SCIENTIFIC SUMMARY - HERALDING A NEW ERA OF EPISODIC, CHRONIC AND REFRACTORY MIGRAINE MANAGEMENT - Springer Healthcare IME
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUM
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
Chaired by Paolo Martelletti
With Lars Edvinsson and Messoud Ashina
Friday 28th September, 2018
14:00–15:00, Florence, Italy
SCIENTIFIC SUMMARY
CONTENTS
3 Chair's welcome
4 Faculty biographies
6 Introduction
Paolo Martelletti
7 Advances in the pathophysiology of migraine
Lars Edvinsson
11 New therapeutic options for episodic migraine
Messoud Ashina
14 Management of the chronic/refractory patient
Paolo Martelletti
18 Delegate feedback
18 Self-assessment quiz
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
2
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUM
CHAIR'S WELCOME
Dear Colleagues
Thank you for attending the independent satellite symposium entitled ‘Heralding
a new era of episodic, chronic and refractory migraine management’ at the 12th
European Headache Federation (EHF) Congress, which we hope you found
engaging and educational.
Florence provided an excellent host city for this conference, bringing together
emerging doctors, neurologists, and general practitioners to work towards a
shared goal: to increase awareness of headache disorders and improve the quality
of life of those affected by them.
The symposium discussed advances in the pathophysiology of migraine, which
included new and emerging therapeutic options for patients with episodic,
chronic, and refractory migraine, and their role in reducing the burden of this
debilitating condition. Case presentations and interactive keypads were used to
stimulate audience discussion. We hope that by sharing expert experience and
perspectives, we have helped you to navigate the complexities of migraine and
provided you with knowledge that you will be able to seamlessly apply to your
own clinical practice.
We hope that you found this symposium both educational and rewarding.
Yours faithfully,
Professor Paolo Martelletti – Chair
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
3
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUM
FACULTY BIOGRAPHIES
Paolo Martelletti
Associate Professor and Chairman, Internal and Emergency
Medicine, Sapienza University, Rome, Italy
Paolo Martelletti is associate professor and chairman of internal and emergency
medicine in the Department of Clinical and Molecular Medicine at Sapienza
University in Rome, Italy. He is the current president of the European Headache
Federation (EHF), a post he has held since 2016, and editor-in-chief and founder
of the Journal of Headache and Pain.
Professor Martelletti is a world-renowned expert clinician and has been a researcher
in the field of headache disorders for four decades. His studies have primarily
focused on the neuroimmunology of headache disorders, the multifaceted
aspects of advances in therapeutics and, more recently, the application of
personalised medicine to headache.
Professor Martelletti is co-founder and chairman of the World Health Organization
(WHO) global campaign against headache, Lifting the Burden, and is European
expert for the European Medicines Agency. Between 2014 and 2015 he was
president of the Italian Society for the Study of Headache (SISC). He has been,
and is currently, an editorial board member for multiple medical journals and
has authored close to 200 indexed publications and contributed to over 200
book chapters on topics ranging from headache, rheumatology, pain and
internal medicine.
Messoud Ashina
Professor of Neurology, Health and Medical Sciences,
University of Copenhagen, Denmark
Messoud Ashina is professor of neurology in the Faculty of Health and Medical
Sciences, University of Copenhagen, and director of the Human Migraine Research
Unit at the Danish Headache Center and Department of Neurology, Rigshospitalet
Glostrup in Copenhagen, Denmark.
Professor Ashina has been actively involved in headache research since 1995.
His research interests include experimental migraine and cluster headache models,
functional neuroimaging, novel antimigraine drug targets, the mechanism of
migraine and action of antimigraine medications. He has authored over 400
papers, abstracts and book chapters on the topic of headache and migraine.
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
4
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUM
Lars Edvinsson
Professor of Internal Medicine, Lund University, Sweden
Lars Edvinsson is professor of internal medicine at the Lund University in Sweden
and a physician in the Department of Emergency and Internal Medicine at the
Skåne University Hospital, Scania, Sweden. He is currently president of the
International Headache Society, has co-authored over 950 scientific publications
and is the author of Cerebral Blood Flow & Metabolism, a major textbook in this
field.
Professor Edvinsson is a leading expert in the field of cerebral circulation and
migraine and has received global recognition for his work on vascular intervention
and receptor regulation. His extensive research has been a major contributor to
what is known about the roles of the cerebral vasculature in health and diseases
such as stroke and primary headaches.
His expertise is in immunohistochemistry, molecular biology of cell signaling,
proteomics, animal models for acute stroke and acute myocardial infarcts,
pharmacology and treatment methods, string and perfusion myography for
receptor and functional studies of isolated blood vessels.
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
5
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUM
PAOLO MARTELLETTI
Symposium Chair
Sapienza University, Rome, Italy
Click here to view a clip from Professor
Martelletti’s presentation
Professor Martelletti opened this independent satellite symposium by describing
migraine as a neurological disorder that requires further understanding to
optimise management. He explained how this symposium would examine
advances in the pathophysiology and genetics of migraine as a chronic
neurological condition, allow discussion of emerging therapeutic options for
patients with episodic and chronic migraine, and highlight the importance in
reducing the burden of the condition of the patient. In addition, this symposium
would consider how to identify and optimally manage patients with chronic
refractory migraine. Using case studies and interactive keypads, the delegates
would be asked to vote on which treatment options they would use at defined
points along the patients’ therapeutic journey and compare their treatment
choices with that of their peers.
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
6
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUM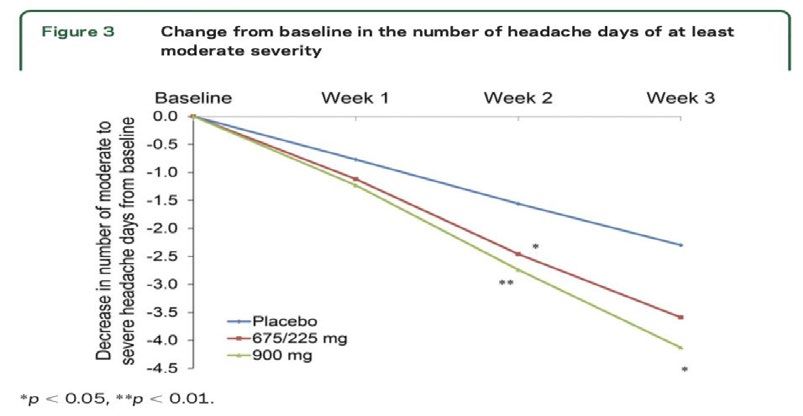
ADVANCES IN THE PATHOPHYSIOLOGY OF MIGRAINE
Lars Edvinsson
Lund University, Sweden
Click here to view a clip from Professor
Edvinsson’s presentation
Professor Edvinsson opened his presentation by explaining that migraine is a
progressive disease, as defined by diagnostic criteria from the International
Headache Society. Low frequency episodic manifestations can progress and
become more frequent until they result in chronic migraine, a process referred to
as clinical transformation.1 (Figure 1).
Figure 1: Episodic migraine increases in attack frequency over time leading to chronic
migraine. Data taken from Bigal M. Lipton RB. Headache 2006; 46: 245-252, Bigal ME,
Lipton RB. Neurology 2008; 71: 848–55. 1,2
Migraine is a progressive disease
Relatively Stable, Episodic Migraine Evolving Most Refractory
Low Risk Pool to Chronic Migraine Stage
Low Frequency Intermediate Frequency High Frequency Chronic Migraine
Episodic Migraine Episodic Migraine Episodic Migraine
1-2 days/month 3-7 days/month 8-14 days/month 15+ days/month
Low disability Some disability High disability Highest disability
Prevalence = 7.5% Prevalence = 2.5% Prevalence = 1.5% Prevalence = 1.5%
Only requires acute care Some require prevention (most All require prevention and All require prevention
use generic) many failed to generic
Most are treated with OTCs Only BTX is FDA approved
High chance to develop
chronic migraine
Primary care
Need Prevention
Neurologist/Headache specialist
He described migraine as a global disease affecting 12% of the population
worldwide or 1 billion people, and added that migraine is currently ranked as
the seventh most disabling disease, with severity of disease varying between
patients.3
Most migraine symptoms across the different phases of an attack (premonitory
phase, aura, headache phase, postdrome) have neurologic origins and Professor
Edvinsson noted that it could be described as a ‘brain-derived disease’
(Figure 2). For example, migraine aura, where many symptoms of the premonitory
phase, along with associated nausea/vomiting, likely arise as a result of neurologic
events.4,5
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
7
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUM
Figure 2: Many migraine symptoms across the different phases of an attack are
neurologic in nature. Data taken from Cady R, et al. Headache 2002; 42: 204–16,
Goadsby P. Trends Mol Med 2007; 13: 39–44.4,5
Most symptoms have neurologic origins
Aura Headache
Scotoma phase
Fortification spectrum Headache
Paresthesia Nausea and vomiting
Weakness Photophobia
Vertigo Phonophobia
Osmophobia
Premonitory Postdrome
Fatigue Fatigue
Cognitive difficulty Cognitive difficulty
Heightened sensory Heightened sensory
awareness awareness
Food craving Food craving
Mood changes
Anorexia
Cady R et al. Headache 2002;42:204-16.
Goadsby P. Trends Mol Med. 2007;13:39-44.
Migraine is often described as a complex disease with genetic implications, but
which genes are responsible? Professor Edvinsson explained that genome-wide
association studies initially identified 13 independent loci associated with migraine.
More recently, 44 independent single-nucleotide polymorphisms significantly
associated with migraine risk have been identified that mapped to 38 distinct
genomic loci.6 He added that mutations in four genes have been identified in
familial hemiplegic migraine (FHM), from which CACNA1A (FHM type 1)
and SCN1A (FHM type 3) code for neuronal voltage-gated calcium or sodium
channels, respectively, while ATP1A2 (FHM type 2) encodes the α2 isoform of
the Na+/K+-ATPase’s catalytic subunit, thus classifying FHM primarily as an ion
channel/ion transporter pathology.
Professor Edvinsson questioned how migraine could be controlled and explained
that the trigeminovascular system is thought to comprise neurons located in
the trigeminal ganglion that innervate the cerebral vasculature including the
dura mater.7 He noted that this system appears to be a key regulator of several
vasoactive neuropeptides that are associated with neurogenic inflammation,
including calcitonin gene-related peptide (CGRP), which may modulate pain
transmission and vascular tone, therefore making them an important target in the
management of migraine. He explained that CGRP is found in small to medium-
sized neurons (about 50%) and in nerve fibres that are dispersed within the
trigeminal ganglion and in perivascular CGRP-positive nerve fibres.
Professor Edvinsson noted that the trigeminal synapse, from where CGRP is
released, is the clear target for migraine pharmacotherapy, highlighting that CGRP
receptor antagonists (e.g. gepants), anti-CGRP antibodies and anti-CGRP receptor
antibodies have proved effective for migraine pain relief, strongly supporting the
hypothesis that CGRP has a major role in migraine pathophysiology8 (Figure). He
then asked the audience to select the site of action of therapeutic antibodies in
the treatment of migraine – 33% responded that antibodies competed with CGRP
for the receptor in the synaptic gap, while 21% thought CGRP, triptans, gepants,
and antibodies interact with central nervous system (CNS) CGRP mechanisms.
Only 1% of the audience specifically agreed that antibodies passed the blood-
brain barrier, although 30% of the audience responded that all three statements
were correct.
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
8
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUM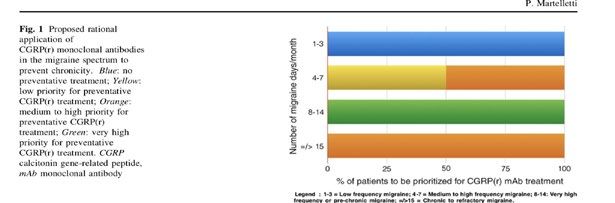
Figure 3: CGRP is a clear therapeutic target as it has a major role in migraine
pathophysiology. Reproduced by permission from Springer Nature: Springer. Nat
Rev Neurol 2018; 14: 338–350. Edvinsson L, et al. https://doi.org/10.1038/s41582-018-
0003-1 © 2018 Springer Nature Limited. All rights reserved.8
The target is clear - the trigeminal synapses?
Trigeminal Nerve
Triptans
CGRP
Antibody
CGRP
CGRP Gepants
Receptor
Antibody
AC
Gα
cAMP
s
Vascular Smooth PKA
Muscle Cell, Glial cells,
Neurons Vasodilation
Edvinsson L et al. Nat Rev Neurol 2018;14:338-50.
The site of action of migraine drugs and whether these agents really needed to
cross the blood-brain barrier was then discussed. Professor Edvinsson highlighted
that sumatriptan (3%), CGRP blockers (2%), and antibodies (30 times higher than in the CNS. This finding suggests that the
trigeminal ganglion could provide an important drug target site with a direct
effect on the trigeminal system.12
Finally, Professor Edvinsson addressed whether circulating CGRP, or its family
of peptides, could influence the tone of the middle cerebral artery. He presented
evidence to show that α or βCGRP can act on smooth muscle cell receptors in
the rat middle cerebral artery, but were effectively prevented from reaching these
receptors from the blood by the arterial endothelium.13
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
9
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUM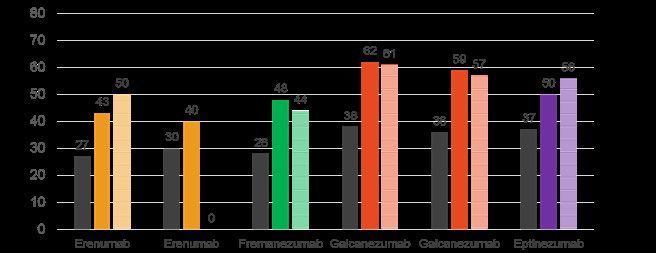
REFERENCES
1. Bigal ME, Lipton RB. Clinical course in migraine: conceptualizing migraine transformation.
Neurology 2008; 71: 848–55.
2. Bigal M. Lipton RB. Modifiable risk factors for migraine progression. Headache 2006; 46:
1334-43.
3. Linde M, Dahlöf C. Attitudes and burden of disease among self-considered migraineurs--a
nation-wide population-based survey in Sweden. Cephalalgia 2004; 24: 455–65.
4. Cady R, Schreiber C, Farmer K, Sheftell F, Goadsby P. Primary headaches: a convergence
hypothesis. Headache 2002; 42: 204–16.
5. Goadsby P. Recent advances in understanding migraine mechanisms, molecules and
therapeutics. Trends Mol Med 2007; 13: 39–44.
6. Gormley P, Anttila V, Winsvold BS, et al. Meta-analysis of 375,000 individuals identifies 38
susceptibility loci for migraine. Nat Genet 2016; 48: 856–66.
7. Edvinsson L. CGRP receptor antagonists and antibodies against CGRP and its receptor in
migraine treatment. Br J Clin Pharmacol 2015; 80: 193–99.
8. Edvinsson L, Haanes KA, Warfvinge K, Krause DN. CGRP as the target of new migraine
therapies - successful translation from bench to clinic. Nat Rev Neurol 2018; 14: 338–50.
9. Schankin CJ, Maniyar FH, Seo Y, et al. Ictal lack of binding to brain parenchyma suggests
integrity of the blood-brain barrier for 11C-dihydroergotamine during glyceryl trinitrate-
induced migraine. Brain 2016; 139 (Pt 7): 1994–2001.
10. Amin FM, Hougaard A, Cramer SP, et al. Intact blood-brain barrier during spontaneous
attacks of migraine without aura: a 3T DCE-MRI study. Eur J Neurol 2017; 24: 1116–24.
11. Eftekhari S, Salvatore CA, Johansson S, Chen TB, Zeng Z, Edvinsson L. Localization of CGRP,
CGRP receptor, PACAP and glutamate in trigeminal ganglion. Relation to the blood-brain
barrier. Brain Res 2015; 1600: 93–109.
12. Lundblad C, Haanes KA, Grände G, Edvinsson L. Experimental inflammation following
dural application of complete Freund’s adjuvant or inflammatory soup does not alter brain
and trigeminal microvascular passage. J Headache Pain 2015; 16: 91.
13. Edvinsson L, Nilsson E, Jansen-Olesen I. Inhibitory effect of BIBN4096BS, CGRP(8-37), a
CGRP antibody and an RNA-Spiegelmer on CGRP induced vasodilatation in the perfused
and non-perfused rat middle cerebral artery. Br J Pharmacol 2007; 150: 633–40.
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
10
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUMNEW THERAPEUTIC OPTIONS FOR EPISODIC MIGRAINE
Messoud Ashina
Health and Medical Sciences,
University of Copenhagen, Denmark
Click here to view a clip from Professor
Ashina’s presentation
Professor Messoud Ashina opened his presentation by explaining that two
types of migraine exist – episodic migraine and chronic migraine – and that his
presentation would focus on the episodic type. He noted that currently available
migraine-specific acute treatments include sumatriptan, eletriptan, rizatriptan,
zolmitriptan, almotriptan, naratriptan, and frovatriptan. Professor Ashina added
that patients with episodic migraine in his home country of Denmark would
typically start to receive sumatriptan as it was the cheapest triptan.
He then asked the audience how they would treat a 45-year-old patient with
known coronary artery disease and frequent migraine. Most delegates (44%)
opted to prescribe NSAIDs, while neurostimulation, ditans, and triptans were
selected by 24%, 16%, and 15% of delegates, respectively. He commented that this
was an interesting result given that available data suggest possible safety issues
when using NSAIDs in patients with coronary disease.
The role of serotonin (5-HT) is recognised as the cornerstone for currently
available therapeutic options such as the triptans – for example, sumatriptan acts
as an agonist for serotonin 5-HT1B and 5-HT1D receptors (located on meningeal
arteries and peripheral trigeminal neurons). Professor Ashina explained that
lasmiditan is a specific 5-HT1F receptor agonist, developed as a new group known
as ‘ditans’ which have a nonvascular mechanism of action. The 5-HT1F receptor
is located in the trigeminal ganglion and in the trigeminocervical complex
and lasmiditan was developed to meet the unmet needs of currently available
medications and circumvent unwanted vascular adverse effects. Professor Ashina
highlighted that data from Phase III SAMURAI and SPARTAN studies for the acute
treatment of migraine showed that a greater percentage of patients treated with
lasmiditan (50 mg, 100 mg, and 200 mg doses) were migraine -pain free at two
hours following the first dose compared with placebo.1
As CGRP has emerged as a key neuropeptide involved in the pathophysiology
of migraines, Professor Ashina highlighted that several small molecule CGRP
receptor antagonists were currently under development which comprised the
‘gepant’ class of compounds for acute migraine therapy. Of these, he noted that
top-line Phase III data from ACHIEVE I for ubrogepant (50 mg and 100 mg
doses) appear positive compared with placebo in the treatment of a single
migraine attack in adults.2 Both doses showed a significantly greater percentage
of ubrogepant patients achieving pain freedom at two hours after the initial dose
as compared with placebo patients (50 mg vs placebo, p=0.0023, 100 mg vs
placebo, p=0.0003) along with a significantly greater percentage of ubrogepant
patients achieving absence of the most bothersome migraine-associated
symptom at two hours after the initial dose as compared with placebo patients
(50 mg vs placebo, p=0.0023; 100 mg vs placebo, p=0.0023). In addition, no
cardiovascular or liver safety concerns were identified. Similar data from
ACHIEVE II were also achieved using ubrogepant 25 mg and 50 mg versus
placebo.3 He then presented data from two Phase III studies of rimegepant, both
of which met their co-primary endpoints of freedom from the most bothersome
migraine symptom and pain freedom two hours after the first dose.4 Thus, he
confirmed that in addition to the current use of triptans for the treatment of acute
migraine, future treatment options would likely include lasmiditan, ubrogepant,
and rimegepant.
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
11
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUMProfessor Ashina then asked the audience how they would treat a 45-year-old
patient with episodic migraine who was judged to be at increased risk of coronary
artery disease. Nearly half (45%) of the audience opted for lasmiditan, while a
similar number (40%) would use a gepant. Remaining audience members selected
triptans (8%), NSAIDs (7%), and neurostimulation (1%).
He then focused his attention on preventive treatments for episodic migraine
highlighting that available treatments such as metoprolol, topiramate, and
flunarizine all have non-migraine-related indications, apart from botulinum toxin
type A, which is currently approved for use in chronic migraine. Data from a Phase
IIb/III study with atogepant, a CGRP receptor antagonist, have demonstrated
robust efficacy and safety in episodic migraine prevention. All active treatment
arms of atogepant (10 mg QD, 30 mg QD, 60 mg QD, 30 mg BID, 60 mg BID)
met the primary endpoint across all doses and dose regimens, with a significant
reduction from baseline in monthly migraine/probable migraine headache days in
patients with episodic migraine treated with atogepant compared with placebo
for 12 weeks. (Allergan press release 04.27.2018).5
Other future treatments for episodic migraine prevention include erenumab, a
human monoclonal antibody that inhibits the receptor for CGRP, and monoclonal
antibodies binding to CGRP, which include eptinezumab, galcanezumab, and
fremanezumab. Phase III data from the use of these agents in the prevention of
episodic migraine, while not a direct comparison, suggest a significantly higher
number of responders (defined as ≥50% responders) with all four treatments
compared with placebo (Figure 1).6-11 Professor Ashina added that these new
treatments also appear to provide an early onset of efficacy in the prevention of
episodic migraine, with efficacy typically seen within one week.
Figure 1: Comparison of CGRP monoclonal antibodies (vs placebo) in the
prevention of episodic migraine. Data taken from: Goadsby et al. Headache 2017;
57 (Suppl 3): 128, Dodick et al. Headache 2017; 57 (Suppl 3): 191, Stauffer et al.
Headache 2017; 57, Conley et al. Headache 2017; 57, Aycardi et al. IHC 2017,
Saper et al. IHC 2017 poster. 6-11
DANISH HEADACHE CENTER
Episodic Migraine: CGRP mAbs Vs
Current Therapy (Phase III)
*
*
*
≥50% responders (%)
EPISODIC MIGRAINE
Placebo
* *
*
Dose 1
Dose 2
N= 316 312 318 288 282 290 287 288 425 210 208 450 226 220
Dose: 70/140mg, sc1 70mg, sc2 225/675mg, sc3 100/300mg, iv4 120/240mg, sc5 120/240mg, sc6
1. Goadsby et al. Headache 2017; 57 (Suppl 3):128; 2. Dodick et al. Headache 2017; 57 (Suppl 3): 191; 3. Stauffer
et al. Headache 2017; 57; 4. Conley et al. Headache 2017; 57; 5. Aycardi et al. IHC 2017; 6. Saper et al. IHC 2017
poster
In addition, there are some data to suggest efficacy of neurostimulation in both
treatment and prevention of acute episodic migraine. Finally, Professor Ashina
asked the audience how they would treat a 50-year-old woman with high
frequency episodic migraine. Most delegates (75%) responded that they would
prescribe anti-CGRP/CGRP receptor monoclonal antibodies, while 13% would use
topiramate, 7% atogepant, 5% candersartan, and 1% neurostimulation. Professor
Ashina commented that while most delegates would opt to use anti-CGRP/
CGRP receptor monoclonal antibodies, cost of treatment may impact on the final
decision.
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
12
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUMREFERENCES
1. Eli Lilly, data on file.
2. https://www.allergan.com/news/news/thomson-reuters/allergan-announces-positive-top-
line-phase-3-resul
3. https://www.allergan.com/news/news/thomson-reuters/allergan-announces-second-
positivephase-3-clinica.
4. Lipton et al. American Headache Society (AHS) Annual Meeting 2018. Abstract #IOR-02LB.
Presented June 30, 2018.
5. https://www.prnewswire.com/news-releases/allergans-oral-cgrp-receptor-antagonist-
atogepant-demonstrates-robust-efficacy-and-safety-in-episodic-migraine-prevention-in-a
phase-2b3-clinical-trial-300663770.html
6. Goadsby, PJ, et al. Non-invasive vagus nerve stimulation for the acute treatment of episodic
and chronic cluster headache: Findings from the randomized, double-blind, sham-controlled
ACT2 Study. Headache 2017; 57 (Suppl 3): 128.
7. Dodick DW et al. A Phase 3, randomized, double-blind, placebo-controlled study to evaluate
the efficacy and safety of erenumab in migraine prevention: primary results of the ARISE
trial. Headache 2017; 57 (Suppl 3): 191.
8. Stauffer et al. The relationship between headache frequency and illness burden prior to
treatment randomization in two phase 3 episodic migraine clinical trials. Headache 2017; 57
(Suppl 3): 190.
9. Conley et al. Phase 3 studies (EVOLVE-1 & EVOLVE-2) of Galcanezumab in episodic
migraine: results of 6-month treatment phase. Cephalalgia 2017; 37 (Suppl).
Abstract PO-01-197.
10. Aycardi E, Bigal M, Yeung P, et al. Efficacy and safety of 2 dose regimens of subcutaneous
administration of fremanezumab (TEV-48125) versus placebo for the preventive treatment
of episodic migraine. Cephalgia 2017; 37 (Suppl): PO-01-201.
11. Saper J, Lipton R, Kudrow D, et al. A Phase 3, randomized, double-blind, placebo-
controlled study to evaluate the efficacy and safety of eptinezumab in frequent episodic
migraine prevention: Primary results of the PROMISE 1 (PRevention Of Migraine via
Intravenous eptinezumab Safety and Efficacy 1) trial. Cephalgia 2017; 37 (Suppl): Abstract
PO-01-194.
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
13
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUMMANAGEMENT OF THE CHRONIC/REFRACTORY PATIENT
Paolo Martelletti
Symposium Chair
Internal and Emergency Medicine, Sapienza University, Rome, Italy
Click here to view a clip from Professor
Martelletti’s presentation
Professor Martelletti began his presentation by explaining that chronic migraine
represents a natural evolution from its episodic form, typically developing after
a slow increase in headache frequency over months to years, and was typically
defined as headaches on at least 15 days per month.1 He explained that current
treatment (drug prophylaxis) for chronic migraine with the highest level evidence
(≥2 randomised controlled studies) included topiramate and botulinum toxin
type A, with the latter being the only medication currently licensed for prevention
of chronic migraine. However, he noted that available clinical data suggest that
chronic migraine becomes refractory to botulinum toxin type A by the second
year of treatment.2
Professor Martelletti explained that chronic migraine frequently and cyclically
fluctuates, with the transition to more frequent attacks often leading to an acute
overuse of medications. However, such medication overuse can complicate every
type of headache and is itself associated with chronic migraine. In addition, while
EHF criteria for refractory chronic migraine have identified the ease of stopping
medications, they also highlight the difficulty in preventing relapse. He noted
that setting up a collaborative, multidisciplinary team of specialists in headache
practices with the goal of modifying physical, environmental, and psychological
triggers for chronic migraine may facilitate treatment of these patients, including
those experiencing refractory disease. He added that any comorbid conditions,
such as depression and anxiety disorders, which both represent undisputable co-
factors in the progression of migraine chronification, must be identified at an early
stage and adequately treated.
Professor Martelletti noted that a significant minority of individuals with chronic
migraine fail conventional medical treatment, becoming highly disabled. So,
how can we manage refractory patients? An open-label exploratory study has
previously assessed the use of spinal cord stimulation in the management of
chronic, medically refractory migraine (including a lack of response to botulinum
toxin type A) and found that 50% (7/14) patients achieved a >30% reduction in
headache days.3
He then turned his attention to humanised monoclonal antibodies against CGRP
and explained that an integrated analysis of data from three Phase III, randomised,
double-blind, placebo-controlled studies in patients with episodic (EVOLVE-1/2)
or chronic (REGAIN) migraine has demonstrated that galcanezumab 120 mg/240 mg
significantly (pThe onset of efficacy of fremanezumab as a preventive treatment of chronic
migraine has been assessed in a randomised placebo-controlled study where
once-monthly injections of fremanezumab 675/225 mg or 900 mg were
compared with placebo.6 He explained that fremanezumab demonstrated a
significant improvement within 1 week of therapy initiation in patients with chronic
migraine (Figure 1).
Figure 1: Fremanezumab demonstrated a significant improvement in number
of headache days within 1 week of therapy initiation in patients with chronic
migraine. Reproduced by permission from Wolters Kluwer. Bigal ME, Dodick DW,
Krymchantowski AV, et al. TEV-48125 for the preventive treatment of chronic
FREMANEZUMAB WORKS WITHIN ONE WEEK
migraine: Efficacy at early time points. Neurology 2016; 87: 41–8. https://doi.
org/10.1212/WNL.0000000000002801 6
al et al. 2016
rology, 87, 41-48
When proposing the rational application of CGRP monoclonal antibodies in
the migraine spectrum to prevent chronicity, he noted that patients with 8–14
migraine
12th days per month (defined as those with
EHF Congress very high2018
28 September frequency or pre-
chronic migraine) have the highest priority for preventative CGRP treatment.7
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
15
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUMFigure 2: Proposed rational application of CGRP monoclonal antibodies suggests
patients with very high frequency or pre-chronic migraine have the highest priority.
Reproduced by permission from Springer International Publishing. BioDrugs 2017; 31:
483–5. Martelletti P. All rights reserved © Springer International Publishing AG 2017.
https://doi.org/10.1007/s40259-017-0251-4.7
PRIORITISING CGRP(r) MONOCLONAL ANTIBODIES USE
12th EHF Congress 28 September 2018
Professor Martelletti then presented two case studies. The first was a 43-year-old
woman attending his tertiary headache centre who had complained of headaches
since the age of 21 years. The subject received the diagnosis of chronic migraine
when aged 36 and in more recent years had experienced a long history of
fluctuating migraine periods (‘in/out chronic migraine’). Despite treatment with
botulinum toxin type A (from February 2016 through to September 2017), he
explained that the use of triptans by the patient had progressively increased up
to 15/18 days per month during this time. He added that a diagnosis of Brugada
syndrome (rare inherited heart rhythm disturbance) was made in September
2017 which led to the abrupt suspension of triptans and an increase in migraine
headache days. The patient’s current diagnosis of refractory chronic migraine
has meant that multiple rehabilitation processes (e.g. psychological support and
physiotherapy) have been used.
He asked the audience if they agreed that cardiovascular risk screening would be
mandatory in this patient before any decision was made to switch her to a new
anti-CGRP monoclonal antibody when available. More than half (53%) did not
think such screening would be needed, 21% felt it would (unqualified), 16% agreed
with screening and felt it should include transoesophageal echocardiography
(TEE) and electrocardiography, while 10% would agree with screening which
included TEE and brain magnetic resonance imaging. Professor Martelletti
commented that while cardiovascular risk screening was not mandatory, there
does appear to be some interaction between anti-CGRP monoclonal antibodies
and the cardiovascular system.
Professor Martelletti’s second case study was a 49-year-old female patient with
major clinical depression and migraine without aura from the age of 12 years.
Since the age of 26 years, this patient had used preventive topiramate and
valproate until she decided to become pregnant. He explained that at 36 years
of age, this patient had a complicated pregnancy and rare migraine with aura
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
16
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUMappeared, with rapid progression to chronic migraine plus medication overuse.
Use of detoxification subsequently allowed the efficacious use of botulinum
toxin type A, although at 44 years of age, the patient had an ovariectomy with
subsequent menopause that reduced the efficacy of this treatment. In December
2016, she was diagnosed with refractory chronic migraine plus medication
overuse. He added that a multimodal rehabilitation procedure had achieved >30%
efficacy and highlighted that future treatments such as galcanezumab could help
this patient further.
Professor Martelletti finally asked the audience if they would have suggested an
appropriate pregnancy prevention programme for this patient prior to precribing
valproate when she was 26 years old? Most delegates (73%) indicated they would,
while 14% said they would not, 8% would opt to only do this following a 3-month
washout period, and 5% would do this only after failure of botulinum toxin type A.
REFERENCES
1. Schwedt TJ. Chronic migraine. BMJ 2014; 348: g1416.
2. Tassorelli C, Tedeschi G, Sarchielli P, et al. Optimizing the long-term management of chronic
migraine with onabotulinumtoxinA in real life. Expert Rev Neurother 2018; 18: 167–76.
3. Arcioni R, Palmisani S, Mercieri M, et al. Cervical 10 kHz spinal cord stimulation in the
management of chronic, medically refractory migraine: A prospective, open-label,
exploratory study. Eur J Pain 2016; 20: 70–8.
4. Zhang Q, Ruff DD, Pearlman EM, Govindan S, Aurora SK. Efficacy of galcanezumab in
patients who failed to respond to preventives previously: Results from EVOLVE-1, EVOLVE-2
and REGAIN Studies (S20.004). Neurology 2018; 90 (15 Supplement) Abstract S20.004.
AAN 70th Annual Meeting, Los Angeles, CA, USA.
5. Lipton R, Saper J, Ashina M, et al. Primary results of PROMISE-1 (Prevention of Migraine
via Intravenous eptinezumab Safety and Efficacy-1) trail: a phase 3, randomized, double-
blind, placebo-controlled study to evaluate the efficacy and safety of eptinezumab for the
preventive treatment of chronic migraine. Abstract S20.001. AAN 70th Annual Meeting, Los
Angeles, CA, USA.
6. Bigal ME, Dodick DW, Krymchantowski AV, et al. TEV-48125 for the preventive treatment of
chronic migraine: Efficacy at early time points. Neurology 2016; 87: 41–8.
7. Martelletti P. The application of CGRP(r) monoclonal antibodies in migraine spectrum: Needs
and priorities. BioDrugs 2017; 31 :483–5.
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
17
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUMDELEGATE FEEDBACK
One third (34%; n=74) of all symposium attendees completed the evaluation form.
Following completion of this educational activity, 81% of delegates agreed/
strongly agreed that they were now better able to describe advances in the
pathophysiology and genetics of migraine as a chronic neurological condition.
Similarly, 91% of delegates felt more able to discuss emerging treatment options
for patients with episodic and chronic migraine and 77% felt better able to
deliberate how to identify patients with chronic refractory migraine and optimally
manage this patient subgroup. The quality of the symposium was ranked highly
(response of 7-10 using a scale from 0 [poor] to 10 [excellent]) by 86% of
attendees.
When commenting on the overall meeting, most attendees agreed/strongly
agreed that the meeting was based on relevant and current evidence (86%),
increased level of knowledge (79%), and focused on competencies relevant to
clinical practice (77%). Importantly, although there no time was for any panel
discussion at the end of the symposium, nearly two thirds (61%) of attendees felt
that the presentations given had already answered any questions they may have
had. After attending the symposium, 74% of delegates would definitely/possibly
make changes to their clinical practice, with most (85%) agreeing that there was
no commercial or personal bias during the symposium.
SELF-ASSESSMENT QUIZ
In order to assess your learning following the symposium and meeting report we
invite you to participate in a short quiz to further increase your knowledge and
understanding of the pathophysiology and new therapeutic options for episodic,
chronic and refractory chronic migraine.
To start the quiz click here
HERALDING A NEW ERA OF EPISODIC,
CHRONIC AND REFRACTORY
MIGRAINE MANAGEMENT
18
12th European Headache Federation Congress
INDEPENDENT MEDICAL EDUCATION SYMPOSIUMThis independent programme is made possible thanks to educational sponsorship from Eli Lilly and Company
You can also read