Progressive supranuclear palsy (PSP): General
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

PSP
48
23/03/07 PSP
Progressive supranuclear palsy (PSP): General
pathology and visual signs and symptoms
Richard Armstrong, Vision Sciences, Aston University
P
rogressive supranuclear palsy (PSP) This article describes the general clinical and
is a rare, degenerative disorder of the pathological features of PSP, its specific
brain believed to affect between 1.39 visual signs and symptoms, discusses the
and 6.6 individuals per 100,000 of usefulness of these signs in differential
the population. The disorder is likely to be diagnosis, and considers the various
more common than suggested by these data treatment options.
due to difficulties in diagnosis, and
especially in distinguishing PSP from other Clinical signs and symptoms
conditions with similar symptoms such as The onset of PSP is usually between 60 and
multiple system atrophy (MSA), corticobasal 65 years of age and the duration of the
degeneration (CBD), and Parkinson’s disease disease normally between 5 and 6 years.2
(PD). PSP was first described in 1964 by The average time from the appearance of
Steele, Richardson and Olszewski and early symptoms to an actual diagnosis of the
originally called Steele-Richardson- patient is 3.6 to 4.9 years but many
Olszewski syndrome.1 The disorder is the individuals with the disorder remain
second commonest syndrome in which the undiagnosed.3
patient exhibits ‘parkinsonism’, viz., a range The clinical development of PSP varies
of problems involving movement most considerably from patient to patient. The
typically manifest in PD itself, but also seen most characteristic symptoms involve
in PSP, MSA and CBD. Although primarily a difficulties with gait and balance, the patient
brain disorder, patients with PSP exhibit a walking clumsily and often falling
range of visual clinical signs and symptoms backwards. The most obvious visual sign is
that may be useful in differential diagnosis. an inability to direct the gaze of the eyes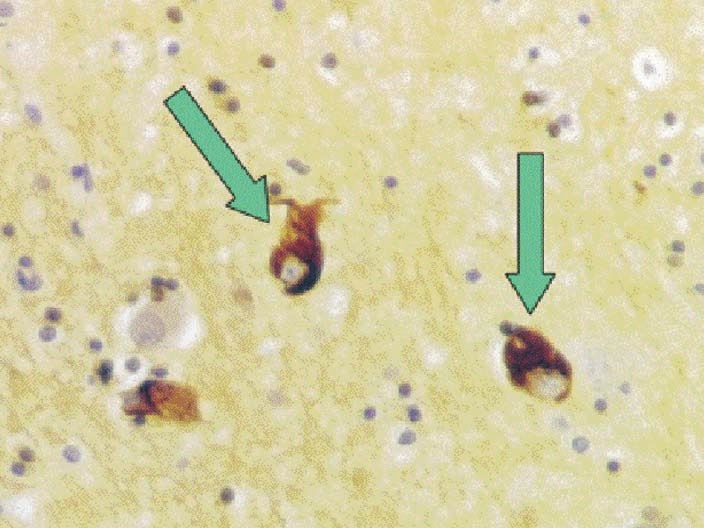
PSP
PSP. The NFT occur in at least two
different morphological forms
termed globose and flame-shaped
NFT. The NFT are accompanied by
other neurons that exhibit some
degree of abnormal swelling of the
cell body (‘ballooned neurons’)
and by the appearance of abnormal
‘tufted’ astrocytes. The human tau
gene is located on chromosome 17
and in normal individuals
produces approximately equal
amounts of two tau isoforms
termed ‘3-repeat (3R) tau’ and ‘4-
repeat (4R) tau’, depending on the
49
number of repeats of the
microtubule binding peptide
23/03/07 PSP
domain that are present. By
contrast in PSP, the ratio is 3:1 in
favour of 4R tau. Recent studies
suggest that the presence of a
mutation in exon 10 of the tau
Figure 1: Midline sagittal section of human brain showing the major areas gene can cause an increase in the
affected in progressive supranuclear palsy (PSP). splicing of this exon giving rise to
increased amounts of 4R tau.5
Another hypothesis as to the cause
downwards. These developments size. When the midbrain is of PSP suggests that a deficiency
may be accompanied by sectioned, (Figure 2), the in mitochondrial DNA causes
depression and even mild substantia nigra and red nuclei oxidative stress.6 Hence, PSP
dementia. There may be changes often appear discoloured. could result from a combination of
in personality and loss of interest On microscopical investigation, first, a mitochondrial defect that is
in the ordinary activities of life. several characteristic features of genetic or toxic in origin
The patient may tire easily, PSP are apparent. There is loss of producing an intracellular
become forgetful and lose neurons, proliferation of glial cells chemical environment that
emotional control, laughing or (gliosis), the presence of abnormal encourages tau aggregation in
crying for no apparent reason. protein aggregates in neurons combination with a genetic defect
Apathy interspersed by angry termed neurofibrillary tangles in the tau gene resulting in the
outbursts is common. As the (NFT), the appearance of vacuoles overproduction of 4R tau.
disease progresses, there is in some cells (granulovacuolar
blurring of vision and difficulty in change), and loss of myelin. The Visual signs and symptoms
controlling eye and eyelid distribution of the pathological Approximately two-thirds of PSP
movements. Speech becomes features in the brain shows a patients will develop visual
slurred and the patient finds it consistent pattern. The globus symptoms within the first year. For
increasingly difficult to swallow pallidus is nearly always affected the purpose of this article these
solid food or liquid. Tremor of the along with the subthalamic symptoms will be considered
hands, a common sign in many nucleus, red nucleus, substantia under the following headings, viz.,
patients with PD,4 however, is rare nigra, periaqueductal gray matter, those affecting: a) eyelids,
in PSP. pontine tegmentum, and dentate b) pupillary function, c) fixation,
nucleus. d) eye movements,
Pathological features The appearance of NFT in e) the vestibulocular reflex,
At post-mortem, the brain of a specific brain areas is a f) psychophysical performance,
patient with PSP may show only characteristic pathological sign of and g) electrophysiology (Table 1).
minor abnormalities and is often PSP (Figure 3). The most
normal in appearance (Figure 1). important molecular constituent of Eyelids
Brain weight may be reduced to the NFT is the microtubule A disorder of eyelid mobility has
some extent compared with associated protein (MAP) tau, been observed in approximately a
normal and if there are brain which is involved in the assembly third of PSP patients7 with both
abnormalities present, these and stabilization of the spontaneous and voluntary eye
usually involve the midbrain microtubules. This observation has movements affected8. Since ocular
which can be shrunken in suggested to researchers that and eyelid movements are highly
appearance. In the cerebellum, the aggregation of an abnormal form of coordinated mainly in the vertical
superior peduncles and the tau may be the most immediate plane, supranuclear
dentate nuclei may be reduced in cause of brain malfunctioning in ophthalmoplegia with downgaze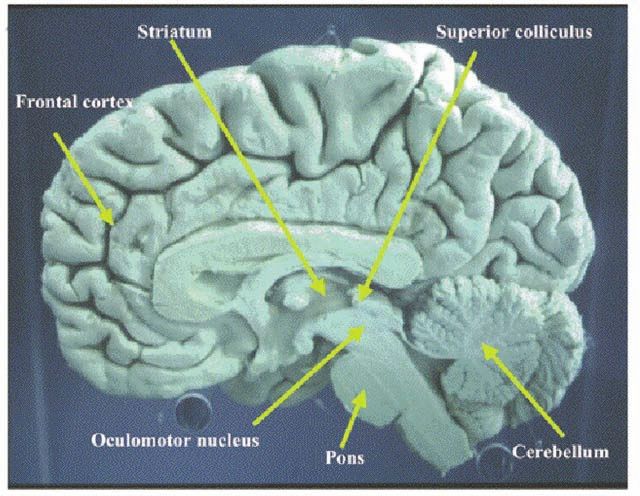
PSP
impairment is often regarded as a system10,11 and as a consequence, PSP patients also exhibit a slowing
cardinal feature of PSP. Eyelid reflexes pupil dilation in response to of saccadic eye movements, a
are generally preserved with the tropicamide may be similar to that of significantly decreased ability to carry
exception of the ‘acoustic startle patients with Alzheimer’s disease out vertical saccades, and early
reflex’, which is a response to a (AD), thus further demonstrating the slowing of horizontal saccades.16
sudden and unexpected sound non-specific nature of the tropicamide Additional saccadic movements are
involving a brief closing of the eye. effect.10,12 often necessary for PSP patients to
Eyelid problems in PSP can seriously achieve fixation especially in the
impair vision as a result of difficulties Fixation vertical plane.17 Saccadic eye
in opening the eyes after voluntary Abnormal ocular fixation has been movements involve the frontal eye-
closure (apraxia of eye opening). This shown in seven out of eight patients fields, the supplementary eye-fields,
problem is likely to be attributable to a with PSP14; individuals demonstrating the parietal and occipital cortices, as
loss of the reciprocal relationship a ‘fixation instability’ accompanied by well as the superior colliculus and
between the levator palpebrae and the side to side movements of the head.13 cerebellum. Neuronal loss specifically
pretarsal portion of the orbicularis This type of response is relatively rare in the superior colliculus and
50 oculi muscles both of which contract in PD patients.14 cerebellum may be an important cause
together rather than exhibiting a of saccadic eye movement problems in
23/03/07 PSP
normal opponent action.9 Eye movements PSP.
Eye movement problems are a Smooth pursuit movements may also
Pupillary function characteristic feature of patients with be affected, the median gain of the
Some studies have demonstrated that PSP. One of the cardinal signs of the pursuit movements being less than in
the latency and amplitude of the blink disease is a ‘supranuclear normal subjects.18 Hence, small
reflex response is normal in PSP8 ophthalmoplegia’ with downgaze corrective saccades are often necessary
whereas others suggest enhanced impairment.7 Halliday et al.15 found a to bring the eyes to the target. Smooth
recovery of the R2 response in a 40% decrease in neurons in the pursuit movements involve the
proportion of patients.9 In addition, an substantia nigra of a PSP patient with participation of several brain areas
abnormally enhanced blink reflex downgaze palsy suggesting that including the parietal and occipital
recovery curve has been detected in a degeneration of the pathway from the cortices, the frontal eye-fields, and
proportion of patients.8 PSP is also substantia nigra to the superior cerebellum as well as nuclei in the
characterised by a widespread deficit colliculus may be an important cause basal area of the pons, many of which
in the cholinergic neurotransmitter of this symptom. are likely to suffer significant neuronal
losses in PSP (Figures 1,2).19
Features Signs and symptoms Reference
Vestibulo-ocular reflex (VOR)
The vestibulo-ocular reflex (VOR) is a
Eyelids Apraxia of lid opening Vall-Sole et al 1997
reflex eye movement that stabilizes
Eyelid mobility impaired Grandas et al 1994
Lid retraction images on the retina during
Blepharospasm movements of the head. This is
Pupillary function Enhanced recovery of R2 blink reflex Piccione et al 1997 achieved by the brain inducing an eye
Normal latency and amplitude movement in the opposite direction to
the head movement. The ‘gain’ of the
Fixation Abnormal, side to side head movement Friedman et al 1992 VOR is the ratio of the change in eye
angle to head angle during a head turn.
If the gain is impaired (ratio not equal
Eye movements Supranuclear downglaze palsy Grandas et al 1994 to 1), head movements result in image
Upgaze affected Rivand-Pechoux et al 2000 motion on the retina and blurred
vision.
Decreased saccadic velocity The gain of the VOR in the dark is
Abnormal vertical saccades cancelled by fixation. The ability to
Slowing of horizontal saccades cancel this gain, however, is reduced
Impairment of horizontal smooth pursuit in PSP compared with patients with
Movements Malessa et al 1994 PD and normal subjects20, and may be
VOR Capacity to cancel ‘gain’ impaired Rascol et al 1995 related to cerebellar dysfunction in
these patients.
Psychophysics Impaired contrast perception Langheinrich et al 2000 Psychophysics
Patients with PSP exhibit impaired
contrast perception21; an effect that is
less apparent, for example, in patients
Electrophysiology Reduced ERG amplitude Langheinrich et al 2000
EMG from orbiclaris oculi reduced Vall-Sole et al 1997 with MSA.
In patients with PD, this problem is
often attributable to impaired
Table 1: Visual signs and symptoms in patients with progressive supranuclear palsy (PSP) processing of contrast in the retina.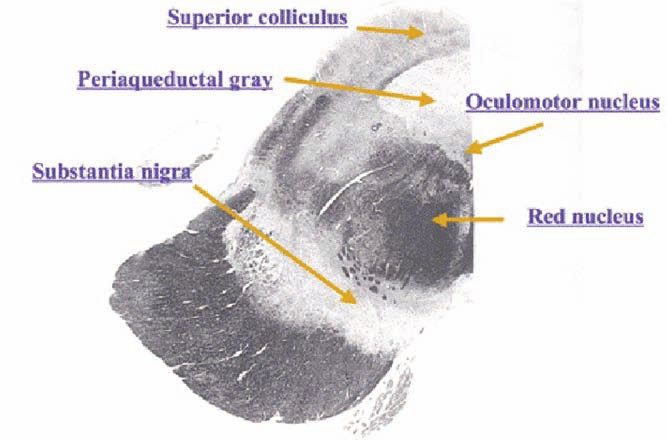
PSP
Electrophysiology
Abnormal electrophysiological
responses have been detected in PSP
patients on some tests. For example,
the amplitude of the electroretinogram
(ERG) is reduced, as is the
electromyogram (EMG) when recorded
from the orbicularis oculi muscle.
Differential diagnosis
One of the difficulties in diagnosing
PSP is that it is one of a group of
disorders in which problems with
movement are prominent and which
consequently have similar or
overlapping clinical features. This 51
group contains CBD, MSA, Lewy body
23/03/07 PSP
dementia (LBD),22 and PD. Of these
disorders, MSA often has an earlier
age of onset than PSP and frontal lobe
dysfunction is often more severe in
PSP. PSP can resemble some forms of
LBD in that both have similar ages at
presentation and duration of disease
and both may show supranuclear gaze
palsy and balance disturbance. CBD
also has a similar age of onset and Figure 2: A section of the midbrain through the substantia nigra and the red nucleus
some symptoms in common with PSP showing the major areas affected in progressive supranuclear palsy (PSP). Many of the
but the presence of abnormal gait visual problems seen in PSP result from brain degeneration affecting these areas.
accompanied by supranuclear gaze
palsy and bilateral bradykinesia in Treatment and management prevent the drying of eyes due to
PSP may enable the two disorders to Few drugs have had a consistently decreased blinking. Patients with
be distinguished. beneficial effect on the symptoms of difficulties in opening their lids may
The greatest difficulty in diagnosis patients with PSP. Hence, the drug L- have “lid crutches” fitted to spectacles
is often in separating PSP from PD dopa, which is particularly effective in frames that can hold the lids open. In
early in the disease process before treating PD, has only a transient addition, blepharospasm has been
ocular symptoms become apparent. A beneficial effect on PSP. The drugs treated successfully with botulinum
brain scan employing positron Efaroxan (alpha-2-antagonist) and toxin A injected at the junction of the
emission tomography (PET) may be Pramipexole (a dopaminergic agent) preseptal and pretarsal parts of the
helpful in separating these two have little beneficial effect on motor palpebrae and orbicularis oculi
disorders. In addition, if the patient is function whereas Zolpidem (hypnotic muscles.9
given the drug L-dopa then notable GABA-ergic agonist) does appear to
improvements in symptoms can be have some short-term benefit in PSP. Conclusions
seen in PD but the drug has less In addition, Physostigmine PSP is an uncommon
benefit in PSP. When ocular signs and (cholinesterase inhibitor) appears to neurodegenerative disease
symptoms are apparent, then the have little benefit in the treatment of characterised by symptoms that
separation between PD and PSP dysphagia in PSP. Some studies resemble those seen in other
becomes more straightforward. employing Donepezil (cholinesterase movement disorders. Although
Atypical features of PSP include inhibitor) have shown modest considerably less common than PD,
slowing of upward saccades, moderate improvements on some cognitive tasks PSP is likely to have been under-
slowing of downward saccades, the but a worsening of motor function. diagnosed in the past due to the
presence of a full range of voluntary Antidepressant medications, such as difficulties in separating it from other
vertical eye movements, a curved Prozac and Tofranil, have had some types of movement disorder.
trajectory of oblique saccades, and modest success as a treatment of PSP Nevertheless, there is a group of visual
absence of square-wave jerks.23 but they do not appear to act by signs and symptoms that may help
Particularly useful in separating PSP relieving depression. separate PSP from other movement
from PD is the presence in the former Various procedures may help the disorders most specifically PD. A
of vertical supranuclear gaze palsy, patient cope with the visual symptoms combination of vertical supranuclear
fixation instability, lid retraction, of PSP. For example, patients may gaze palsy, fixation instability, lid
blepharospasm, and apraxia of eyelid have prisms inserted into spectacles to retraction, blepharospasm, and apraxia
opening and closing.13 redirect their gaze and to help in of eyelid opening and closing may be
Downgaze palsy is probably the alleviating downwards gaze problems. the most useful visual signs in
most useful diagnostic clinical PSP patients may complain of dry eye identifying PSP. A diagnosis of
symptom of PSP. and artificial tears can be used to probable PSP is useful for the patientPSP
McCrary JA (1992) Neuro-ophthalmic
findings in progressive supranuclear
palsy. J Clin Neuro-ophthalmol 12:
104-109.
14. Rascol O, Sabatini U,
Simonettamoreau M, Montrastric JL,
Rascol A, Clanet M (1991) Square-
wave jerks in parkinsonism
syndromes. J Neurol Neurosurg
Psychiatr 54: 599-602.
15. Halliday GM, Hardman CD,
Cordato NJ, Hely MA, Morris JGL
(2000) A role for the substantia nigra
pars reticulata in the gaze palsy of
progressive supranuclear palsy. Brain
52 123: 724-732.
16. Revaud-Pechoux S, Vidailhet
23/03/07 PSP
M, Gallonedec G, Litvan I, Gaymard B,
Pierrot-Deseilligny C (2000)
Longitudinal ocular motor study in
corticobasal degeneration and
progressive supranuclear palsy. Neurol
54: 1029-1032.
Figure 3: Histological section of brain of a patient with progressive supranuclear palsy 17. Rottach KG, Riley DE,
showing 4R tau positive neurofibrillary tangles (NFT) DiScenna AO et al. Dynamic
properties of horizontal and vertical
eye movements in parkinsonian
because although drug therapy has mitochondrial genes from patients syndromes. Ann Neurol 39: 368-377.
been relatively unsuccessful, there are with progressive supranuclear palsy. J 18. Das VE, Leigh RJ (2000)
specific visual problems in PSP that Neurochem 75: 1681-1684. Visual-vestibular interaction in
need to be recognized and managed by 7. Grandas F, Esteban A (1994) progressive supranuclear palsy. Vision
the optometrist. Eyelid motor abnormalities in Res 40: 2077-2081.
progressive supranuclear palsy. J 19. Malessa S, Gaymard B,
Neurol Transm (Supp) 42: 33-41. Rivaud S, Cervera P, et al (1994) Role
8. Valls-Sole J, Valldeoriola F, of pontine nuclei damage in smooth-
References Tolosa E, Marti MJ (1997) Distinctive pursuit impairment of progressive
abnormalities of facial reflexes in supranuclear palsy: a clinico-
1. Steele JC, Richardson JC, patients with progressive supranuclear pathological study. Neurol 44: 716-
Olszewski T (1964) Progressive palsy. Brain 120: 1877-1883. 721.
supranuclear palsy. Arch Neurol 10: 9. Piccione F, Mancini E, Tonin 20. Rascol O, Sabatini U, fahre N,
333-359. P, Bizzarini M (1997) Botulinum toxin Senard JM et al. (1995) Abnormal
2. Nath U, Ben-Schlomo Y, treatment of apraxia of eyelid opening vestibulo-ocular cancellation in
Thompson RG et al. (2001) Clinical in progressive supranuclear palsy: multiple system atrophy and
features of progressive supranuclear report of two cases. Arch Phys Med progressive supranuclear palsy but not
palsy (PSP) in the UK. Neurol 56: Rehab 78: 525-529. in Parkinson’s disease. Movement
458. 10. Litvan I, FitzGibbon EJ (1996) Disord 10: 163-170.
3. Golbe LI, Davis PH, Can tropicamide eye drop response 21. Langheinrich T, van Elst LT,
Schoenberg BS et al. (1998) Prevalence differentiate patients with progressive Lagreze WA, Bach M et al. (2000)
and natural history of progressive supranuclear palsy and Alzheimer’s Visual contrast response functions in
supranuclear palsy. Neurol 38: 1031- disease from healthy control subjects? Parkinson’s disease: evidence from
1034. Neurol 47: 1324-1326. electroretinogram, visually evoked
4. Armstrong RA (1997) 11. Shinotoh H, Namba H, potentials and psychophysics. Clin
Parkinson’s disease and the eye. Yamaguchi M et al. (1999) Positron Neurophysiol 111: 66-74.
Ophthal Physiol Opt 17: S9-S16. emission tomographic measurement of 22. Armstrong RA (2003)
5. Stanford PM, Halliday GM, acetylcholinesterase activity reveals Dementia with Lewy bodies: A ‘new’
Brooks WS et al. (2000) Progressive differential loss of ascending type of dementia with visual
supranuclear palsy pathology caused cholinergic systems in Parkinson’s symptoms. OT Jan 10: 39-41.
by a novel silent mutation in exon 10 disease and progressive supranuclear 23. Averbach-Heller L, Paulson
of the tau gene: expansion of the palsy. Anns Neurol 46: 62-69. GW, Davoff RB, Leigh RJ (1999)
disease phenotype caused by the tau 12. Armstrong RA (1995) Whipple’s disease mimicking
gene mutations. Brain 123: 880-893. Alzheimer’s disease and vision: A progressive supranuclear palsy, the
6. Swerdlow RH, Golbe LI, proposed new diagnostic test. OT Jul diagnostic value of eye movement
Parks JK et al. (2000) Mitochondrial 17: 16-17. recording. J Neurol Neurosurg
dysfunction in cybrid lines expressing 13. Friedman DI, Jankovic J, Psychiatr 66: 532-535.You can also read

















































