Short Notes on MRI - MRI of the adult spine - www.hkmacme.org January 2019 - If you're a HKMA Member, please click the ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

www.hkmacme.org January 2019
B U L L E T I N
Short Notes on MRI –
MRI of the adult spine
Dr. KWOK Kai Yan
CME
LIVE
HKMA CME Bulletin
Contents
Editorial 1
Spotlight 2
Short Notes on MRI - MRI of the
adult spine
Cardiology 5
A 54 year old lady with heart
murmur
Dermatology 7
A girl with rough nails for one year Spotlight
Answer Sheet 11 Short Notes on MRI -
CME Notifications 14 MRI of the adult spine
Meeting Highlights 17
CME Calendar 18
HKMA CME Bulletin – MONTHLY SELF-STUDY
SERIES to help you grow!
Please read the following articles and answer the
questions. Participants in the HKMA CME Programme
will be awarded credit points under the Programme
for returning the completed answer sheet via fax
(2865 0943) or by mail to the HKMA Secretariat on
or before 15 February 2019. Answers to questions
will be provided in the next issue of the HKMA CME
Bulletin. (Questions may also be answered online at The Hong Kong Medical Association is dedicated to providing a coordinated CME
www.hkmacme.org) programme for all members of the medical profession. Under the HKMA CME
Programme, a CME registration process has been created to document the CME
efforts of doctors and to provide special CME avenues. The Association strives to
foster a vibrant environment of CME throughout the medical profession. Both members
as well as non-members of the Association are welcome to join us. You may contact
the HKMA Secretariat for details of the programme.
HKMA CME Enquiry Hotline
Tel: 2527 8452
Address: 5/F, Duke of Windsor Social Service Building,
15 Hennessy Road, Hong Kong Advertising Enquiry: 2527 8452 Fax: 2865 0943/Email: cme@hkma.org
CME Bulletin & Online Editorial Board
EDITORIAL
Chief Editor
Dr. LAM Ho
Dr. WONG Bun Lap, Bernard
Executive Committee
Dr. CHAN Yee Shing, Alvin Dearest HKMA Fellow Colleagues
Dr. CHENG Chi Man
Dr. CHEUNG Hon Ming
Happy new year 2019’
Dr. CHOI Kin
Dr. HO Chung Ping, MH, JP
In this very happy beginning of our new year 2019’
Dr. HO Hung Kwong, Duncan please kindly let me share with you my collection on
Dr. LAM Tzit Yuen, David
Dr. LI Sum Wo, MH words of wisdom about new year.
Dr. TSE Hung Hing, JP
Dr. WONG Bun Lap, Bernard
“Write it on your heart that every day is the best day of the year.”
~ Ralph Waldo Emerson (1803-1882), American essayist,
Cardiology Neurology
Dr. CHEN Wai Hong Dr. FONG Chung Yan, Gardian lecturer, philosopher and poet
Dr. HO Hung Kwong, Duncan Dr. TSANG Kin Lun, Alan
Dr. LEE Pui Yin
Dr. LI Siu Lung, Steven Neurosurgery
“Cheers to a new year and another chance for us to get it right”
Dr. WONG Bun Lap, Bernard Dr. CHAN Ping Hon, Johnny ~ Oprah Winfrey (1954-), American media executive, actress,
Dr. WONG Shou Pang, Alexander talk show host, television producer and philanthropist
Dr. WONG Wai Lun, Warren Obstetrics and Gynaecology
Dr. CHAN Kit Sheung
Cardiothoracic Surgery “Be at war with your vices, at peace with your neighbors, and let
Dr. CHENG Lik Cheung Ophthalmology
Dr. CHIU Shui Wah, Clement Dr. LIANG Chan Chung, Benedict every new year find you a better man.”
Dr. CHUI Wing Hung Dr. PONG Chiu Fai, Jeffrey ~ Benjamin Franklin (1705-1790), American polymath, one of
Dr. LEUNG Siu Man, John
Orthopaedics and Traumatology
the Founding Fathers of United States, leading author, printer,
Colorectal Surgery Dr. IP Wing Yuk, Josephine political theorist, politician, freemason, postmaster, scientist,
Dr. CHAN Cheung Wah Dr. KONG Kam Fu inventor, humorist, civic activist, statesman and diplomat.
Dr. LEE Yee Man Dr. POON Tak Lun
Dr. TSE Tak Yin, Cyrus Dr. TANG Yiu Kai
“Come, gentleman, I hope we shall drink down all unkindness.”
Dermatology Paediatrics
Dr. CHAN Hau Ngai, Kingsley Dr. CHAN Yee Shing, Alvin ~ William Shakespeare (1564-1616), English poet, playwright
Dr. HAU Kwun Cheung Dr. FUNG Yee Leung, Wilson and actor, greatest writer in the English language and the
Dr. TSE Hung Hing, JP
Endocrinology Dr. YEUNG Chiu Fat, Henry
world’s greatest dramatist
Dr. LEE Ka Kui
Dr. LO Kwok Wing, Matthew Plastic Surgeon “At a dinner party one should eat wisely but not too well, and talk
Dr. NG Wai Man, Raymond
ENT well but not too wisely.”
Dr. CHOW Chun Kuen Psychiatry ~ W Somerset Maugham (1874-1965), British playwright,
Dr. LAI Tai Sum, Tony
Family Medicine Dr. LEUNG Wai Ching novelist and short story writer, most popular writers of his era
Dr. LAM King Hei, Stanley Dr. WONG Yee Him, John and the highest-paid author during the 1930s.
Dr. LI Kwok Tung, Donald, SBS, JP
Radiology
Gastroenterologist Dr. CHAN Ka Fat, John “Going to a party, for me, is as much a learning experience as,
Dr. NG Fook Hong Dr. CHAN Yip Fai, Ivan you know, sitting in a lecture.
General Practice Respiratory Medicine ~ Natalie Portman (1981-), Israeli-American film actress,
Dr. YAM Chun Yin Dr. LEUNG Chi Chiu producer, and director
Dr. WONG Ka Chun
General Surgery Dr. YUNG Wai Ming, Miranda
Dr. LAM Tzit Yuen, David “All of us every single year, we’re a different person. I don’t think
Dr. LEUNG Ka Lau Rheumatology
Dr. CHAN Tak Hin
we’re the same person all our lives.
Geriatric Medicine Dr. CHEUNG Tak Cheong ~ Steven Spielberg KBE OMRI (1946-) American Filmmaker,
Dr. KONG Ming Hei, Bernard highest-grossing film director in history, one of the founding
Dr. SHEA Tat Ming, Paul Urology
Dr. CHEUNG Man Chiu pioneers of the New Hollywood era and one of the most
Haematology Dr. KWOK Ka Ki popular directors and producers in film history.
Dr. AU Wing Yan Dr. KWOK Tin Fook
Dr. MAK Yiu Kwong, Vincent
Vascular Surgery “Your success and happiness lies in you. Resolve to keep
Hepatobiliary Surgery Dr. TSE Cheuk Wa, Chad
Dr. CHIK Hsia Ying, Barbara Dr. YIEN Ling Chu, Reny
happy, and your joy and you shall form an invincible host against
Dr. LIU Chi Leung difficulties.”
HKMA Secretariat ~ Helen Keller (1880-1968), American author, political activist,
Medical Oncology Ms. Jovi LAM
Dr. TSANG Wing Hang, Janice Miss Irene GOT and lecturer, the first deaf-blind person to earn a bachelor of
Miss Ivy IP arts degree.
Nephrology
Dr. CHAN Man Kam
Dr. HO Chung Ping, MH, JP
Dr. HO Kai Leung, Kelvin
The HKMA CME Bulletin Editorial Board and CME
Committee wish you all a prosperous, healthy and
NOTICE
happy new year 2019’
Medical knowledge is constantly changing. Standard safety precautions must be followed, but as new research
and clinical experience broaden our knowledge, changes in treatment and drug therapy may become necessary
or appropriate. Readers are advised to check the most current product information provided by the manufacturer Dr. WONG Bun Lap, Bernard
of each drug to be administered to verify the recommended dose, the method and duration of administration, and
contraindications. It is the responsibility of the practitioner, relying on experience and knowledge of the patient, to Chief Editor
determine dosages and best treatment for each individual patient. Neither the Publisher nor the Authors assume any
liability for any injury and/or damage to persons or property arising from this publication. Hong Kong Medical Association CME Bulletin
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this publication does
not constitute a guarantee or endorsement of the quality or value of such product or of the claims made of it by its
manufacturer.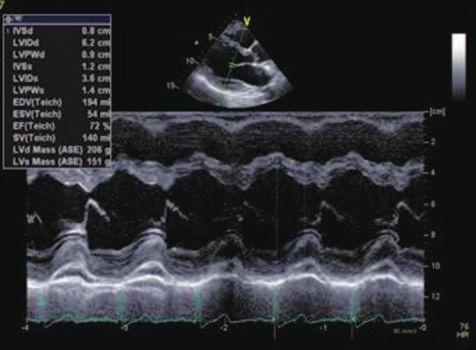
SPOTlight
Short Notes on MRI – Dr. KWOK Kai Yan
MRI of the adult spine MBChB (CUHK), FRCR, FHKCR, FHKAM
(Radiology), Dip Med (CUHK), PDipCAH (HK)
Specialist in Radiology
for incidental lesions in the regions not originally planned to
Introduction be investigated. Although there is similar practice about the
sagittal scanning ranges for each region of the spine, the
Magnetic Resonance Imaging (MRI) of the spine is one of the coverage by axial images can vary for the same region of
most commonly performed MRI examinations. In this short the spine in different patients. The axial imaging may span all
article, I would share some technical issues which may be levels of the included sagittal scanning range, or cover the
useful for clinicians when adult patients are referred for MRI of levels of clinical interest, or cover the levels where abnormality
the spine. is detected on imaging. The acquisition of axial images is
often the most time-consuming component during MRI of the
Indications for MRI of the spine spine. Depending on clinical indications and imaging findings,
radiologists may decide to focus on certain spinal levels to
MRI provides excellent soft tissue contrast. Concerning the improve the image quality (e.g. by adjusting the slice thickness
imaging of spine, it is the only radiological investigation that and inter-slice gaps etc.) for better assessment while skip
allows non-invasive evaluation of the internal anatomical certain spinal levels to control the overall imaging time.
structure of spinal cord. MRI is superior in assessing the spinal
cord, nerve roots, intervertebral discs, bone marrow and other
soft tissue structures along the spine when compared with
other imaging modalities. It also lacks radiation and is the ideal
imaging method for conditions that require repeated follow up.
Indications for MRI of the spine are numerous, including
neoplastic, infective, inflammatory, autoimmune, traumatic,
vascular, degenerative, congenital and many other
miscellaneous conditions. In daily practice, majority of patients
would have already undergone thorough assessment by
clinical history, physical examination and other investigations
before they are referred to MRI. The Clinical Referral
Guidelines from Hong Kong College of Radiologists1 and the
Appropriateness Criteria from American College of Radiology2
provide good guidance concerning the referral for MRI of the
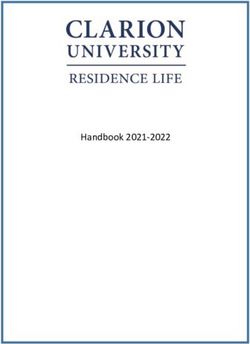
spine. Figure 1a. Sagittal T2W Figure 1b. Localizer image of
image of lumbar spine. Note the same patient in figure 1a.
the inferior scan range only Note the limited image quality.
Technical considerations reaches upper sacrum. The localizer image facilitates
the counting of vertebral
bodies and planning of
imaging planes, but the image
MRI of the spine is a time consuming investigation. It is quality is insufficient for lesion
important that the examination can address the clinical Figure 1. MRI of lumbar spine. assessment.
concern in a time-efficient manner so that more patients can
be served. Limiting the scanning time also reduces the chance
The plane of scan is another important technical consideration.
of patient movement which may jeopardize the image quality.
Sagittal plane is essential and is usually the first scanning plane
to obtain, while axial plane is also needed for most situations.
The range of scan is one of the most important considerations.
The axial imaging plane of the spine refers to the plane parallel
MRI of the spine can be divided into three regions namely
to the intervertebral discs or perpendicular to the spinal
cervical spine, thoracic spine and lumbar spine. MRI of cervical
canal. As the spine is a curved structure, the axial planes at
spine usually covers skull base to T1; MRI of thoracic spine
different levels of the spine would have different orientations. In
usually covers C7 to L1; while MRI of lumbar spine usually
patients with severe kyphoscoliosis, the planning of scanning
covers T12 to upper sacrum. The sacrum and coccyx are
planes may be complex. When indicated by relevant clinical
often not fully included by a routine protocol of MRI of lumbar
information and imaging findings, additional scanning planes
spine (Figure 1a). Therefore, if complete assessment of the
such as oblique (angled sagittal) planes and coronal planes
sacrum and coccyx is needed, it should be specified in the
can be performed. For instance, in cervical region where the
request. For MRI of lumbar spine and thoracic spine, localizer
neural foramina have oblique orientation, imaging in oblique
images would include cervical region to facilitate the counting
(angled sagittal) planes may improve the assessment of the
of vertebral bodies (Figure 1b). These localizer images are at
neural foramina3-5.
lower resolution and insufficient to provide proper assessment
2 HKMA CME Bulletin
www.hkmacme.org
SPOTlight
appropriate, referring clinicians should request MRI of a
targeted region of the spine to focus on the clinical concern.
Referring clinicians can also help to improve the efficiency and
quality of scanning by providing adequate clinical information
(e.g. the anticipated diagnosis, the predicted location of
neurological deficit etc.), so that radiologists can tailor-make
the imaging protocol to address the clinical concern in the
most efficient manner with optimal imaging quality.
Limitations of MRI of the spine
Despite MRI is an excellent tool for the assessment of the
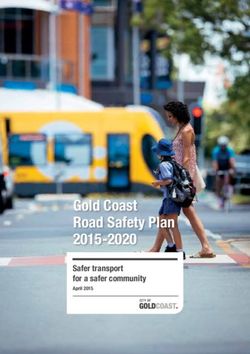
Sagittal T1W image Sagittal T2W image Sagittal T1W fat- spine, it has some limitations.
suppressed post-
contrast image. Note
the multiple enhancing
foci of leptomeningeal
metastasis
Figure 2. Leptomeningeal
metastasis. Note that
intravenous administration of
Gadolinium-based contrast
agent (GBCA) facilitates the
detection of leptomeningeal
metastasis.
Axial T1W post-contrast image at T1
level of the spine. Note the enhancing
focus of leptomeningeal metastasis.
Various MRI sequences can be chosen to image the spine Lateral radiograph of T Sagittal T1W image of Sagittal T2W image of
spine T spine T spine
and their details are beyond the scope of this short article.
Most centers have established MRI protocols with standard Figure 3. Lateral radiograph and MRI of thoracic spine in a patient with
sequences for the routine evaluation of common referrals posterior spinal fusion. Note the artifacts caused by metallic implant,
such as suspected spinal stenosis, suspected radiculopathy with distortion of the contour and signal of the spinal cord, spinal canal,
vertebrae and adjacent soft tissue.
etc. Nevertheless, the application of additional sequences
(e.g. various fat-suppression techniques and vascular
techniques etc.) is sometimes necessary and they are guided
by the clinical information and imaging findings. Intravenous Various artefacts can be caused by patient movement,
administration of Gadolinium-based contrast agent (GBCA) respiration, swallowing, bowel peristalsis, pulsation from blood
is not without risk and it takes addition time to perform post- vessels and CSF flow etc. The presence of metallic implants,
contrast sequences. The need for GBCA injection should be even when they are MRI compatible, can cause artifacts
evaluated for individual patients. For instance, if MRI of the (Figure 3). There are various imaging techniques to reduce
spine is performed with the aim to look for leptomeningeal these artifacts; nevertheless, additional imaging modalities are
metastasis (Figure 2), administration of GBCA is indicated. On occasionally needed to provide complementary assessment.
the other hand, if a patient is already known to have multiple
spinal metastases and MRI is performed with the sole purpose Comparing with MRI, CT provides better visualization of
to assess acute cord compression for treatment planning, cortical bone and calcification. CT is complementary to MRI
GBCA administration may not be necessary. Injection of GBCA for evaluating the bone in tumors with osseous involvement,
is usually needed in some situations such as the assessment and in conditions like ossified posterior longitudinal ligament8,9
of intra-spinal tumors, infectious conditions, inflammatory (Figure 4).
conditions, demyelinating conditions, and for the differentiation
of scar tissue from disc material in patients with previous In trauma cases when time and clinical stability of patient is
spine surgery 3,6,7 etc. When necessary, discussion with the paramount concern, radiographs and CT scan can provide
radiologists is recommended to determine the need of GBCA rapid radiological assessment of the spine when necessary.
administration. MRI remains a good problem-solving tool if the status of spinal
cord and soft tissue injuries need to be evaluated.
The overall examination time in MRI depends on many factors
such as the actual scanning range, the number of imaging Conventional MRI of the spine is performed in supine position.
planes, the number of sequences in each imaging plane and Most MRI scanners cannot assess the dynamic changes of
the parameters of each imaging sequence. It typically takes the spinal components during physiological loading and in
20 to 30 minutes to scan one region of the spine and around various flexion or extension positions. Traditional investigation
an hour to scan the whole spine in common protocols. When like lateral flexion-extension radiography still remains valuable
www.hkmacme.org HKMA CME Bulletin 3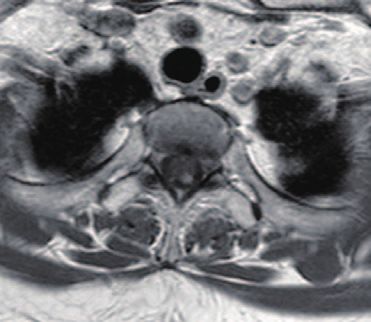
SPOTlight
Reference
1. Hong Kong College of Radiologists. Clinical Referral Guidelines. Available at
https://www.hkcr.org/lop.php/clinical_referral_guideline. Accessed 29 Oct
2018.
2. American College of Radiology. ACR Appropriateness Criteria. Available at
https://acsearch.acr.org/list. Accessed 30 Oct 2018.
3. American College of Radiology. ACR-ASNR-SCBT-MR-SSR Practice
parameter for the performance of magnetic resonance imaging (MRI) of the
adult spine. Available at https://www.acr.org/-/media/ACR/Files/Practice-
Parameters/MR-Adult-Spine.pdf?la=en. Accessed 30 Oct 2018.
4. Shim JH, Park CK, Lee JH, et al. A comparison of angled sagittal MRI and
conventional MRI in the diagnosis of herniated disc and stenosis in the
cervical foramen. Eur Spine J. 2009; 18: 1109-1116.
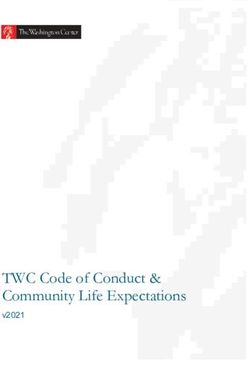
Sagittal T2W image of C-spine Sagittal T1W image of C-spine 5. Park HJ, Kim SS, Lee SY, et al. A practical MRI grading system for cervical
foraminal stenosis based on oblique sagittal images. Br J Radiol. 2013; 86:
20120515.
6. Van Gothem JW, Parizel PM, Kinkins JR. Review article: MRI of the post-
operative lumbar spine. Neuroradiology. 2002; 44: 723-739.
7. Bradley WG. Use of contrast in MR imaging of the lumbar spine. Magn
Reson Imaging Clin N Am. 1999; 7: 439-457.
8. Kang MS, Lee JM, Zhang HY, et al. Diagnosis of cervical OPLL in lateral
radiograph and MRI: Is it reliable? Korean J Spine. 2012; 9: 205-208.
9. Abiola R, Rubery P, Mesfin A. Ossification of the posterior longitudinal
ligament: etiology, diagnosis, and outcomes of nonoperative and operative
management. Global Spine J. 2016; 6: 195-204.
Complete Spotlight, 1 CME Point
will be awarded for at least five correct
Axial T2W image at C3 level of the spine CT scan of C-spine
reformatted in sagittal plane
Q&A Self-Assessment
Questions:
answers
Figure 4. Ossified posterior longitudinal ligament. Note that MRI and CT Answer these on page 11 or make an online submission at: www.hkmacme.org.
provides complementary assessment. MRI provides excellent evaluation of Please indicate whether the following statements are true or false.
the spinal canal and status of spinal cord, while CT scan provides excellent 1. Radiologists can modify the imaging protocol to improve the
demonstration of the ossification.
efficiency and quality of MRI of the spine for individual patients.
2. MRI of cervical spine covers C7 to L1 levels.
in assessing the segmental instability of the spine. Although 3. All MRI of lumbar spine would fully include the whole sacrum and
upright MRI and kinematic MRI etc. are under development, coccyx without the need to specify in the request.
their availability is extremely limited and their application needs 4. In MRI of the spine, the axial imaging planes at different levels of
further evaluation. the spine can have different orientations.
5. Imaging in oblique planes may improve assessment of the neural
Last but not least, the general considerations of MRI safety foramina at cervical region.
should always be observed for MRI of the spine. In patients
with contraindications to MRI, clinicians should collaborate 6. Intravenous administration of Gadolinium-based contrast
agent (GBCA) is usually not necessary for the assessment of
with radiologists to consider the most appropriate alternative
leptomeningeal metastasis in MRI of the spine.
investigations.
7. In patients with prior spinal surgery, intravenous administration
of Gadolinium-based contrast agent (GBCA) can help to
Conclusion differentiate scar tissue from disc material.
8. It only takes one to two additional minutes to perform a typical
There are many technical considerations for MRI of the spine. MRI of the whole spine comparing with a typical MRI of the
By choosing the appropriate scanning ranges and providing lumbar spine for the same patient.
adequate clinical information, referring clinicians can help 9. MRI-compatible metallic implants can still cause artifacts on MRI
radiologists to plan the scanning strategy to provide efficient images.
and high quality imaging.
10. CT and MRI are complementary in the assessment of ossified
posterior longitudinal ligaments.
Answer to December 2018
Spotlight 1-Fighting against hypercholesterolemia with statin for
over 20 years since the 4 S Study 1994
1. F 2. F 3. F 4. F 5. F 6. T 7. T 8. T 9. T 10. T
Spotlight 2-Short Notes on MRI-MRI Safety
1. F 2. F 3. F 4. T 5. F 6. F 7. T 8. T 9. T 10. T
4 HKMA CME Bulletin
www.hkmacme.org
Cardiology
The content of the January Cardiology Series is provided by:
Dr. CHEUNG Ling Ling
Complete Cardiology case, MBBS(HK), MRCP(UK), FHKCP, FHKAM(Med), Specialist in Cardiology
0.5 Cardiology will be awarded for
at least 2 correct answers in total
A 54 year old lady with heart murmur
A 54-year-old woman, suffering from hypertension complaint of increasing shortness of breath and decreased
exercise tolerance. Physical examination revealed a 2/6 diastolic aortic murmur over left lower sternal border.
Electrocardiography showed normal sinus rhythm. Transthoracic echocardiography was performed and the
images were shown below.
Figure 1. Parasternal short axis view of left ventricle
Quadricuspid aortic valve (QAV) is a rare congenital cardiac
anomaly with an incidence of 0.01-0.04% causing aortic
regurgitation usually in the fifth to sixth decade of life.
Figure 2. 5 chamber view
Figure 3. M mode of left ventricle
The LVDD measured 6.2cm which is dilated
Q&A
Please answer ALL questions
Answer these on page 11 or make an online submission at: www.hkmacme.org
1) What is the diagnosis in Figure 1? 3) What abnormality is shown in Figure 3?
A) Unicuspid aortic valve A) Dilated left ventricle
B) Bicuspid aortic valve B) Impaired left ventricular ejection fraction
C) Tricuspid aortic valve C) Left ventricular hypertrophy
D) Quadricuspid aortic valve
4) What is the commonest congenital anomaly
2) What condition is mostly commonly caused by the associated with Figure 1?
pathology in Figure 1 (as shown in Figure 2)?
A) Coronary artery anomalies
A) Aortic stenosis B) Atrial septal defect
B) Aortic regurgitation C) Patent ductus arteriosus
C) Mitral regurgitation D) Mitral valve prolapse
D) Tricuspid regurgitation
www.hkmacme.org HKMA CME Bulletin 5
Cardiology
December Answers
1.E echo. Absence of reciprocal ST depression at anterior leads
made inferior STEMI less likely in this situation. In addition
This is a common scenario encountered almost every day in normal wall motion from focus echo is helpful in ruling out
A&E: a patient with ST segment elevation in ECG. The chest this potentially fatal possibility. Hypertrophic cardiomyopathy
pain as described was pleuritic in nature with pericardial rub (HCM) is associate with “thick wall” especially at interventricular
on examination which was unrelieved by sublingual nitrate, septum which may result in dynamic left ventricular outflow tract
these features were rather unusual in myocardial infarction. obstruction. Clinical manifestation included exertional angina
The ECG demonstrated diffuse ST segment elevation with the and dyspnea, which are not evident in this case. Absence of
exception of aVR. Given the scenario of acute chest pain with left ventricular hypertrophy by voltage criteria is uncommon in
ST elevation, the differential diagnoses included acute inferior HCM. Overt hypothyroidism instead of hyperthyroidism could
STEMI, acute pericarditis and acute aortic dissection with flap associate with circumferential pericardial effusion.
extension to right coronary artery. Blood tests like cardiac
enzymes, D-dimer and even urgent CT aortogram/pulmonary 4.C
angiogram are reasonable investigations to order but are
time-consuming to process. Thus, the point-of-care focus The first line treatment for acute pericarditis should be
echocardiography allowed us to make an instant diagnosis, non-steroidal anti-inflammatory drug (NSAID) preferably
i.e. absence of regional wall motion abnormalities (RWMA) indomethacin and ibuprofen if there were no contraindication
+/-presence of pericardial effusion together with diffuse ST like NSAID allergy and active gastrointestinal bleeding. The
elevation basically confirmed the diagnosis of acute pericarditis. recommended dosage would be indomethacin 25-50mg
TDS and ibuprofen 400-600mg TDS. Prednisolone should be
2.B reserved as second line treatment in view of risk of relapses
upon tapering and withdrawal. Pericardiocentesis should
The point-of-care focus echo in parasternal long-axis view: be performed in case patient develops cardiac tamponade,
i.e. with hypotension and tachycardia but these features are
not present in this patient. Pericardial fluid aspiration should
be considered if there is suspicion of unknown bacterial or
neoplastic etiology. Percutaneous coronary intervention and
betablocker would be indicated in acute coronary syndrome but
not in pericarditis.
5.B
Colchicine 0.5mg daily is the drug of choice (those less than
70kg) for incessant or recurrent pericarditis as recommended
by the current ESC guideline. It has been proven in the
randomized controlled trial (CORP 1) that colchicine reduced
the risk of recurrent pericarditis by 56% at 18 months. There
is no data to suggest aspirin is superior to other NSAIDs.
Should prednisolone consider as second line therapy, the
RV: Right ventricle; IVS: Interventricular septum; AV: Aortic prescription dosage is 0.25-0.5mg/kg instead of 10mg daily.
valve; LA: Left atrium; MV: Mitral valve; PS: Posterior segment Surgical intervention i.e. pericardiectomy is regarded as last
of left ventricle. P.E.: Pericardial effusion. Ao: Aorta. resort (fourth line), it is indicated only if all the medical therapies
(NSAID, colchicine, steroid, intravenous immunoglobulin,
The most striking abnormality from this parasternal long- azathioprine) have been failed. Psychiatry referral is not
axis view was the presence of pericardial effusion i.e. echo- appropriate in view of persistent pleuritic chest pain and high
lucent (dark) space surrounding the heart. The right ventricle CRP.
was not grossly dilated in the view. To distinguish pericardial
effusion from pleural effusion, the descending aorta was the
landmark structure to identify. As the rule of thumb, pericardial
effusion should be anterior to descending aorta which was Reference
shown clearly in the image, whereas pleural effusion should be
posterior to descending aorta. 1. Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis
and management of pericardial diseases: the Task Force for the Diagnosis
3.D and Management of Pericardial Diseases of the European Society of
Cardiology (ESC) endorsed by: the European Association for Cardio-
According to diagnostic criteria of European Society of Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.
Cardiology (ESC), this patient fulfilled at least three out of four 2. Snyder M, Bepko J, White M. Acute Pericarditis: Diagnosis and
criteria which included pleuritic chest pain, pericardial rub and Management. Am Fam Physician. 2014;89(7):553-560.
pericardial effusion although the ST elevation from this ECG 3. Markel G, Imazio M, Brucato A, et al. Prevention of recurrent pericarditis with
colchicine in 2012. Clin Cardiol. 2013 Mar. 36:125-8.
may not be the classical one. Stress cardiomyopathy, i.e.
4. Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for
apical ballooning syndrome, is rather unlikely as there was no acute pericarditis. N Engl J Med 2013;369:1522-8.
“paradoxical” dilatation of apex in systole as suggested by the 5. Imazio M, Brucato A, Cemin R, et al. Colchicine for recurrent pericarditis
(CORP): a randomized trial. Ann Intern Med 2011;155:409-14..
The content of the December ECG Series is provided by:
Dr. KAM Ka Ho, Kevin
MBChB (CUHK), FHKAM (Medicine), Specialist in Cardiology
6 HKMA CME Bulletin
www.hkmacme.org
Dermatology
Dermatology Series for January 2019 is provided by:
Dr. LEUNG Wai Yiu, Dr. TANG Yuk Ming, William, Dr. CHAN Hau Ngai, Kingsley,
Dr. KWAN Chi Keung and Dr. CHANG Mee, Mimi
Specialists in Dermatology & Venereology
Complete Dermatology case,
0.5 Dermatology will be awarded for
at least 2 correct answers in total
A girl with rough nails for one year
A 11-year-old girl presented with a one-year history of progressive
‘rough nails’ which raised her parent’s concern. The girl had no
history of other skin diseases such as lichen planus, psoriasis, eczema
or alopecia areata, and her family history was unremarkable. On
examination, she had sandpaper-like nails and small superficial pits on
all her finger nails.
Q&A
Please answer ALL questions
Answer these on page 11 or make an online submission at: www.hkmacme.org
1. What is the clinical diagnosis? 3. What other parts of body would you examine ?
A. Onychomycosis A. Scalp and hair
B. Lichen planus B. Oral mucosa
C. Psoriasis C. Complete skin examination
D. Trachyonychia D. All of the above
2. Who tend to be most likely affected by this skin 4. What is the most appropriate treatment for this
disease? patient?
A. Children A. Reassurance
B. Adult male B. Oral anti-fungal drug
C. Those with positive family history or affected C. Intralesional steroid to the nail fold or systemic
monozygotic twins corticosteroids.
D. Elderly D. Phototherapy such as topical PUVA (psoralen
and ultraviolet A therapy)
December Answers
1. C 2. A
The diagnosis are Fordyce Spots. Fordyce spots Fordyce spots can be diagnosed clinically with no
are a variant of sebaceous glands. They may further investigation needed.
present at birth but become bigger after puberty.
3. False
Fordyce spots are small yellowish or white papules
or spots that can appear on vermillion border of the Fordyce spots is benign variant of sebaceous
lips, the glans or shaft of the penis, or the vulva of glands and will not progress to cancer.
the female. 4. E
Fordyce spots are harmless and therefore no
further treatment is needed. Different treatment
modalities including CO 2 laser surgery,
electrosurgery, surgery and oral retinoid can help
to improve the condition.
Dermatology Series for December 2018 is provided by:
Dr. CHAN Hau Ngai, Kingsley, Dr. TANG Yuk Ming, William, Dr. KWAN Chi Keung,
Dr. LEUNG Wai Yiu and Dr. CHANG Mee, Mimi
Specialists in Dermatology & Venereology
www.hkmacme.org HKMA CME Bulletin 7
HKMA CME Lecture Online Scheme 2019 Policy
To facilitate members in joining CME Lectures, the HKMA launched the HKMA CME Lecture Online Scheme. The Medical
Council of Hong Kong approved that by viewing the lecture in real-time and completing the online quiz, CME points will be
counted as attending the lecture physically under the “CME Programme for Practising Doctors who are not taking CME
Programme for Specialist.” for non-specialists.
Step 1
Add “HKMA CME Live” as Facebook friend
Step 2
Fill in Online Registration Form using HKMA website/Scan QR Code on CME Bulletin
(Must provide Facebook Account Name and Email)
Step 3
Receive an email with Facebook Group URL
Join group by clicking the URL and press “request to join group”
(Please join the group 3 days before the online lecture)
Step 4
HKMA will approve doctors’ request to join the group 2 days before the lecture
Step 5
Watch Real-time live broadcast at designated time
Step 6
Complete lecture quiz (10 Q&A) and answer questions within two hours after the lecture
Step 7
Receive CME point(s) if doctors completed the quiz online with at least 70% correct
Policy for HKMA CME Lecture Online Scheme
1. As approved by the Medical Council of Hong Kong, the CME Accreditation for CME Lecture Online is for non-
specialists only.
2. Doctors must have a Facebook Account to join the CME Lecture Online.
3. Registration can be done by scan the QR code on CME Bulletin Cover and complete the online form or registration
through HKMA website
4. Doctors can either attend in person or watch lecture online at one point in time.
5. Doctors must watch the lecture at real time
6. Doctors should complete lecture quiz within 2 hours after the lecture. Late submission of the quiz will not be
accepted. 1 CME point will be awarded for doctors with 70% or above correct answer afterward.
7. One Facebook Group is intended for one specific CME Lecture only. Doctors must register with the HKMA
Secretariat for specific lecture and email will be sent to doctors for joining the Facebook group and to gain CME
point.
8. You are recommended to connect to Wi-Fi on your mobile device or computer while watching the lecture through
Facebook Live. Unstable internet connection will cause interruption to your viewing.
9 In case of technical issue and broadcast interruption, please be patient while our technicians will work on fixing the
problem; the video should resume in a few minutes.
10. Due to copyright issue, the Facebook group is exclusive for doctors who have registered; and the video recording,
PowerPoint slides and quiz link MUST not be shared with non-registrants.Answer Sheet
January 2019
ANSWER SHEET
SPOTlight
at least five
1 2 3 4 5 6 7 8 9 10
Cardiology Dermatology
at least two at least two
A maximum of 20 points
1 2 3 4 1 2 3 4 can be awarded for self-
study per year and no
upper limit of CME points
for attending CME lectures
CME Physical Lecture Policy and Procedure
Registration Information for Participants
1. Please complete the reply slip and return to HKMA Secretariat in Special weather arrangement
person or by fax/mail/email. When Tropical Storm Warning Signal No. 8 (or above) or a
2. Enrollment priorities will be given to doctors who have purchased Black Rainstorm Warning Signal is in force within 3 hours of the
packages. For Community Network Lectures, priorities will be commencement time, the relevant CME function will be cancelled. (i.e.
given to doctors from that Community Network with Packages, CME starting at 2:00 pm will be cancelled if the warning signal is hoisted
then doctors from that Community Network. or in force any time between 11:00 am and 2:00 pm).
3. No walk in or on-site payment will be accepted. Attendance
without registration will not be recognized and CME point will not The function will proceed as scheduled if the signal is lowered three
be accredited. hours before the commencement time. (i.e. CME starting at 2:00 pm
4. Please ensure that your registration is confirmed before attending will proceed if the warning signal is lowered at 11:00 am, but will be
lecture. Only successfully registered doctors who paid could cancelled even if it is lowered at 11:01 am).
attend the lecture.
5. The HKMA Secretariat will notify doctors who have successfully When Typhoon No. 8 Signal or a Black Rainstorm signal is in force
enrolled to arrange for payment. If doctors have not arranged for after CME commencement, announcement will be made depending on
payment within a specified period after the notification, the seat the conditions as to whether the CME will be terminated earlier or be
will be released to doctors on waiting list without further notice. conducted until the end of the session.
Payment The above are general guidelines only. Individuals should decide on
1. All HKMA CME lectures that involve registration and enrollment their CME attendance according to their own transportation and work/
through the HKMA would require the collection of lecture fee home location considerations to ensure personal safety.
(unless otherwise specified).
2. The lecture fee is $50 for HKMA members and $100 for non- General lecture policy
members per lecture. 1. Doctor should sign for own CME.
3. Cash payments have to be paid in person at HKMA Secretariat 2. Registration will cease when Q & A Session starts.
and cheque payments have to be mailed or paid in person at 3. No recording unless permission is granted by the HKMA.
HKMA Secretariat. 4. The HKMA will investigate when non-compliance at CME Session
4. Fee can be paid together in one cheque for lecture within the is reported, further action will be considered to ensure all CME
same month. Only combined cheque payment for not more than activities are properly held.
2 packages will be accepted. 5. For enquiries, please contact the CME Department of the HKMA
5. No refund or transfer will be allowed after payment is made. Secretariat at 2527-8452.
Payment cannot be transferred to other lectures or for other
specified doctors.Advertorial
Professor Ivan Fan Ngai HUNG
Update on Influenza Clinical Professor
Chief, Division of Infectious Diseases,
Vaccination – Herd Department of Medicine
Li Ka Shing Faculty of Medicine
The University of Hong Kong
Immunity, Immunogenicity
and Heterologous Protection
The Hong Kong Medical Association (HKMA) severity was high in all age groups (children, adults
organized a Continuous Medication Education (CME) and elderlies).6 The epidemic was likely a result of the
programme lunch lecture on October 31, 2018 Singaporean strain migrating to the US, which was
entitled Update on Influenza Vaccination, which was not contained in the flu shots then. In Hong Kong last
sponsored by AstraZeneca Hong Kong. Professor year, there was a large summer peak that caused
Ivan Fan Ngai Hung (Specialist in Infectious Disease, 400-500 deaths, 7 again likely exacerbated by an
Clinical Professor, Department of Medicine, Li Ka antigenic mismatch. According to Prof. Hung, since
Shing Faculty of Medicine, The University of Hong there had not been a summer peak this year, a large
Kong) spoke on the latest key issues in influenza winter surge might be expected.
vaccination, which include strategies for reducing
infections, hospitalizations and deaths, enhancing Reducing Infections, Hospitalizations and
immunogenicity, and achieving heterologous protection. Deaths: Herd Immunity
Latest Worldwide Challenges: Rising Mortality Different kinds of vaccines are available for
and Antigenic Mismatch influenza prevention, including the common
inactivated quadrivalent intramuscular vaccines,
In terms of influenza-related mortality worldwide, the the life-attenuated intranasal vaccines (LAIVs), and
World Health Organization (WHO) has increased the recombinant vaccines (in the US). The questions are
estimate to up to 650,000 deaths annually.1 For last which to use and on what target populations. The
year, 2017-2018, the US Centers for Disease Control LAIVs have demonstrated high efficacy in young
and Prevention (CDC) estimated 79,400 deaths from children aged 6 months to 7 years (compared with
influenza.2 In Hong Kong, seasonal influenza caused placebo in trials and with inactivated vaccines in a
501 reported deaths in Winter 2015 alone. 3 High- meta-analysis), 8 and the intranasal administration
risk populations such as elderlies, infants aged ≤2, is suitable for children who may be more repelling
patients with chronic illnesses (e.g. heart condition against needle injections. In the US, LAIVs were not
or diabetes) and smokers are particularly vulnerable. immunogenic for the 2015-2016 Bolivian strain, 9
There are also the continuous threats of antigenic but are recommended by the CDC this year. 10
shifts (esp. in the hemagglutinin H1 and H3 families) Contraindications include egg allergy (as in other
and the emergence of new subtypes (esp. from the inactivated vaccines), aspirin therapy and Reye
H5 and H7 families). In combating against influenza syndrome; precautions may include pregnancy or
epidemics, some major concerns are that i) people a weakened immune system (e.g. post-transplant
are at risk but not immunized, ii) protection from recipients).11
vaccination may not last through to the summer
peak season (particularly among elderlies), and iii) the According to Prof. Hung, the best influenza
circulating seasonal influenza subtype may not match prevention strategy would be universal vaccination;
with that of the vaccine. while it is not yet feasible, a newer notion of protection
involves herd immunity. The idea is that vaccinating
Since the 1960s, the US have established continuous children, in particular kindergarten and primary school
surveillance on the impact and burden of influenza,4 children, may block influenza transmission from
which now includes monitoring three major indicators: within schools toward families (including to parents
outpatient visits, hospitalizations and deaths from and grandparents) and communities. This was
influenza-like illnesses. While the US CDC estimated demonstrated in a 2010 study in Alberta, Canada in
that vaccination prevented 5 million illnesses and the relatively close Hutterite communities.12,13 A total
71,000 hospitalizations in 2015-2016, 5 in 2017- of 947 children and adolescents aged 36 months to
2018, for the first time ever, the estimated influenza 15 years (83% coverage) received the study vaccine
12 HKMA CME Bulletin
www.hkmacme.orgAdvertorial
and 2,326 received placebo (hepatitis A vaccine; 79% – Children may be administered the life-attenuated
coverage). Among non-recipients in the communities, intranasal spray vaccine, without the need of
3.1% vs. 7.6% had confirmed influenza illness (by using needles.
RT-PCR), for a protective effectiveness of 61%
(95% confidence interval: 8-83%, p = 0.03). More – For enhancing immunogenicity in elderlies and
recently, the UK childhood LAIV programme offered protection in case of antigenic drifts, strategies
universal vaccination to children aged 2-11 in certain include using i) an immunologic adjuvant, ii)
pilot areas,14 and found that cumulative emergency a high-dose vaccine, or iii) topical imiquimod
department respiratory attendances, influenza- before intradermal vaccination.
confirmed hospitalisations and intensive care unit
admissions were consistently lower (although mostly
non-significantly), in both targeted and non-targeted
age groups compared with non-pilot areas. References
1. World Health Organization. https://www.who.int/mediacentre/news/
Enhancing Immunogenicity and Heterologous statements/2017/flu/en/. Last accessed: Nov 8, 2018.
Protection 2. US Centers for Disease Control and Prevention. https://www.cdc.gov/flu/
about/burden/estimates.htm. Last accessed: Nov 8, 2018.
As mentioned, enhancing immunogenicity has 3. Department of Health. https://www.dh.gov.hk/english/press/2016/160128.
html. Last accessed: Nov 8, 2018.
been an old problem in influenza vaccination, which
4. US Centers for Disease Control and Prevention. https://www.cdc.gov/flu/
is particularly important for elderlies. Prof. Hung about/burden/index.html. Last accessed: Nov 8, 2018.
discussed several strategies for tackling with the 5. US Centers for Disease Control and Prevention. https://www.cdc.gov/flu/
issue. First, the use of an adjuvant with trivalent about/disease/2015-16.htm. Last accessed: Nov 8, 2018.
inactivated influenza vaccine had been reported to 6. US Centers for Disease Control and Prevention. https://www.cdc.gov/flu/
about/season/flu-season-2017-2018.htm. Last accessed: Nov 8, 2018.
increase effectiveness by about 20-30%.15 Second,
7. Centre for Health Protection, Department of Health. Flu Express.
high-dose vaccine (at 4 times normal dosage) had 15(5). Available at: https://www.chp.gov.hk/files/pdf/fluexpress_
been shown to increase immunogenicity by about week05_08_02_2018_eng.pdf. Last accessed: Nov 8, 2018.
twofold, 16 but at an increased cost. Third, Prof. 8. Osterholm T, Kelley S, Sommer A, Belongia A. Effcacy and effectiveness of
Hung and colleagues had performed studies that influenza vaccines: a systematic review and meta-analysis. Lancet Infectious
Disease. 2012;12:36-44.
applied topical imiquimod before administering the
9. Pebody R, McMenamin J, Nohynek H. Live attenuated influenza vaccine
intradermal trivalent vaccine. In a prospective trial (LAIV): recent effectiveness results from the USA and implications
of 91 participants (mean age 73), 17 the approach for LAIV programmes elsewhere. Archives of Disease in Childhood.
demonstrated an increased seroconversion rate 2018;103(1):101-105.
10. Grohskopf LA, Sokolow LZ, Fry AM, et al. Update: ACIP recommendations
(compared with an aqueous cream) that was
for the use of quadrivalent live attenuated influenza vaccine (LAIV4) — United
sustained from day 7 to year 1 (p < 0.001) and was States, 2018–19 influenza season. Morbidity and Mortality Weekly Report.
associated with fewer hospitalizations for influenza or 2018;67(22):643-645.
pneumonia (p < 0.05). Imiquimod is a toll-like receptor 11. FluMist Quadrivalent [prescribing information RAL-FLUQV7]. Gaithersburg,
MD, USA: MedImmune; 2018.
7 agonist that attracts dendritic cells, which likely
12. Loeb M, Russell M, Moss L, et al. Effect of influenza vaccination of children
enhanced antigen presentation and downstream on infection rates in Hutterite communities. JAMA. 2010;303(10):943-950.
T-cell and B-cell activation at local lymph nodes.17 In 13. Wang B, Russell M, Moss L, et al. Effect of influenza vaccination of children
a further phase 2b/3 trial (n = 160), topical imiquimod on infection rate in Hutterite communities: follow-up study of a randomized
and intradermal vaccination were found to also trial. PLoS ONE. 2016;11(12):e0167281.
significantly improved immunogenicity against non- 14. Pebody R, Sinnathamby M, Warburton F, et al. Uptake and impact of
vaccinating primary school-age children against influenza: experiences
vaccine strains, such as the antigenically drifted H3N2 of a live attenuated influenza vaccine programme, England, 2015/16.
strain of 2015 that was not included in the 2013-2014 Eurosurveillance. 2018;23(25):1700496.
recommended vaccine.18 15. Vesikari T, Knuf M, Wutzler P, et al. Oil-in-water emulsion adjuvant with
influenza vaccine in young children. New England Journal of Medicine.
2011;365(15):1406-1416.
Summary Points 16. DiazGranados CA, Dunning AJ, Kimmel M, et al. Efficacy of high-dose
versus standard-dose influenza vaccine in older adults. New England Journal
– Where universal vaccination is not yet of Medicine. 2014;371(7):635-645.
achievable, data have shown that vaccinating 17. Hung F, Zhang J, To K, et al. Immunogenicity of intradermal trivalent
influenza vaccine with topical imiquimod: a double blind randomized
school children reduced overall influenza controlled trial. Clinical Infectious Diseases. 2014;59(9):1246-1255.
infections and related hospitalizations in the 18. Hung F, Zhang J, To K, et al. Topical imiquimod before intradermal trivalent
community. influenza vaccine for protection against heterologous non-vaccine and
antigenically drifted viruses: a single-centre, double-blind, randomised,
controlled phase 2b/3 trial. Lancet Infectious Diseases. 2016;16(2):209-218.
www.hkmacme.org HKMA CME Bulletin 13CMEnotifications
CME Lectures in February 2019
Organizer/ : HKMA New Territories West HKMA Hong Kong East Community Network and
Co-organizer Community Network Primary Care Office of Department of Health (DH)
Date : Thursday, 21 February 2019
Topic : The Current Situation and Latest An Overview of Common Developmental
Management of Nasopharyngeal Carcinoma Problems in Children
in Hong Kong
Speaker : Dr. LAM Wing Hung, Eddy Dr. LEE Mun Yau, Florence
Specialist in Otorhinolaryngology Consultant Paediatrician,
Child Assessment Service, DH
Time : 1:00 – 2:00 p.m. Registration & Lunch
2:00 – 2:45 p.m. Lecture
2:45 – 3:00 p.m. Q&A Session
Venue : Atrium Function Room, Lobby Floor, The HKMA Wanchai Premises
Hong Kong Gold Coast Hotel, 1 Castle Peak Road, 5/F, Duke of Windsor Social Service Building,
Gold Coast, Hong Kong 15 Hennessy Road, Wanchai
( )
Moderator : Dr. CHEUNG Kwok Wai, Alvin Dr. YIP Yuk Pang, Kenneth
Chairman, Vice-chairman (In.),
HKMA NTW Community Network HKMA Hong Kong East Community Network
Deadline : Friday, 8 February 2019
Fee : $50 – Member; $100 – Non-member Free-of-charge (For Members only)
Capacity & : Capacity is 50 Capacity is 80
Registration
Registration is strictly required on a first come, first served basis. Priority will be given to doctors
practising in NTW districts/HKE districts.
Enquiry : Miss Antonia LEE Ms. Candice TONG
: Tel: 2527 8285. *Please call and confirm that your facsimile has been successfully transmitted to the
HKMA Secretariat if you do not receive confirmation 7 days before the event.
CME Accreditation : Each of the lectures carries 1 CME point under the MCHK/HKMA CME Programme.
Accreditation from various colleges is pending.
REPLY SLIP
HKMA New Territories West & Hong Kong East Community Networks Fax: 2865 0943
CME Lectures in February 2019 Please “✓” as appropriate
I would like to register for the following lecture(s).
PAYMENT METHOD
21 February 2019 (NTW) 21 February 2019 (HKE) The payment shall be made by: (please indicate one of the following
Name: payment methods, you may refer to p.11 for terms and conditions)
HKMA No.:
Cash Cheque Lecture Package
Preferred means of communication#:
Practising location:
Mobile No. (SMS): OR
In New Territories West districts (Please specify *: )
In Hong Kong East districts (Please specify *: ) E-mail:
#
Others (Please specify: ) Please fill in your updated mobile number or email address so that you can be
notified of your application via SMS/email.
* Null entry will be treated as non- NTW or HKE member registration.
Signature: Date:
Data collected will be used and processed for the purposes related to these events only.
14 HKMA CME Bulletin
www.hkmacme.orgCME Facebook Live
CMEnotifications
CME Lectures in February 2019
Organizer : HKMA Central Western & Southern Community HKMA Kowloon East Community Network
Network
Date : Wednesday, 20 February 2019 Thursday, 21 February 2019
Topic : Physiotherapy for Common Orthopaedic Improving Dyslipidaemia Management: An
Conditions (Part 2) Update on International Guideline and More
Speaker : Dr. WONG Kam Hung, Francis Dr. CHEUNG Ling Ling
Consultant Physiotherapist Specialist in Cardiology
Time : 1:00 – 2:00 p.m. Registration & Lunch
2:00 – 2:45 p.m. Lecture
2:45 – 3:00 p.m. Q&A Session
Venue : The HKMA Central Premises, V Cuisine, 6/F., Holiday Inn Express Hong Kong
Dr. Li Shu Pui Professional Education Centre, Kowloon East, 3 Tong Tak Street, Tseung Kwan O
2/F., Chinese Club Building,
21-22 Connaught Road, Central
Moderator : Dr. TSANG Chun Au Dr. CHU Wen Jing, Jennifer
Hon. Treasurer, Hon. Secretary,
HKMA CW&S Community Network HKMA Kln East Community Network
Deadline : Monday, 11 February 2019
Fee & : $50 – Member; $100 – Non-member. Capacity is 80 for CW&S and Capacity is 48 for Kln East.
Capacity Registration is strictly required on a first come, first served basis. Priority will be given to doctors
practising in CW&S (20 Feb)/ Kln East districts (21 Feb)
Facebook : Please scan the QR code on cover page
registration
Enquiry : Miss Antonia LEE, Tel: 2527 8285
*Please call and confirm that your facsimile has been successfully transmitted to the HKMA
Secretariat if you do not receive confirmation 7 days before the event.
Sponsor :
CME Accreditation : Each of the lectures carries 1 CME point under the MCHK/HKMA CME Programme.
Accreditation from various colleges is pending.
REPLY SLIP
HKMA CW&S & Kln East Community Networks Fax: 2865 0943
CME Lectures in February 2019 Please “✓” as appropriate
I would like to register for the following lecture(s):
PAYMENT METHOD
20 February 2019 (CW&S) 21 February 2019 (Kln East) The payment shall be made by: (please indicate one of the following
Name: payment methods, you may refer to p.11 for terms and conditions)
HKMA No.:
Cash Cheque Lecture Package
Preferred means of communication#:
Practising location:
Mobile No. (SMS): OR
In Central, Western & Southern districts (Please specify *: )
In Kowloon East districts (Please specify *: ) E-mail:
#
Others (Please specify: ) Please fill in your updated mobile number or email address so that you can be
notified of your application via SMS/email.
* Null entry will be treated as non-CW&S or Kln East member registration.
Signature: Date:
Data collected will be used and processed for the purposes related to these events only.
www.hkmacme.org HKMA CME Bulletin 15CMEnotifications
Antibiotic Stewardship Programme in Primary Care
Co-organizers : HKMA Yau Tsim Mong HKMA Kowloon City HKMA Kowloon West
Community Network Community Network Community Network
and The Centre for Health Protection (CHP) of the Department of Health (DH)
Date : Tuesday, 19 February 2019 Friday, 22 February 2019 Tuesday, 26 February 2019
Speaker : Dr. Leo LUI
Associate Consultant, Infection Control Branch, CHP, DH
Time : 1:00 – 2:00 p.m. Registration & Lunch
2:00 – 2:45 p.m. Lecture
2:45 – 3:00 p.m. Q&A Session
Venue : Crystal Ballroom, 2/F, President’s Room, Spotlight Fulum Palace, Shop C,
The Cityview Hong Kong, Recreation Club ( ), 4/F., G/F, 85 Broadway Street,
23 Waterloo Road, Kowloon Screen World, Site 8, Whampoa Mei Foo Sun Chuen
Garden, Hunghom, Kowloon
Moderator : Dr. HO Kit Man, Carmen Dr. CHAN Man Chung, JP Dr. LEUNG Gin Pang
Committee Member, District Coordinator, HKMA Hon. Treasurer
HKMA YTM Community Network Kln City Community Network HKMA Kln West Community
Network
Deadline : Friday, 1 February 2019 Monday, 4 February 2019 Friday, 8 February 2019
Fee : Free-of-charge (For Members only)
Capacity : Capacity is 80 Capacity is 36 Capacity is 60
Registration is strictly required on a first come, first served basis. Priority will be given to doctors
practising in YTM districts (for lecture on 19 Feb)/Kln City districts (for lecture on 22 Feb)/Kln West
districts (for lecture on 26 Feb).
Enquiry : Ms. Candice TONG Miss Antonia LEE
Tel: 2527 8285. Please call and confirm that your facsimile has been successfully transmitted to the
HKMA Secretariat if you do not receive confirmation 7 days before the event.
CME Accreditation : Each of the lectures carries 1 CME point under the MCHK/HKMA CME Programme.
Accreditation from various colleges is pending.
REPLY SLIP
HKMA YTM, Kln City & Kln West Community Networks Fax: 2865 0943
Antibiotic Stewardship Programme in Primary Care
I would like to register for the following lecture(s).
19 February 2019 (YTM) 22 February 2019 (KC) 26 February 2019 (KW)
Name: HKMA No.:
#
Mobile No. (SMS): OR # E-mail:
#
Please fill in your updated mobile number or email address so that you can be notified of your application via SMS/email.
Practising location:
In Yau Tsim Mong districts (Please specify *: )
In Kln City districts (Please specify *: )
In Kln West districts (Please specify *: )
Others (Please specify: )
* Null entry will be treated as non-Yau Tsim Mong or Kowloon City or Kowloon West member registration.
Signature: Date:
Data collected will be used and processed for the purposes related to these events only.
16 HKMA CME Bulletin
www.hkmacme.orgMeeting Highlights
HKMA-HKSH CME Programme 2018-2019 The HKMA Central, Western and Southern Community Network (CW&SCN) ~
“Update in Medical Practice” Dr. YIK Ping Yin
Dr. YAM Chun Yin (right) presenting a souvenir to the Group photo taken during the lecture on 5 December 2018 Group photo taken during the lecture on 19 December 2018
speaker Dr. NG Ping Wing (left) during the lecture on 4 From left: Dr. POON Man Kay (moderator), Dr. YIK Ping Yin, From left: Dr. POON Man Kay, Dr. Leo LUI (speaker), Dr. LAW Yim Kwai
December 2018. Prof. Francis WONG (speaker) and Dr. LAW Yim Kwai and Dr. TSANG Chun Au (moderator)
The HKMA Hong Kong East Community Network (HKECN) ~ The HKMA Kowloon East Community
Dr. CHAN Nim Tak, Douglas Network (KECN) ~ Dr. AU Ka Kui, Gary
Dr. Michele YUEN (left, speaker) receiving the souvenir from Dr. Simon Dr. Kenneth YIP (left, moderator) presenting the souvenir to Dr. LAU Dr. Gary AU (left, moderator) presenting the souvenir to Dr. Samuel
AU (moderator) during the lecture on 6 December 2018 Ching Wa (speaker) during the lecture on 20 December 2018 LEE (speaker) during the lecture on 6 December 2018
The HKMA New Territories West Community Network (NTWCN) ~
Dr. CHEUNG Kwok Wai, Alvin
Dr. Ivan SHIU (right, moderator) presenting the souvenir to Dr. WONG
King Ying (speaker) during the lecture on 13 December 2018
Dr. LEE Shin Cheung (left, moderator) presenting the souvenir to Dr. Group photo taken during the lecture on 13 December 2018
CHEUNG Ling Ling (speaker) during the lecture on 6 December 2018 From left: Dr. Alvin CHEUNG (moderator), Dr. Leo LUI (speaker),
Dr. TSANG Yat Fai and Dr. Lambert CHAN
The HKMA Tai Po Community Network
The HKMA Kowloon West Community Network (KWCN) ~ (TPCN) ~ Dr. CHIU Sik Ho, Bonba
Dr. TONG Kai Sing
Dr. Bernard CHAN (left, moderator) presenting the souvenir to Dr. Group photo taken during the lecture on 11 December 2018 Dr. CHOI Kin (right) presenting the souvenir to Dr. Patrick CHOW (speaker)
TAM Wing Kei (speaker) during the lecture on 4 December 2018 From left: Dr. Bernard CHAN, Dr. Gabriel YIP (speaker), Dr. LAM Ngam during the lecture on 4 December 2018
(moderator) and Dr. LEUNG Gin Pang
www.hkmacme.org HKMA CME Bulletin 17You can also read