Percutaneous Ultrasonic Fasciotomy: A Novel Approach to Treat Chronic Plantar Fasciitis - Clerisy publishers
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Journal of
Surgical Procedures and Techniques
Research Open Access
Percutaneous Ultrasonic Fasciotomy: A Novel Approach to Treat Chronic
Plantar Fasciitis
Rahul Razdan1,*, Eric Vander Woude1, Aaron Braun1, Bernard F. Morrey2
1
Vascular and Interventional Radiology, Advanced Medical Imaging, Lincoln, Nebraska 68506
2
Professor of Orthopedic Surgery, University of Texas Health Science Center, San Antonio, Texas
*Corresponding author: Rahul Razdan, Vascular and Interventional Radiology, Advanced Medical Imaging, Lin-
coln, Nebraska 68506; E-mail: razdanr@gmail.com
Received Date: May 04, 2018 Accepted Date: June 01, 2018 Published Date: June 04, 2018
Citation: Rahul Razdan (2018) Percutaneous Ultrasonic Fasciotomy: A Novel Approach to Treat Chronic Plantar
Fasciitis. J Surg Proced Tech1: 1-6.
Abstract
Purpose: Evaluate percutaneous ultrasonic fasciotomy as a safe and definitive treatment for chronic, refractory plantar
fasciopathy.
Methods: Prospectively gathered and retrospectively analyzed the data from 100 consecutive procedures performed be-
tween August 2013 through May 2014 was assessed. Inclusion criteria included symptomatic plantar fasciitis for a minimu-
mof 4 months’ duration and failure of at least one conservative treatment measure. Patients were treated with the Tenex-
Health TX1™ device with a standardized procedure. Time of TX1 activation was at the discretion of the operator. All patients
completed a standardized postprocedure rehabilitation program. Foot and Ankle Disability Index (FADI) score was assessed
preprocedure, 2 weeks, 6 weeks and 6 months’ postprocedure.
Results: FADI scores indicated symptomatic improvement at each assessed time point (P
2
Introduction The plantar fascia connects the medial calcaneal tu-
Chronic plantar fasciitis, or fasciopathy, is the most berosity to the proximal aspect of the phalanges, plays a ma-
common debilitating foot complaint, affecting approximately jor role in supporting the medial longitudinal arch, and aids
10% of the population and accounting for over one million of- in dynamic shock absorption [7]. The term plantar fascia is
fice visits and nearly $300,000,000 per year [19]. This condi- actually a misnomer since this structure is not a facial layer,
tion most commonly affects women age 40 -60 years [16]. Risk but a tendinous aponeurosis that shares histological and me-
factors include excessive running, limited ankle dorsiflexion, chanical traits with tendons and ligaments [3]. Currently the
flatfoot deformity, obesity, and prolonged work-or activity- most commonly offered treatment for chronic plantar fascii-
related weight bearing [16]. tis is open surgical plantar fasciotomy which results in only
Plantar fasciitis is a condition characterized by de- moderate patient success rates, extended recovery times, and
generation of the plantar fascia and perifascial structures with potential complications such as plantar fascial rupture, medial
isolated inferior heel pain, particularly with the first steps of longitudinal arch destabilization and altered loading patterns
the day and after prolonged sitting [9]. Diagnosis of chronic [12]. Percutaneous ultrasonic fasciotomy is a minimally inva-
plantar fasciitis is predicated on clinical history of tenderness sive ultrasound guided method of cutting and removing ten-
over the medial tubercle of the calcaneus (the plantar fascial dinopathic tissue. Percutaneous ultrasonic plantar fasciotomy
insertion site) with weight bearing of at least 3 months’ dura- has been previously described. However these procedures do
tion, first-step pain in the morning and pain relief and pain not remove the diseased tissue and the available literature re-
reproduced with manual palpation over the medial calcaneal ports only small patient cohorts and limited duration of follow
tubercle [22]. Imaging techniques can be employed to aid in up.
diagnosis of plantar fasciitis. Plantar calcaneal heel spur is vis- The purpose of this study was to assess the safety, efficacy and
ible on lateral foot x-ray in 38.3% of cases [22]. Ultrasound im- durability of ultrasound guided percutaneous ultrasonic fasci-
aging has been demonstrated to be both sensitive and specific otomy as a definitive treatment for chronic plantar fasciitis in
for diagnosis of plantar fasciitis (Figure. 1). a relatively large patient cohort.
Materials and Methods
This is a prospective non randomized study of 100
consecutive patients who were enrolled between August 2013
and May 2014. Evaluation and treatment was performed by
one of two different interventional radiologists in a single out-
patient surgery center. All patients provided verbal consent
to allow their depersonalized clinical and imaging data to be
used in this study. This study was approved by the internal re-
view board of Catholic Health Institute.
Inclusion criteria included: duration of symptoms > 4
months and failure of at least one conservative treatment includ-
ing but not limited to, analgesics, activity modification, physical
therapy and arch supports. Patient sex, age, Body Mass Index
(BMI), TX1 device activation time and plantar fascia thickness
were recorded along with individual clinical features (Table 1).
Average Value (±1 SD)
Figure 1. An ultrasound image of normal plantar fascia (left). Female gender 72%
Chronic fasciitis is associated with hypoechoic thickening of Age (y) 50.4 ± 12.8
the attachment site at the medial tubercle of the calcaneus
Body Mass Index (BMI) 29.8 ± 5.5
(right).
Treatment Time (seconds) 103 ±24
Ultrasound features of plantar fasciitis include plan- Plantar Fascia Thickness 6.1 ±1.2
tar fascial thickness >4mm, hypoechoic appearance of the
plantar fascia and loss of fascia edge sharpness [17]. MRI has Table 1: Summary of patient, disease and treatment charac-
also been shown to be an effective diagnostic tool in the evalu- teristics
ation of plantar fasciitis [2].
The Foot and Ankle Disability Index (FADI) score
(Figure.2) was collected preprocedure, 2 weeks, 6 weeks and 6
months postprocedure. This index recognizes 5 levels of pain
from none (0) to unbearable (4) for 4 activity levels [10].
Clerisy Publishers J Surg Proced Tech 2018 | Vol 3: 102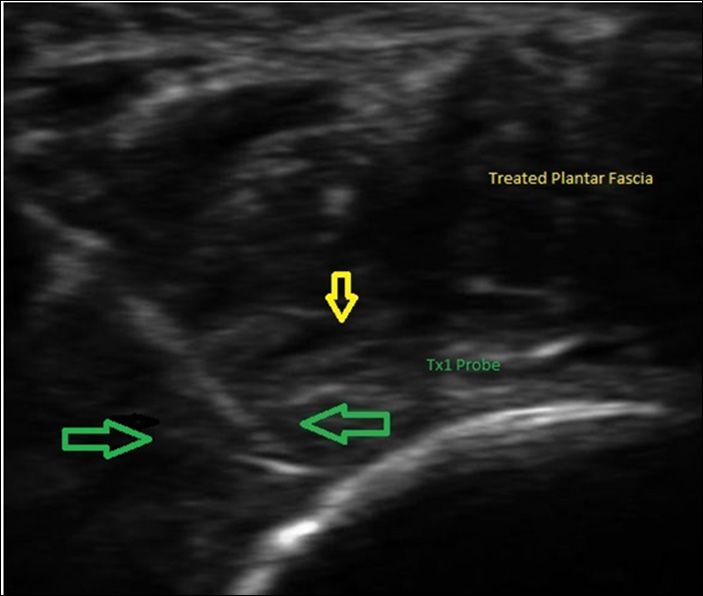
3
Patient Name: _________________________________________ Date: __________
Please answer every question with one response that most closely describes your condition within the past week by
marking the appropriate number in the box. If the activity in question is limited by something other than your foot or
ankle, mark N/A.
0 Unable to do 2 Moderate difficulty 4 No difficulty
1 Extreme difficulty 3 Slight difficulty
Standing Walking up hills
Walking on even ground Walking down hills
Walking on even ground without shoes Going up stairs
Walking on uneven ground Going down stairs
Stepping up and down curves Squatting
Sleeping Coming up to your toes
Walking initially Walking 5 minutes or less
Walking approximately 10 minutes Walking 15 minutes or greater
Home responsibilities Activities of Daily Living
Personal Care Light to moderate work (standing, walking)
Heavy work (push/pulling, climbing, carrying) Recreational activities
Sports Module:
Running Jumping
Landing Squatting and stopping quickly
Cutting, lateral movements Low-impact activities
Ability to perform activity with your normal Ability to participate in your desired sports as
technique long as you would like
Pain related to the foot and ankle:
0 Unbearable 2 Moderate Pain 4 No Pain
1 Severe Pain 3 Mild Pain
General level of pain Pain at rest
Pain during your normal activity Pain first thing in the morning
Heavy work (push/pulling, climbing, carrying) Heavy work (push/pulling, climbing, carrying)
Figure 2: Details of the FADI. Note comprehensive nature of this tool.
Statistical analysis: Procedure Technique
All statistical analysis was conducted by a professional The TX1 device (Tenex Health, Lake Forest, CA) con-
statistician at the University of Nebraska. Linear mixed models sists of a handheld 18G needle based probe the tip of which
were estimated using restricted maximum likelihood (REML) when activated, oscillates at a proprietary ultrasonic frequency
in SAS PROC MIXED to investigate the overall pattern of specifically calibrated to cut tendinopathic tissue while having
change that was present in the data. An initial model which little effect on normal tissue. Saline irrigation passes through
is equivalent to the multivariate repeated measures analysis an outer sleeveinto the treatment field as it cools the ultrasonic
of variance (ANOVA) model was estimated using an unstruc- tip; a vacuum provides simultaneously aspirates and removes
tured R matrix (i.e., each variance and covariance parameter the cut and debrided tissue through the needle lumen (Figure.
between the four time points was allowed to vary) as well as a 3).
saturated means model (SAS 9.3). The model included three
covariates (i.e., age, BMI, and plantar fascia thickness) as well
as each covariant’s interaction with linear and quadratic time
trends. The final model included linear and quadratic trends
over time, age, treatment duration, interaction between linear
trend and treatment time, and interaction between the linear
trend and age.
Clerisy Publishers J Surg Proced Tech 2018 | Vol 3: 102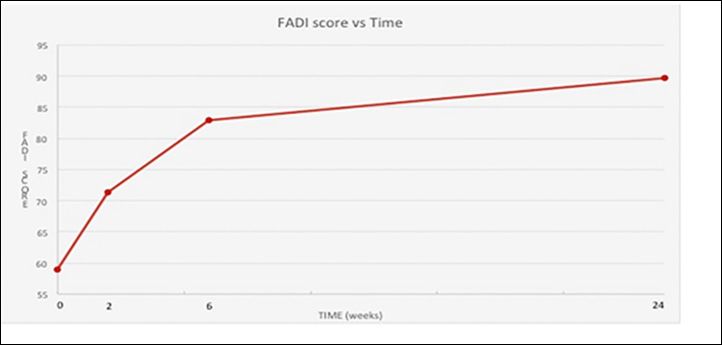
4
The duration of activation was at the discretion of the
operator and ranged from 46 to185 seconds. Technical success
was defined as the ability to place and activate TX1 hand piece
into pathologic portion of the plantar fascia. A standardized
postprocedure rehabilitation program consisted of placing the
treated foot in a pneumatic cam walker boot for 2 weeks’ dura-
tion. A physical therapy program was initiated on post op day
3 consisting of education on stretching and exercise, evalua-
tion for shoe inserts and gait evaluation.
Results
Technical success, identifying and entering the le-
sion, was achieved in 100% of patients. As noted Foot and An-
kle Disability Index (FADI) scores were assessed preprocedure,
2 weeks, 6 weeks, and 6 months postprocedure.Patient follow
up was 100% (100 patients) at 2 weeks, 94% (94 patients) at 6
weeks and 82% (82 patients) at 24 weeks post procedure. Aver-
age FADI scores were 59 preprocedure, 71 at 2 weeks, 83 at 6
weeks and 90 at 24 weeks post procedures (P5
Complications The documented outcomes reveal an excellent safety
Our study protocol stratified potential complications profile with no reportable minor or major complications. This
as minor or major based on Society of Interventional Radiolo- is consistent with several reports utilizing the TX1 device for
gists consensus criteria. (www.sirweb.org; practice guidelines) treatment of elbow tendinopathy [1,13,18].
However, there was only one minor complication of a patient The high procedural success rate appears to be inde-
who experienced moderate post procedure related pain which pendent of plantar fascial thickness, BMI or patients’ age. Cur-
resolved with a 3 day course of tramadol.No additional pro- rently the optimal activation time for plantar fascial treatment
cedure related complications were encountered. Specifically, cannot be defined based on the existing clinical evidence.
there were no post procedure infections, plantar fascia rup- However, this study suggests that longer treatment times may
ture, or nerve injury. result in better outcomes. This experience suggests the most
effective treatment time is between 2 and 3 minutes. Further
Discussion study is warranted in regards to length of activation time. Im-
portantly, additional treatment time does not appear to subject
Plantar fasciitis when diagnosed in its acute stage the patient to addition risk of complications.
(6
References 18) Seng C, Mohan PC, Koh SB, et al. (2016) Ultrasonic percu-
1) Barnes DE, Beckley JM, Smith J (2015) Percutaneous ul- taneous tenotomy for recalcitrant lateral elbow tendinopathy.
trasonic tenotomy for chronic elbow tendinosis: a prospective Am J Sports Med. 2:504-510.
study. J Shoulder Elbow Surg. 1:67-73. 19) Tong KB, Furia, J (2010) Economic burden of plantar fas-
2) Berkowitz JF, Kier R, Rudicel S (1991) Plantar fasciitis: MR ciitis treatment in the United States. Am J Orthop.39:227-231.
imaging. Radiology 179: 665–667.
20) Traister L (2014) The Effect of Percutaneous Tenotomy Us-
3) Boabighi A, Kuhlmann JN, Luboinski J, Landjerit B (1993) ing Tenex On Short Term Average Pain Scores in Refractory
Aponeuroses and superficial fascia. Mechanical and structural Tendinopathies. Annual Meeting of American Medical Soci-
properties. Bull AssocAnat (Nancy) 77: 3–7. ety for Sports Medicine.
4) Davis PF, Severud E, Baxter DE (1994) Painful heel syn- 21) Wolgin M, Cook C, Graham C, Mauldin D (1994) Con-
drome: Results of nonoperative treatment. Foot Ankle servative treatment of plantar heel pain: Long-term follow-up.
Int.15:531–535. Foot Ankle Int.15:97–102.
5) Elattrache N, Morrey B (2013) Percutaneous Ultrasonic
22) Yi TI, Lee GE, Seo IS, Huh WS, Yoon TH, Kim BR (2011)
Tenotomy as a Treatment for Chronic Patellar Tendinopathy –
Clinical Characteristics of the Causes of Plantar Heel Pain.
Jumper’s Knee. Operative Techniques in Orthopaedics. 23:98-
Annals of Rehabilitation Medicine.35:507-513.
103.
6) Kamineni S, Butterfield T, Sinai A (2015) Percutaneous ul-
trasonic debridement of tendinopathy-a pilot Achilles rabbit
model. J OrthopSurg Res.10:70.
7) Khan KM, Cook JL, Taunton JE, Bonar F (2000) Overuse
tendinosis, not tendinitis part 1: A new paradigm for a difficult
clinical problem. Phys Sportsmed. 28:38-48.
8) Koh JS, Mohan PC, Howe TS, Lee Bp, Chia SL, Yang Z, et al.
(2013) Fasciotomy and surgical tenotomy for recalcitrant lat-
eral elbow tendinopathy: early clinical experience with a novel
device for minimally invasive percutaneous microresection.
Am J Sports Med 41: 636-644.
9) Lynch DM, Goforth WP, Martin JE, Odom RD, Preece CK,
Kotter MW (1998) Conservative treatment of plantar fasciitis.A
prospective study. J Am Pediatr Med Assoc.88:375–380.
10) Martin RL, Burdett RG, Irrgang JJ (1999) Development of
the Foot and Ankle Disability Index (FADI).J Orthop Sports
Phys Ther. 29: A32-33.
11) Martin RL, Irrgang JJ, Conti SF (1998) Outcome study
of subjects with insertional plantar fasciitis. Foot Ankle Int.
19:803–811.
12) Miller L, Latt D (2015) Chronic Plantar Fasciitis is Me-
diated by Local Hemodynamics: Implications for Emerging
Therapies. N Am J Med Sci. 7:1-5.
13) Mohan PC, Koh JSB, Morrey BF, Lee BPH, Howe TS, Png
MA (2015) Lateral elbow tendinopathy: correlation between
ultrasound findings and clinical outcomes after percutaneous
ultrasonic tenotomy. ECR Congress.
14) Patel MM (2015) A novel treatment for refractory plantar Submit your manuscript to Clerisy journals
fasciitis.Am J Orthop 44:107-110.
and benefit from:
15) Patel MM, Patel SM, Patel SS, Daynes J (2015) A pilot
study of a novel treatment method for refractory painful plan- ¶¶ Convenient online submission
tar fibromas.Austin J Orthopade&Rheumatol.2:1014. ¶¶ Rigorous peer review
16) Riddle DL, Pulisic M, Pidcoe P, Johnson RE (2003) Risk ¶¶ Immediate publication on acceptance
factors for Plantar fasciitis: A matched case-control study. J ¶¶ Open access: articles freely available online
Bone Joint Surg Am. 85-A:872–877.
¶¶ High visibility within the field
17) Sabir N, Demirlenk S, Yagci B, Karabulut N, Cubukcu S
(2005) Clinical Utility of Sonography in Diagnosing Plantar ¶¶ Better discount for your subsequent articles
Fasciitis. J Ultrasound Med 24: 1041-1048. Submit your manuscript at
http://www.clerisyonlinepublishers.org/submit-manuscript.
Clerisy Publishers J Surg Proced Tech 2018 | Vol 3: 102You can also read