SURVEY OF HEALTH SERVICES FOR PEOPLE WITHOUT SECURE HOUSING NORTHERN NSW - A survey conducted by the Homelessness Action Group under the ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
SURVEY OF HEALTH SERVICES
FOR PEOPLE WITHOUT SECURE HOUSING
NORTHERN NSW
A survey conducted by the Homelessness Action Group under the leadership of the North Coast NSW
Alliance to Improve Services to Vulnerable Members of the Community
ACKNOWLEDGEMENT
The North Coast NSW Alliance to Improve Services
to Vulnerable Members of the Community (the
Alliance) appreciates the contribution of all the
members of the Homelessness Action Group.
DISCLAIMER
The Homelessness Action Group has taken
reasonable steps to ensure the information
contained in this report, Survey of Health Services
for People Without Secure Housing, Northern
NSW, August 2014, is accurate and up-to-date and
is not responsible for any errors or omissions in
the content and reserves the right to revise or add
to the content at any time without notice to you.
No part of this report may be reproduced,
transmitted, stored in a retrieval system or
adapted in any form or by any means (electronic,
mechanical, photocopying, recording or otherwise)
without permission of North Coast NSW Medicare
Local (NCNSWML).
RECOMMENDED CITATION
North Coast NSW Medicare Local, Survey of Health
Services for People Without Secure Housing
Northern NSW, August 2014
ENQUIRIES
Enquiries should be addressed to Manager,
Strategic Development and Program Design,
NCNSWML by emailing planning@ncml.org.au
2
CONTENTS
Page
ACKNOWLEDGEMENT 2
EXECUTIVE SUMMARY 4
INTRODUCTION 6
BACKGROUND 6
SURVEY DESIGN AND HOW IT WAS CONDUCTED 7
FINDINGS OF THE SURVEY 8
Sample of Respondents 8
Responses from the Homelessness and Community Services Sector 8
Responses from Services that are Primarily Health Care 17
DISCUSSION 27
CONCLUSION 29
APPENDICES
Appendix 1 – North Coast NSW Alliance to Improve Services to the Vulnerable 30
Members of the Community Memorandum of Understanding
Appendix 2 – Diagrammatic Representation of Alliance and Action Groups 33
Appendix 3 – Homelessness Action Group Terms of Reference 34
Appendix 4 –Survey Questionnaire 36
Appendix 5 – Summary of Responses to the open ended questions 46
3
support services for people without secure
EXECUTIVE SUMMARY housing. Of the 289 responses, 54.7% were
received from the health care sector and 45.3%
The Survey on Health Services for People without from the homelessness and community services
Secure Housing, Northern NSW was conducted by sector, representing a relatively even response
the Homelessness Action Group (HAG) which was from the two sectors. Issues covered include
established by the North Coast NSW Alliance to accessibility to health services, information
Improve Services to the Vulnerable Members of the needed, problems encountered, communications
Community (The Alliance) in May 2014. and suggestions for improvements. The open
ended questions provided opportunity for
The Alliance was established under a respondents to provide detailed information about
memorandum of understanding between barriers, challenges and solutions demonstrating
Northern NSW Local Health District (NNSWLHD), the multi-faceted complexities in providing
the Department of Family and Community Services effective health care.
(FACS) and North Coast NSW Medicare Local
(NCNSWML) in October 2013.
KEY FINDINGS
The Terms of Reference articulate a vision of
• Barriers to accessing health care include cost,
“fostering a response to the needs waiting times, transport, lack of services and
of the vulnerable members of the lack of understanding about the health system
North Coast community that is and fear of judgement.
client centred, multi-sectoral and • Inability to identify a home address made it
is integrated and cohesive where difficult to secure appointments, particularly
services are provided”. (See where these were notified by mail and also on
Appendix 1) the ability to provide outreach services.
• Agencies found some health care services
easier to work with than others, citing quality
The Alliance established the Homelessness Action
of service delivery, staff attitudes and
Group to
understanding of homelessness, accessibility,
communication and collaborative work
“drive action and empower
practices as key to effective working
people experiencing or at risk of
relationships.
homelessness and those delivering
• Generally, only a small proportion of health
services to facilitate change”(See
care services always provided agencies with
Appendix 2).
sufficient and detailed information required to
assist clients.
• The survey highlighted a lack of clarity
The Survey of Health Services for People without
around ‘who to contact’. Communication
Secure Housing Northern NSW, was collaboratively
designed and widely distributed with the support difficulties between agencies was a
of both the health and homelessness support commonly identified and identified the need
services sectors. It was developed to better for an improved mechanism to share
understand the barriers in the health sector for information on
people without secure housing and the challenges o clients and their healthcare needs
experienced by workers planning and delivering
o availability of support services and
care and support. The scope of the survey included
hospital inpatient and emergency services, pathways
community based services and primary health care o access to emergency housing
services including general practice as well as a o social workers or care workers who
wide range of agencies providing housing and could assist navigating the
other support to people without secure housing. healthcare or social housing sector.
• A consistent theme was the perception that
The survey was administered via the on-line survey
health services were not sensitive to the
tool, Survey Monkey. It comprised 26 questions
including 12 open ended questions directed at trauma experienced by people without
informants from organisations that primarily secure housing and didn’t understand the
provide health care services and those providing problems they encountered. It was reported
4
that this impacted upon the clients
perception of being judged or discriminated
against, and also the ability of healthcare
workers to deliver effective client centred
health care.
The survey provides an indicator of the difficulties
faced in accessing and delivering healthcare
services for people without secure housing. It will
shape the work of the HAG, identify areas for
further consultation and inform the development
of a regional action plan to improve health care
services to people without secure housing. It also
provides a base line to monitor progress over time.
It is hoped it will inform the work of other agencies
in the region and provide the catalyst for further
discussion and investigation.
5
from the health and homelessness and community
INTRODUCTION services sectors. (See Appendix 3)
This report has been compiled under the The Homelessness Action Group quickly identified
leadership of the North Coast NSW Alliance to
the limited data relating to homelessness and in
Improve Services to Vulnerable Members of the
Community (the Alliance). particular, the barriers to people accessing health
care and that currently, the majority of work
The Homelessness Action Group (HAG) is one of focuses on housing. To better understand the
the action groups formed out of the Alliance and barriers in the health sector for people without
convened by North Coast NSW Medicare Local secure housing and the challenges experienced by
(NCNSWML).
health and community service workers planning
and delivering care, the Survey on Health Services
This report, developed by the HAG, provides an
for People without Secure Housing Northern NSW
overview of the results of the on-line Survey of
was developed.
Health Services for People without Secure Housing,
Northern NSW, over the period 11 April to 6 May The survey was collaboratively designed and
2014. This work has been led by NCNSWML and widely distributed with the support of both the
members of the Alliance’s Homelessness Action health and homelessness support services sectors.
Group. It was developed to better understand the barriers
in the health sector for people without secure
The survey has been well supported by both health housing and the challenges experienced by health
services and the homelessness and support workers planning and delivering care and targeted
those supporting the health and housing of these
services agencies.
people, as valuable informants about the problems
encountered by their clients, patients and services.
The scope of the survey included hospital inpatient
BACKGROUND and emergency services, community based
services and primary health care services including
The Alliance was established under a general practice as well as a wide range of
memorandum of understanding (MOU) between agencies providing housing and other support to
Northern NSW Local Health District (NNSWLHD), people without secure housing.
the Department of Family and Community Services
(FACS) and North Coast NSW Medicare Local
(NCNSWML) in October 2013. This MOU
articulates a vision of
“fostering a response to the needs
of the vulnerable members of the
North Coast community that is
client centred, multi-sectoral and
is integrated and cohesive where
services are provided”. (See
Appendix 1)
Central to achieving this vision has been the
establishment of relevant action groups to
respond to these needs. (See Appendix 2) The
Homelessness Action Group was formed in
response to the need for action to support the
health needs of people at risk of, or experiencing,
homelessness. The Terms of Reference for this
group was developed by the current membership
consisting of a variety of regional organisations
6
SURVEY DESIGN AND • whether patients of health care services
are asked about their living situation
HOW IT WAS • what problems are encountered by health
CONDUCTED service providers delivering services to
people without secure housing
The survey was administered via the on-line survey • quality of communication between health
tool, Survey Monkey. It comprised 26 questions services and support services
including 12 open ended questions directed at • suggestions from health care providers on
informants from organisations that primarily how to deliver more effective health care
provide health care services and those providing to people without secure housing
support services for people without secure
housing. (See Appendix 4) Open ended questions were analysed manually by
coding sentences or part sentences and organising
Questions 2 to 11 were directed at organisations into themes. Closed questions are presented
that primarily provide health care services. directly from survey monkey.
Questions 13 to 25 were directed at organisations It should be noted that for some questions
that provide support services for people without
secure housing. (Q2 & 3) respondents were able to select more
than one response. This was unintended. For
Question 12 asked respondents if they would be these questions, the denominator is the number of
prepared to participate in further discussions, and respondents, rather than the number of
those that agreed were asked for their contact responses. This anomaly will be corrected in
details in Question 26. future surveys. Overall, these questions still
provide a good indication of the spread of agencies
The survey was distributed widely by email on 11
responding to the survey.
April 2014 via the Homelessness Action Group
(HAG) network to the Northern NSW Local Health
District, the NSW Department of Family and
Community Services, members of the Northern
Rivers Housing and Homelessness Forum,
Aboriginal Medical Services, General Practitioners
and NCML networks and the not-for-profit sector.
A three week time frame for the survey response
was provided initially, but responses received up
to the date of analysis on 6 May 2014 were
accepted. A follow up reminder email was sent on
29 April 2014.
The main issues covered by the survey include:
• ease or difficulty accessing health services
by both clients and organisations
providing support to them
• the factors that make a health service
easy or difficult to work with
• the information required by a support
organisation from a health service
• suggestions from support organisations
on how to better support people without
secure housing to access health services
7
FINDINGS FROM THE SURVEY
SAMPLE OF RESPONDENTS
Q 1. Is your organisation primarily a health care service?
Responses to the survey were well supported by both the health services and homelessness support services
sectors. A slightly greater response was received from the health care sector (158 responses or 54.7%) than
the homelessness and community services sector (131 responses or 45.3%) (Table 1).
Table 1
Is your organisation primarily a health care service?
Answer Options Response Percent Response Count
Yes (skip to question 12) 54.7% 158
No 45.3% 131
answered question 289
skipped question 1
RESPONSES FROM THE HOMELESSNESS AND COMMUNITY SERVICES SECTOR
Those organisations which were NOT primarily providing health care
(Questions 2 to 11 targeted organisations not primarily providing health care)
Q 2. What is the primary focus of your organisation? (Choose the one that best fits)
The majority of respondents to the survey who are not primarily health care service providers were from:
homelessness, housing and accommodation services; multi focus agencies; family support services; domestic
and family violence and women’s services; and community development/information provision services. Full
details are shown in Table 2.
8
Table 2*
Primary focus of organisation (homelessness and community service provider)
Answer Options Response Percent Response Count
Multi focus agency 28.9% 33
Domestic and Family Violence and Women's Services 7.0% 8
Mainstream eg Centrelink, Legal Aid, Financial Counselling 3.5% 4
Homelessness Housing and Accommodation 37.7% 43
Education and Training 6.1% 7
Family Support 12.3% 14
Children's Services 4.4% 5
Community Development /Information Provision 7.0% 8
Youth 7.0% 8
Other 18.4% 21
*In Q2 & Q3 some respondents selected more than one response. The denominator is the total number of respondents.
Q 3. Please select the statement that best describes your main role?
The majority of homelessness and community services respondents were either front-line service providers
(53.4%), or Managers (29.7%) (Table 3).
Table 3
Main role of respondent (homelessness and community service provider)
Answer Options Response Response Count
Percent
Frontline Service Provider (main role is direct client 53.4% 63
contact and service provision)
Manager 29.7% 35
Administrative Support 5.9% 7
Other 14.4% 17
Q 4. This survey is interested in those clients without secure housing. This may include people
who are living rough, in transient or temporary accommodation or are having difficulty
sustaining their tenancy. In relation to your clients without secure housing, how often do you
encounter people reporting difficulty accessing health care?
The rate of reported difficulty in accessing health care services by people without secure housing is
shown in Table 4 below. 16.3% of organisations (who are not primarily health care providers)
encounter people without secure housing, reporting difficulty accessing health care every day, and
45% report this occurring every week (Table 4).
9
Table 4
How often do homelessness and community services service providers encounter people without secure
housing reporting difficulty accessing health care
Answer Options Response Percent Response Count
Every day 16.3% 13
Every week 45.0% 36
Every month 22.5% 18
Rarely 16.3% 13
answered question 80
skipped question 210
Q 5. What difficulties have they reported regarding access and use of health services?
Sixty four people responded to this open question about the difficulties reported by clients in accessing health
care services.
Key themes were cost, waiting times, transport costs and availability, lack of suitable services, understanding
the health system, homeless people having different priorities, judgment by others, no address for
correspondence, disability access, difficult to provide services when client has no home and security issues.
Some sample responses for the most frequently mentioned themes are provided below. A more detailed list of
sample responses is provided at Appendix 5.
Cost - mentioned 25 times:
“particularly mental health but bulk billing doctors or any type of allied health is very difficult to access;
lack of bulk billing especially in rural areas; lack of funds to pay for any pre-treatment options such as x-
rays”
Waiting times- mentioned 20 times:
“Wait lists for services; high waiting times to access the services presently available; availability of some
specialists; wait lists for mental health; having to wait 3 weeks for an appointment; unable to access
appropriate care in a timely manner”
Transport costs/availability – mentioned 19 times
geographical isolation, inability to use public transport due to mobility or Mental Health issues; unable to
get to services; unable to get to appointment with doctors; lack of transport to broaden options;
Lack of services - mentioned 12 times
“Lack of Drop in Services; lack of services in the Tweed; no General Practitioner (GP); access to mental
health support workers; access to primary health services; mental health and bulk billing; access to
specialist services eg podiatrist, psychologist; health services OK but accessing housing is difficult”
Understanding the health system, age care, cultural barriers – mentioned nine times
“Understanding the aged care system or other health system; not understanding what they need to do to
secure services; knowledge of what exists; lack of knowledge of how to access mental health supports;
lack of cultural awareness by local GPs”
10Different priorities for homeless people – mentioned five times
“Their housing is their main focus and priority – cannot look at health care needs until they secure
housing; inability to remember appointments or work to a calendar/watch”
Judgement by others, fear, shame – mentioned five times
“Judgement by providers; stigma, disempowered by ‘client/health provider’ relationship”
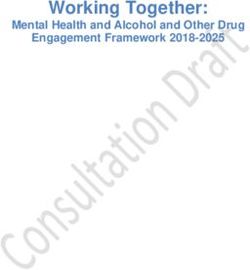
Q 6. Based on your experiences, rate the level of ease or difficulty in dealing with the following
services when coordinating care or case managing clients without secure housing.
Services most frequently mentioned as either good or easy to work with are
• Aboriginal Health Services (66.3%),
• Community Health Services (73.8%),
• Drug and Alcohol services (58.8%)
• General Practice (57.6%).
Services most frequently mentioned as difficult or very difficult to work with are
• Mental Health Services (45%)
• Hospital Inpatient Services (34.2%).
Opinions over ease of working with Mental Health Services are quite divided; they recorded the highest
number of ‘difficult to work with’ responses but also the equal highest number of ‘very easy to work with’
responses (Table 5; Figure 1).
Table 5
Ease or difficulty dealing with health care services for homelessness and community service
providers
Answer Options Very easy Good to Difficult to Very I don't Response
to work work with work with difficult to know Count
with work with
General Practice 6.3% 51.3% 23.8% 5.0% 15.0% 80
Hospital Emergency 3.8% 49.4% 20.3% 7.6% 20.3% 79
Services
Hospital Inpatient 1.3% 44.3% 24.1% 10.1% 20.3% 79
Services
Dental Services 2.5% 29.1% 21.5% 7.6% 39.2% 79
Aboriginal Health 6.3% 60.0% 17.5% 3.8% 12.5% 80
Services
Community Health 12.5% 61.3% 12.5% 3.8% 10.0% 80
Services
Mental Health 12.5% 41.3% 25.0% 20.0% 2.5% 80
Services
Drug and Alcohol 7.5% 51.3% 22.5% 6.3% 13.8% 80
Services
answered question 81
skipped question 209
11Figure 1
Q 7.Please explain what makes a service easy to work with?
Seventy seven responses were received to this open ended question. Sixty four people responded to this open
question about the difficulties reported by clients in accessing health care services.
Key themes were:
• quality of systems, service delivery, and client centered service
• attitude of staff, relationships and understanding homelessness issues
• accessibility – cost and availability
• clear and open communication and information
• collaborative work practices
Some sample responses for the most frequently mentioned themes are provided below. A more detailed list of
sample responses is provided at Appendix 5.
12Quality of systems, service delivery, and client centered service - mentioned by 37 respondents.
“clear eligibility and referral processes, shared case management; good referral systems, professionalism,
organized internal systems, flexibility; commitment to client centered approach, ability to take on
feedback; not sending clients around many services in circles (wrong door); timely response or call backs,
they are client focused and have good referral networks; cultural competency, flexible outreach models,
diversity of treatment models, early intervention and prevention services; structure, willingness,
determination; return calls emails etc within a reasonable time frame, workers don’t dump difficult
clients with inappropriate referrals; clear pathways;”
People; attitude, relationships, understanding homelessness issues – mentioned by 29 respondents.
“non-judgmental, patient and non-threatening; attitude, non-judgmental, compassion, no prejudice,
respect, listening etc friendly interested staff; genuine interest in helping people; staff understanding
homelessness issues; being aware and adjusting attitude towards vulnerable people; having one person
to talk to about a particular client (not having to explain the story to numerous people)”
Accessible – cost and availability- mentioned by 24 respondents.
“the service has to be readily accessible; available to talk, give advice (to staff and potential patients)s;
willing to accept bulk billing patients with no fixed address; taking on new patients; accessible, short
waiting list/time;”
Clear and open communication and information – mentioned by 22 respondents.
“being able to share information readily; being transparent, open and honest; explains what service they
can provide, returns calls; open and honest communication; staff who can explain what support/service is
available to clients and direct them appropriately if they are unable to assist; returning phone calls,
feedback letter or discharge summary; they are quick to respond to calls/messages and take time to
explain what is happening barriers;”
Collaborative work practices – mentioned by 14 respondents.
“One that works in cohesion with other allied services; relationships between service providers and
“health services are strong, with collaborative coordination of care; responsive because there is an
established working relationship via engagement in mutual programs and inter-agencies, shared
knowledge”
Q 8. Please explain what makes a service difficult to work with?
Seventy four responses were received to this open ended question. Generally the responses to this question
were the opposite of responses to question seven. Key themes were; quality/internal systems, access
(availability and cost), staff attitude, poor communication, lack of integration and team work, and unrealistic
expectations.
Some sample responses for the most frequently mentioned themes are provided below. A more detailed list of
sample responses is provided at Appendix 5.
Quality/internal systems – mentioned by 26 respondents
“firm guidelines not allowing flexibility, ‘not my job/role’ attitude; not being able to refer appropriately
and too lazy to help client through the maze of processes; not able to brain storm/work around issues
that arise – ie no flexibility not able to individualise; inefficient or non-existent referral system, non-
professionalism, no organisation, non flexible in service delivery; not client focused and not willing to go
beyond providing a basic service to clients; no outreach models, only service provision in regional centres,
13lack of flexibility, stringent eligibility requirements, dilution of funding for supportive care models such as
community mental health;”
Access – availability and cost - mentioned by 25 respondents
“no vacancies/availability; accessibility and cost; do not accept bulk billing patients- have limited
available appointments (long wait times); hard to access service, complex to refer, work in isolation, not
working from trauma informed framework; unexplained hours of closing/meeting times; not enough case
managers, case managers/support workers not attending services with clients”
Staff - attitude, non understanding - mentioned by 18 respondents
“attitude, judgmental, prejudice (colour and poverty), arrogance, stereo-typing; impatient/rude
/judgmental staff, threatening demeanor with nervous clients; staff who are rude, uninterested and
unhelpful; no understanding of homelessness and how that impacts on clients lives professional snobbery,
stigmatizing of clients with Alcohol and Other Drug (AOD) issues in particular; attitude that health service
knows best; services that don’t understand the Aboriginal people;”
Poor communication – mentioned by 12 respondents
“Not willing to provide information though confidentiality forms have been signed by client; poor
communication to client; lack of ability to share information, health legislation makes this difficult
where women and children are victims of domestic violence”
Q 9. When your clients without secure housing are attending a health service, what information
is MOST important for you to receive from the health service so you can support them with
their housing problems?
Seventy three people answered this open ended question providing a comprehensive list of information
needs. Some examples of responses are listed below. A more detailed list of sample responses is provided at
Appendix 5.
• Thorough case management communications, Doctors’ reports, for effective outreach follow up and
evaluation of recovery;
• Information about the support they will need to enable them to access secure housing;
• Ability to live in housing, specific health needs that will impact on seeking or living in housing;
• Mental health status; complex health needs and what supports are already involved;
• How to access service, public transport links and nearby accommodation options;
• What type of accommodation most/more suitable and why. The effects lack of secure housing has on
clients wellbeing;
• Does the client have a condition that requires monitoring, and if so what has been put in place to
ensure this is addressed, in particular with mental health conditions; reason for housing crisis, eg
Black listed, mental health;
• Whether pet is medical companion;
• Documentation of injuries and impacts of domestic violence
• Person to contact from the health provider; recent A1 assessment, Comprehensive Risk Assessment
and Management Plan, Substance Abuse Assessment if applicable), Care Plan and Workplace Health
and Safety Community Mental health checklist
• Detailed support letter stating clients health condition and a realistic request for a particular product
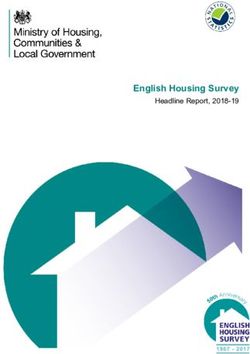
14Q 10. In your experience, how often is this information currently provided to you?
Only 1.2% of homelessness and community services providers stated that they always received the
required information from health care services and 29.8% stated that it was rarely or never
provided. (See Table 6 and Figure 2.)
Table 6
How often is the information required from health care services currently provided to homelessness and
community service providers
Answer Options Response Response Count
Percent
Always 1.2% 1
Most of the time 17.9% 15
Sometimes 51.2% 43
Rarely 25.0% 21
Never 4.8% 4
answered question 84
skipped question 208
Figure 2
15Q 11.Please suggest ways to better support people without secure housing to access the health
care they need?
Sixty six responses were received to this open ended question. Key themes were:
• More funding, staffing, services
• Better access, bulk billing
• Information
• Transport
• Quality of service
• Training staff
• Increased collaboration and coordination
Some sample responses for the most frequently mentioned themes are provided below. A more detailed list of
sample responses is provided at Appendix 5.
More funding, staffing, services - mentioned by 22 respondents
“dedicated services rather than multiple people trying to help; more health services equipped to handle
mentally ill patients and patients who can’t handle schedules appointment-style services; Lack of staffing
is a major concern in terms of access to health services, in this instance mental health services
particularly; increased drop in services (outside of Lismore), facilitate health open days once per quarter
with access for transient/rough sleepers to health services”
Better access, bulk billing - mentioned by 16 respondents
“ensure services are accessible; more bulk billing; provide or promote more bulk billing in regional areas;
easier access to dental, mental health and Aboriginal specific services; support workers to assist clients to
fill in forms”
Information - mentioned by 16 respondents
“Provide written information, especially contact details and names of staff referred; easy access to a local
directory describing relevant health services, affordable options on an individual basis; organization
constantly need to be advised about services available to clients; have more community knowledge about
what is going on in Aboriginal communities; list of local GPs and other health providers willing to see new
clients/bulk billing options;”
Transport - mentioned by 10 respondents
More transport; transport funded to and from the health centre; we live in an area where public transport
is non existent and the specialist services are often over 100 kms away, free transport is a good start;
community transport more often and more flexible
Q 12.Would you be prepared to participate further in discussions, consultations or the design of
initiatives to improve health care for people without secure housing?
Thirty six (36) respondents out of a possible 131 responded positively to this question.
16RESPONSES FROM THOSE IDENTIFYING AS PRIMARILY HEALTH CARE SERVICE
(Questions 13 to 25 targeted organisations primarily providing health care)
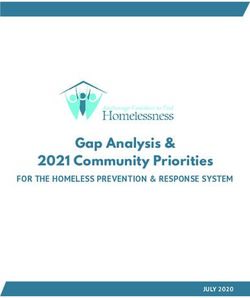
Q. 13. What is the primary focus of the health care service where you work?
Highest numbers of respondents to the survey from the Health Care sector were from Community Health
Services (29.1%), Mental Health Services (19.1%), Hospital Inpatient Services (17.3%), Hospital Emergency
Services (13.6%) and General Practice (9.1%) (see Table 7 and Figure 3).
Table 7
Primary Focus of the Health Care Services
Answer Options Response Percent Response Count
General Practice 9.1% 10
Hospital Emergency Services 13.6% 15
Hospital Inpatient Services 17.3% 19
Dental Service 1.8% 2
Aboriginal Health Services 4.5% 5
Community Health Services 29.1% 32
Mental Health Services 19.1% 21
Drug and Alcohol Services 5.5% 6
answered question 110 110
skipped question 182 182
17Figure 3
Q. 14. What description best describes your role in the organisation?
The majority of health care service respondents were clinicians (71.3%) followed by managers (12.0%) (Table
8).
Table 8
Role of respondent – health care services
Answer Options Response Response Count
Percent
Clinician 71.3% 77
Manager 12.0% 13
Administration Support 2.8% 3
Other 13.9% 15
answered question 108
skipped question 184
18Q 15. This survey is interested in those patients without secure housing. This may include
people who are already homeless (living rough, in transient or temporary accommodation) or
are having difficulty in sustaining their tenancy and so are at risk of becoming homeless. In
your experience, how often does your service provide health care for patients without secure
housing?
More than a third of health care service providers (36.4%) care for a person without insecure housing at least
once a day and a further third (33.6%) at least once per week (Table 9 and Figure 4).
Table 9
Frequency of care of patients without secure housing – health service providers
Answer Options Response Response Count
Percent
A number of times every day every week 17.3% 19
At least one person - someone most days 19.1% 21
Someone every week 33.6% 37
Someone every month 14.5% 16
Rarely 11.8% 13
I don't know 3.6% 4
answered question 110
skipped question 182
Figure 4
19Q 16. Reflect on a time you were caring for someone that did not initially identify they had
housing difficulties, but this was later disclosed during this period of care. Are patients asked
about their living situation when they visit your health service?
Less than half (48.1%) of health care respondents always ask clients for details about their housing situations
(Table 10).
Table 10
Are patients asked about their living situation when they visit a health care service
Answer Options Response Response Count
Percent
Always 48.1% 52
Most of the time 24.1% 26
Sometimes 18.5% 20
Rarely 2.8% 3
Never 2.8% 3
Don't know 3.7% 4
answered question 108
skipped question 184
This means that health care providers have no knowledge of the housing situation of over 50% of clients.
Q 17. Please describe any other mechanism your service has in place to alert you if a patient
does not have secure housing.
Forty seven people responded to this question with a wide range of comments including that assessments are
made by other people (e.g. triage), they come as referrals, they are asked for a mailing address each time they
ask for an appointment, Doctor asks about living arrangement, or an address is always needed.
Q 18. Describe problems you encounter in delivering or planning care when patients without
secure housing are not adequately identified early?
Seventy two responses were received to this question. This question supposedly limits the respondent to
situations where insecure housing was not identified early. Some replied to that question, for example ‘in my
experience this has not happened’, but the majority of respondents answered more generally about problems
delivering or planning care for homeless clients which are addressed more fully in following questions
Therefore only those few responses which appear to answer the question correctly have been provided below
• Some are at risk of homelessness when we first contact for case management and then find themselves
homeless
• In my experience this has not happened
• they are identified early
• Identification is not the main problem, the problem occurs when you are unable to do anything about
the situation
• Early identification or late identification - the problem is one of housing supply
• Causes significant problems when planning their treatment options
• Hasn't been an issue to date
20Q 19. When caring for patients identified as being without secure housing, what information
would be helpful to your service to better address their health care needs?
Sixty five responses were received to this open ended question. Key themes were:
• How to access emergency and secure housing, or a drop-in centre
• Support services and pathways
• Information about the client
• Access to social workers or care workers
Some sample responses for the most frequently mentioned themes are provided below. A more detailed list of
sample responses is provided at Appendix 1.
How to access emergency and secure housing, or a drop-in centre - mentioned by 30 respondents
“Somewhere they can go even temporarily whilst recovering; where there is a drop in situation for
showering and clothes washing, meals; temporary accommodation they can access in Casino; crisis
accommodation access; after hours accommodation list; location and availability of supported care living
options; a central housing information hub would be useful;”
Support services and pathways – mentioned by 13 respondents
“Simple information on pathway to access secure housing and case management support to do so; what
services are available to provide housing support and pathways for referral; knowing what is available
for these persons to access upon discharge from hospital while they are recovering eg accommodation,
services that will accept such clients or case management services”
Information about the client – mentioned by seven respondents
“previous health, psychosocial history, current family and social support in place; where they have been
living or with who, previous difficulties with housing, any financial difficulties (not details, just general
issues); other supports, community programs involved and their input, prognosis and expected medical
outcomes or friends national pharmacy/medical information scheme”
Access to social workers or care workers – mentioned by four respondents
“The contact details of a liaison officer or care workers to ensure results are followed up; access to social
housing workers; social workers to contact”
Q 20. How would you describe the overall communication you have with other agencies
involved in supporting a person identified as being without secure housing?
Only a small proportion of respondents stated that communication was excellent (6.4%). The most frequent
response to this question is “communication is sometimes good but it relies on my individual relationships’
(29.8%) followed by ‘communication is mostly good’ (23.4%). Almost one quarter of respondents stated that
communication is either poor (12.8%) or very bad (9.6%) (Table 11).
21Table 11
Level of communication with other agencies
Answer Options Response Response Count
Percent
Most services are excellent and I get the information I 6.4% 6
need to help the patient
Communication is mostly good 23.4% 22
Communication is sometimes good but it relies on my 29.8% 28
individual relationships
Communication is generally poor 12.8% 12
Communication is very bad and it makes it difficult for 9.6% 9
me to meet the needs of the patient
Not applicable in my role 18.1% 17
answered question 94
skipped question 198
Figure 5
22Q 21. Please explain why you chose this response?
The 73 responses to this question were varied and there were no particular themes or trends identified.
Respondents stating that communication was ‘very bad’ or ‘poor’ had various experiences including: non-
availability of social workers, non-availability of services such as accommodation, services not available after
hours, services refusing care if there is no address, or not being aware of what was available. Lack of a
standard practice, overwhelming bureaucracy, or simply ‘no communication lines’ were also provided as
explanations for their response to Question 20.
Q 22. When caring for people who do not have secure housing, is it clear to you who to contact
for assistance with:
In many cases health care service workers are not clear about who to contact for assistance with patients
without secure accommodation. Greatest clarity exists around the services available to support health and
well being (40.2% are clear). Least clarity is around issues relating to case management being undertaken by
other agencies (42.4% unclear) (see Table 12).
Table 12
Is it clear who to contact for assistance with:
Answer Options Yes No Not Sure N/A to my Respons
type of e Count
service or
role
Issues about retaining their current 34.8% 31.5% 19.6% 14.1% 92
accommodation
Issues about finding new or more secure 38.0% 35.9% 14.1% 12.0% 92
housing
Issues relating to case management 25.0% 42.4% 19.6% 13.0% 92
being undertaken by other agencies
Planning transfer of care from hospital 25.3% 36.3% 15.4% 23.1% 91
(discharge) for people without housing
Planning to deliver care in a community 33.3% 29.0% 23.7% 14.0% 93
setting including assistance with post
discharge care
Identifying what services are available to 40.2% 31.5% 21.7% 6.5% 92
the patient that could support their
health and wellbeing
answered question 94
skipped question 198
Q. 23. Please describe the BIGGEST difficulty you experience when providing health care
services to people without secure housing who visit your service?
Eighty nine responses were received to this open ended question. Key themes were:
• Making contact, following up, home visit
• Self care, personal wellbeing and self esteem issues for the individual and children
• Lack of appropriate housing/ emergency/crisis housing
• Health care not a priority for homeless people
• Discharge planning
• Lack of services
23Some sample responses for the most frequently mentioned themes are provided below. A more detailed list of
sample responses is provided at Appendix 5.
Making contact, following up, home visit – mentioned by 20 respondents
“Making contact, making appointments, finding a venue to offer treatment; inability to follow up or visit
at home; stability, consistency in offering ongoing care; to ensure the baby will be cared for in a safe
environment and they are close to medical services; we cannot plan long term care, for instance putting
in necessary home modifications; Collecting I.D to get services to get housing”
Self care, personal wellbeing and self esteem issues for the individual (and children) – mentioned by 16
respondents
“Self esteem, self care issues, difficult to care for people who have little regard for themselves; their
immediate needs are critical and the needs of the parent and or child can be compromised in the near
future or the long term; responding to levels of stress, poverty, exposure to violence”
Lack of appropriate housing/ emergency/crisis housing – mentioned by 15 respondents
Our inability to find housing for them; they do not want assistance, just a bed for the night out of the
elements; solve the accommodation and their crisis resolves; no available emergency housing options AT
ALL!; finding secure housing and avoiding admission to hospital; lack of emergency housing and the ten
year waiting list for housing commission house”
Health care not a priority for homeless people – mentioned by 12 respondents
“difficult to focus on any health issue when not securely housed; their housing becomes their focus and all
sorts of mental health issues are exacerbated such as anxiety and depression; unable to address other
issues (D&A, child protection etc) without secure housing;”
Discharge planning – mentioned by six respondents
“Patients want to remain in hospital because they have no accommodation available; prolonged stay in
mental health inpatient unit with subsequent bed block resulting in other patients awaiting a bed in step
down unit. Often waiting for weeks in High Dependency Unit when this care is no longer required”
Lack of services – mentioned by three respondents
“No social worker; mental health clients needing supported accommodation; providing support services
for young people trying to support them to get secure accommodation is the biggest challenge, especially
when they need support”
24Q 24. What OTHER difficulties do you encounter when providing health care services to people
without secure housing who visit your service?
Seventy nine people responded to this question. These comments are varied with themes difficult to identify.
Only themes/comments not covered in Question 23 are listed below. A more detailed list of sample responses
is provided at Appendix 5.
• Food insecurity, financial difficulties, mental health issues, women facing homelessness. I had a client
who was on a program that was supposed to assist her retain her accommodation due to hoarding,
when I spoke to the person involved she stated "she is no longer on the 16 week program" as when
she spoke to client several times on the phone she stated everything was ok, after the program was
finished the client was evicted due to her issues and was homeless. I wanted to know why the
program hadn’t been out to the clients home.
• We see a lot of people who are angry and frustrated at the system. who have been sent from one
service to another and land back here as they don’t know where else to go. It is then our job not only
to find services to provide them with their needs but also to calm them into believing we are trying to
assist them with their needs.
• Undertaking the physical requirements of looking for secure housing when one is on chemotherapy or
radiation therapy is near impossible for many.
• Insecurity from patients and confusion
• They repeatedly seek the service even if other advocates have attempted to align them with
alternatives to health care through a GP, or community service.
• Being unsure who else may be present in temporary accommodation can pose security issues
• On-going care for patient - referral to COPS is excellent, concerned they become non-government org.
• Difficulties with referral to Hospital in the Home Program.
• Often multifactorial and can include mental health issues for themselves and involved people - can be
hard to develop rapport and trust/ compliance issues - not a word I like but can be a huge issue.
• Only feeling helpless to provide any assistance when they disclose their living situation with me.
• Intergenerational lack of basic skills or cooking, cleaning, washing, budgeting. They often have a long
history of problematic rental & sharing housing, with eventual homelessness due to inability to cope
with the multiple factors in caring for a home. Linking to health services is almost impossible, unless
there is a point of contact eg The Winsome in Lismore.
• Ensuring safe secure places for children of these people
Q 25. Please suggest what would help you to deliver more effective health care to people
without secure housing.
Eighty three responses were received to this open ended question. Key themes were:
• More housing available
• A centrally located service
• Information about housing and services
• Services, social workers, case management support
Some sample responses for the most frequently mentioned themes are provided below. A more detailed list of
sample responses is provided at Appendix 1.
More housing available – mentioned by 34 respondents
“a short term housing situation where post patients can recover and receive services; increase in stock of
affordable housing, more social housing and/or crisis accommodation; more crisis accommodation for
25men not located at a pub; by giving them a place to stay overnight as opposed to long term housing;
more housing options in rural areas; more low cost accommodation is urgently needed in the Tweed area-
small I bed units especially; respite – convalescence places for post medical issues that don’t require ACAT
or have ‘nursing home’ stigma”
A centrally located service – mentioned by 14 respondents
“A centrally located service. an outreach worker to see clients at this clinic as a one stop facility; a contact
hub for phone messages, mail and venue for appointments; Venue for drop in service; community clinics
co-located with welfare services; centrally located service where clients can receive outpatient care/clinic;
a local resource centre; to have a clinic where they go to receive all services who can give long term care
;a hub that the homeless felt comfortable to go to as a central/safe contact point; central point of contact
where clients can receive outpatient care/ clinic.”
Information about housing and services –mentioned by 12 respondents
“Printed (web) resource detailing steps a person can take, local resources (and what they actually do);
having a clear pathway for clients to follow to find secure housing; someone to contact for follow up;
telephone advice line; available options for young people aged between 12-25 yrs;”
Services, social workers, case management support – mentioned by 12 respondents
“Case management support to people who need to access secure housing; more assisted accommodation
packages; SOCIAL WORKERS!; more community welfare support officers; welfare officers or social
workers; supervised, supported accommodation specifically designed for people who have failed to
maintain a home”
26DISCUSSION
The purpose of this survey was to better understand the barriers in the health care sector for people without
secure housing and the challenges experienced by health workers planning and delivering care.
The responses to the survey were wide ranging with people from both health and non-health related
organisations participating in fairly even proportions.
The 12 open ended questions provided opportunity for respondents to expand on responses and provide
detailed information about barriers, challenges and solutions. They made clear the complexities involved in
providing more effective health care, with many responses being multi-faceted.
For people without secure housing barriers to access include cost, waiting times, transport, lack of services,
and lack of understanding about the health system and fear of judgement.
Agencies providing support to people without secure housing (not primarily health care) found some health
care services easier to work with than others, citing quality of service delivery, staff attitudes and
understanding of homelessness, accessibility, communication and collaborative work practices as key to
working with a service easily.
These agencies stated that only a small proportion of health care services always provided the information
they required and provided a detailed list of the information they require to assist clients with their housing
problems. When asked about ways to better support people without secure housing to access health care,
more funding/staffing/services, better access including more bulk billing, more low cost transport, and better
information provision were the key themes emerging.
Generally these agencies who primarily provide health care noted communication difficulties with other
agencies involved in supporting a person without secure housing. They reported that better information about
the client, support services and pathways available, how to access emergency housing, and access to social
workers or care workers, would allow them to better address health care needs.
These agencies also reported a lack of clarity around who to contact for assistance when caring for people
without secure housing.
When asked to describe the biggest difficulty experienced in providing health care to people without secure
housing the key themes to emerge were: making contact, following up, home visits; self care, personal
wellbeing for the individual and children; lack of appropriate emergency housing; health care not being a
priority for people without secure housing; discharge planning and lack of services.
When asked for suggestions about what would help them to deliver more effective health care to people
without secure housing, key responses from respondents who primarily provide health care include increased
housing availability, a centrally located service; information on housing and services; social workers and case
management support.
The following points summarises the key findings
• Barriers to accessing health care include cost, waiting times, transport, lack of services and lack of
understanding about the health system and fear of judgement.
• Inability to identify a home address made it difficult to secure appointments, particularly where these
were notified by mail and also on the ability to provide outreach services.
• Agencies found some health care services easier to work with than others, citing quality of service
delivery, staff attitudes and understanding of homelessness, accessibility, communication and
collaborative work practices as key to effective working relationships.
• Generally, only a small proportion of health care services always provided agencies with sufficient and
detailed information required to assist clients.
27• The survey highlighted a lack of clarity around ‘who to contact’. Communication difficulties between
agencies was a commonly identified and identified the need for an improved mechanism to share
information on
o clients and their healthcare needs
o availability of support services and pathways
o access to emergency housing
o social workers or care workers who could assist navigating the healthcare or social housing
sector.
• A consistent theme was the perception that health services were not sensitive to the trauma experienced
by people without secure housing and didn’t understand the problems they encountered. It was reported
that this impacted upon the clients perception of being judged or discriminated against, and also the
ability of healthcare workers to deliver effective client centred health care.
28CONCLUSION
In conclusion, this survey has provided detailed information about barriers to accessing health care and
challenges in providing services for people without secure housing. It also provides suggestions for more
effective health care delivery and ways to support clients to better access health care.
The information needs of both health care and homelessness support agencies are now documented as a
result of the survey.
The information from this survey will provide a resource for health care and other agencies providing services
to people without secure housing to assist them with service planning, developing checklists for information
requirements, and advocacy.
The information from this survey provides a base line for further research and reporting on a number of
aspects of the provision of health services to people without secure housing. Future surveys can utilise the
information from the open ended questions in this survey to develop a survey with fewer open ended
questions that will be easier to analyse and report. Additionally, this report will form a basis for future
discussions and progression on actions.
29APPENDIX 1
North Coast NSW Alliance to Improve Services to the Vulnerable Members of
the Community Memorandum of Understanding
VISION & AIM
The North Coast NSW Alliance to Improve Services to the Vulnerable Members of the Community has the vision
of fostering a response to the needs of the vulnerable members of the North Coast community that is client
centred, multi-sectoral and is integrated and cohesive where services are provided.
The population groups the Alliance will focus its work are
• The Homeless
• People with Disability
• Children and Young People at Risk of Significant Harm
OBJECTIVES OF THE PARTNERSHIP
The objectives of the Alliance are
• Determine and set the framework and agenda for addressing the needs of the vulnerable members of the
North Coast North Coast of NSW community
• Work to foster and facilitate greater cross agency collaboration and partnership
• Facilitate and champion the agenda for addressing the complex needs of the homeless, people with
disabilities and children and young people at risk of significant harm.
FRAMEWORK AND AGENDA
Two levels of work will be pursued
(1) System change (driven by Alliance and the Leadership Group)
(2) Service Integration (driven at the service delivery level)
Lasting outcomes are achieved when integration and changes takes place at both above mentioned levels.
Pivotal to a fruitful collaboration and partnership is an overarching framework that gives shape to activities
and initiatives. This framework will facilitate
• Development of common priorities
• Delineation of responsibilities for involved agencies
• Achievement of higher degrees of coherence and integration within, and among, the various organisations
and agencies.
The Leadership Group sets the framework, the priorities and the overall direction for the Alliance. It receives
reports and tracks the implementation of the actions.
The Leadership Group will ensure systematic, persistent and cohesive action to achieve the objectives of the
Alliance, including
• Undertaking joint strategic and operational activities (including needs assessment, use of common tools
and definitions, joint planning and evaluation)
• Setting and aligning Performance Indicators that measure outcomes and whole-of-system improvement
• Sharing (where appropriate) de-identified and aggregated data, and information
• Determining mechanisms for sharing resources (where possible) in order to achieve the best outcomes and
best value for the community and clients
30You can also read