Quality Account - April 2020 - March 2021 - Lincolnshire Community Health Services NHS Trust
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Lincolnshire Community
Health Services
NHS Trust
Quality Account
April 2020 - March 2021
Quality Account 2020/21 Contents Contents ........................................................................................................ 2 Part 1 Statements ......................................................................................... 3 Statement on 2020 / 2021 quality from the Chief Executive of Lincolnshire Community Health Services NHS Trust ..................................................... 3 2020/21 Statement of Directors’ responsibilities in respect of the Quality Account ......................................................................................................... 6 The LCHS Way .............................................................................................. 8 Part 2: Priorities for improvement .............................................................. 9 Looking back at our quality priorities 2020/2021 ...................................... 9 Looking forward to our Quality Account priorities for 2021/22 .............. 17 Statements of assurance from the board including core indicators ..... 26 Reporting against core indicators ............................................................ 37 Part 3: Review of quality performance ..................................................... 38 Care Quality Commission (CQC) .............................................................. 38 Evaluation of patient safety ....................................................................... 41 Evaluation of clinical effectiveness .......................................................... 48 Other quality developments ...................................................................... 58 Core Standards and Metrics ...................................................................... 60 Finance Metrics .......................................................................................... 61 Performance Metrics .................................................................................. 61 Appendix 1: Statements from NHS Lincolnshire Commissioning Group and Healthwatch Lincolnshire ....................................................... 67 Appendix 2: Local Clinical Audits 2020/21 ............................................... 72 Appendix: 4 National Clinical Audits 2019/20 .......................................... 74 Glossary:..................................................................................................... 75 Contact details ........................................................................................... 77 2
Quality Account 2020/21 Part 1 Statements Statement on 2020 / 2021 quality from the Chief Executive of Lincolnshire Community Health Services NHS Trust We are Lincolnshire Community Health Services NHS Trust (LCHS), the primary community healthcare provider in Lincolnshire delivering community-based services. We work in partnership with other health and social care services to care for thousands of patients across Lincolnshire every day delivering joined-up care in a range of community settings appropriate to the needs of the patient including: patients’ homes or a place of residence they call home, including nursing and care homes; GP surgeries; community clinics; hospices; homes providing community transitional care beds; community hospitals; and within acute hospital settings. This puts us at the heart of the Lincolnshire healthcare economy. LCHS has an annual turnover of c. £111m and employs c. 2,000 members of staff. Our mission is to provide outstanding community care. By providing services aimed at preventing health problems from getting worse, we help to support a shift from care in acute hospitals into more joined-up care close to the patient’s home. Patients are at the heart of everything we do, and it is important that they are involved not just in decisions about their care, but also in decisions that shape the current and future health services in Lincolnshire. The trust prides itself on delivering clinical practice that is safe for patients, effective in delivery and provides a great patient experience. This year the trust has been required to deliver services with agility and flexibility. Our services have been delivered differently; new pathways, new skills, new relationships and using technology to enable patient care. LCHS continues to measure the quality of its services through a series of metrics and quality improvements that are described in detail in this Quality Account. The year 2020/2021 will be one that, for many, will not be forgotten - living and working through the national pandemic of Covid19 has provided us all with a different experience. 3

Quality Account 2020/21 The trust has also worked hard to ensure we have the right staff with the right skills in place to support delivery of safe services – examples include volunteer teams supporting LCHS to ensure PPE and clinical sundries were available, increasing patient safety resources in the infection prevention team, temporary risk based approaches to ward staffing and the deployment of corporate services differently to release clinical capacity. With many of the clinical services needing to be restructured or delivered differently and done so at pace - this year our focus has been heavily invested in maintaining patient safety, continuing to deliver safe quality services and pay attention to the well-being of our most valuable asset – our staff. The publication of the National Staff Survey results provided us with continued positive feedback reflective of our strong organisational vision and values. The trust achieved the top score in health and wellbeing for community trusts nationally and also received the highest score for community trusts for ‘Quality of Care’, with more than 80 % of colleagues saying they are satisfied with the quality of care they are able to give. To continue to provide robust assurance on delivery of safe and quality services, the trust has designed and introduced interim governance frameworks; supporting the trust to continue to meet existing as well as new statutory and regulatory quality governance. Throughout the pandemic the trust’s Quality and Risk Committee has continued to keep a clear focus on both the delivery of services in line with the LCHS Clinical Strategy and meeting the pandemic priorities of patient safety. The delivery of our clinical services continues to be strongly driven through our LCHS Clinical Strategy which was developed through engagement with stakeholders including our clinical teams. The trust has, mid-way through the year, refreshed the Clinical strategy to reflect the changes which have been heightened as a result of the Covid-19 pandemic with the acceleration of digital solutions, addressing health inequalities and the health and wellbeing of our staff receiving further prominence. This year the Trust has continued to play a strong partner role in the county and has taken the opportunity to lead on many areas of transformation in the Lincolnshire health and care system. LCHS and system partners have worked together to deliver the Mass Vaccinations Centre (MVC) services for Lincolnshire to ensure the people of Lincolnshire receive timely access to vaccinations which has helped to maintain patient safety. The MVC programme exemplifies partnership working and we continue to work with our system partners, to deliver the programme and to work on planning for future vaccination programmes so that our population remains protected. 4

Quality Account 2020/21 LCHS holds an overall rating of outstanding from the CQC; with a rating of good for the safe, effective and caring domains and outstanding in the responsive and well- led domains. This rating is something that everyone who works for the trust is extremely proud of and as we recover from the pandemic and move into a Lincolnshire Integrated Care System where quality and safety governance will be assessed and assured on a system wide basis; LCHS will continue to work hard to improve quality for patients in partnership with them. Maz Fosh Chief Executive, Lincolnshire Community Health Services NHS Trust June 2021 5

Quality Account 2020/21
2020/21 Statement of Directors’ responsibilities in respect
of the Quality Account
The directors of the Trust are required under the Health Act 2009 and the National
Health Service (Quality Accounts) Regulations to prepare Quality Accounts for each
financial year. NHS Improvement guidance to NHS trust boards on the form and
content of the annual Quality Account incorporates the above legal requirements.
In the reporting period of this report April 2020 to March 2021 the nation has been
subject to a pandemic and as such variations in service as required to support health
and wellbeing of the population of Lincolnshire have required prioritisation.
In preparing the Quality Account, directors are required to take steps to satisfy
themselves that:
• The content of the Quality Account report meets the requirements set out in the
guidance
• That the report presents a balanced view of the Trusts quality related
performance
• The performance information reported in the Quality Report is reliable and
accurate
• There are proper internal controls over the collection and reporting of the
measures and these controls are subject to review to confirm that they are
working effectively in practice
• The data underpinning the measures of performance reported in the Quality
Account is robust and reliable, conforms to specified data quality standards
• The Quality Account report has been prepared in accordance with NHS
Improvement’s annual reporting manual and supporting guidance which
incorporates the Quality Accounts regulations
In preparing the Quality Account, directors are also required to satisfy themselves
that the content is consistent with internal and external sources of information
including:
• Board minutes and papers for the period April 2020 to March 2021
• The trust’s complaints report published under regulation 18 of the Local
Authority Social Services and NHS Complaints Regulations 2009
• The national staff survey 2020 / 2021
6
Quality Account 2020/21 • CQC Inspection reports for the period April 2020 to March 2021 During the reporting period, the production of some data sets to support the Quality Account report have been delayed by the work of the Trust to respond to the national pandemic of Covid-19. The directors confirm to the best of their knowledge and belief that they have complied with the above requirements in preparing the Quality Account. June 2021 Trust Board Chair June 2021 Chief Executive 7

Quality Account 2020/21 Our approach to care and working together is important to us. All our staff work in an ‘LCHS Way’. This reinforces the right behaviours and approach we take in everything we do, contributing to better care for patients and a better working environment in our Trust. We listen: we engage with everyone we work with | we are united | we are always positive We care: everyone is valued, respected and developed | knowledge and skills are nurtured | success is celebrated We act: Clear goals and the right resources | freedom coupled with accountability | emphasis on simplicity We Improve: we are creative, resourceful and innovative | integration & collaboration is the way forward | we’re always striving to do better 8
Quality Account 2020/21
Part 2: Priorities for improvement
Quality priorities support the Trust to grow, innovate and stretch in relation to patient
safety, experience and clinical effectiveness. This part of our Quality Account
demonstrates the trust’s achievements in respect of the quality account priorities we
agreed for 2020/21 and then outlines the quality account priorities for the coming
year of 2021/22.
Looking back at our quality priorities 2020/2021
The quality account priorities for 2020/21 were discussed with stakeholders including
staff groups and patients and were then agreed with the LCHS Quality and Risk
Committee and Trust Board.
The priorities were chosen in consideration of the national audit recommendations,
local prevalence and feedback from Lincolnshire Healthwatch and input from
Lincolnshire commissioners.
Delivery of the 3 quality priorities agreed for the year have been severely impacted
on as our response to the pandemic necessitated that we prioritise clinical delivery
and patient safety over the delivery of the quality account. Some progress has been
made and the section below describes what has been achieved. The priorities and
the achievement of them were:
QUALITY ACCOUNT PRIORITY DELIVERY
Priority 1: Safe
Improving management of patients identified as at risk of falls as an
inpatient
Priority 2: Effective
Development of individualised person-centred care and treatment plans
for all patients with diabetes for optimum health care planning and
including the promotion of self-care for patients with diabetes
Priority 3: Responsive
Improving our responsiveness to patients requiring or referred for
continence assessment including the appropriate identification of
patients requiring referral for continence specialist input
9
Quality Account 2020/21 Priority 1: Safe Improving management of patients identified as at risk of falls as an inpatient Senior Lead: Rachel Harvey, Physiotherapy Clinical Lead & falls group lead Why was this a quality priority? This was identified as a quality priority to support driving a review and update in the management of patient falls in our inpatient areas. High number of patients admitted to LCHS care are frail with increased risk of falls and the consequential harm that can occur. For many of our patients – they have fallen before in the community or other care settings and our care is focussed on achieving maximum rehabilitation goals and re-establishing patient confidence where possible before serious harm occurs. We are seeing an increase in frailty syndromes in our Lincolnshire population and we recognise that if we look at falls through a lens of frailty, we can influence improvements in outcomes and quality of life. How was the quality priority to be delivered? A programme of work aligned to and in consideration of best practice was to be developed; driven by a falls group and in consideration of NICE Guidance CG161. The work would consider the learning from our thematic review findings and clear changes made in terms of our planning, assessment, management, education, medication controls, safety monitoring and care. We agreed to do the work and make the changes in partnership with staff, patients, families and carers ensuring we asked them their views. Final evidence of success would be provided through audit – reducing incidence and harm whilst demonstrating increased patient outcomes. Has the priority been delivered? This priority has not been completed. The Trust established a falls group which set a programme of work and then soon after was stood down. The re-prioritisation of services required to provide care as part of the National level 4 NHS response to the pandemic were redirected. In the past months our hospitals have been required to provide care for patients outside of our usual rehabilitation criteria including those awaiting adult social care, patients unable to return home due to covid19 status risks, 10
Quality Account 2020/21 patients requiring a place of safety when care at home has broken down and patients admitted as alternative place of care to the acute trust. This priority has delivered some areas of improvement detailed below. Reducing the prevalence and impact of slips trips and falls will remain a key patient safety priority in 2021/22. What did the quality priority deliver? Towards the end of Quarter 4 this year and as part of our restoration – the falls group has been reconvened. A baseline assessment of our falls management has been undertaken and local policy and guidelines reviewed. An education programme that was developed and delivered only once (with great feedback) before we paused has now been restarted. Baseline audits of our falls screening, care planning and screening, education needs analysis and polypharmacy reviews have been completed and are now being analysed to influence the work programme. All wards have implemented lying and standing blood pressure recordings for all admissions as standard practice and when this is audited, we review our pathway of care relating to monitoring. Following assessment on admission to any ward, all patients are now immediately and consistently assessed for rehabilitation and reablement goals by a physiotherapist and/or occupational therapist and included in this assessment is suitability of mobility aids. This not only ensures the most appropriate mobility aid are used but that aids are constantly reviewed in a timely manner contributing to optimised rehabilitation. A safety programme to ensure patients are provided with appropriate footwear on admission when they don’t have it themselves has now been implemented across all four hospitals. A pathway to refer to patients for chiropody services has been established and referrals can be made to see patients at home or on the hospital ward; the pathway includes for more complex footcare needs, a referral to the Trust Podiatry service. The programme of work being reinstated will also be in consideration of clinical documentation – electronic care records and bedside. 11
Quality Account 2020/21 Priority 2: Effective Development of individualised person-centred care and treatment plans for all patients with diabetes for optimum health care planning and including the promotion of self-care for patients with diabetes Senior Lead: Karen Barton, Matron and Claire Griffiths Head of Clinical Services Why was this a quality priority? The number of people living with diabetes in the UK is over 4 million and in particular type 2 diabetes has been growing at an accelerated rate and is now one of the world’s most common long-term health conditions (Diabetes UK 2019). Diabetes prevalence in the UK is estimated to rise to 5 million by 2025. This priority is directly aligned to the local population reflecting the links to the high prevalence of diabetes within Lincolnshire and in particular the increasing levels of type 2 diabetes linked to wider healthcare conditions. Supporting patients in good self-management of their diabetes can improve their quality of life and reduce the risk of developing complications; it has been shown that supporting patients to care more for themselves can help to prevent hospital admissions and / or reduce length of stay. How was the quality priority to be delivered? The changes we planned to make involved the assessment of opportunity to move patients to become self-caring for their diabetes. Following assessment of suitability patients would then share in the development of more individualised person-centred care and treatment plans. The work was to be led by a team of clinicians including diabetes nurse specialists, district nurses and community teams working together to support patients differently. Our progress would be measured by audit and reviews on patient outcomes. Patient cohorts identified were to be assessed regarding their cognition, vision and dexterity and individualised care plans developed outlining targeted interventions and opportunities self-care. 12
Quality Account 2020/21 Has the priority been delivered? This priority has been delivered. A patient possible cohort across community teams was identified of 276 patients – currently on insulin and not self-caring. A target goal of 80% assessed for suitability of self-caring was agreed. In March 2021 audit data demonstrated 88.4% of patients (244 patients) requiring administration of insulin had an individualised care plan, developed with them. Quarter 3 audit data demonstrated that 38 patients were discharged completely to self-care. Friends and Family Testing for January 2021 scored 91% positive with a return rate of 11%. What did the quality priority deliver? The development of the plans included an assessment of dexterity, cognition and vision to understand all potential, barriers and support required to achieve a level of self-care. New Individualised care plans were developed with specific prompts to guide staff through introducing a process of self-care where clinically appropriate. Diabetes Specialist Nurses and community nurses have developed a “Shared Care Agreement” to complete with patients and families and carers to ensure partnership goals are agreed and understood. A specialised programme has been rolled out across community teams - “Diabetes in the Older Person” to increase core diabetes care skills within community teams which will be evaluated in the coming months. 13
Quality Account 2020/21 Priority 3: Responsive Improving our responsiveness to patients requiring or referred for continence assessment including the appropriate identification of patients requiring referral for continence specialist input Senior Lead: Bev Adams – Matron Community Nursing Sally Haire, Continence Lead Practitioner Why was this a quality priority? This quality priority sought to introduce a revised process for delivery of initial continence assessments, triage and visit allocation by health care support. The service the patients were receiving was not responsive or prioritised. How was the quality priority to be delivered? The changes would introduce waiting list reviews, triage of referrals, development of skills, allocation of dedicated resources with clinical specialist oversight. The new ways of working would seek to provide a timelier service with assessment and interventions including any product selection undertaken by an appropriately trained professional. Introduction of a triage pathway will ensure priority is given to individual patient need. The interdependencies with tissue viability management and the impact of poor continence management on skin integrity, mobility, and general wellbeing were recognised as areas of improved outcomes. The work would also inform future service developments for the Trust to better understand the future requirements of our patients and broaden the workforce skills and competencies for registered and non-registered staff. The quality priority was to be delivered in community nursing teams with suitably trained senior healthcare support workers, having received skills training and competencies in the appropriate triage of patients requiring continence assessment. Clinical oversight and guidance would be given by continence nurse specialists. 14
Quality Account 2020/21
Has the priority been delivered?
The priority has been delivered. A target of referral to treatment time of 6 weeks
was set at 75% - by December 77% of all referrals were seen by 6 weeks and by
March this had risen to 90% with a wait that is measured in days and not weeks.
Coinciding with this improvement the number of referrals is noted to have increased
month on month, making this improvement even more significant.
34 training sessions have been delivered providing training to 300 staff
Friends and family test results for the patients on continence caseloads has been
recorded as follows: -
Month Response % Score
rate
September 2020 7% 80%
October 2020 13% 75%
November 2020 15% 86%
December 2020 9% 80%
January 2021 25% 93%
15Quality Account 2020/21 What did the quality priority deliver? Introduction of a triage caseload management system which applies a RAG (RED, Amber, Green) associated with clinical assessment and complexity ensures priority is applied to patient needs Establishment of specialised caseloads with dedicated resources to ensure consistency in care and skills including continence champions in all teams Significantly improved responsiveness of service with positive patient feedback Detailed information on patient needs assessments Training has also been delivered across partner organisations including care homes, care agencies – initially face to face and then later in the pandemic on digital Microsoft teams. The training included bowel management, catheterisation and bladder ultrasound scanning. 34 training sessions were delivered with a total of 300 staff trained. Community Nursing teams are managing the continence caseloads in each area effectively with a clear focus on quality of care and response times to reduce risk of skin damage. Specialised product and assessment training across services Further work has been developed around the continence skills and competency framework aimed at staff during induction In 2021 the feedback and patient outcomes will be reviewed to inform the future service development. 16
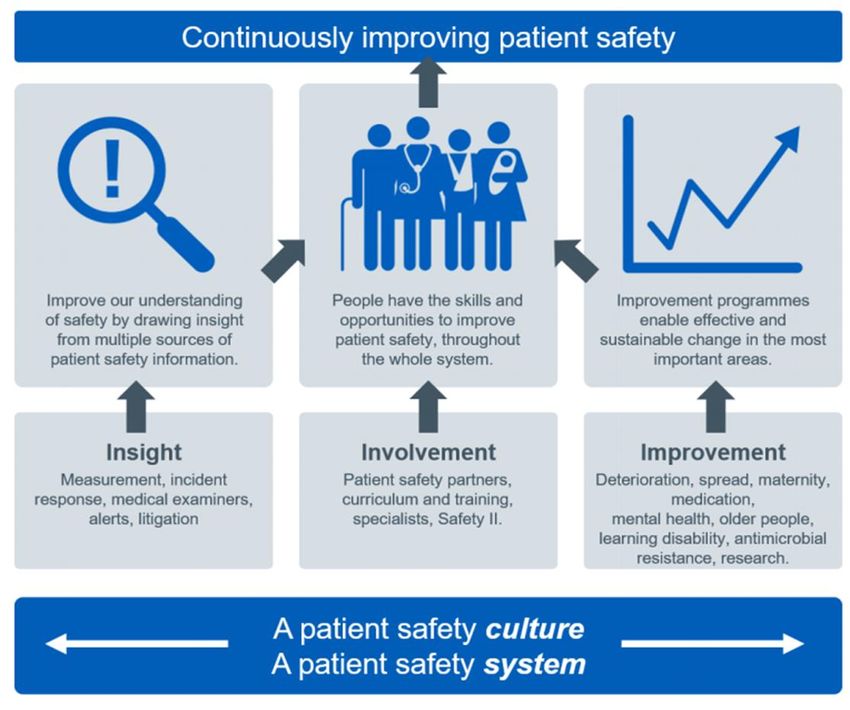
Quality Account 2020/21 Looking forward to our Quality Account priorities for 2021/22 The trust is continually striving to improve the quality of the services it provides and to learn from things that did not go so well. Following engagement with a range of stakeholders, including clinical and corporate staff, executives, non-executives, Clinical Commissioning groups and Lincolnshire Healthwatch - the LCHS Trust Board has agreed three new quality improvement priorities for 2021/22. The priorities have been developed linking closely with the trust’s strategic objectives, areas of improvement identified within the trust and the new National Patient Safety Strategy. The priorities are clinically driven and owned and align to the three quality domains of Patient Safety, Clinical Effectiveness and Patient Experience as well as three of the Care Quality Commission key lines of enquiry - Safe, Effective and Responsive. Progress against these priorities will be reported in the integrated performance report to the Quality and Risk Committee and the Trust Board. Priority 1: EFFECTIVE Patient involvement and patient partners Priority 2: SAFE Embed the principles of the safety culture (National Patient Safety Strategy) Priority 3: RESPONSIVE Personalised Care and Support Planning (PCSP) 17
Quality Account 2020/21
Priority 1: EFFECTIVE
Patient involvement and patient partners
Senior Leads:
Heather Emmerson – Stakeholder engagement manager
Sally Darley - Volunteer manager
Quality Assurance Managers
Service and team operation leaders with designated leads in each area
Why is this one of our priorities?
Immediately prior to the Covid19 pandemic the Trust articulated a programme of
work with a desire to improve and promote the patient voice and experience in
delivery of our services. The developments contributed to creating an environment
which improves the experiences of our patients, promotes listening and learning –
providing greater understanding of how patients feel about care locally.
Our key drivers are: -
✓ Ensuring patient public involvement is increased and is robust
✓ To ensure learning from Covid19 continues to be embedded to support patient
generated assurance and scrutiny to help shape future services
✓ Creating an environment in which the views of patients and the public are
maximised through increased opportunities
✓ Creating an environment in which the patient voice can directly influence future
developments and change the perspective of our learning
✓ Provide an opportunity for the trust to work towards understanding and
addressing local inequalities
How will the quality priority be delivered?
Changes we will make include the proactive recruitment of patients in a variety of
roles and functions to help to embed the patients voice in all aspects of service
delivery.
This quality account priority seeks to support delivery of the programme of the work
by applying a level of priority to reset and launch the patient voice work and will
support establishing the patient partner framework within the trust.
18Quality Account 2020/21 The programme of work is articulated in three levels of patient partner role and function. Level 1 - Panel member - receive regular information about the Trust, share their views via surveys Level 2 - Service specific interest group - established around specific service lines. Developed to work in partnership, to progress specific projects, share views via surveys or consultation. Level 3 – Patient partners - core group of trained panel members, who can take part in visits, sit on appropriate LCHS committee/meetings and participate on recruitment panels. How will the quality priority be measured? An implementation plan has been agreed including the identification of quarterly millstones which will be further reviewed and developed as the implementation progresses. Progress will be reviewed in local governance meetings and will be reported through the Stakeholder Engagement and Involvement Group (SEIG). A plan to include 2 measures has been agreed. 1st Measure: Patient Partners Q1: Review and collaboratively update the patient partner proposal baseline present position. Q2: Review support payment options in line with national guidance and system intentions. Develop patient partner role description Q3: Identify pilot patient partner area and recruit to pilot Q4: Evaluation of progress and pilot set recruitment trajectory for the organisation. 2nd Measure: Volunteer services Q1: Establish and recruit to Volunteering Services Manager Formal review and scoping of current volunteer roles and volunteer’s experiences Q2: Continued scoping exercise of current volunteer roles and experiences across the system including local population inequalities reviews Q3: Collaboratively develop volunteering role descriptions Q4: Roll out of volunteer recruitment to agreed areas 19
Quality Account 2020/21 Identify opportunities to enhance the patient and service experience through using an additional resource with a different skill set. Evidence of learning from the patient partners will be included in governance reporting including where they have influenced our understanding and views of our care delivery. Evidence of progress will include case studies to provide evidence of patient involvement which can be articulated through Quality & Risk feedback Andy and Wayne – two of our amazing volunteers during the Covid19 pandemic 20
Quality Account 2020/21 Priority 2: SAFE Embed the principles of the safety culture (National Patient Safety Strategy) Senior Leads: Lorna Adlington – Patient Safety Strategy lead Quality Assurance Managers Service and team operation leaders with designated leads in each area Why is this one of our priorities? Implementing this priority will ensure LCHS takes proactive steps to respond to the recommendations made within the National Patient Safety Strategy specifically the embedding of the concept of the ‘Just Culture Guide’ and appropriate investigation of patient safety incident investigation. The focus on the National Patient Safety Strategy formally adopted and then embedded trough a quality account priority programme will ensure the ‘Just Culture Guide’ is formally adopted and built into Trust policies enabling improvement in the quality of incident reporting as one of the principles of improving safety culture. The trust is keen to ensure staff are equipped to respond to patient safety incidents and to undertake patient safety incident investigation and that learning from safety incidents continue to shape future service provision. How will the quality priority be delivered? The National Patient Safety Strategy has been widely shared with clinical teams over the past months and a gap analysis will be included to refresh our current understanding on skills, capability, capacity within the organisation to assess Trust safety culture and deliver robust management of patient safety incident management and investigation. The Trust will adopt the NHS Improvement ‘Just Culture Guide’ and Human factors awareness. Investigation of incidents will be delivered under the new Patient Safety Incidences Response Framework (PSIRF). Training programmes adopting the framework applicable to all staff trust wide who are required to conduct incident investigation will be delivered. Trust wide awareness and stakeholder events will be planned and delivered. 21
Quality Account 2020/21 Implementation timescales are dependent on the release of national guidance and programmes but will broadly be as follows: - How will the quality priority be measured? Quarterly progress will be reported to the Clinical Safety and Effectiveness group and then to the Quality & Risk Committee. Baseline data will be established from safety culture questions within the 2020 NHS national staff survey results. Quarterly delivery plan: Q1: Embed ‘Just Culture Guide’ into Trust policy and process. Review existing investigation tools and modify to reflect shift in focus Q2: Completion of gap analysis for sharing and stakeholder engagement Q3/Q4: Development of plan for implementation of new Patient Safety Incidences Response Framework (PSIRF) Implementation and embedding of PSIRF from Q1 2022 to fit in with National rollout programme. This programme of work may be subject to update aligned to the new CQC strategy and the focus on learning from safety. 22
Quality Account 2020/21 Priority 3: RESPONSIVE Personalised Care and Support Planning (PCSP) Senior Leads: Liz Allen – Head of Clinical Services Claire Griffiths – Head of Clinical Services Tina Bramley – Head of Clinical Services Why is this one of our priorities? This priority will support the development of a clear vision and drive forward a consistent approach to Personalised Care and Support Planning (PCSP) across LCHS clinical services, aligned to and with all partners within the Lincolnshire health and care system. The development supports a consistent PCSP approach within LCHS; ensuring patient goals and plans are developed in line with what matters to patients and outcomes are maximised in line with the national personalisation agenda. Supporting patients through PCSPs also supports the trusted assessment principles of “do once and share’’, promotes the effectiveness of care by reducing duplication, maximising the plan for the patient and shared agreed outcomes and responsibilities for delivery of those outcomes. How will the quality priority be delivered? Personalised Care and Support Planning from an individual’s perspective is ‘’Health and social care workers being able to have ‘proactive conversations with ‘me’, the people who are important to me and the professional/s involved in my life. It asks what’s your story? The planning and the plan should be owned by me and shared with the right people. Where possible this should be held as a digital book with chapters that are unique to me.’’ Patient needs (“what matters to you”) are identified with the patient following an initial conversation and subsequent series of conversations in which the person whose plan is being discussed actively participates. The conversations recognise a person’s strengths and skills. Services ‘wrap around’ the patient to support the achievement of agreed outcomes including the development and use of 23
Quality Account 2020/21 standardised methods of patient reported evaluation. The plan is owned by the individual and is shared and contributed with and by the right people. The approach is underpinned by an agreed definition of personalised care and support planning, which follows the 6-stage approach outlined by NHSE The Trust will use an agreed PCSP approach and documentation, allowing for appropriate variation which is clinically determined We will ensure that PCSPs are developed with patients and that this information is shared as appropriate with system partners in the pathway to enable seamless care. The scope of the programme will be all patients within community nursing, community therapy, specialist and transitional care services. How will the quality priority be measured? A quarterly implementation plan has been agreed. Progress will be reviewed at local quality assurance groups and reported quarterly to the Clinical Safety and Effectiveness Group (CSEG). A plan to include 3 measures has been agreed. 1st Measure: PCSP implementation ✓ Baseline count of personalised care plans (person centred plan) in place 24
Quality Account 2020/21 2nd Measure: Patient voice Evidence on how patients are involved in the planning and evaluation of care (including evaluation tools as appropriate to service PROMs, TOMs, PAMs). ✓ Impact of PCSPs patient reported measure 3rd Measure: Information sharing LCHS approach developed in partnership with the wider system Personalisation Board. Patient story’s impact of joined up care, lessons learnt, and changes made. ✓ Evidence of information sharing - patient stories and lessons learnt 25
Quality Account 2020/21 Statements of assurance from the board including core indicators Care Quality Commission registration LCHS is registered with the Care Quality Commission and its current registration status is registered with no conditions attached. In September 2018 the trust was inspected by the Care Quality Commission and achieved a rating of ‘outstanding’ overall. The trust currently has 22 locations registered with the CQC and is registered to carry out the following regulated activities: • Diagnostic and screening procedures • Family planning services • Maternity and midwifery services • Nursing care • Personal care • Surgical procedures • Transport services, triage and medical advice provided remotely • Treatment of disease, disorder or injury The Care Quality Commission has taken no enforcement action against LCHS during 2020/2. All CQC inspection information about the trust can be found here: - http://www.cqc.org.uk/provider/RY5/registration-info National confidential enquiries None in 2020/21 Review of services During 2020/21 Lincolnshire Community Health Services NHS Trust provided and/or sub-contracted 122 relevant health services. Due to the Global COVID19 Pandemic some health services as per national guidance were paused and later restored. 26
Quality Account 2020/21
Lincolnshire Community Health Services NHS Trust has reviewed all the data
available to them on the quality of care in 122 of these relevant health services.
The income generated by the relevant health services reviewed in 2020/21
represents 100% of the total income generated from the provision of relevant health
services by Lincolnshire Community Health Services NHS Trust for 2020/21.
Payment by Results
Lincolnshire Community Health Services NHS Trust was not subject to the Payment
by Results (PbR) clinical coding audit during 2020/21 by NHS Improvement as no
services are commissioned on a PbR basis.
Participation in clinical audit
To ensure that the services provided by the trust achieve meaningful outcomes for
patients and carers, LCHS undertake a range of activities: clinical audit is one. The
organisation aims to participate in 4 levels of audit activity:
1. External must be done e.g. national audits (NCAPOP, NCEPOD), DH
statutory requirements such as infection control monitoring
2. Internal must be done e.g. complaints, re-audit, serious incidents
3. Organisational e.g. local topics important to the organisation
4. Clinician/professional interest e.g. educational audits
The focus is to ensure that all clinical audit activity results in learning and
improvements in care. Participation in clinical audit enables the trust to provide
effective, responsive and safe care and details of our participation is included in
Appendix 4 of this report.
Local Clinical Audits
On 30th January 2020, WHO declared the outbreak of COVID-19 a “Public Health
Emergency of International Concern” (PHEIC). In line with national guidance, all
research and audit plans and activities were placed on hold. During February 2020
preparedness for Covid 19 included safely concluding or pausing all audits.
Learning affecting required changes in practice following all incidents and issues has
continued to be embedded and assurance gathered through a robust yet flexible
quality governance framework.
27Quality Account 2020/21 Internal Audit Internal Audit have undertaken review and scrutiny in three areas – Effectiveness of the Transformation Delivery Group, medicines management and the Trust’s CQC preparedness. Trust Board Assurance Framework (BAF) and Risk Management – Significant assurance with some improvement required was achieved. Five minor recommendations have been made with one action for improvement, all of which were noted as low risk. The audit concluded the trust had a robust Risk Management Strategy in place which is supported by clearly defined operational procedures. Clear connection exists between the BAF and the Trust’s strategic objectives. Patient Experience - Internal Audit reviewed the LCHS Complaints process as a whole, selecting a number of completed complaint to assess. The IA team have confirmed a rating of significant assurance with some improvement required which, as stated by Grant Thornton Auditors, is a rare and very commendable achievement as only a handful of NHS Trusts have been awarded this rating of assurance. Three overall low risk recommendations have been noted and actions against which are already in progress. CQC preparedness – Significant assurance with some improvement required was achieved with three suggested areas for improvement of low risk for consideration. Overall, we have concluded that, the Trust has developed a robust governance structure to assist with the oversight and monitoring of its CQC compliance that is underpinned by an appropriate committee and meetings structure. The process provides the Trust Board with oversight of areas of risk and the actions being implemented and allows information to be disseminated from Board to senior clinical roles. Effectiveness of the Transformation Delivery Group - Significant assurance was achieved with three suggested areas for minor improvements for consideration. The audit noted that the work of the three strategic programmes has been well managed and has developed and delivered at pace. The TDG has been instrumental in the 28
Quality Account 2020/21 control and management of the work programmes operating within the fast changing and challenging environment the Trust has experienced due to the Covid19 pandemic. Medicines management - Partial assurance with improvement required. The audit overall concluded that, in the areas examined, there are some good controls and processes in place to manage medicines safely. However, whilst some areas were compliant with the Trust’s policies, in some areas the operational compliance was variable, and requires further improvement. The committee received a comprehensive improvement plan on actions Participation in clinical research 312 Lincolnshire patients were recruited to NHS National Institute for Health and Social Care Research (NIHR) portfolio research studies in 2020/21, 143 through Lincolnshire Community Health Services and 169 through NHS Lincolnshire Clinical Commissioning Groups. This recruitment included 3 Urgent Public Health (UPH) studies for Covid-19. NIHR took the decision early in the pandemic to pause many research studies so that trusts could focus on Covid-19 studies. The restart programme has now been initiated. The Lincolnshire Poacher study, which LCHS is sponsor for, opened and is recruiting from GP practices. This study is comparing usual patient care (following NICE guidance) and nurse-led clinics for patients with new irritable bowel syndrome (IBS). Lincolnshire Community Health Services, United Lincolnshire Hospitals Trust, Lincolnshire Partnership Trust and East Midlands Ambulance Service are working more collaboratively to enable Lincolnshire’s population to be involved in research studies that are linked to Lincolnshire’s needs. Proportion of income conditional to Commissioning for Quality and Innovation payments (CQUINs) As part of the emergency governance and financial arrangements for 2020/21, contract monitoring and incentive initiatives were suspended (and remain so) in order to allow NHS organisations to focus on responding to the emerging and 29
Quality Account 2020/21 ongoing issues relating to the Covid-19 pandemic. As such Commissioning for Quality and Innovation (CQUIN) initiatives and monitoring were not undertaken in 2020/21. Source: COVID-19-SOP-PHARM-PUBLICATION (england.nhs.uk) Secondary Uses Service for inclusion in the Hospital Episode Statistics Lincolnshire Community Health Services NHS Trust submitted records during 2020/21 to the Secondary Uses Service for inclusion in the Hospital Episode Statistics which are included in the latest published data. The percentage of records in the published data which included the patient’s valid NHS number was: • 100% for admitted patient care • 99% for accident and emergency care. Which included the patient’s valid General Medical Practice Code was: • 100% for admitted patient care; • 100% for accident and emergency care. Information Governance There were no Serious Incidents Requiring Investigation (SIRI) relating to Information Governance reported to the Information Commissioner’s Office (ICO) during 2020/21. The Information Governance Management Assurance Group (IGMAG) oversees all Information Governance (IG) and Data Protection (DP) issues and reports to the Finance, Performance and Investment Committee (FPIC) whilst also providing assurance to the Trust Board to ensure that statutory and regulatory requirements are met. The IGMAG is chaired by the Senior Information Risk Owner (SIRO), who is the Director of People and Innovation. The submission for the Data Security and Protection Toolkit (DSPT) was published 1st May 2020 with all standards met and gained ‘Significant Assurance with some improvement required’ from the Auditors. 30
Quality Account 2020/21
Actions to improve data quality
The Performance and Information team conduct regular data quality checks on
datasets and reports. They are also involved with national NHS Benchmarking work
which enables the Trust to benchmark its own data with that of other Trusts to
enable comparators and scope for improvement. The team works closely with the
Digital Health team to enable front-end changes to correlate into meaningful data
and analysis.
The Performance and Information team conduct regular data quality checks on
datasets and reports. They are also involved with national NHS Benchmarking work
which enables the Trust to benchmark its own data with that of other Trusts to
enable comparators and scope for improvement. The team works closely with the
Digital Health team to enable front-end changes to correlate into meaningful data
and analysis.
A Data Quality Group provides the Trust with assurance that the Trust’s data and
information, provided both internally and externally, is being carefully monitored and
that improvements are being identified and implemented where necessary. It also
enables the Trust to demonstrate its commitment to encouraging a culture of
continuous improvement and accountability. The Finance, Performance and
Investment Committee has oversight for the Data Quality Group and receives a
report from them every 6-8 weeks on data quality assurance. The report then goes to
the Trust Leadership Team and Trust Board meetings
Freedom to speak up
Our Freedom to Speak up Guardian (FTSUG) plays a lead role in engagement and
interaction with our staff. This role supports the organisation in complying with the
outcomes set up by the National Guardian Office and the outcomes include:
✓ A culture of speaking up being instilled throughout the organisation;
✓ Speaking up processes are effective and continuously improved;
✓ All staff have the capability to speak up effectively and managers have the
capability to support those who are speaking up;
✓ All staff are supported appropriately when they speak up or support other people
who are speaking up;
✓ The Board is fully sighted on, and engaged in, all Freedom to
31Quality Account 2020/21
✓ Speak Up matters and issues that are raised by people who are speaking up;
✓ Safety and quality are assured.
The 10 principles of the FTSUG role.
In October 2020 the National Guardian Office (NGO) published their index of the
Guardians. This uses the national staff survey to benchmark the ‘speak up’ culture
across the NHS and seeks to ensure that a culture of speaking up, listening and
openness is the way our business is conducted on a day to day basis.
Lincolnshire Community Health Services has scored 83.6% in this index. This places
LCHS high on the national list, with the highest scoring trust scoring 86.6%.
Scoping from several of the neighbouring and highest placed trusts has been
undertaken and reviewed noting:
✓ The visibility of our leaders and executive team is seen as a priority;
✓ Back to floor visits from senior leaders and executives are increasing;
✓ An ethos of compassionate leadership is embedded;
✓ Staff have the opportunity for informal discussions with leaders;
✓ We have a robust induction programme which includes meeting an executive
and hearing messages from the speak up guardian and staff side team;
✓ We have an active staff side
LCHS improved its scoring in the 4 Speak up questions to 85.5 % from 83.6% last
year – this was 5th highest in the country rankings. The national average is 79.2%
and the highest performing trust was 87.6%.
In response to the new question ‘’I feel safe to speak up about anything that
concerns me in the organisation’’ – measuring ‘strongly agree’ or ‘agree’ the Trust
scored 74.3% the highest being 78.3%, putting us just outside of the top 10. During
32Quality Account 2020/21 the pandemic we have used technology to ensure that staff continued to have good access to support, and that the guardian and other leaders were visible. The National Guardians Office has produced two e-learning modules Speak Up and Listen up which have been promoted in LCHS and are available to staff via the intranet. In 2020/21 there was a total of 60 concerns raised with the Freedom to Speak Up Guardian compared to 29 for 2019/20. The main reason for staff contacting the Guardian was noted to be staff seeking an independent view of a situation they find themselves in – often the support relates to helping them make decisions on next steps and actions on how to resolve a concern themselves. FTSUG champions have been established this year recruited from across the workforce, with a focus on those who may face additional barriers to speak up including those in learner/ student roles and the medical workforce. Learning from deaths During 2020/21,194 patients were recorded to have died in LCHS community hospitals at Louth, John Coupland Gainsborough, Skegness and Johnson Hospital Spalding and the Butterfly Hospice - noting the hospice was closed during Q1-Q3). The Trust participates and chairs a county wide learning from deaths panel meeting where all cases are subject to review using the following grading system. During the pandemic these panels continued with a core membership and were held virtually using technology. The core group membership consisted of the medical director, learning from deaths lead, safeguarding representative, deteriorating patient and resuscitation officer and associate Macmillan clinical nurse specialist. 33
Quality Account 2020/21
Any death which is assessed as falling into either grade 2 or 3 will then be
investigated further. The following table is the summary of the grading scores during
2020/21 by quarter.
Q1 Q2 Q3 Q4
47 Grade 0 43 Grade 0 48 Grade 0 45 Grade 0
2 Grade 1 2 Grade 1 4 Grade 1 3 Grade 1
All patient deaths that occurred within the 4 community hospitals and Butterfly
Hospice (once reopened) were reviewed and as of the end March 2021, 185 case
record reviews had been carried out in relation to the 194 deaths. In relation to some
of the deaths that occurred during March 2021, the information for these will be
reviewed in Q1 of 2021/22 (hence the difference in number of deaths that occurred
to number of deaths reviewed).
There were no instances where circumstances surrounding the patient death
suggested that any further investigation was required.
Equality, Diversity and Inclusion
Lincolnshire Community Health Services fully embraces Equality, Diversity and
Inclusion across all protected characteristics. The Trust has a range of policies and
procedures to support this. There are also legislative requirements that underpin the
Trust’s practice, policy and service developments. These are subject to regular
scrutiny in the governance framework of the Trust.
• During 2020, through the Covid-19 Pandemic, the Trust has had a number of
successes including publishing the Equality, Diversity and Inclusion Annual
Report as well as the delivery of the actions plans for the Workforce Race
34Quality Account 2020/21
Equality Standard (WRES), the Workforce Disability Equality Standard
(WDES), the Equality Delivery System (EDS) and the Gender Pay Gap in line
with the Public Sector Equality Duty (PSED).
• The Trust already had staff networks and during 2020 we increased the
opportunity of access. The Black, Asian, Minority and Ethnic (BAME) staff
network started weekly support meetings and the Mental and Physical Lived
Experience (MAPLE) staff network started a weekly support group aimed at
staff with disabilities and long- term conditions. The Lesbian, Gay, Bisexual
and Trans (LGBT) staff network has also seen an increased uptake from staff
accessing the network.
• Other support staff networks have emerged – the Faith and Belief Group,
Carers staff network, Women’s Group and Men’s Group.
• The BAME Staff Network has worked with the Trust Board who has supported
the BAME Chair to attend Trust Board as the BAME Board Advisor.
• The Trust implemented Risk Assessments to all staff, ensuring we understood
and responded to the support required by our BAME colleagues and those
colleagues with disabilities and long-term conditions.
• Lincolnshire Community Health Services has a diverse community of patients,
visitors and staff that come from Lincolnshire and the surrounding areas; our
strategy has been engaging with as many communities as we can, working
alongside or partners in both the private and public sector areas. During
2020, access has been limited, however, we have continued to engage with
local communities through using different technologies.
35Quality Account 2020/21
• The Trust has strong links nationally, working closely with NHS Employers
and NHS England and Innovation. This has been supported by technology,
accessing webinars and being involved in discussions both regionally and
nationally regarding disproportionate impacts of Covid-19 particularly on
BAME communities.
• The Trust, working as a system, has also continued to engage with staff
through 2020 and the impact Covid-19, celebrating LGBT History Month and
Black History month all through the medium of technology putting on a
successful raft of webinars with national and local speakers. These were well
attended across the three Lincolnshire Trusts. The webinars were also
recorded so if staff wanted to access them at a different time, they could.
• Within Lincolnshire our EDI team has had to work differently engaging with
the local food factories, of which 80% of their workforce are Eastern
European, holding ‘health days’ with the Tuberculosis team, Sexual Health
and Children’s Services. Due to Covid-19 access to the food factories had to
be put on hold. However, updates on the NHS Covid-19 and how to access
services were continued using technology to keep in touch, raise awareness
and supported in different languages.
36Quality Account 2020/21
Reporting against core indicators
All NHS trusts are required to report performance against a set of core indicators
using data made available to them by the Health and Social Care Information
Centre. Many of the core indicators are not relevant to community services; those
that are applicable to us at Lincolnshire Community Health Services NHS Trust are
shown in the information below.
Prescribed Information 18/19 19/20 20/21
The percentage of staff employed by, or under
contract to, the trust during the reporting period who
21. 85% 88% 89%
would recommend the trust as a provider of care to
their family or friends
The percentage of patients who were admitted to
23. hospital and who were risk assessed for venous
100% 99.14% N/A**
thromboembolism during the reporting period
The number and where available, rate of patient
25. safety incidents that occurred within the trust during 2474 2390 2490
the reporting period
The percentage of such patient safety incidents that
25. 0.04% 0% 0%
resulted in severe harm or death
** Paused and not recorded during the pandemic.
21. LCHS has taken consistent action to enhance our staff engagement programme,
supporting our people during the Covid-19 pandemic in many ways and details of
these can be found later in the account in the workforce and Covid19 sections.
25. The Trust has for many years been a high and consistently high reporter of
incidents indicative of a positive safety culture with harm related rates remaining
consistently low or absent.
37You can also read