Revision surgery following minimally invasive decompression for lumbar spinal stenosis with and without stable degenerative spondylolisthesis: a ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CLINICAL ARTICLE
Revision surgery following minimally invasive
decompression for lumbar spinal stenosis with and
without stable degenerative spondylolisthesis: a 5- to
15-year reoperation survival analysis
Nizar Moayeri, MD, PhD,1 and Y. Raja Rampersaud, MD, FRCSC2,3
1
Department of Neurology and Neurosurgery, University Medical Center Utrecht, The Netherlands; 2J. Bernard Gosevitz Chair
in Arthritis Research at UHN, Department of Orthopaedic Surgery, Toronto Western Hospital, Schroeder Arthritis Institute,
University Health Network (UHN), Toronto; and 3University of Toronto, Toronto, Ontario, Canada
OBJECTIVE Minimally invasive decompression (MID) is an effective procedure for lumbar spinal stenosis (LSS). Long-
term follow-up data on reoperation rates are lacking. The objective of this retrospective cohort study was to evaluate
reoperation rates in patients with LSS who underwent MID, stratified for degenerative lumbar spondylolisthesis (DLS),
with a follow-up between 5 and 15 years.
METHODS All consecutive patients with LSS who underwent MID between 2002 and 2011 were included. All patients
had neurogenic claudication from central and/or lateral recess stenosis, without or with up to 25% of slippage (grade I
spondylolisthesis), and no obvious dynamic instability on imaging (increase in spondylolisthesis by ≥ 5 mm demonstrated
on supine-to-standing or flexion-extension imaging). Reoperation rates defined as any operation on the same or adjacent
level were assessed. Revision decompression alone was considered if the aforementioned clinical and radiographic
criteria were met; otherwise, patients underwent a minimally invasive posterior fusion.
RESULTS A total of 246 patients (mean age 66 years) were included. Preoperative spondylolisthesis was present in
56.9%. The mean follow-up period was 8.2 years (range 5.0−14.9 years). The reoperation rates in patients with and
without spondylolisthesis were 15.7% and 15.1%, respectively; fusion was required in 7.1% and 7.5%, with no significant
difference (redecompression only, p = 0.954; fusion, p = 0.546). For decompression only, the mean times to reoperation
were 3.9 years (95% CI 1.8−6.0 years) for patients with DLS and 2.8 years (95% CI 1.3−4.2 years) for patients without
DLS; for fusion, the mean times to reoperation were 3.1 years (95% CI 1.0−5.3 years) and 3.1 years (95% CI 1.1−5.1
years), respectively.
CONCLUSIONS In highly selected patients with stable DLS and leg-dominant pain from central or lateral recess steno-
sis, the long-term reoperation rate is similar between DLS and non-DLS patients undergoing MIS decompression.
https://thejns.org/doi/abs/10.3171/2021.6.SPINE2144
KEYWORDS revision rates; minimally invasive; lumbar surgery
L
umbar spinal stenosis (LSS) is the most common lifestyle modification, and multidisciplinary rehabilitation,
indication for spinal surgery in people older than do not sufficiently address symptoms caused by neurogen-
65 years,1 with an estimated prevalence of 5.7% in ic claudication with varying degrees of back pain.7
the general population.2 It is often associated with multi- Both traditional open laminectomy and less-invasive
ple imaging findings, of which spondylolisthesis deserves techniques such as minimally invasive laminotomies have
special attention due to the ongoing debate about the need been shown to be effective for LSS decompression.8–10
for fusion.3 Depending on the clinical population, age, and However, conventional open laminectomies violate stabi-
screening method, degenerative lumbar spondylolisthesis lizing midline bony and ligamentous structures and may
(DLS) is seen in about 15% to 40% of patients with LSS.4–6 cause spondylolisthesis or exacerbate preexisting spondy-
Surgery is only warranted if adequate trials of nonsurgical lolisthesis.11,12 Minimally invasive decompression (MID)
care, such as medications, physiotherapy, spinal injections, through tubular or similar retractors is an alternative pro-
ABBREVIATIONS DLS = degenerative lumbar spondylolisthesis; LSS = lumbar spinal stenosis; MID = minimally invasive decompression.
SUBMITTED January 28, 2021. ACCEPTED June 18, 2021.
INCLUDE WHEN CITING Published online October 22, 2021; DOI: 10.3171/2021.6.SPINE2144.
© 2021 The authors, CC BY-NC-ND 4.0 (http://creativecommons.org/licenses/by-nc-nd/4.0/) J Neurosurg Spine October 22, 2021 1
Unauthenticated | Downloaded 11/30/21 03:18 AM UTC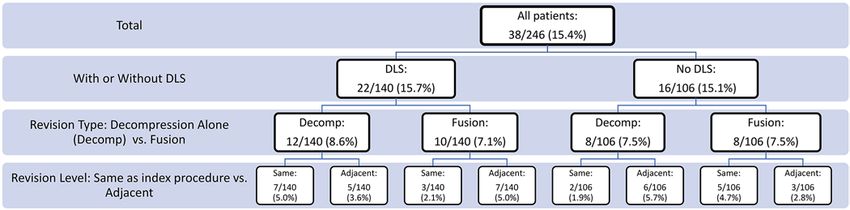
Moayeri and Rampersaud
cedure for decompression of LSS, which avoids detach- spinous process, which allowed us to partially remove the
ment of the paraspinal muscles and preserves posterior contralateral hypertrophied medial facet after flavectomy
stabilizing ligamentous and bony spinal structures,8,9,13–15 from within the spinal canal. If there was a clinical and
resulting in less postoperative instability as indicated by radiological predominant side for bilateral symptoms, the
biomechanical studies.16–19 incision was typically performed on the more dominant
Current recommendations on the surgical treatment side.
of degenerative spondylolisthesis include decompression If LSS was present at more than one level, we per-
and fusion.20,21 As demonstrated in the SPORT trial, de- formed the decompression at each level, sparing the lami-
compression and fusion remains the most commonly nae between. All operations were performed by a single
performed procedure in LSS with degenerative spondylo- experienced spine surgeon or under his direct supervision.
listhesis.22 More recent reports suggest similar functional Patients were typically discharged home on the same sur-
improvement and reoperation rates after MID in patients gical day (90%), except for patients with significant medi-
with LSS and DLS after short- to midterm follow-up.8,9,14,23 cal comorbidities requiring monitoring in the postopera-
However, long-term follow-up data are lacking. Therefore, tive phase.
we conducted a retrospective analysis of a prospectively
collected cohort to evaluate the long-term reoperation Follow-Up
rates in patients with and without low-grade stable de- To minimize the risk of missing data regarding any
generative spondylolisthesis and LSS who had undergone lumbar reoperation performed elsewhere, after our rou-
MID with a minimum 5-year follow-up. tine follow-up period of 5 years, we contacted all patients
and requested additional surgical and radiographic data
Methods in case they underwent reoperation elsewhere. Based on
Patient Selection the single-payer healthcare delivery model in Ontario
with associated limited access to spine surgeons, assess-
Institutional review board approval was obtained from ment by other surgeons is uncommon (i.e., patients are
the review board committee of the University Health Net- redirected back to their original surgeon because of long
work at Toronto Western Hospital, Toronto, Ontario, for respective waiting lists). Revision surgery was performed
subanalysis of a prospective cohort study. We retrospec- if significant pain or spine-related symptoms (e.g. sen-
tively reviewed all consecutive patients who underwent sorimotor claudication without pain) recurred from the
MID using tubular retractors for symptomatic LSS with decompressed lumbar level or adjacent level along with
or without degenerative spondylolisthesis grade 1 between evidence of continued lumbar stenosis on MRI or myelog-
2002 and 2011. Patients with a history of previous lumbar raphy with postmyelography CT scans during follow-up.
surgery were excluded. All patients presented with typical Revision decompression alone and/or adjacent-segment
neurogenic claudication signs and symptoms of LSS (e.g., decompression alone was considered using the same MID
significant leg-dominant pain related to standing or walk- technique if there was a leg-dominant symptom presenta-
ing that was relieved by postural change and/or rest) with tion and no radiological dynamic instability (as defined
no to tolerable mechanical low-back pain. LSS was radio- above) was shown; otherwise, patients underwent a mini-
graphically confirmed by MRI or myelography with post- mally invasive posterior instrumented fusion with transfo-
myelography CT scans when MRI was contraindicated. raminal interbody fusion and percutaneous pedicle screw
Patients underwent decompression alone if they had leg- instrumentation at revision.26
dominant symptoms as noted above, attributable to cen-
tral and/or lateral recess stenosis, with up to 25% of slip- Statistical Analysis
page (grade I spondylolisthesis) and no obvious dynamic
instability on imaging. Radiographic dynamic instability Revision rates were calculated for the entire group
was defined as an increase in spondylolisthesis by 5 mm and stratified for concomitant preoperative spondylolis-
or more demonstrated on supine to standing or flexion- thesis. Kaplan-Meier survival graphs for revision surgery
extension imaging as previously described.24,25 Patients (decompression alone with or without posterior fusion)
were calculated and plotted for patients with or without
with dominant leg symptoms consistent with the existing
spondylolisthesis. Possible risk factors based on patient’s
nerve root (confirmed by a selective nerve root block if
(baseline) characteristics for developing dynamic insta-
clinically unclear) of the surgical segment(s) with correla-
bility after the initial minimally invasive decompression,
tive foraminal stenosis underwent fusion with foraminal
including age, sex, BMI, level and segment(s) of lumbar
height distraction using a transforaminal interbody fusion
stenosis, and presence of degenerative spondylolisthesis,
technique.26 were assessed using uni- and multivariate logistic regres-
sion. All categorical variables were assessed using the chi-
Surgical Technique square test. Continuous variables were assessed using the
The minimally invasive procedure is described in de- independent t-test or Wilcoxon t-test; p < 0.05 was consid-
tail elsewhere.23 In brief, surgery was performed using an ered significant.
operating microscope and tubular retractor system (16 or
18 mm) through a 20-mm parasagittal longitudinal inci-
sion (MetRx, Medtronic). We performed a unilateral lami- Results
notomy for ipsilateral decompression, followed by medial Demographic Data
angulation of the tube and undercutting the base of the Between 2002 and 2011, all consecutive patients with
2 J Neurosurg Spine October 22, 2021
Unauthenticated | Downloaded 11/30/21 03:18 AM UTCMoayeri and Rampersaud
TABLE 1. Patient demographics stratified for preexisting DLS
with degenerative stenosis
w/o DLS w/ DLS p Value
No. of patients 106 (43.1) 140 (56.9)
Sex
Female 36 (14.6) 76 (30.9)
Male 70 (28.5) 64 (26.0)
Mean age ± SD, yrs 63.7 ± 11.1 68.0 ± 10.1 0.003
Mean BMI ± SD 29.1 ± 4.2 27.7 ± 4.2 0.084
FIG. 1. Flowchart of excluded and included consecutive patients. Mean baseline ODI 41 45 0.205
Mean baseline VAS leg 6.8 6.8 0.983
Mean baseline VAS back 6.0 6.1 0.634
LSS who underwent an MID for one or more lumbar lev- Level of decompression
els were included. The total number of consecutive pa- L2–3 3 4
tients along with the inclusion and exclusion criteria are
L3–4 22 21
shown in Fig. 1. A total of 246 patients, of whom 45.5%
were females, with a mean age of 66 years (20−88 years) L4–5 43 73
at the time of the initial surgery were included; 134 pa- L5–S1 2 1
tients (54.1%) were 65 years of age or older. The mean Combined 36 41
overall BMI was 28.3 ± 4.2 (range 20.7−41.4). Patients in No. of decompressed levels
DLS group were slightly older than those without DLS. 1 71 98
Table 1 summarizes patient demographics stratified for
2 27 31
DLS in the current series.
No significant difference was seen in the preoperative >2 8 11
Oswestry Disability Index or visual analog score for leg ODI = Oswestry Disability Index; VAS = visual analog scale.
and back pain between patients with and those without Values represent the number of patients (%) unless stated otherwise. Boldface
DLS (Table 1). Preoperative spondylolisthesis at the level type indicates statistical significance.
of spinal stenosis was present in 56.9% of patients. The
majority of patients (68.7%) underwent one-level decom-
pression, followed by 23.6%, 6.1%, and 1.6% for 2, 3, and
4 levels, respectively. The most common decompressed without DLS were 3.9 years (95% CI 1.8–6.0 years) and
level was L4–5 (47.2%), followed by L3–4 (17.5%), L2–3 2.8 years (95% CI 1.3−4.2 years), respectively, for decom-
(2.8%), L5–S1 (1.2%) and a combination of two or more pression only, and 3.1 years (95% CI 1.0−5.3 years) and 3.1
levels (31.3%). years (95% CI 1.1−5.1 years), respectively, for fusion. The
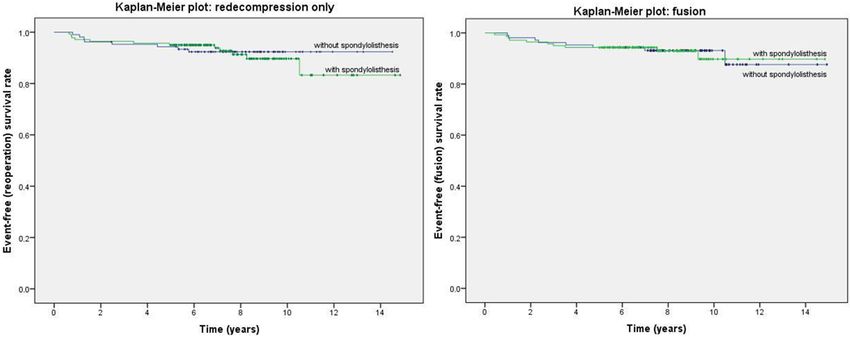
distribution of time to revision surgery (both decompres-
sion only and fusion) in patients with and without DLS did
Reoperation Rate not differ significantly (log-rank test, p < 0.318). Kaplan-
Of the 246 patients, 220 (89.4%) were available for long- Meier survival plots of the revision operation and rate
term follow-up assessment 5 to 14.9 years after surgery (decompression only or fusion) at the index or adjacent
(mean 8.2 years); 26 patients (10.6%) could not be reached level(s) are shown in Fig. 3.
after the 5-year follow-up and therefore their analyzed
follow-up period remained at 5 years. During this period,
38 patients underwent subsequent surgery, accounting for Discussion
an overall reoperation rate of 15.4%. After stratifying for Many studies have reported short- to moderate-term
DLS, the reoperation rates were 15.7% (22/140 patients) results of unilateral and bilateral laminotomy for decom-
and 15.1% (16/106 patients), respectively, for DLS and pression of LSS as a less-invasive surgical option. Our
non-DLS patients. Postoperative symptoms or instability current series is a 5- to 15-year survival analysis of reop-
not meeting the criteria noted above and thus requiring eration rates after minimally invasive lumbar decompres-
fusion was seen in 10 (7.1%) of 104 patients with DLS sion in patients with neurogenic claudication from central
and 8 (7.5%) of 106 patients without DLS. In both same- and/or lateral recess stenosis with and without stable (as
level and adjacent-level reoperations, DLS did not play a defined above: < 5 mm of motion) grade I degenerative
significant role as a risk factor for future reoperation, as spondylolisthesis. Overall, the long-term reoperation rate
shown in Fig. 2. In addition, except for a slightly overrep- at a mean of 8 years in this series was similar between
resentation of older patients in the DLS group, none of the those with (15.7%) and those without (15.1%) degenerative
baseline and surgical characteristics shown in Table 1 ap- spondylolisthesis. In addition, the type of revision (de-
peared to be significant as a risk factor for reoperation or compression alone vs decompression and fusion) was also
fusion. Due to the small number of revision cases for DLS similar between the groups. Surprisingly, progression of
and non-DLS patients, no meaningful predictive analysis spondylolisthesis after MID in patients with preexisting
could be conducted and is thus not reported. DLS necessitating a fusion at the same level as the index
The mean times to revision surgery in patients with and decompression procedure only occurred in 2.1% of DLS
J Neurosurg Spine October 22, 2021 3
Unauthenticated | Downloaded 11/30/21 03:18 AM UTCMoayeri and Rampersaud
FIG. 2. Distribution of all patients who underwent surgery stratified for DLS, decompression alone, and fusion. Based on the
criteria requiring a fusion (see Follow-Up in Methods), if there was a need for reoperation attributed to the adjacent level and a
fusion was required, the previously decompressed level with or without DLS was included in the fusion. Figure is available in color
patients. Same-level reoperations were performed in 6.9% ies are likely more representative of the natural history of
of all patients, more than half (56.9%) of whom had DLS. LSS (i.e., spine osteoarthritis).
The mean time for reoperation surgery (decompression In our series, the reoperation (decompression alone) rate
only or with fusion) was 3.1 years for both groups. at the same level as the index procedure was 3.7% (9/246),
In the present series, the 15.4% incidence of overall regardless of the presence of DLS. This is generally simi-
surgery-related reoperation for clinically significant reste- lar to or lower than most rates reported for minimally in-
nosis at the operated levels, progressive stenosis at adja- vasive tubular retractor laminectomy in the literature, with
cent segment(s), or spinal instability (de novo or second- a mean reoperation rate of 8.1% (range 1.2%–15%) and
ary) falls within the range of incidences reported in the mean follow-up period of 25 months (range 9–42 months),
literature (10% to 23%) for decompression with or without as shown in Table 2.8,9,13,15,23 An overall explanation could
fusion in patients with LSS, with follow-up between 3 and be better preservation of the spinal integrity (bony and soft
10 years.11,27–30 It has been stipulated that factors such as tissue) with the unilateral laminotomy for bilateral decom-
laminar bone regrowth and progressive mechanical dis- pression, with minimal postoperative bone regrowth.32 As
ruption of the lumbar spine integrity and postoperative a progressive degenerative disease, LSS often affects the
instability could contribute to the failure in long-term entire lumbar spine, with degenerative changes still pres-
follow-up.31 Bone regrowth in a surgical defect after pos- ent after decompressive surgery. This may explain the
terior decompression in LSS has been reported to occur in long-term reoperation rate of 8.5% for stenosis and/or
44% to 94% of patients.31,32 In this series, we also included lumbar disc herniation of segments other than those that
adjacent-segment reoperations (8.5%) as part of the over- were surgically treated in the current series. Stenosis and
all reoperation rate to account for the patient’s perspective. disc herniation at adjacent levels might occur irrespective
However, in the absence of a fusion and with an anatomy of the selected operative technique for decompression of
preserving decompression alone, these additional surger- LSS. However, it is known that fusion of one or more seg-
FIG. 3. Kaplan-Meier survival plots of the revision operation and rate stratified for re-decompression only (left) or fusion (right).
Figure is available in color online only.
4 J Neurosurg Spine October 22, 2021
Unauthenticated | Downloaded 11/30/21 03:18 AM UTCMoayeri and Rampersaud
TABLE 2. Comparison of reoperation rates (decompression the criteria noted in the study by Ghogawala et al.38 In
only or fusion) in minimally invasive tubular decompression, as their study, all patients with grade I lumbar spondylolis-
reported in the literature thesis (degree of spondylolisthesis, 3 to 14 mm) with lum-
No. of FU Total Reop Reop w/ bar stenosis and neurogenic claudication with or without
Authors & Year Cases Duration Rate Fusion Rate lumbar radiculopathy were eligible for inclusion. Patients
were excluded “if radiography revealed lumbar instability
Parikh et al., 200815 60 9 mos 3.4% NA (motion of >3 mm at the level of listhesis, as measured
Kim et al., 20128 57 42 mos 15% 7% on flexion–extension radiographs of the lumbar spine), if
Müslüman et al., 20129 84 24 mos 1.2% 0% they were judged by the enrolling surgeon to have lumbar
Palmer & Davison, 201213 54 27 mos NA 2% instability because of a history of mechanical low back
Alimi et al., 201523 84 28 mos 12.9% 3.5%
pain with axial loading of the spine, if they had had previ-
ous lumbar spinal surgery….”38 In the study by Försth et
FU = follow-up; NA = not applicable. al., patients with “pseudoclaudication in one or both legs
and back pain (score on visual-analogue scale >30)” and
a minimum of 3 mm of listhesis were included.37 These
ments could change the biomechanics of the adjacent lev- patients are likely more heterogeneous than those enrolled
els and cause accelerated degeneration. However, the clin- in the study by Ghogawala et al. or the current series. With
ical significance and whether this would result in higher the specific patient and radiographic selection criteria out-
number of reoperations remains to be elucidated. lined, our long-term results suggest that a durable outcome
Revision surgery with spinal fusion for primary con- as it relates to reoperation is feasible after decompression
cerns at the same level as the index procedure was nec- alone for selected DLS patients. In particular, a midline
essary in 3.3% of all patients in the present series (2.1% preserving approach to decompression may further reduce
and 4.7% in DLS and non-DLS patients, respectively). the reoperation rates in decompression alone and provide
There was no increased significant difference in rate of further evidence of noninferiority of decompression alone
fusion between patients with preexisting DLS and those for appropriately selected patients. To establish this propo-
without. Our data are comparable with reoperation fusion sition in a higher level of evidence, a pragmatic random-
rates reported in the literature, with a mean rate of 3.1% ized multicenter controlled trial is currently being led by
(range 0%–7%) and mean follow-up period of 30 months the senior author in Canada (https://clinicaltrials.gov/ct2/
(range 24–42 months).8,9,13,23 In patients without preopera- show/NCT02348645).
tive spondylolisthesis, rates of progressive postoperative Our results present the longest follow-up interval of
spondylolisthesis up to 31% and for those with a preop- LSS patients stratified for DLS treated with MID. Persis-
erative listhesis up to 100% (30%–100%) have been re- tent inclusion criteria, clinical homogeneity of the patient
ported.11,33–35 Therefore, a substantially higher incidence of population, reliability and consistency of MID surgical
postoperative spinal instability and associated reoperation technique (performed or supervised by one single spine
rate (range 7%–24%) has been reported in laminectomy surgeon), together with clear and reproducible outcome
and bilateral laminotomy series for both DLS and non- criteria, reflect the strength of the present study. However,
DLS patients.11,27,30,34,36 these strengths also negatively affect the study’s generaliz-
It must be noted that reoperation is not a binary deci- ability and limit its reproducibility, especially in a setting
sion based on presence or absence of postoperative insta- where one single spine surgeon was involved. Addition-
bility. This is reflected in the wide variation of reported ally, as is the case for every retrospective analysis, there is
reoperation rates that reflects the reality that reoperation an inherent risk of recall, misclassification, and informa-
rates will be driven by three key factors: patient factors tion bias. Loss to follow-up might bias the clinical results;
(e.g., symptoms and choice), surgeon factors (e.g., radio- however, the follow-up rate in this series was almost 90%.
graphic, clinical, and surgical technique), and regional Moreover, relying on dynamic radiological imaging to as-
health system factors (e.g., limited resources vs incentives sess spinal instability might underestimate actual preop-
to perform more surgery). For example, in the two recent erative instability and failure to assess postoperative sur-
decompression versus decompression and fusion trials gery-induced spinal instability. As has been stipulated in
for DLS, the reoperation rate (mean 6.5 years) reported the literature, the degree of radiologically confirmed de-
by Försth et al. in Sweden was 21% for decompression compression and evidence of instability are poorly related
alone compared with 22% for decompression and fusion, to the surgical outcome.11,37–39 Moreover, we did not assess
whereas the reoperation rate at 4 years in the US series for one or more radiological parameters that may have sig-
by Ghogawala et al. was 34% for decompression alone nificant effect to the need of fusion in the future (such as,
compared with 14% for fusion.37,38 In both series, lami- but not limited to, pelvic parameters, regional and global
nectomies were used for decompression. Thus, it is pos- sagittal alignment, disc height, facet angle, or specific dis-
sible that the lower rate of reoperation in the current se- tance of slippage). For the purpose of this particular study,
ries was related to the use of the midline-preserving MID we excluded these parameters because we only aimed to
technique. However, differences in patient selection and study the effect of spondylolisthesis in this heterogeneous
surgeon and system biases are also likely contributory. In cohort in combination with the MID, which we believe
the current series, a single surgeon’s criteria (see Methods) has little effect on the general biomechanical status of the
were used to select patients for decompression alone in lumbar region. Furthermore, these specific radiographic
DLS patients. Comparatively, these criteria are closest to parameters, although clinically considered by the senior
J Neurosurg Spine October 22, 2021 5
Unauthenticated | Downloaded 11/30/21 03:18 AM UTCMoayeri and Rampersaud
author, are not used above and beyond the criteria outlined 14. Pao JL, Chen WC, Chen PQ. Clinical outcomes of microen-
in Methods for decision-making to consider decompres- doscopic decompressive laminotomy for degenerative lumbar
sion alone in the DLS patients. Nonetheless, in a separate spinal stenosis. Eur Spine J. 2009;18(5):672-678.
study in a small series of more recent DLS patients, the 15. Parikh K, Tomasino A, Knopman J, Boockvar J, Härtl R.
Operative results and learning curve:microscope-assisted
senior author has assessed the correlation to progression tubular microsurgery for 1- and 2-level discectomies and
of radiographic slip and Oswestry Disability Index after laminectomies. Neurosurg Focus. 2008;25(2):E14.
decompression alone. In that study, the mean baseline slip 16. Abumi K, Panjabi MM, Kramer KM, Duranceau J, Oxland T,
was 17.2% (SD 8%) in patients undergoing surgery with Crisco JJ. Biomechanical evaluation of lumbar spinal stabil-
the same selection criteria as in the current article.39 ity after graded facetectomies. Spine (Phila Pa 1976). 1990;
15(11):1142-1147.
17. Cardoso MJ, Dmitriev AE, Helgeson M, Lehman RA, Kuklo
Conclusions TR, Rosner MK. Does superior-segment facet violation or
In highly selected patients with stable DLS and leg- laminectomy destabilize the adjacent level in lumbar trans-
dominant pain due to central or lateral recess stenosis, the pedicular fixation? An in vitro human cadaveric assessment.
long-term reoperation rate is similar between DLS and Spine (Phila Pa 1976). 2008;33(26):2868-2873.
18. Delank KS, Gercek E, Kuhn S, Hartmann F, Hely H, Rölling-
non-DLS patients undergoing MID. hoff M, et al. How does spinal canal decompression and dor-
sal stabilization affect segmental mobility? A biomechanical
References study. Arch Orthop Trauma Surg. 2010;130(2):285-292.
19. Hamasaki T, Tanaka N, Kim J, Okada M, Ochi M, Hut-
1. Deyo RA. Treatment of lumbar spinal stenosis:a balancing
ton WC. Biomechanical assessment of minimally invasive
act. Spine J. 2010;10(7):625-627.
decompression for lumbar spinal canal stenosis:a cadaver
2. Yabuki S, Fukumori N, Takegami M, Onishi Y, Otani K,
study. J Spinal Disord Tech. 2009;22(7):486-491.
Sekiguchi M, et al. Prevalence of lumbar spinal stenosis,
20. Herkowitz HN, Kurz LT. Degenerative lumbar spondylolis-
using the diagnostic support tool, and correlated factors in
thesis with spinal stenosis. A prospective study comparing
Japan:a population-based study. J Orthop Sci. 2013;18(6):
893-900. decompression with decompression and intertransverse pro-
3. Lurie J, Tomkins-Lane C. Management of lumbar spinal cess arthrodesis. J Bone Joint Surg Am. 1991;73(6):802-808.
stenosis. BMJ. 2016;352:h6234. 21. Kreiner DS, Shaffer WO, Baisden JL, Gilbert TJ, Summers
4. Ishimoto Y, Yoshimura N, Muraki S, Yamada H, Nagata K, JT, Toton JF, et al. An evidence-based clinical guideline for
Hashizume H, et al. Association of lumbar spondylolisthesis the diagnosis and treatment of degenerative lumbar spinal
with low back pain and symptomatic lumbar spinal stenosis stenosis (update). Spine J. 2013;13(7):734-743.
in a population-based cohort:the Wakayama Spine Study. 22. Weinstein JN, Lurie JD, Tosteson TD, Hanscom B, Tosteson
Spine (Phila Pa 1976). 2017;42(11):E666-E671. AN, Blood EA, et al. Surgical versus nonsurgical treatment
5. Ong KL, Auerbach JD, Lau E, Schmier J, Ochoa JA. Periop- for lumbar degenerative spondylolisthesis. N Engl J Med.
erative outcomes, complications, and costs associated with 2007;356(22):2257-2270.
lumbar spinal fusion in older patients with spinal stenosis and 23. Alimi M, Hofstetter CP, Pyo SY, Paulo D, Härtl R. Minimal-
spondylolisthesis. Neurosurg Focus. 2014;36(6):E5. ly invasive laminectomy for lumbar spinal stenosis in patients
6. Segebarth B, Kurd MF, Haug PH, Davis R. Routine up- with and without preoperative spondylolisthesis:clinical out-
right imaging for evaluating degenerative lumbar stenosis: come and reoperation rates. J Neurosurg Spine. 2015;22(4):
incidence of degenerative spondylolisthesis missed on supine 339-352.
MRI. J Spinal Disord Tech. 2015;28(10):394-397. 24. Kelleher MO, Timlin M, Persaud O, Rampersaud YR. Suc-
7. Sengupta DK, Herkowitz HN. Lumbar spinal stenosis. Treat- cess and failure of minimally invasive decompression for
ment strategies and indications for surgery. Orthop Clin focal lumbar spinal stenosis in patients with and without
North Am. 2003;34(2):281-295. deformity. Spine (Phila Pa 1976). 2010;35(19):E981-E987.
8. Kim S, Mortaz Hedjri S, Coyte PC, Rampersaud YR. Cost- 25. Simmonds AM, Rampersaud YR, Dvorak MF, Dea N,
utility of lumbar decompression with or without fusion for Melnyk AD, Fisher CG. Defining the inherent stability of
patients with symptomatic degenerative lumbar spondylolis- degenerative spondylolisthesis:a systematic review. J Neuro-
thesis. Spine J. 2012;12(1):44-54. surg Spine. 2015;23(2):178-189.
9. Müslüman AM, Cansever T, Yılmaz A, Çavuşoğlu H, Yüce 26. Aleem IS, Rampersaud YR. Elderly patients have similar
İ, Aydın Y. Midterm outcome after a microsurgical unilateral outcomes compared to younger patients after minimally
approach for bilateral decompression of lumbar degenerative invasive surgery for spinal stenosis. Clin Orthop Relat Res.
spondylolisthesis. J Neurosurg Spine. 2012;16(1):68-76. 2014;472(6):1824-1830.
10. Slätis P, Malmivaara A, Heliövaara M, Sainio P, Herno A, 27. Rompe JD, Eysel P, Zöllner J, Nafe B, Heine J. Degenerative
Kankare J, et al. Long-term results of surgery for lumbar spi- lumbar spinal stenosis. Long-term results after undercutting
nal stenosis:a randomised controlled trial. Eur Spine J. 2011; decompression compared with decompressive laminectomy
20(7):1174-1181. alone or with instrumented fusion. Neurosurg Rev. 1999;
11. Fox MW, Onofrio BM, Onofrio BM, Hanssen AD. Clinical 22(2-3):102-106.
outcomes and radiological instability following decompres- 28. Tsai RY, Yang RS, Bray RS Jr. Microscopic laminotomies for
sive lumbar laminectomy for degenerative spinal stenosis:a degenerative lumbar spinal stenosis. J Spinal Disord. 1998;
comparison of patients undergoing concomitant arthrodesis 11(5):389-394.
versus decompression alone. J Neurosurg. 1996;85(5):793- 29. Tuite GF, Stern JD, Doran SE, Papadopoulos SM, McGil-
802. licuddy JE, Oyedijo DI, et al. Outcome after laminectomy for
12. Mardjetko SM, Connolly PJ, Shott S. Degenerative lumbar lumbar spinal stenosis. Part I:Clinical correlations. J Neuro-
spondylolisthesis. A meta-analysis of literature 1970-1993. surg. 1994;81(5):699-706.
Spine (Phila Pa 1976). 1994;19(20)(suppl):2256S-2265S. 30. Javid MJ, Hadar EJ. Long-term follow-up review of patients
13. Palmer S, Davison L. Minimally invasive surgical treatment who underwent laminectomy for lumbar stenosis:a prospec-
of lumbar spinal stenosis:two-year follow-up in 54 patients. tive study. J Neurosurg. 1998;89(1):1-7.
Surg Neurol Int. 2012;3:41. 31. Postacchini F, Cinotti G. Bone regrowth after surgical de-
6 J Neurosurg Spine October 22, 2021
Unauthenticated | Downloaded 11/30/21 03:18 AM UTCMoayeri and Rampersaud
compression for lumbar spinal stenosis. J Bone Joint Surg Br. 39. Ravinsky RA, Crawford EJ, Reda LA, Rampersaud YR.
1992;74(6):862-869. Slip progression in degenerative lumbar spondylolisthesis
32. Chen Q, Baba H, Kamitani K, Furusawa N, Imura S. Postop- following minimally invasive decompression surgery is not
erative bone re-growth in lumbar spinal stenosis. A multi- associated with increased functional disability. Eur Spine J.
variate analysis of 48 patients. Spine (Phila Pa 1976). 1994; 2020;29(4):896-903.
19(19):2144-2149.
33. Jönsson B. Vertebral slipping after decompression for spinal
stenosis. Acta Orthop Scand Suppl. 1993;251:76-77. Disclosures
34. Nakai O, Ookawa A, Yamaura I. Long-term roentgenograph- Dr. Rampersaud: consultant and royalties from Medtronic.
ic and functional changes in patients who were treated with
wide fenestration for central lumbar stenosis. J Bone Joint Author Contributions
Surg Am. 1991;73(8):1184-1191.
35. Thomas NW, Rea GL, Pikul BK, Mervis LJ, Irsik R, Mc- Conception and design: both authors. Acquisition of data: both
Gregor JM. Quantitative outcome and radiographic compari- authors. Analysis and interpretation of data: both authors.
sons between laminectomy and laminotomy in the treatment Drafting the article: Moayeri. Critically revising the article:
of acquired lumbar stenosis. Neurosurgery. 1997;41(3):567- both authors. Reviewed submitted version of manuscript: both
575. authors. Approved the final version of the manuscript on behalf
36. Katz JN, Lipson SJ, Chang LC, Levine SA, Fossel AH, Liang of both authors: Rampersaud. Statistical analysis: Moayeri.
MH. Seven- to 10-year outcome of decompressive surgery for Administrative/technical/material support: Rampersaud. Study
degenerative lumbar spinal stenosis. Spine (Phila Pa 1976). supervision: Rampersaud.
1996;21(1):92-98.
37. Försth P, Ólafsson G, Carlsson T, Frost A, Borgström F, Frit- Correspondence
zell P, et al. A randomized, controlled trial of fusion surgery Y. Raja Rampersaud: Toronto Western Hospital, University Health
for lumbar spinal stenosis. N Engl J Med. 2016;374(15):1413- Network, Toronto, ON, Canada. raja.rampersaud@uhn.ca.
1423.
38. Ghogawala Z, Dziura J, Butler WE, Dai F, Terrin N, Magge
SN, et al. Laminectomy plus fusion versus laminectomy
alone for lumbar spondylolisthesis. N Engl J Med. 2016;
374(15):1424-1434.
J Neurosurg Spine October 22, 2021 7
Unauthenticated | Downloaded 11/30/21 03:18 AM UTCYou can also read

















































