SARS-COV2 - TEST, TEST, TEST BUT HOW, WHO, AND WHEN? - CLAUDIA DENKINGER DIVISION CLINICAL TROPICAL MEDICINE, UNIVERSITY HOSPITAL HEIDELBERG ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
SARS-CoV2 - Test, test, test… but how, who, and when? Claudia Denkinger Division Clinical Tropical Medicine, University Hospital Heidelberg Heidelberg July 2020
Content • SARS-CoV2 - Test, test, test… but how, who, and when? – Why do we test – What are available tests and How do we test – Who and When to test
Test, test, test……… https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19--- 16-march-2020
What do we want to test for? – Use Cases • Am I infected? - Triage, Diagnosis • Was I infected? - Exposure • How many people have been infected? - Exposure • How many people are infected? – Population surveillance • Am I immune? - Immunity

WHAT ARE AVAILABLE TESTS
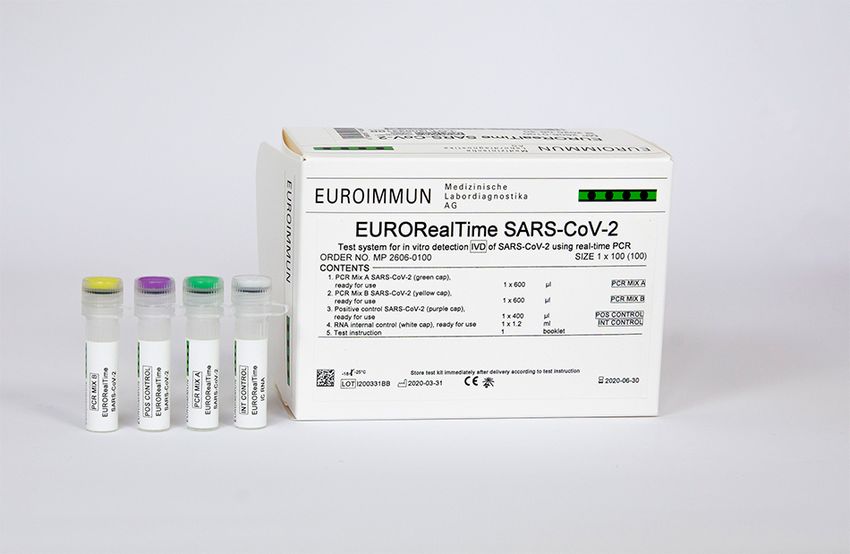
Tests for Diagnosis – PCR
• Nucleic acid tests, the current gold standard for
direct detection of SARS-CoV2
• Characteristics: Abbott
– highly specific
– sensitivity may be affected Molbio
• by falling viral-load after symptom-onset;
• initial infectious dose of virus;
• a difficult & uncomfortable sampling method
• Other: Isothermal, Sequencing Cepheid
https://www.medrxiv.org/content/10.1101/2020.04.24.20078949v1.full.pdf
https://pubmed.ncbi.nlm.nih.gov/32358057/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7185831/
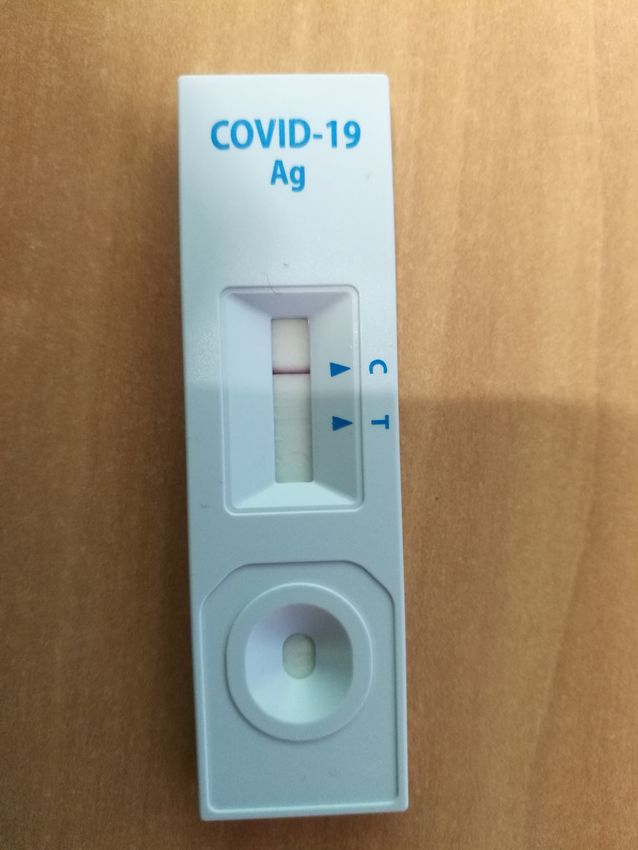
Tests for Diagnosis/Triage – Antigen Tests
• Antigen tests, directly detect virus
• ~10 commerically available
• Mind. 1 FDA approved (Quidel)
Rapigen
• Variable sensitivity: 60-80% and
specificity
• Ongoing study in Heidelberg, SD Biosensor
Berlin, Liverpool
Quidel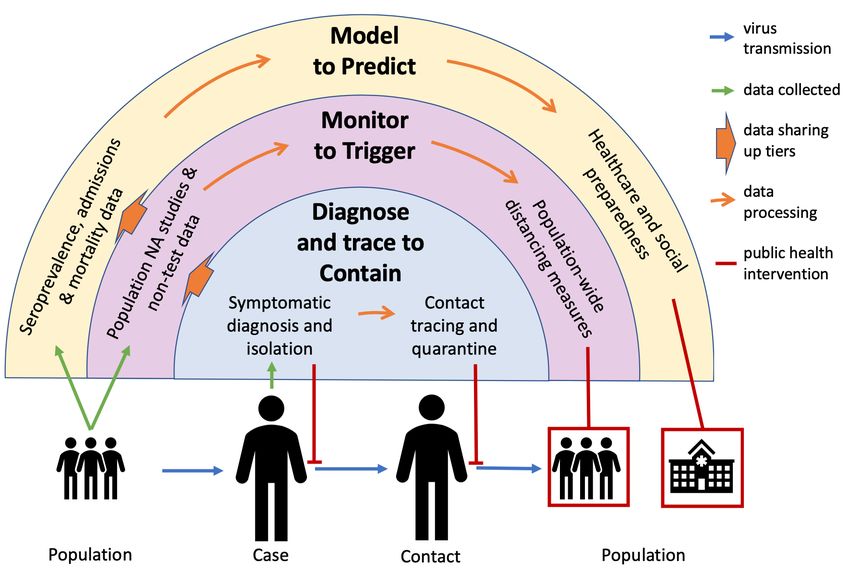
Antigen-Validation study in Schwetzingen • In collaboration with FIND, a WHO collaborating center • Evaluating at least 5 rapid antigen tests that have been submitted for accreditation by WHO • Ongoing in HD, Berlin and Liverpool (planned Lima, Rio de Janeiro, Cape Town) • Against a PCR reference standard • Sample size ~ 5000; Problem: # positives cases

Antigen – PCR Triage Algorithm
• Advantages:
– Rapid isolation of high viral load cases;
– Decisions on access to high-risk settings & precautions
• Disadvantages:
– Cost? Only solution for countries of the
– False security? Global South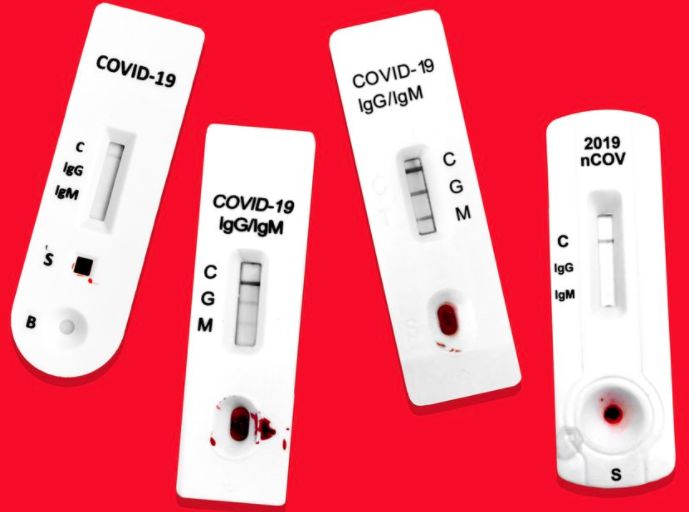
Factors affecting the accuracy & biological significance of PCR tests https://www.medrxiv.org/content/10.1101/2020.04.24.20078949v1.full.pdf
Tests for exposure - Antibody Tests
• Detect circulating IgM/IgG/IgA
• + depending on target after 7-21d
• Variable sensitivity and specificity
• POC or lab-based tests
• Cross-reaction with other COV and
non-specific reaction due to other
infections (estimated reduction in
specificity of 2-10%)
https://www.theverge.com/2020/5/7/21248734/coronavirus-antibody-tests-explained-covid-19-immunity-accurate
https://www.biorxiv.org/content/10.1101/2020.05.14.095414v1
https://pubmed.ncbi.nlm.nih.gov/32584464/How to interpret an Antibody test – or any test • There is no test that is 100% accurate • With any test that is not 100% accurate there are four possible outcomes for a person: – Test is positive and you have the disease (true +) – Test is positive and you don’t have the disease (false +) – Test is negative and you don’t have the disease (true negative) – Test is negative and you have the disease (false negative) • The probability of each depends on the pre-test probabilty, i.e. how many people really do have the disease
5% cumulative incidence: If you are negative,
you are negative, if you are positive, flip a coin
https://www.scientificamerican.com/article/coronavirus-antibody-tests-have-a-mathematical-pitfall/25% cumulative incidence: If you are negative,
you are negative, if positive, you likely had it
https://www.scientificamerican.com/article/coronavirus-antibody-tests-have-a-mathematical-pitfall/Do antibodies confer immunity? • Extrapolating from other coronavirus studies, it is expected that a partial immunity will be present: i.e. reinfection results in less symptoms and less viral replication • The duration is probably medium term (i.e. months to a year); antibodies seem to disappear within months • It is unclear to date whether a person who does not develop any antibody response has immunity or not Reed J Med Vir 1984 Callow Epi Infect 1990 Long Nature Medicine 2020 https://www.nature.com/articles/s41591-020-0965-6
HOW DO WE TEST
Symptomatic suspected case
• PCR - Gold standard diagnostic test, Antigen test alternative or
sequential
• Positive test confirms diagnosis
– Pitfalls: During a high-prevalence phase of the pandemic, a positive result may
be coincidental, or only partly explain the individuals symptoms
• Negative test makes COVID-19 less likely.
– Pitfalls: likelihood of a false negative in an individual with influenza-like illness
include: long disease course & severe disease e.g. oxygen requirementsContacts of confirmed cases and
healthy high-risk groups
• PCR: Positive result confirms current/recent infection
– Negative result - unlikely to be infected; Pitfall - Still at risk
of being in incubation period with no viral shedding
• Antibody test:
– Positive result: indicates past infection
• PPV would have to be high to guide individual advice, which requires a
high pre-test probability, especially if cumulative incidence is low
– Negative result: indicates no past infection, though doesn’t
confirm it since the test is not fully sensitive.Sample of population independent of
symptoms
• PCR: Positive test: infection confirmed
– Negative test: good NPV with a low pre-test probability, but this does not rule
out future infection.
– The proportion of positive results would give important insight into
asymptomatic/pre-symptomatic infection
• Antibody testing:
– Results can be used on a population level to estimate the proportion of the
population exposed.
– On a population level, imperfect accuracy of the test and uncertain biological
significance of the test results should still be considered but can be accounted
for in models or in sequential testingWHO AND WHEN DO WE TEST
3-tiered strategy
against COVID-19
Picture: Courtesy: Timesh Pilay3-tiered strategy against COVID-19
• Tier 1: Diagnose and trace to contain
– most immediate public health value > captures active
cases > isolation to prevent further transmission
• Tier 2: Monitor to trigger
– representative sampling (overall or in high risk settings) >
inform public health measure
• Tier 3: Model to predict
– incorporates data from Tiers 1 & 2 along with
seroprevalence data to predict future phases and inform
wider healthcare and social preparednessSampling methods
Nasopharyngeal >
Orophayngeal >
Tongue = Buccal = Saliva
Difference ~ 5-10%
Self-Testing
Tu medRxiv doi: https://doi.org/10.1101/2020.04.01.20050005, https://www.nejm.org/doi/full/10.1056/NEJMc2016321
Yang Y, DOI:10.1101/2020.02.11.20021493.
Wyllie medRxiv 2020; : 2020.04.16.20067835.Self-testing/ Screening apps
• Known to work for
Influenza in a Gates-funded
project in Washington State
• Emerging data to be a
viable option for COVID-19
• Resource saving
• Pooling
• Screening apps
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2767065?resultClick=1TB in times of COVID
Commonalities & differences - TB & COVID-19?
Tuberculosis COVID-19
From person to person through
From person to person through
How it spreads? droplets, aerosols and through
droplet nuclei
contaminated surfaces
Systemic/generalised symptoms
Fever, cough (usually dry), sore
include fever, weight loss and night
throat & shortness of breath &
Disease Symptoms sweats. Lung specific symptoms :
olfactory abnormalities. Most
cough, shortness of breath, chest
patients are mildly symptomatic .
pain and coughing up blood
Sputum for PTB.
Swabs from naso-pharynx & oro-
Sample Type Samples from site of disease for
pharynx (late sputum)
EPTB
Bacteria: Mycobacterium RNA virus: Severe acute respiratory
Pathogen
tuberculosis syndrome coronavirus 2
Good airborne infection control Good airborne infection control
Prevention and respiratory hygiene measures. and respiratory hygiene measures.
Preventive therapy for LTBI Social distancing.
https://www.ncbi.nlm.nih.gov/books/NBK554776/
Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395: 497–506
https://www.theunion.org/news-centre/covid-19/body/2020_04_22_FAQ-Version-2-English-FINAL-1.pdfDo TB patients have a higher risk of COVID-19
• MTB infection more common than other co-morbidities (36%
vs diabetes 25%; hypertension 22%; CHD 8%; COPD 6%).
• MTB co-infection linked with disease severity (severe/critical
78% vs mild/moderate cases 22%; p=0.005)
• More rapid disease progression:
– More rapid development of symptoms (MTB+COVID: 6.5+/-4.2 days vs
COVID alone: 8.9+/-5.2 days; p=0.07);
– More rapid development of severe disease (MTB +COVID: 3.4+/-2.0
days vs COVID alone: 7.5+/-0.5 days; p=0.075).
Liu, Yongyu & Bi et al. (2020). Active or latent tuberculosis increases susceptibility to COVID-19 and disease severity. 10.1101/2020.03.10.20033795.How will COVID-19 affect the TB incidence?
Stop TB Partnership with Imperial College, Avenir Health, Johns
Hopkins and USAID conducted a modelling exercise
– Potential impact of short-term lockdowns on TB incidence
and mortality over the next 5 years in HBC
– 3 countries in 3 different settings selected for modelling -
• India (high TB burden, private health system)
• Kenya (HIV is a driver of the TB epidemic)
• Ukraine (high proportion of drug-resistant TB)
http://www.stoptb.org/assets/documents/news/Modeling%20Report_1%20May%202020_FINAL.pdfHow will COVID-19 affect the TB incidence?
Country Excess cases between 2020-2025 Excess deaths between 2020-2025
(% increase) (% increase)
2-month lockdown 3-month lockdown 2-month lockdown 3-month lockdown
+ 2-month recovery + 10-month + 2-month recovery + 10-month
recovery recovery
India 514,370 (3.55%) 1,788,100 (12.32%) 151,120 (5.70%) 511,930 (19.31%)
Kenya 12,154 (1.51%) 40,992 (5.08%) 4,873 (2.15%) 15,800 (6.99%)
Ukraine 2,348 (1.19%) 7,589 (3.86%) 455 (2.40%) 1,578 (8.31%)
Global 1,826,400 (3.1%) 6,331,100 (10.7%) 342,500 (4.0%) 1,367,300 (16.0%)
2021 incidence: last seen in 2013 2021 TB deaths: last seen in 2016COVID-19 impacts TB for years
• Scenario of 3 months lock down and 10 months restoration:
Between 2020 and 2025 (globally):
• Additional 6.3 million will develop TB, and 1.4 million more will die of TB
• Setback of at least 5 to 8 years in the fight against TB
• TB incidence per unit population will increase to levels seen 5-8 yrs ago
• Could be conservative estimate as it does not factor in other
possible impacts of the pandemic on
• TB transmission, treatment interruptions, poorer treatment outcomes,
potential implications due to disruptions in HIV careTB diagnostic platforms for COVID-19?
2 decentralized TB molecular test platforms have been put
• Emergency use authorization accorded for the Cepheid
into use for diagnosis of COVID-19: Xpert Xpress SARS-CoV-2 test (March 20 2020)
• GeneXpert • TrueNAT available primarily in India
• TrueNat
Decentralized available TB platforms ensure early
access to quality COVID-19 tests BUT cost is limiting
Centralized test platforms have quickly added SARS-CoV2 in • Roche Molecular Diagnostics cobas® SARS-CoV-2 (for
their portfolio use on the cobas® 6800/8800 Systems)
Competiton of limited capacity or
synergy?
https://www.finddx.org/covid-19/pipeline/COVID-19 is likely to stay with us and TB as well
• Increased focus on health systems gives opportunity to -
– Strengthen and leverage infrastructure, HC delivery mechanisms &
prevention practices
– Foster cough and respiratory hygiene
• Lot of TB learning can be used for tackling COVID-19
– Resource material – e.g. manage associated stigma; Contact tracing
– Supply chain mechanism & access strategies
àNot to create parallel structures, but leverage the strengths
and in solidarity with TB programsThank you • Thank you to Aakshi Kalra for slides to TB & COVID
You can also read