Survival and patient reported outcome in surgically managed pancreatic and periampullary tumours - DUO
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Survival and patient reported outcome
in surgically managed
pancreatic and periampullary tumours
A doctoral thesis submitted
for the degree of
PhD
Bart M. G. Baekelandt, M.D.1
Main supervisor: Professor Trond A. Buanes, M.D., PhD1,2
Supervisor: Knut Jørgen Labori, M.D., PhD2
Supervisor: Professor Turid Heiberg, PhD3,4
1
Institute of Clinical Medicine, Faculty of Medicine, University of Oslo
2
Department of Hepato-Pancreato-Biliary Surgery, Oslo University Hospital
3
Regional Research Support, Oslo University Hospital, University of Oslo
4
Østfold University College, Halden, Norway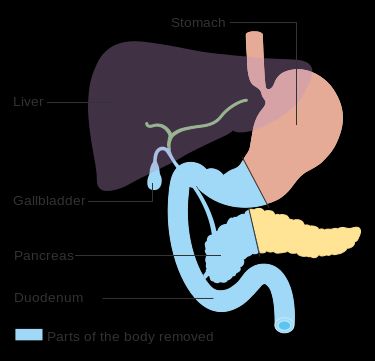
© Bart M. G. Baekelandt, 2020 Series of dissertations submitted to the Faculty of Medicine, University of Oslo ISBN 978-82-8377-766-6 All rights reserved. No part of this publication may be reproduced or transmitted, in any form or by any means, without permission. Cover: Hanne Baadsgaard Utigard. Print production: Reprosentralen, University of Oslo.
“The impediment to action advances action. What stands in the way becomes the way.”
Marcus Aurelius, Meditations
3|Page4|Page
Table of Contents
1. Acknowledgements ................................................................................................................... 7
2. Abbreviations ............................................................................................................................ 9
3. Article overview ...................................................................................................................... 11
3.1. List of publications ................................................................................................................... 11
3.2. Thesis at a glance ..................................................................................................................... 12
4. Norsk vitenskapelig sammendrag .......................................................................................... 13
5. Background .............................................................................................................................. 15
5.1. The pancreas and pancreatic cancer ....................................................................................... 15
5.1.1. Burden and epidemiology of pancreatic cancer ............................................................... 15
5.1.2. Anatomy, physiology and pathology ................................................................................. 16
5.2. Surgical treatment and complications ..................................................................................... 18
5.2.1. Surgical procedures ........................................................................................................... 18
5.2.2. Complications and complication scores ............................................................................ 20
5.3. Treatment endpoints ............................................................................................................... 21
5.3.1. Historical perspective on endpoints in pancreatic surgery ............................................... 21
5.3.2. Patient reported outcome................................................................................................. 22
5.3.3. Psychometrics.................................................................................................................... 23
6. Thesis aims .............................................................................................................................. 25
7. Material and methods............................................................................................................. 26
7.1. Ethics ........................................................................................................................................ 26
7.2. Study design: Thematic Pancreas Tumour Project .................................................................. 26
7.3. Population and measures ........................................................................................................ 27
7.3.1. Paper I................................................................................................................................ 27
7.3.2. Paper II............................................................................................................................... 28
7.3.3. Paper III.............................................................................................................................. 28
7.4. Statistics ................................................................................................................................... 29
7.4.1. Paper I................................................................................................................................ 29
7.4.2. Paper II............................................................................................................................... 29
7.4.3. Paper III.............................................................................................................................. 30
5|Page8. Synopsis of results ................................................................................................................... 31 8.1. Paper I ...................................................................................................................................... 31 8.2. Paper II ..................................................................................................................................... 31 8.3. Paper III .................................................................................................................................... 31 9. Discussion ................................................................................................................................ 32 9.1. Methodological considerations ............................................................................................... 32 9.2. Main findings ........................................................................................................................... 34 9.2.1. Preoperative prognostic factors ........................................................................................ 34 9.2.2. The effects of postoperative complications ...................................................................... 37 9.2.3. Patient reported outcome measures and the PACADI score ............................................ 41 9.3. General discussion ................................................................................................................... 44 10. Conclusion ............................................................................................................................... 47 11. Implications and future perspectives ..................................................................................... 48 List of references............................................................................................................................ 51 Publications .................................................................................................................................... 65 6|Page
1. Acknowledgements
The realization of the present thesis would not have been possible without the support of
colleagues, friends and family. I would particularly like to express my deepest gratitude to the
following:
Trond A. Buanes, Professor of Surgery, main supervisor, for his kind, attentive and inspiring support.
Without him, this thesis would truly have been impossible. His great experience in the field of
pancreatic surgery as well as in supervising PhD-candidates has been invaluable for my progress in
scientific research. I’m thankful for his interest in my professional and personal progress. He has
always had an open door, always been there on short notice and always available for an interesting
discussion. His contagious optimism has been a driving factor for the completion of the thesis.
Knut Jørgen Labori, co-supervisor, for his exceptionally systematic approach to scientific problems
and his ability to distil relevant information. I’m forever in debt to him for his decisive role in my
work. Despite his busy working schedule, he always found time for our research. His clear thoughts,
curiosity and knowledge in the field of pancreatic surgery have been stimulating. I’ve appreciated his
analytical mind and I aspire to this in own my future projects, whatever they may be.
Turid Heiberg, second co-supervisor, for opening my eyes to the importance of patient reported
outcome measures in patient treatment and clinical research. Her passion for developing valuable
questionnaires for measuring how patients are affected by their disease has been inspiring. I will
forevermore keep this patient focused perspective in mind in my future clinical work.
Tom Nordby, for ploughing the fields before my endeavour into the project. His considerate help
during my first year as a research student was conducive to my further success and my integration
into the research group. Without his work to build on, my project would not have been born.
Morten W. Fagerland, for his unique expertise in biomedical statistics and ability to convey his
knowledge to me. I’m thankful for his thoughtful and inspiring advice in my analyses. His guidance
has been important for my interest in statistics.
Several co-authors, for having been instrumental to the project. Marianne J Hjermstad, Elin H. Kure
and Tore K. Kvien, your contribution to the project has been crucial and I thank you all.
7|PageBjørn Atle Bjørnbeth, previous head of department at the Department of Hepato-Pancreato-Biliary Surgery, Oslo University Hospital, for hiring me as a junior doctor and allowing me to be introduced to clinical side of pancreatic cancer management. My professional foundations were laid during the year working at his department, with several inspiring role models among my colleagues. The Research Program for medical students at the University of Oslo, Faculty of Medicine and the Research Council of Norway, for allowing me to dive deeper into surgical research and scientific reasoning at a young age. The present PhD thesis is a direct consequence of the work I did as a research student between 2012 and 2016. The University of Oslo, Faculty of Medicine, for allowing me to enrol in the PhD-program, despite my unorthodox application. Finally, my family, especially my wife, Helene Dahl Jørum, for her patience and encouragements throughout the years, and my daughter Aurora for her affection and the deep meaning she brings to my life. I’ve borrowed from your time with me in order to complete this thesis; this work also belongs to you. I love you. 8|Page
2. Abbreviations
ANN Artificial neural networks
ALP Alkaline phosphatase
ASA American Society of Anaesthesiologists
BMI Body mass index
CA19-9 Carbohydrate antigen 19-9
CF Cognitive function
CCI Comprehensive Complication Index
CRCI Cancer Related Cognitive Impairment
CRP C-reactive protein
CT Computer Tomography
EORTC European Organisation for Research and Treatment of Cancer
EQ-5D EuroQol Group 5 dimensions
ESAS Edmonton Symptom Assessment System
ESPAC European Study group for Pancreatic Cancer
FDA U.S. Food and Drug Administration
FTR Failure to rescue
HRQoL Health related quality of life
ICCTF International Cognition and Cancer Task Force
ICU Intensive care unit
IPMN Intraductal papillary mucinous neoplasm
ISGPF International Study Group for Pancreatic Fistula
LDH Lactate dehydrogenase
LNR Lymph node ratio
LOS Length of (hospital) stay
OMERACT Outcome Measures in Rheumatology
9|PagePACADI Pancreatic Cancer Disease Impact PD Pancreatoduodenectomy PDAC Pancreatic ductal adenocarcinoma PNET Pancreatic neuroendocrine tumour POPF Post-operative pancreatic fistula PPPD Pylorus preserving pancreatoduodenectomy PRO Patient reported outcome PROM Patient reported outcome measure PV Portal vein QoL Quality of life RAID Rheumatoid Arthritis Impact of Disease RR Relative Risk SMA Superior mesenteric artery SMV Superior mesenteric vein TPTP Thematic Pancreatic Tumour Project 10 | P a g e
3. Article overview
3.1. List of publications
1. Baekelandt BMG, Hjermstad MJ, Nordby T, Fagerland MW, Kure EH, Heiberg T, Buanes TA, Labori
KJ
Preoperative cognitive function predicts survival in patients with resectable pancreatic ductal
adenocarcinoma
HPB (Oxford) 2015; 18(3), 247-254
2. Baekelandt BMG, Fagerland MW, Hjermstad MJ, Heiberg T, Labori KJ, Buanes TA
Survival, Complications and Patient Reported Outcomes after Pancreatic Surgery
HPB (Oxford) 2019; 21(3), 275-282
3. Heiberg T, Baekelandt BMG, Kvien TK, Buanes TA
Psychometric performance of the Pancreatic Cancer disease impact (PACADI) score
Pancreatology 2019; 19(7), 971-978
11 | P a g e3.2. Thesis at a glance
Objective Material and Methods Results Conclusions
I Preoperative cognitive function predicts survival in patients with resectable pancreatic ductal adenocarcinoma
In this first paper, we Sixty-six patients with pancreatic Self-reported
1.00
wanted to investigate ductal adenocarcinoma (PDAC) presurgery cognitive
Estimated Surival Probability
0.75
whether preoperative undergoing surgery were function is an
patient reported included from 2008 to 2011. independent and
0.50
outcome measures Forty-four patients had strong prognostic
(PROMs) could function completed preoperative factor in PDAC
0.25
as prognostic factors for Edmonton Symptom Assessment patients undergoing
survival. System (ESAS), European potentially curative
0.00
Organisation for Research and 0 6 12 18 24 30
Survival Time (Months)
36 42 48
surgery.
Number at risk
Treatment of Cancer (EORTC) HighCF = 0 14 13 7 3 1 0 0 0 0
HighCF = 1 30 29 23 18 15 11 6 4 1
QLQ-C30 and PAN26 PROM- Low Cognitive Function High Cognitive Function
questionnaires. There was no
difference in core clinical data Preoperative Cognitive function (CF) score in
between these 44 and the 22 EORTC QLQ-C30 was the only factor significantly
who did not complete associated with survival. Median survival for
questionnaires. We analysed the patients with low CF (≤ 67%) and high CF (83% or
predictive value of PROM-items. 100%) was 10 months and 21 months respectively
Survival analysis was performed (p4. Norsk vitenskapelig sammendrag
Bakgrunn: Kreft i bukspyttkjertelen er en alvorlig sykdom. Omtrent 3% av nye kreftdiagnoser årlig i
Norge er bukspyttkjertelkreft, men diagnosen er årsak til over 7% av kreftdødeligheten (1). Pasienter
med pankreatisk duktalt adenokarsinom (PDAC), den vanligste kreftformen i bukspyttkjertelen, har
en femårsoverlevelse i underkant av 5%. Kirurgi er den eneste behandlingen som kan gi
langtidsoverlevelse. Dessverre har de aller fleste pasientene lokal eller metastatisk spredning ved
diagnosetidspunkt, med henholdsvis 10 og 5 måneders median overlevelse (2). En femtedel av
pasientene har en begrenset lokal svulst som er tilgjengelige for operasjon, med en median
overlevelse på 20 måneder og rundt 20 % femårsoverlevelse (2). Hvordan sykdommen og
behandlingen påvirker pasientenes livskvalitet er av stor betydning. De siste 10-20 årene har det
vært økt fokus på livskvalitet hos kreftpasienter, men vi vet fortsatt lite om samspillet mellom
livskvalitet og behandling ved PDAC (3-5). Målet med avhandlingen er å utforske sammenhengene
mellom livskvalitet, overlevelse og kirurgi hos pasienter med kreft i bukspyttkjertel, gallegang og
papillen / ampulla Vateri. Materiale og metode: I oktober 2008 startet inklusjon i en observasjonell
kohortstudie av pasienter henvist med mistanke om kreft i bukspyttkjertelen, opprettet ved Oslo
Universitetssykehus. Vi registrerte en rekke kliniske data som alder, komorbiditet, operasjonsdata,
komplikasjoner og overlevelse. I tillegg samlet vi inn livskvalitetsdata ved hjelp av spørreskjemaene
ESAS (6), EORTC QLQ-C30 (7) og PAN26 (8). PACADI, et nytt skjema som forskningsgruppen vår har
utviklet (9), ble også benyttet som en del av valideringsprosessen. I første artikkel inkluderte vi 44
pasienter med PDAC, operert mellom oktober 2008 og desember 2011, som hadde fylt ut
preoperative spørreskjemaer. Målet var å kartlegge den potensielle prognostiske verdien av
livskvalitetsfaktorer. I andre artikkel inkluderte vi i samme tidsperiode totalt 208 pasienter operert
for ondartet eller godartet svulst i bukspyttkjertelen. Vi samlet inn livskvalitetsskjemaer preoperativt
samt ved tre og seks måneder etter operasjon. Komplikasjoner ble klassifisert etter Clavien-Dindo-
klassifiseringen (10) og hver pasient fikk en komprehensiv komplikasjonsindeks-skår (CCI) fra 0-100,
avhengig av antall komplikasjoner og deres alvorlighetsgrad (11). Komplikasjoners effekt på
overlevelse, liggedøgn og livskvalitet ble undersøkt. Tredje artikkel er en videre validering av PACADI.
Vi inkluderte 360 pasienter med mistenkt kreft i bukspyttkjertelen mellom 2012 og 2016, og
undersøkte PACADIs psykometriske karakteristika sammenlignet med ESAS og EQ-5D (12). Disse
skjemaene ble fylt ut ved inklusjon og ved 1, 2, 3, 6, 9 og 12 måneder etter. Vi undersøkte test-retest
reliabilitet (konsistens over tid), intern konsistens, responsivitet for endring, konkurrent validitet
(korrelasjon med eksisterende skjemaer), diskriminant validitet (diagnosespesifisitet) og prediktiv
verdi for overlevelse. Resultater: Det eneste livskvalitetsmålet vi fant som signifikant prediktor for
13 | P a g eoverlevelse, var preoperativ kognitiv funksjon. Pasienter som rapporterte normal eller tilnærmet normal kognitiv funksjon hadde median overlevelse på 21 måneder, mot kun 10 måneder for pasienter som rapporterte kognitiv svekkelse (p
5. Background
5.1. The Pancreas and pancreatic cancer
5.1.1. Burden and epidemiology of pancreatic cancer
While pancreatic cancer is relatively rare; estimated to be the 11th most common cancer in the USA
in 2019 with an estimated 56 770 new cases (3.2% of total cancers), it’s one of the most common
causes of cancer related death; estimated to be the 3rd most common cause of cancer death in the
USA in 2019, with an estimated 45 750 deaths (7.5% of all cancers) (20). Similar numbers are true for
Norway; in 2018, 34 190 patients were diagnosed with cancer in Norway, 909 (2.7%) of whom were
diagnosed with pancreatic cancer, while in 2017, out of 11 016 cancer deaths in Norway, 787 (7.1%)
were caused by pancreatic cancer (1). Globally, pancreatic cancer is estimated to be the 11th most
common cancer while being the 7th most common cause of cancer death (21).
The main reason for the discrepancy between incidence and mortality is the low survival rates. There
are several reasons for this poor survival: the biologically aggressive nature of pancreatic cancer, the
lack of curative chemotherapy, and the late onset of serious symptoms when the disease has already
spread, leaving approximately 20% of patients as candidates for surgery at time of diagnosis (2).
While some cancers have a relatively benign development, such as prostate cancer, other types of
cancer with historically poor survival rates are now treated efficiently, such as leukaemia, kidney
cancer or testicular cancer. Survival rates for pancreatic cancer have remained particularly low, even
though there has been a significant increase the past 10 years. In the beginning of the 1990s, 5-year
survival for pancreatic cancer (of all types) in Norway was around 2%, by the beginning of the 2000s
it was 4%, and in the period from 2014 - 2018, 10.9% of pancreatic cancer patients survive 5 years (1).
This increase in survival is related to several factors, such as improvements in adjuvant
chemotherapy (22-24) and the increased use of computer tomography (CT) scans in patients with
unrelated symptoms, which results in incidental diagnosis at an early stage, when prognosis is more
favourable (25). Important contributions to increased survival also stem from progress in surgery,
such as more comprehensive vascular reconstruction (17), which has opened the door to potentially
curative surgery for patients with borderline resectable and locally advanced pancreatic cancer (26, 27).
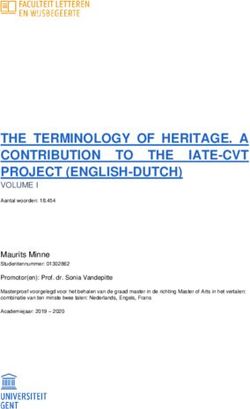
15 | P a g e5.1.2. Anatomy, physiology and pathology The pancreas is a retroperitoneal organ in the upper part of the abdomen, located behind the stomach. It is surrounded by a thin capsule of connective tissue, has a lobulated form, weighs about 100 g and measures around 20 cm in length in the adult. It is both an endocrine and an exocrine organ; the former means that the pancreas produces hormones secreted into the blood circulation (such as insulin and glucagon, which regulate carbohydrate metabolism) while the latter means enzymes are secreted locally (pancreatic juices – essential for digestion). These enzymes are secreted via the pancreatic duct, which begins in the tail of the pancreas, passes right through the body and neck before turning inferiorly after entering the head. It connects to the common bile duct to form the ampulla of Vater, which opens into the duodenum via the major duodenal papilla. Figure 1 – The pancreas, pancreatic duct and peripancreatic structures. Reproduced with permission from Blausen.com staff, "Blausen gallery 2014", Wikiversity Journal of Medicine. 16 | P a g e
Two major abdominal vessels pass right left of the pancreatic head; the superior mesenteric vein
(SMV) ending in the portal vein (PV), and the superior mesenteric artery (SMA). This close relation to
major blood vessels means these can be involved in pancreatic tumours.
Symptoms of pancreatic cancer are slowly progressive jaundice, non-specific upper abdominal pain
or discomfort, weight loss and anorexia. Jaundice is most common in pancreatic head tumours
because of the proximity to the bile duct which can get obstructed, while body and tail tumours give
more non-specific symptoms such as weight loss and discomfort. These symptoms are not perceived
as acute and rarely lead to a prompt visit to the doctor. At time of diagnosis, most patients have
metastatic disease. Because of the organ’s venous drainage, metastases are often found in the liver
and lungs.
The most common origin of cancer is exocrine ductal cells; this cancer is called pancreatic ductal
adenocarcinoma (PDAC). The prognosis is grim, with less than 5% of patients surviving 5 years or
more. Approximately 60% of PDAC patients have metastasis at time of diagnosis, another 20% have
locally advanced disease. These patients are unsuited for surgery and have a median survival of 5
and 10 months respectively. The last 20%, patients with local tumours or borderline resectable
tumours, have a median survival of around 20 months, with around 20% surviving more than 5 years
(2)
.
Intraductal papillary mucinous neoplasms (IPMN) are cystic precursor lesions with clear malignant
potential. They account for approximately 5% of tumours in the pancreas. They have a better
prognosis than PDAC, with 43% 5-year survival for invasive IPMN and 77% for non-invasive IPMN (28).
Pancreatic neuroendocrine tumours (PNET) are hormone producing tumours. They are often
detected early because of the serious symptoms they can cause, such as low blood sugar in patients
with insulinomas. PNETs account for about 5% of pancreatic malignancies and have an overall 5-year
survival of 42%, with survival depending on size and Ki-67 levels (a cell proliferation marker in
neuroendocrine tumours) (29).
The periampullary tumours are not located in the pancreas, but give rise to similar symptoms
because of their proximal location. They comprise of duodenal tumours, extrahepatic bile duct
tumours and ampullary tumours. 5-year survival after surgery is 49%, 27% and 45% respectively (30).
In addition to the malignant tumours, benign lesions may result in similar symptoms and radiological
findings as pancreatic cancer. The most common of those lesions are pancreatic cysts, pseudocysts
and non-alcoholic chronic pancreatitis.
17 | P a g eThe carcinogenesis of pancreatic cancer is not completely understood. Further understanding of
tumour biology and pathogenesis may give rise to new future non-surgical treatment (31).
Some risk factors are associated with the development of pancreatic cancer. Smoking is an
important risk factor, being the only exogenous risk factor reported consistently in the literature,
with a relative risk (RR) of 2-3 (32, 33). Other reported factors are nonhereditary and chronic
pancreatitis (RR: 2-4) (34), long-standing diabetes mellitus (RR: 2) (35), obesity (RR: 1-2) (36) and non-O
blood group (RR: 1-2) (37). There’s also a genetic component, as familial pancreatic cancer is
associated with increased risk (38). It’s estimated that 5-10% of cases have an inherited component
(39)
. Several genetic syndromes have been associated with pancreatic cancer (31).
Prognostic factors are important in order to select the right patients for surgery, given that many
patients will not be cured of their cancer despite surgery. Some clinicopathological prognostic
factors are well known, such as TNM-stage (40-42), lymph node ratio (LNR), tumour size, histological
differentiation (grade or G) (43), perineural invasion (44), tumour necrosis (45), immunohistochemical
biomarkers (46) and resection margin status (R) (47-50). However, much of this information is collected
after surgery and histological examination of the removed tissue, and does not aid in the
preoperative decision-making. Few factors enable prediction of outcome in advance of surgery, one
such factor is Carbohydrate antigen 19-9 (CA19-9) (51), a tumour marker which in addition to
preoperative prediction also predicts the effect of adjuvant chemotherapy (52).
5.2. Surgical treatment and complications
5.2.1. Surgical procedures
The pancreas has a great secretory reserve function; hence a relatively small portion of healthy
pancreatic tissue is sufficient to maintain physiological function without the appearance of
symptoms (53). This reserve function also means large parts of the pancreas can be surgically
removed without lethal consequences.
Depending on the location of the tumour, different surgical procedures are required. For tumours
located in the pancreatic head, pancreatoduodenectomy (PD) is performed, often with pylorus
preserving method (PPPD) which shows less intraoperative blood loss and shorter operating time (54).
In classical PD, the pylorus, gallbladder, extrahepatic bile ducts, distal part of the stomach,
duodenum and pancreatic head are removed, while in PPPD, the transection is at the proximal part
18 | P a g eof the duodenum instead of proximal to the pylorus. After resection, the body of the pancreas, the
remaining part of the stomach and the remaining bile duct are connected to the small bowel.
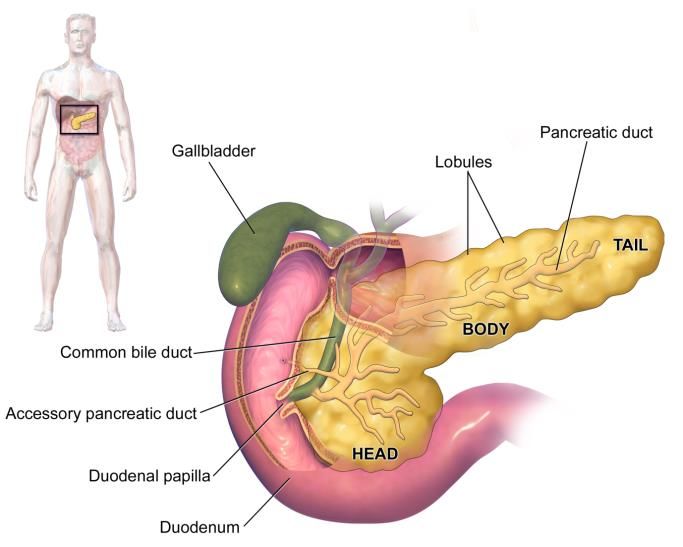
Figure 2 – Diagram showing the area removed Figure 3 – Diagram showing the resulting
during pancreatoduodenectomy (PD). From anatomy after a PD. From Cancer Research UK
Cancer Research UK / Wikimedia Commons. / Wikimedia Commons (freely useable).
If the tumour growth involves the head and body / tail, a total pancreatectomy may be required.
This surgery is similar to PD, but the entire pancreas is removed resulting in severe insulin
dependent diabetes and the need for lifelong enzyme replacement therapy.
For tumours in the body or tail of the pancreas, distal pancreatectomy may be performed. In
contrast to total pancreatectomy and pancreatoduodenectomy, mostly performed by open
laparotomy, distal pancreatectomy is frequently a minimally invasive / laparoscopic surgical
procedure. In this case, only the body / tail of the pancreas and the spleen are removed, and the
gastrointestinal tract is left intact.
If the tumour invades a vascular structure, vascular resection / reconstruction may be required to
achieve radical removal of cancer tissue. While venous resection of the SMV and PV is considered
standard of care in patients with a reconstructible vein, arterial resections are only performed in
highly selected patients. Depending on the location of the vascular resection, the border of the
resection, and the length of vessel removed, different techniques may be used, such as end-to-end
anastomosis, patch or graft. Resection of the SMV and PV is not associated with lower long-term
19 | P a g esurvival compared to PD without venous reconstruction (55). When vascular reconstruction during
pancreaticoduodenectomy is required, a vascular or transplantation surgeon assists the
gastroenterological surgeons.
Other types of surgery may be useful in the setting of pancreatic tumours, such as enucleation of
small benign tumours or resection of the duodenum if the tumour is located only there.
5.2.2. Complications and Complication Scores
Despite the relative low 30-day postoperative mortality of 1-3% (56, 57), perioperative morbidity is
common after pancreatoduodenectomy. The rate depends on how complications are defined; not all
hospitals have used the same standards, numbers have varied greatly, especially before
complication classifications were developed (58). However, complications have been reported in 30-
60% of operated patients. Higher perioperative mortality and complication frequencies are reported
in hospitals performing few pancreatoduodenectomies (59, 60), an important argument for centralizing
this type of surgery to tertiary centres. Common but less serious complications may not be treated
at the tertiary institution performing the operation, but at the patient’s home or local hospital, thus
being underreported in the scientific literature.
Complications may be divided into medical and surgical ones. Medical complications after
pancreatoduodenectomy include delayed gastric emptying, urinary tract infection, pneumonia, and
less frequently kidney failure, hospital infections, pulmonary embolus, delirium, cardiovascular
events and portal vein thrombus. Surgical complications include wound infection, pancreatic fistula /
leakage, bile leakage, abdominal abscess and intraabdominal bleeding. Some of these complications
are common for all types of surgery, such as pneumonia or wound infection, while others are
specific for this type of surgery, such as pancreatic fistula.
Complications may be individually graded, such as grade A, B and C for delayed gastric emptying (61),
pancreatic fistula / leakage (62) and bile leakage (63).
Complications can also be scored using a scoring system that doesn’t differentiates between the
type of complication, but on the clinical consequence of the complication. The Clavien-Dindo
complication score (10) is widely used in surgical literature (Table 1). Another example of such a
scoring system for surgical complications is the Accordion-classification (64).
20 | P a g eGrade Definition
I Any deviation from the normal postoperative course without the need for pharmacological
treatment or surgical, endoscopic and radiological interventions. Allowed therapeutic
regimens are: drugs as antiemetics, antipyretics, analgetics, diuretics and electrolytes and
physiotherapy. This grade also includes wound infections opened at the bedside.
II Requiring pharmacological treatment with drugs other than such allowed for grade I
complications. Blood transfusions and total parenteral nutrition are also included.
IIIa Requiring surgical, endoscopic or radiological intervention not under general anaesthesia
IIIb Requiring surgical, endoscopic or radiological intervention under general anaesthesia
IVa Life-threatening complication requiring ICU – single organ failure (including dialysis)
IVb Life-threatening complication requiring ICU – multi organ dysfunction
V Death of a patient
Table 1 – Classification of Surgical Complications (Clavien-Dindo) (10)
The Comprehensive Complication Index (CCI) builds further on the Clavien-Dindo score, integrating
all events with their respective severity in an individual patient, with a resulting score from 0 to 100,
thus reflecting the total complication burden suffered by patients with multiple complications (11, 65).
Age and comorbidity have been associated with increased risk for complications (66). Low
preoperative albumin level has been identified as a strong risk factor for complications (67). Low
albumin level is associated with cachexia - loss of weight, muscle atrophy, fatigue and loss of
appetite - which is associated with cancer and a number of chronic diseases. Sarcopenia, the
degenerative loss of skeletal muscle mass, is part of the clinical picture of cachexia, and is both
associated with increased risk of complications and lower long-term survival (68).
5.3. Treatment endpoints
5.3.1. Historical perspective on endpoints in pancreatic surgery
While some surgical procedures have their origin in antiquity, pancreatic surgery, due to its
complexity, is relatively recent. In 1898, the first successful ampullary cancer resection was
performed by William Stewart Halsted at Johns Hopkins Hospital. In 1912, Walter Kausch was the
21 | P a g efirst to perform a successful partial pancreatoduodenectomy on a living patient. In 1935, at the
American Surgical Association meeting in Boston, Allen Oldfather Whipple presented the results of a
two-stage procedure for ampullary cancer with the first radical resection of the duodenum in
humans, along with resection of the head of pancreas (69). Of three patients reported, the first died
postoperatively of anastomotic breakdown, while the two others lived 9 and 25 months and died of
cholangitis and liver metastasis, respectively. In 1946, Whipple published his 10-year experience of
pancreatoduodenectomy, advocating a one-stage procedure and proposing several modifications to
his original 1935 procedure (70). He published his pancreatoduodenectomy reminiscences in 1963 (71).
Pancreatoduodenectomy (PD) is also called Whipple’s procedure.
During Whipple’s career, he performed PD 37 times with a perioperative mortality rate of 33%. From
his days and until the late 1970’s, PD was performed with mortality rates reported at around 20%
and 5-year survival of less than 5% after surgery (72). Some even suggested the abandonment of
radical surgery in favour of palliative treatment (73, 74). With fewer surgeons attempting to perform
PD, and instead referring these patients to tertiary high volume centres, perioperative mortality and
5-year survival radically improved in the 1980’s and 1990’s (75-77). The realization that soft endpoints
such as quality of life were relevant came in the 1990’s. In operated patients, a useful measure of
treatment impact was required after mortality was reduced (78). In inoperable patients, where little
improvement in response rates and survival had taken place, the focus was shifted to symptom
palliation (79). This lead to the creation of the first pancreas cancer disease specific questionnaire:
EORTC QLQ-PAN26 in 1999 (8).
5.3.2. Patient Reported Outcome
Quality of life (QoL) is the perceived quality of an individual’s daily life, an assessment of their well-
being or lack thereof. It can include emotional, social, cognitive, work- or role-related and physical
aspects of life. Health care practitioners have been interested in health related QoL (HRQoL) since
ancient times (80), but this interest has often been limited to the assessment by the doctor of the
patient’s physical abilities. With advent of HRQoL-focus in modern times, doctors collected what
they perceived to be relevant QoL issues from symptoms reported in the literature or in interviews
with colleagues, nurses and patients, then created questionnaires based on these symptoms and let
the patients themselves report on how these symptoms affected them. This is called patient
reported outcome (PRO), based on the approach that the patient knows his or her subjective
22 | P a g eexperience better than an outside observer. EORTC QLQ-C30, a questionnaire from 1993 validated
for cancer patients, is an example of such a patient reported outcome measure (PROM).
Measuring a qualitative feeling by quantitative tools may give limited information, i.e. the answers
depend on the questions that are asked; generic QoL questionnaires often rely on multidimensional
questions covering the different aspects of well-being mentioned above. A common problem in both
clinical practice and in clinical studies is that long, global QoL questionnaires are time-consuming.
Another weakness is that the dimensions and questions may be irrelevant to the patient in their
specific situation; a patient with pancreatic cancer and poor prognosis may find a question about
sexual function to be misplaced. Interest has recently shifted from global QoL to focus on the
patient's symptom burden.
Several disease-specific patient-reported symptom scores have been developed. One example is the
Myelofibrosis Symptom Assessment Form (81), a modified version of which was instrumental to the
approval by the U.S. Food and Drug Administration (FDA) of a new treatment for this disease (82).
Another example is the EULAR Rheumatoid Arthritis Impact of Disease (RAID) score, a patient-
derived PROM for rheumatoid arthritis (83, 84). This takes patient focus one step further, as the
patients themselves selected and provided a relative weight to the different items according to what
was important to them during the development.
Such a disease-specific, patient-derived and patient-reported measure has been developed by our
research group for pancreatic cancer patients; the Pancreatic Cancer Disease Impact (PACADI) score.
A preliminary validation was performed in 2013 (9). When creating a new measurement instrument,
one needs to assess if the instrument is reliable and valid.
5.3.3. Psychometrics
In the physical sciences, a measurement is the discovery or estimation of an objective value,
measured as a ratio to one of seven base units. For example, the measurement of the length of a
table could be 150 centimetres, or three halves of a meter, the base unit for length. In contrast, a
measurement in the social or psychological sciences can be defined as the attribution of a number to
a characteristic by some rule. These characteristics can be nominal, ordinal or interval scales. This
attribution can easily be subjective and erroneous. Specific criteria for measurement can be defined
to counter this. When models for measurement are created, tests to evaluate these models in
23 | P a g erelation to the specified criteria can be developed. The field of study concerned with the objective
measurement of characteristics in the social or psychological sciences is called psychometrics. This
field of study includes the construction and validation of assessment instruments, such as
questionnaires. Reliability and validity are key concepts of psychometrics and are essential elements
for determining the quality of a questionnaire. Both can be assessed statistically (Table 2).
• A reliable measure is consistent across time, individuals and situation. Consistency over
repeat measures can be assessed with the Pearson correlation coefficient or the Interclass
Correlation Coefficient (ICC). This type of consistency is also called test-retest reliability.
Internal consistency, the homogeneity of a test form (i.e. that all items relate to a common
scale), can be assessed by correlating performance on two halves of a test, termed split-half
reliability. A commonly used index of reliability is the Cronbach’s alpha, equivalent to the
mean of all possible split-half coefficients.
• A valid measure measures what is intended to be measured. One of the ways this is done is
by evaluating the responsiveness of the scale to clinical change. This can be calculated with
the Standardized Response Mean (SRM), the ratio between the mean change score and the
standard deviation of that change score. Concurrent validity is the rate of correlation of the
new questionnaire with existing well-established questionnaires, calculated for example by
Spearman’s rank coefficient correlation (Spearman’s rho). Discriminant validity is the ability
of the questionnaire to measure characteristics in a specified group, but not in other groups.
A simple t-test can calculate this for two groups, or the analysis of variance (ANOVA) can be
used for three or more groups.
Psychometric concept Meaning if high Statistical tool used to test
Test-retest reliability Consistent across time Interclass correlation coefficient (ICC)
Internal consistency Items relate to common scale Cronbach’s alpha
Responsiveness to change Measures what is intended Standardized Response Mean (SRM)
Concurrent validity Correlates with existing scales Spearman’s rho
Discriminant validity Specific to one group Student t-test or ANOVA
Table 2 – Psychometric concepts, what it means if a questionnaire scores a high score for that
concept, and which statistical tools are used to test each concept
24 | P a g e6. Thesis aims
The general aim of the thesis was to explore the role of PROMs in the management of resectable
pancreatic cancer patients.
The specific aims were:
I. To investigate whether preoperative PRO could predict survival in patients with pancreatic
ductal adenocarcinoma
II. To explore the consequences of postoperative complications on long term survival and PRO
after pancreatic surgery, secondarily to examine the feasibility of existing PROMs in our
cohort
III. To study the psychometric performance of a new short, patient derived, disease-specific
PROM in patients with pancreatic cancer
25 | P a g e7. Materials and methods
7.1. Ethics
The research protocol was approved by the Regional Ethical Committee for Medical and Health
Research (REK, ref. 265-08412c). All participants were included after signing written informed
consent. Confidentiality and data protection were approved by the Norwegian Data Protection
Authority (Datatilsynet, ref. 08/01409-2/MHN), with concession until the 31st of December 2058.
7.2. Study design: Thematic Pancreas Tumour Project (TPTP)
In October 2008, Oslo University Hospital established a multidisciplinary research program (Thematic
Pancreatic Tumour Project (TPTP)). It is a prospective observational cohort study, including all
patients referred with solid or cystic pancreatic or periampullary tumours. While both surgically and
non-surgically treated patients were included in the project, Paper I and II focused solely on patients
who underwent surgery.
All patients underwent evaluation at the multidisciplinary meeting. Preoperative workup included
physical examination, routine laboratory tests including tumour markers, and a standard protocol for
CT, optimized for imaging pancreatic tumours (85). In addition, chest CT was performed to assess
pulmonary metastasis. During the first years of TPTP, tumours infiltrating the SMV or PV were
considered resectable if there was a patent vein above and below the infiltrated site to allow
reconstruction (86), while metastatic tumours and tumours with infiltration of the celiac trunk or SMA
were considered unresectable (87). Tumours were never considered borderline resectable for our
patients included between 2008 and 2011 (Paper I and II), as international definitions of this concept
were published during the inclusion period. For patients included after 2012, borderline resectable
patients were defined as patients with venous infiltration with patent vein above and below the
infiltration, gastroduodenal artery encasement up to the hepatic artery without extension to the
coeliac artery, or tumour abutment to the SMA of less than 180° of circumference (88). Histological
diagnosis for borderline tumours was confirmed with endoscopic ultrasound fine needle aspiration
(EUS-FNA) (89). Folfirinox, Gemcitabine/Nab Paclitaxel or Gemcitabine monotherapy were given as
neoadjuvant treatment (90). If tumour size was stable or smaller after neoadjuvant treatment,
patients underwent surgical exploration. Preoperative percutaneous biopsy / cytology was not
performed in primary resectable patients; it would not have altered treatment recommendation as
26 | P a g epancreatic cancer cannot be ruled out by biopsy (91). Patients with cystic lesions underwent
endoscopic ultrasound (EUS), and if possible, aspiration of cystic fluid for cytology and biochemical
analysis. Tumours in the body or tail were preferably resected laparoscopically while open PPPD was
preferred for lesions in the head. Intraoperative evaluation of surgical approach for vascular
reconstruction was done in cooperation with the liver transplantation team or vascular surgeons.
The pancreatic resection margin was investigated intraoperatively by frozen section procedure. Total
pancreatectomy was chosen only when mandatory to achieve free resection margins. For
unresectable patients, percutaneous biopsy or cytology was recommended in all cases, but some did
not accept it. These patients were referred to the local hospital Department of Oncology for
palliative treatment. Patients with pancreatic adenocarcinoma who underwent curative surgery
received adjuvant chemotherapy (92) according to the Nordic FLV regimen (5-fluorouracil/leucovorin
every 2nd week for 6 months). Follow-up included a chest and abdominal CT scans every sixth month
or if the patient had symptoms indicating recurrence.
We recorded clinicopathological data such as age, sex, preoperative diabetes mellitus, preoperative
jaundice, TNM-stage, LNR, resection margin, type of surgery, postoperative morbidity, recurrence
and survival. In addition, our cohort includes patent reported outcomes such as ESAS, EORTC QLQ-
C30, PAN26 and an increased use of the PACADI-score throughout the study period. In addition,
sampling of blood, tumour tissue, cyst fluid and bone marrow was performed for translational
research in the TPTP. Patients who were unable to provide informed consent were not included.
7.3. Population and measures
7.3.1. Paper I
We extracted all patients from the cohort who received potentially curable surgical treatment for
PDAC from October 2008 to December 2011. A total of 66 patients were identified. We excluded
patients who did not have presurgery ESAS, EORTC QLQ-C30 and PAN26 data (n=22). There was no
significant difference in core clinicopathological parameters or survival between the 44 included and
22 excluded patients.
For those 44 patients included in the study, EORTC raw scores were calculated using the
recommended EORTC procedures (93). PRO-scores and scales were transformed to continuous scales
27 | P a g efrom 0 to 100%. For cognitive function scores, we chose 66.67% as a cut-off to divide our population
into “high”5 (n=30) and “low”6 (n=14) cognitive function.
7.3.2. Paper II
In the second paper, our focus was not solely on those patients with a final diagnosis of PDAC;
instead, all patients between October 2008 and December 2011 who underwent surgery were
included. In this way, a total of 208 were identified and included in the study. Between the
publication of Paper I and writing Paper II, some patients were reclassified. Sixty-nine patients were
initially identified as receiving surgical treatment for PDAC in the study period, but 3 patients were
excluded from Paper I for metastatic disease diagnosed during surgery, with excision of metastasis.
Of the 66 patients, one was reclassified from pancreatic cancer to bile duct cancer after publication.
Six patients with periampullary cancers were reclassified to PDAC. This gives us a final total of 74
PDAC patients operated between September 2008 and December 2011. A TPTP research paper has
been published on reclassification of diagnosis (94).
In addition to baseline PROMs, follow-up ESAS, EORTC QLQ-C30 and PAN26 questionnaires were
mailed to each patient every third month postoperatively, with no end date. No reminders were
sent and no external incentives were provided.
Complications were classified according to the Clavien-Dindo classification, based on therapeutic
consequences of the complication (95). This classification was used to calculate each patient’s CCI
score (11, 96), an aggregate score from 0 to 100 based on severity and number of complications. There
was no significant difference in American Joint Committee on Cancer (AJCC) stage between patients
with and without complications in the PDAC subgroup.
7.3.3. Paper III
In the last paper, all patients with suspected pancreatic cancer, both operable and inoperable,
included in the cohort between 2012 and 2016 were selected. The aim was to include 200 patients
with confirmed PDAC. A total of 360 patients were included, divided into three diagnostic groups:
5
EORTC QLQ-C30 Cognitive Function score 100% and 83.33%
6
EORTC QLQ-C30 Cognitive Function score 66.67%, 50%, 33.33%, 16.67% and 0%
28 | P a g e210 with PDAC, 109 other types of pancreatic and periampullary malignant lesions and 41 patients
with non-malignant lesions.
In addition to core clinical data, the PACADI score (9) was collected at baseline (inclusion) and after 1,
2, 3, 6, 9 and 12 months (follow-up). Other PROMs collected in the case report form were the EQ-
5D(12) and ESAS(6). These were used as comparison as they are commonly used and of similar length
to the PACADI questionnaire.
7.4. Statistics
Statistical analyses were done with Stata SE versions 13-15.
7.4.1. Paper I
The objective was to investigate whether preoperative PROMs could function as prognostic factors
for survival. For determining individual prognostic value of PROM items, we started by eliminating
parameters with a p-value of > 0.20 in univariable Cox regression analysis. The remaining
parameters were then included in a multivariable Cox regression model with the stepwise
backwards method, where the parameter with the highest p-value was omitted at each step until
only PROM items with statistical significance (p < 0.05) were left. These were then adjusted for
possible core clinicopathological data confounders with multivariate Cox regressions analysis.
When comparing medians of continuous variable we used the Mann-Whitney test (Wilcoxon rank-
sum). Dichotomous variables were compared using the Pearson chi-squared test or the Fisher mid-p
test, if all expected counts were above five or at least one was less than five, respectively. Ordered
categorical variables were compared with Mann-Whitney test and the chi-squared test was used for
unordered categorical variables. To estimate median survival times we used the Kaplan-Meier
estimator, while the reverse Kaplan-Meier method was used to estimate follow-up time.
7.4.2. Paper II
The main focus in the second paper was to investigate whether complications in pancreatic surgery
had long-term effects on survival or patient reported outcome. Change in longitudinal PRO was
initially visually examined using box-plots and scatterplots. The difference in PRO from baseline to 3
months and from baseline to 6 months was compared to CCI using linear regression. Correlation
29 | P a g ebetween CCI and length of hospital stay was estimated with Spearman’s correlation. Mann-Whitney
test (Wilcoxon rank-sum) was used to compare independent continuous variables, without assuming
normal distribution. Chi-squared test was used to examine the relationship between categorical
variables. The Kaplan Meier estimator was used to estimate median survival times. To assess a
variable’s association to survival, Cox regression was used.
7.4.3. Paper III
This study was done to investigate the psychometric performance of the PACADI score.
For test-retest reliability, the ICC was calculated on patients who reported no subjective perception
of change from baseline to 1 month, with a global anchor question.
For internal consistency, we calculated Cronbach’s alpha across dimensions both for PACADI and EQ-
5D at baseline and follow-up.
We also examined responsiveness to change with SRM in the subset of patients who reported
improvement (on the global anchor question). It was calculated as the change in outcome measured
from 2 to 3 months divided by the standard deviation of the change, with Cogen definitions for
effect size used for SRM (97).
Spearman’s rho was used in cross-sectional analysis to examine concurrent validity, as the data were
not normally distributed.
ANOVA was used to compare the three diagnostic groups and to examine discriminant validity of
PACADI, EQ-5D and ESAS “sense of well-being”. Each diagnostic group was also compared to the
other using independent samples t-test.
Longitudinal changes in PRO were analysed from baseline to each time point without imputation for
missing data, using paired sample t-test.
Finally, we used Cox Regression to examine the predictive value of the three PROMs, with early
death (survival8. Synopsis of results
8.1. Paper I
Only six PROM items had a p-value < 0.20 in univariate analysis and were selected for further
analysis, Cognitive Function (CF) score in EORTC QLQ-C30 remained as the only factor significantly
associated with survival in multivariate analysis. When comparing “high” and “low” CF, the hazard
ratio of dying was 3.5 times higher in the latter (p=0.001). Median survival for patients with “low” CF
and “high” CF was 10 months and 21 months respectively (p9. Discussion
9.1. Methodological considerations
In Paper I, our main finding is the strong prognostic role of preoperative cognitive function.
However, the measurement of cognitive function in our study is limited to items 20 7 and 25 8 in the
EORTC QLQ-C30 questionnaire, which form the Cognitive functioning scale (93). No universally
accepted and standardized cognitive assessment measure for the evaluation of cancer-associated
cognitive impairment exists today (98). While the EORTC QLQ-C30 Cognitive function score is a
subjective measure of cognition, the International Cognition and Cancer Task Force (ICCTF) (99) has on
the subject of assessment of cognitive effects of cancer noted that objective neuropsychological
tests remain the gold standard for measuring cognitive function (15). Research has shown a stronger
association between subjective reporting of cognitive dysfunction and mood or fatigue than
between subjective complains and objective tests of cognitive function (14). To improve research
design and facilitate meta-analyses, the ICCTF recommends a standard battery of tests. This includes
the Hopkins Verbal Learning Test-Revised (HVLT-R), Trail Making Test (TMT) and the Controlled Oral
Word Association (COWA) of the Multilingual Aphasia Examination to test learning memory,
processing speed and executive functions. They encourage investigators to supplement this core of
tests with additional tests of working memory based on own preferences. Further studies on
cognitive function in pancreatic cancer patients should include objective tests.
In Paper I, for further analysis of cognitive function as a predictor, patients were divided into two
categories; “high” CF and “low” CF, as such a dichotomy would facilitate simple presentation of
results, e.g. with Kaplan-Meier survival estimates. However, dichotomization of continuous variables
is discouraged by statisticians, as it may lead to loss of information, misclassification and erroneous
effect sizes (100, 101). At the time, we were unaware of the costs of dichotomization. Although
dichotomization is generally discouraged, it can sometimes be justified; when analysis provides clear
support of the existence of two distinct classes with a clear cut-off point, and when the distribution
of a count variable is highly skewed (101). The cut-off in our study was selected by analysing each
distinct score with Kaplan-Meier plots; patients scoring either of the two high scores (100% or 83%)
had similar survival estimate curves, while patients in the low scores (66.67%, 50%, 33.33%, 16.67%
7
EORTC QLQ-C30 question 20: Have you had difficulty in concentrating on things, like reading a newspaper or
watching television?
8
EORTC QLQ-C30 question 25: Have you had difficulty remembering things?
32 | P a g eYou can also read