of well children and young adults as gateway to prevention and treatment services and focused site level program improvements 9
Community Viral Load Suppression By Age
and Gender
*Pooled data from Lesotho, Malawi, Namibia, Swaziland, Tanzania, Uganda, Zambia, and Zimbabwe
from PHIA projects.Sites targeted for intervention to improve viral suppression
Challenges in viral suppression among children
% of Adult ART Patients per Country on ARV Regimens, at
the end of the COP18 TLD Transition (pre June, 2018
WHO/PEPFAR Revised Guidance)
% on TLD % on TLE or TEE % on LNZ % on All other Regimens
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
#PEPFAR15
13% of Adult ARV Patients per Country on ARV Regimen at the
end of the COP 18 TLD Transition (per revised TLD Supply
Plans, submitted in June/July 2018 – Post DTG Safety Notice)
% on TLD % on TLE or TEE % on LNZ % on All other Regimens
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
#PEPFAR15
14% of Adult ART Patients per Country on ARV Regimens,
as of August, 2018
% on TLE or TEE % on TLD % on LNZ % on All other Regimens
100.00%
90.00%
80.00%
70.00%
60.00%
50.00%
40.00%
30.00%
20.00%
10.00%
0.00%
#PEPFAR15
15Conclusions from Modeling of TLD Transition
Phillips
Using a standard DALY (disability-adjusted life-years) framework for comparing health
outcomes from a public health perspective the benefits of transition to TLD for all substantially
outweigh any risks.
Potential to avert 150,000 AIDS deaths/year among 15 million on ART.
Dugdale
• Dolutegravir-based ART would avert >30,000 deaths among women of childbearing age and >5,000
pediatric HIV infections compared to efavirenz-based ART, but result in ~6,000 excess pediatric
deaths over a five-year period in South Africa
• A WHO guideline-concordant approach could mitigate adverse pediatric outcomes, but would result
in many more deaths among women than dolutegravir for all
Bern meeting 9/21: No further models expected. Both models robust for strong benefits for
all-DTG approach. These models will be updated with new data but bottom-line results would
only change if new data demonstrate much higher NTD risk (Tsepamo) or smaller benefit of
DTG compared to EFV (NAMSAL*).
*NAMSAL EFV400 vs DTG initial ART in adults (CdI) 48-wk trial results presented in Glasgow, Oct 31, 2018
16Conclusions
• PEPFAR remains committed to broad implementation of DTG-based
regimens as first and second line treatment.
• We continue to work closely with our country teams to advocate for
broader availability of DTG for women and to provide resources for
implementation.
• The community of women living with HIV must be included in decision
making at every level.
• We support integration of women’s health services into HIV care and are
working with countries to increase contraceptive options.
• We are supporting multiple efforts to obtain additional data on BD risk
rapidly and supporting ongoing birth defect surveillance in Uganda and
Malawi.
17Progress is possible with the right
policies and using data to focus the
program
Progress and has been demonstrated
when we are utilizing the best science
and tools, AND the triangulation of
program data, qualitative data and
community surveys has shown us our
successes and failures and provide a
road map to change the course of the
HIV pandemic
18Where are we?
Eastern and Southern Africa High prevalence
generalized
Expansion of services through deliberative
epidemics
collaboration between PEPFAR, GF,
governments, and community
Demonstrated outcomes lead to
impact; rapid policy adoption,
continuous monitoring of progress
GAPS : Prevention interventions to saturation
15-30 age group
Early Treatment - Men – all ages
Clinical and prevention cascade for key
populationsRefocusing the program around core interventions changed the course of the second pandemic wave
Countries where out-year costs to PEPFAR will decline by 2020
Due to lowering new infections to less than all cause mortality
21Countries where out-year costs to PEPFAR will decline by 2020-2021
Due to lowering new infections to less than all cause mortality
22Countries where out-year costs to PEPFAR will decline after 2021 unless
trajectory changes
23Lesson learned from East and
Southern Africa – the progress to
date – nearly a 50% decline in
incidence has occurred with
missing more than 50% of the men
–especially healthy young men – if
this is addressed the epidemic can
be controlled
24Where are we? West/West Central Africa Low prevalence Slow expansion of critical prevention and treatment mixed services despite resources epidemics Unclear epidemiology with mixed epidemics Slow policy adoption, user fees – formal and informal- prevent access to health services; unrelenting stigma and discrimination; Key gaps Clinical and prevention cascade for key populations Inconsistent political will to address all key populations with necessary interventions Ensuring access to services for young people and men of all ages Strategies to address stigma and discrimination
Countries where we are focusing on policy change to have
impact
26Lesson learned from West
and West Central Africa
region:
POLICIES Matter
Progress in policy changes
necessary for success
27Where are we? Key population epidemics – Eastern Concentrated Europe, Central Asia, Asia, Caribbean and epidemics Latin/Central America Poor performance of prevention and treatment cascades - with PWID>>SW>MSM Different issues in the cascades by risk group Pilots without scaling Unrelenting stigma and discrimination Investments have not achieved impact Key gaps Clinical and prevention cascade for key populations Inconsistent political will to address all key populations with necessary prevention interventions Impactful strategies to address stigma and discrimination
New Infections in Russia vs Ukraine 2000-2017
140,000
120,000
Russia
Number of new HIV infections
100,000
80,000
60,000
40,000
20,000
0
40,000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
35,000
Number of new HIV infections
30,000 Ukraine
25,000
20,000
15,000
10,000
5,000
0
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
29Evolving our programs rapidly using the best science and new tools and evaluating why something is not working
KEY GAP : Prevention and treatment Services for
Young Men AND Adolescent Girls & Young Women
DREAMS
Risk avoidance and reduction
Sexual violence prevention, PrEP
Girls and Finding young men and Well HIV +
Young Women ensuring diagnosis and treatment Young Men
25-35 yo
9-24 yo
HIV
Uninfected
Young Men
VMMC
15-30 yo Condoms
PrEPLocal Indigenous
Partners
Build local capacity and reduce cost of services
Achieve 70% local implementation by 2021
32Burden-Sharing
Current cost sharing model different
across all countries
33The PEPFAR Program: a unique approach to foreign assistance and an dual
use platform
Critical objectives for 2019 and 2020
• Determine what things cost not what we are spending for MoF negotiations
• ABC costing initiative in Kenya and Tanzania
• FBO and NGO funding and differential model of investment
• Movement to indigenous partners (parastatal or private sector)
• Realignment of HQ and “concentrated epidemics” resources for maximal
impact
• Critical review of all elements of program at the site level. What are we
buying and what impact is it having and how long we need to buy each
specific item.
• Positioning for long-term success at the site, district, National level
• Scaling index and self-testing.
• Filling the testing and treatment gaps quarter after quarter
• Comprehensive re-evaluation of West and West-Central investments
unless policy change occurs
34COP 19 Priorities
& Process
35COP 19: Regionalization and Country Pairs
Western
Hemi-
sphere
Western Hemisphere Region: Panama,
Guatemala, Nicaragua, Honduras, El
Salvador, Brazil, Jamaica, Trinidad &
West/Cent
Tobago, Guyana, Barbados, Suriname
ral Africa
West/Central Africa Region: Ghana, Mali,
Regions Togo, Burkina Faso, Senegal, Liberia,
and Asia
Sierra Leone
Country
Pairs
Asia Region: Thailand, Laos, Burma,
Cambodia, Kazakhstan, Kyrgyz Republic,
Haiti/DR Tajikistan, India, Indonesia, Nepal, Papua
New Guinea
Namibia/
Angola Country Pairs: Haiti/DR and
Angola/Namibia
36Purpose of Regionalization
1. To consolidate and share technical assistance and expertise across
former STAR OUs, including the integration of programs currently
receiving their funding through the F Operation Plan (F-OPs).
2. Increase efficiency through the consolidation of functions and the numbers
of U.S. Direct Hires across former STAR countries sharing technical
expertise across the region in an integrated manner.
3. Preserve and increase programmatic funding for effective activities and
expand them regionally.
All countries/regions/pairs will follow the same process for COP 19.
37Principles for COP19 Guidance
COP18 guidance is the foundation of COP19 Guidance
COP19 Guidance includes Standard Process Countries,
Regional Programs and Country Pairs
Continue to use similar format for presenting planning
steps and technical considerations
38Content Updates for COP19 Guidance
Stay the course if there is evidence the implementing partners
have aligned with the new policies, no new requirements
Essential updates in planning, programmatic, and
budget/management categories with emphasis on performance
and proactive addressing of gaps
Retaining priority areas of emphasis for COP18 with additional
emphasis on case finding, TB-IPT, and linking expenditures to
program performance
Continued emphasis on increasing engagement and support to
local, indigenous partners, including faith-based organizations
and use of KPIF as bridge to peer programming
39Two New/Revised Sections
402.2 Minimum Program Requirements
Adoption and implementation of Test and Start across all age, sex, and risk
groups.
Adoption and implementation of differentiated service delivery models,
including six month multi-month scripting (MMS) and delivery models to
improve identification and ARV coverage of men and adolescents.
Completion of TLD transition, including women of childbearing potential and
adolescents, and removal of NVP-based regimens.
Scale up of index testing and self-testing, and enhanced pediatric and
adolescent case finding.
TB preventive therapy (TPT) for all PLHIV must be scaled-up as an integral
and routine part of the HIV clinical care package.
412.2 Minimum Program Requirements (continued)
Direct and immediate (>90%) linkage of clients from testing to treatment
across age, sex, and risk groups.
Elimination of all user fees for direct HIV services and related services, such
as ANC and TB services, affecting access to HIV testing and treatment.
Completion of VL/EID optimization activities and ongoing monitoring to ensure
reductions in morbidity and mortality across age, sex, and risk groups.
Monitoring and reporting of morbidity and mortality outcomes.
Alignment of OVC packages of services and enrollment with 9-17 year-old
populations served through clinical HIV services, including integrated case
management.
422.3 Overcoming Barriers to Epidemic Control
Essential Programmatic Elements for Sustainable Epidemic
Control (ECT I)
Good governance and leadership reflected in policy adoption and data
use
Patient-centered integrated care
Locally led implementation of HIV services
Comprehensive HIV surveillance
Public Health Response
Quality
Supply chain and laboratory optimization
Health Information Systems
Human Resources for Health
Domestic resource mobilization and all-market approach
432.3.2 Transitioning HIV Services to Local Partners
Local Partners play an important role in reaching sustained epidemic control
and are essential in both delivery of direct HIV prevention and care services
and non-service delivery technical assistance.
Build local capacity and reduce cost of services
Achieve 70% local implementation by 2021
COP19 emphasizes increased engagement of local partners, including faith-
based organizations, within all PEPFAR programs – Standard Process and
Regional Programs – and clarifies expectations for including and expanding
local partner engagement throughout the COP19 planning and budget
allocation process.
Intent, current agency progress, and definition of LP – Section 2
Methods to increase Engagement in Service Delivery – Sections 2 and 3
Methods to ensure adequate budgeting given increased costs to deliver services
– Sections 2 and 3
44MER Indicator Reference Guide
• MER 2.0 (v2.3) was
released on September 26,
2018.
• Guidance incorporates data
flow examples and sample
visualizations for new or
more complex indicators
• 35 total indicators:
• 7 new indicators: AGYW_PREV,
CXCA_SCRN, CXCA_TX,
HTS_INDEX, HTS_RECENT,
PrEP_CURR, TX_ML
• 1 indicator retired: TX_RET
• 1 indicator moved from core MER to
host country reporting: HRH_STAFF
45PEPFAR Financial Classification
The PEPFAR financial classification is a
structure whereby PEPFAR activities
Monitoring
and services and corresponding budgets
PEPFAR Program
and expenditures can be conveniently Expenditures
and uniformly organized, clearly
identified, and easily accounted.
It answers the following questions:
1. Organization: Who is spending?
2. Program: What is the purpose?
3. Beneficiary: Who benefits?
4. Object: What was purchased?
The Monitoring PEPFAR Program
Expenditures document provides an Financial
overview of how the structure and Classification
Reference Guide
content of expenditure reporting are
different in FY 2018 to reflect PEPFAR’s
shift from target-based budgeting to
program-based budgeting.
46COP 19 Process – Key Dates
Activity Date
Draft guidance posted for public comment December 1 - 21, 2018 (tentative)
Final guidance released January 16, 2019
In-country strategic retreats January 28 – February 1, 2019
COP 19 In-Person Planning Meetings Group 1: March 4-8, 2019 (South Africa)
Group 2: March 11-15, 2019 (South Africa)
Group 3: March 18-22, 2019 (South Africa)
Asia: April 1-5, 2019 (Bangkok)
Western Hemisphere: April 8-12, 2019 (DC)
COP submission Group 1 March 29, 2019
Group 2: April 5, 2019
Group 3: April 12, 2019
Asia: April 19, 2019
Western Hemisphere: April 26, 2019
Virtual COP approval Groups 1-3: April 15 -25, 2019
Asia + Western Hemisphere: April 30, 2019
Group 1: Burundi, Ethiopia, Kenya, Malawi, Rwanda*, South Sudan, Tanzania, Uganda
Group 2: Botswana, Lesotho, Mozambique, Namibia/Angola, South Africa, Eswatini, Zambia, Zimbabwe
Group 3: Cameroon, Cote d’Ivoire, DRC, Haiti/DR, Nigeria, Ukraine, Vietnam, West Central Africa
*Rwanda-specific guidance forthcoming
47Select Programmatic
and Initiative
Updates
48Key Populations Investment Fund
(KPIF)
49Status Update on KPIF
• IAS announcement on transition to traditional funding mechanism
through PEPFAR Implementing Agencies (CDC and USAID)
• Funds recently received Congressional approval via the normal
Congressional notification process utilized for all PEPFAR funding
and being apportioned to agencies.
• S/GAC has been working with senior agency leadership and SMEs
to plan and coordinate the implementation of the KPIF, including
prioritization of populations, geography and activities.
• A priority is to use current prime local implementing mechanisms to
program grassroots indigenous peer-led KP prevention and
treatment services to key populations.
#PEPFAR15
50KPIF Planned Activities
• Increase KP testing coverage and HIV case finding
through confidential KP-competent self-testing, index
testing, and social network testing strategies with 100%
linkage to treatment and preventions services
• Address structural barriers that inhibit access to and the
effectiveness of HIV services
• Retain KP and achieve viral load suppression
• Scale Undetectable=Untransmittable (U=U) messaging
• Scale PrEP delivery through community-and-facility
based models
• Strengthen the capacity of KP-led indigenous
organizations to implement and document the success
of community-focused HIV and wraparound services
#PEPFAR15
51Opportunities for KP and CSO
Engagement
• Ensure KPIF is a regular agenda item for headquarters-based
meetings with CSOs
• Directed USAID and CDC to ensure local KP groups have been
consulted at the country level prior to finalization and implementation
of country-specific KPIF plans
• Once KPIF implementation has begun, country teams will include
KPIF updates and performance as part of their regular engagements
with local CSOs
#PEPFAR15
52TB
53PEPFAR TB Priorities
1st 95:
• Find and test TB symptomatics (not just TB
pts) for HIV
2nd 95:
• Ensuring all TB/HIV pts receive ART
• Extra dolutegravir (50 mg) for TB/HIV pts on
TLD
3rd 95:
• Integrated TB/HIV Care: Improve retention and
adherence by ensuring all PLHIV with TB
managed in one clinic
Cross-cutting efforts to reduce mortality:
• Improve TB screening and diagnosis in ART patients
Screen for TB symptoms at HIV diagnosis and each clinical encounter
TB symptoms trigger GeneXpert (MTB/RIF) Ultra for all PLHIV with symptoms; urine LAM
for any hospitalized PLHIV with advanced disease
• Increase TB preventive therapy (TPT)
Monitor for adverse events and document completion of therapy
#PEPFAR15
54PEPFAR’s Commitment to TB/HIV Services
• PEPFAR will take responsibility for TB Prevention Treatment (TPT) among enrolled
PLHIV, leveraging the established platform to fully and efficiently provide TPT
• TB/HIV Community of Practice has been formed that includes the PEPFAR
interagency TB, HIV care and treatment, and M&E experts
• Landscape analysis being conducted to better describe country obstacles and
issues for TB & TB/HIV services
• Working with Unitaid and the Aurum Institute to negotiate the cost of rifapentine
(with Sanofi) and to generate manufacturer interest in producing a generic version.
• A full toolkit for TPT implementation has been developed with an educational
webinar series based on it.
• Partnering with Aurum on their IMPAACT4TB platform to better study the potential
impact and feasibility of using the shorter rifapentine-based regimens in PEPFAR
countries.
#PEPFAR15
55DREAMS Achievements & Results
56DREAMS In-person Deep Dive
• Sent teams to 10 original DREAMS countries to better
understand:
• DREAMS Implementation
• Context
• Exploring the following topics and linking with results:
• Core package
• Components of core package implemented and excluded (where & why)
• Changes in core package over time
• Components slow/fast to roll out
• Primary partners & stakeholders, including governance structures
• Rigor of implementation monitoring
• Recruitment of most vulnerable AGYW
• Entry points, criteria
• Layering of interventions
• Country contextConclusions from DREAMS
Monitoring
• Teams are recruiting vulnerable AGYW, but perhaps not the MOST
vulnerable
– Sources: Population Council implementation science & country
narratives
– ACTION TAKEN gathering vulnerability assessments used in each
country to assess where improvements can be made
• Teams report a focus on layering in their implementation of
DREAMS, but few can document their progress quantitatively
– Source: Semi-annual narratives, site visit observations
– ACTION TAKEN New MER indicator that will require teams to have
systems to track layering for unique AGYW. We will now be able to track
layering progress over time at the district level.What we have learned and the
questions that remain
• Comprehensive prevention interventions work for AGYW – most
of the time, and in most places
• What factors might explain differences in new diagnoses between
districts?
o Number of implementing partners; presence of coordinating partner
o Differential VMMC and treatment coverage for young men
o Fidelity to DREAMS evidence-base
• What might explain difficulty achieving results in urban settings?
o How do AGYW lives differ in urban & rural settings?
o What programming changes might help in urban settings?MenStar Coalition
6061
Structure of the Partnership:
Private Sector will focus on the Demand; PEPFAR will focus on the Supply
DEMAND:
Will use its core
competencies in consumer
marketing to develop
segmented messages, SUPPLY:
Will make service
branding, and an overall
delivery/facility-based changes,
marketing campaign to optimized testing strategies, self-
improve the demand for testing, and decentralized,
healthcare services by men community-based services to
improve the supply of healthcare
services for men
62We have a marketing challenge to solve
• We need to improve the demand for healthcare
services by men.
• The private sector is working to solve this challenge
by trying new and different things.
• They are using their core competencies to develop
segmented messages, branding, and an overall
marketing campaign.
• They have already uncovered some valuable
insights that they are using to inform their
campaigns (see next slide).
• Additionally, they are funding HIV Self-Testing
through a number of different avenues.
63Insights: Qualitative Research Findings
• Men do not know the benefits of early testing and treatment
• Men are not indifferent; they are scared
• Many men live with unresolved grief and trauma, as well as
high stress
• Men experience going to the clinic as deeply disempowering
• Fear of disclosure, particularly to one’s main partner, can be
paralyzing
• A positive test threatens a man’s life AND his identity as a
man
• Men who did not actively choose to test may be less likely to
start treatment
Breaking the Cycle of Transmission:
Increasing uptake of HIV testing, prevention and 64
linkage to treatment among young men in South AfricaPEPFAR Status Update
• We are committed to breaking the cycle of transmission and
achieving epidemic control by employing innovative programmatic
approaches over the next year to reach more men with HIV treatment
services.
• We are holding ourselves accountable through clearly outlined
targets to measure progress against. Our goal is to reach an additional 1
million men aged 24-35 with lifesaving HIV services and to virally
suppress 90% of them.
• We have provided our PEPFAR Country Teams with technical
guidance for their COP planning on strategies that could yield greater
results by either being implemented alone or in combination.
• Through our Epidemic Control Teams we have identified successful
solutions that we intend to scale-up (i.e. Men’s Corners in Lesotho;
Community Adherence and Support Groups).
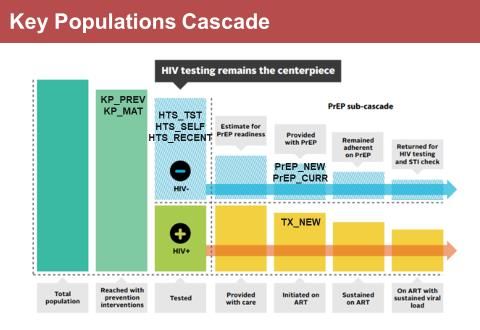
65What indicators are we collecting, and why?
• PEPFAR Monitoring, Evaluation, and Reporting (MER)
indicators will be used to track progress towards coverage
goals, help identify and prioritize geographies, and identify
opportunities for course-correct, as needed.
• MER indicators include:
HTS_TST – Number of men who received HIV testing
services
HTS_TST_POS – Number of men who received HIV
testing services and tested positive
HTS_SELF – Number of HIV self-test kits distributed
TX_CURR – Number of men currently receiving
antiretroviral therapy
TX_NEW – Number of men newly enrolled on
antiretroviral therapy in current quarter
TX_NET_NEW – Net increase number of men currently
on antiretroviral therapy (difference in quarterly
TX_CURR)
TX_PLVS – Percentage of antiretroviral therapy
patients with a suppressed viral load
*Indicators will be aligned to the age group 25 – 34 years, to
the extent possible.
66Enhancing Faith-Based Engagement
to Reach HIV Epidemic Control
2018
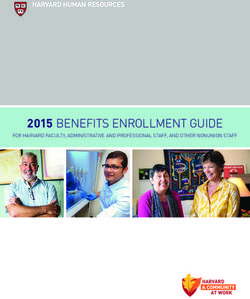
67Reaching Well Men, Women, and Children,
Where They Are:
Pew-Templeton Research
How often do you attend religious services?
“>= Weekly or 1-2 times/month”
BOTSWANA 77
SOUTH AFRICA 82
UGANDA 89
MOZAMBIQUE 91
NIGERIA 91
KENYA 91
RWANDA 82
ZAMBIA 92
TANZANIA 86
0 20 40 60 80 100
PercentageFBO Strategy Staffing Structure
• Three assessment teams – of 3 HQ staff each
• Each team concentrates on FBO priority focus
areas for COP 2018, with primary focus on one
area and secondary focus on remaining two areas
– Reaching men and boys
– Sexual violence prevention and HIV prevention
through avoiding sexual risk among 9-14 year
olds
– Pediatric and adolescent treatment
• Prioritize 10 countries for 2018 – Malawi, Zambia,
Eswatini, Botswana, Lesotho, Haiti, Uganda,
Zimbabwe, Tanzania, Kenya
• Timing of assessments – all completed by Dec 7,
2018Purpose & Objectives Purpose: Identify opportunities to advance reaching HIV epidemic control through enhancing engagement with faith-based partners, including FBOs, FBHPs, & faith communities Objective #1: To engage with key faith-health leaders and organizations to map and analyze the: 1. Access, influence, and capacity of existing faith-based and new indigenous partners to reach well men & boys, women & girls, and underserved in informal settlements, with a focus on gap analysis 2. FBO structures and networks that may be options for advancing education re: 90-90-90 cascade for well men, women, children, and the underserved 3. Potential of existing FBO and new indigenous partners to reach well men, women, children, and underserved with: Services – Optimized testing, linkage/retention, VMMC; and Prevention of sexual violence & HIV through sexual risk avoidance, ages 9-14 4. Potential of existing and new indigenous faith-based partners to prevent harm by addressing stigma and discrimination, and influence of faith healing in religious congregations on ARV adherence
Purpose & Objectives
Objective #2: Based on fact-finding mission for
mapping and gap analysis, develop preliminary
recommendations for enhanced engagement with faith-based partners:
• Tier One: Raise awareness and engage existing and new indigenous faith-
based partners in strategic areas
• Tier Two: Build capacities of existing and new indigenous faith-based groups to
advance services and prevention through their existing structures
• Tier Three: Extend engagement and integration of FBOs and faith-based
groups into current testing, OVC, prevention platforms at clinic/community level
in select SNUsPEPFAR Reauthorization
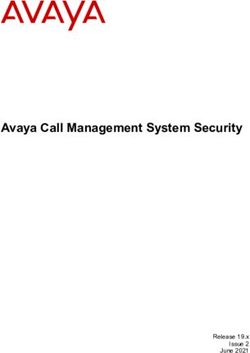
72PEPFAR Reauthorization 2018
• The U.S. House passed H.R.6651 PEPFAR Extension Act of 2018 under suspension by voice vote on November 13 th.
• The U.S. Senate is poised to pass HR.6651 PEPFAR Extension Act of 2018 through the hotline process of unanimous
consent the week of November 26th.
• The Senate and House bills are identical and extend the current PEPFAR authorities through 2023.
U.S. Senate Sponsors & Cosponsors U.S. House Sponsors & Cosponsors
Sen. Corker, Bob [R-TN] 09/18/2018 Rep. Smith, Christopher [R-NJ-4] 08/03/2018
Sen. Menendez, Robert [D-NJ] 09/18/2018 Rep. Lee, Barbara [D-CA-13] 08/03/2018
Sen. Cardin, Benjamin L. [D-MD] 09/25/2018 Rep. Royce, Edward R. [R-CA-39] 08/03/2018
Sen. Rubio, Marco [R-FL] 09/25/2018 Rep. Engel, Eliot L. [D-NY-16] 08/03/2018
Sen. Isakson, Johnny [R-GA] 09/25/2018 Rep. Ros-Lehtinen, Ileana [R-FL-27] 08/03/2018
Sen. Young, Todd C. [R-IN] 09/25/2018 Rep. Bass, Karen [D-CA-37] 08/03/2018
Sen. Udall, Tom [D-NM] Rep. Fitzpatrick, Brian K. [R-PA-8] 09/25/2018
09/25/2018 Rep. Connolly, Gerald E. [D-VA-11] 09/26/2018
Sen. Booker, Cory A. [D-NJ] 09/25/2018 Rep. Sherman, Brad [D-CA-30] 09/27/2018
Sen. Coons, Christopher A. [D-DE] 10/03/2018 Rep. Reichert, David G. [R-WA-8] 09/27/2018
Sen. Sullivan, Dan [R-AK] 10/03/2018 Rep. Cicilline, David N. [D-RI-1] 09/27/2018
Sen. Boozman, John [R-AR] 10/03/2018 Rep. McCaul, Michael T. [R-TX-10] 09/27/2018
Sen. Shaheen, Jeanne [D-NH] 10/03/2018 Rep. Thomas Garrett [R-VA-5] 10/30/2018
Sen. Alexander, Lamar [R-TN] 10/11/2018 Rep. Alcee Hastings [D-FL-20] 11/09/2018
Sen. Kaine, Tim [D-VA]
10/11/2018
Sen. Durbin, Richard J. [D-IL] 10/11/2018
Sen. Sasse, Ben [R-NE]
10/11/2018
Sen. Joni Ernst [R-IA] 11/13/2018
Sen. Elizabeth Warren [D-MA] 11/13/2018
Sen. Shelley Moore Capito [R-WV] 11/13/2018
73
Sen. Jeff Merkley [D-OR] 11/13/2018World AIDS Day
2018
74World AIDS Day 2018 – Latest Results
Stay tuned to www.pepfar.gov for updates and
announcements:
• Annual program results
• New results from Nigeria AIDS Indicator and
Impact Survey (NAIIS) and Ethiopia Population-
based HIV Impact Assessment (PHIA)
• PEPFAR receipt of Eisenhower Global Citizens
Award (BCIU)
• Participation at Mandela 100: Global Citizens
Festival in South Africa
• DREAMS report with 3 year impact data
• A Global Battle: An Atlantic Forum on HIV/AIDS
Today
75Thank You
You can also read