THE PROBLEM AND RESOLUTION OF THE OPIOID ADDICTION EPIDEMIC - CHARLES H. PIERCE, MD, PHD, FCP, CPI - COLLEGE OF MEDICINE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Problem and Resolution of
the Opioid Addiction Epidemic
Charles H. Pierce, MD, PhD, FCP, CPI
University of Saskatchewan
College of Medicine, Class of 1968
1 March 07
Disclosure
I confirm that I have no
financial relationship or
conflict of interest in
relation to this talk-
educational activity ... just
the will to educate and that
to your right...
2
Learning Objectives
▶ Understand the nature and management of Opioid
Addiction
▶ Describe the most effective way to view the Addict
▶ Compare the addictions of the many different
agents
▶ Explain why Buprenorphine is effective in the
management of Opioid Addiction
▶ Determine the method of discontinuing the
Buprenorphine program
▶ Evaluate your success in changing a life
3
Topics/Areas I will cover
▶ What is this disease called “Addiction”?
▶ Role of cigarette smoking? An Addiction
▶ Is Marijuana included as an Addiction?
▶ What’s this Drug / Opioid Epidemic all about?
▶ The Treatment / Management of Addiction
▶ The Role of us Docs in this epidemic?
4
“Addiction Defined“
5 August 05
Disease = Addiction ?
▶ Definition of “Disease”: Any deviation from or interruption of
the normal structure or function of any body part, organ, or
system that is manifested by a characteristic set of symptoms
and signs and whose etiology, pathology, and prognosis may
be known or unknown.
▶ ASAM Definition of the “Disease of Addiction”: addiction is a
primary, chronic disease of the brain reward, motivation,
memory and related circuitry. Dysfunction in these circuits
leads to characteristic biological, psychological, social
and spiritual manifestations.
▶ The definition fits and both can be fatal without treatment.
SUD costs Americans >$700 Billion/year in increased health
care costs, crime, and lost productivity
6
Addiction is a Disease - of the Brain
▶ Addiction is a chronic relapsing brain condition with
strong genetic and environment components that
affects memory, motivation and inhibition...
▶ This is a physical condition, not caused by a lack of
willpower or morals and not cured by good advice.
▶ Substance Use Disorder (SUD) is a general CNS
disease as over time, nerve cells in the brain ‘learn’
to crave opiates and other substances.
▶ SUD: a chronic & treatable disease affecting 20.8 M
Americans, like diabetes and heart disease and
should be viewed from the same portal.
7
Genetic factors account for between 44-60 % of a person's vulnerability to addiction, including the effects of environment on gene expression and function.
Substance Use Disorder / Addiction ?
The Hallmarks of the SUD / Addiction epidemic
▶ Genetic and environmental factors
▶ Chronic and relapsing - by definition
▶ Craving and binging - a hallmark
▶ Brain and chemistry changes
▶ Tolerance requiring more of the same for effect
▶ Drug availability: parents, friends have influence
▶ Consequences include stigmatization
9
For SUD: Language Matters
Stigmatizing words and Phrases should be discouraged
and replaced in the minds of everyone ...
‘Abuser’
▶ negates that SUD is a medical condition and ignores the
environmental, genetic and psychological factors
▶ Tends to absolve the supplier.
▶ Use ‘misuse’, ‘inappropriate use’, ‘hazardous use’,
‘problem use’, ‘risky use’
‘Addict’, ‘Drug Addict’, ‘Junkie’, ‘Degenerate’, ‘Dope
Fiend’, ‘Crackhead’ should never be used/considered
▶ No distinction between the person and their disease
▶ Denies the dignity and humanity of the individual
▶ Suggests permanency.
10Opioid Use Disorder - Criteria
1.Opioids taken in larger amounts/longer time than intended
2. Persistent/unsuccessful desire / efforts to cut down dose
3. Excess time is spent to obtain, use or recover from effects
4.Craving, or a strong desire or urge to use opioids
5.Recurrent use resulting in failure to fulfill roles at work, home
6.Continued use despite social / interpersonal problems caused
7. Social, occupational or recreational activities reduced due to..
8. Recurrent opioid use in situations that may be hazardous
9. Continued use despite persistent or recurrent physical or
psychological problem most likely cause by the substance
10.Tolerance i.e. a need to increase the amount for effect and a
diminished effect by the same dose
11.Physical Dependence...
11Ask and you will know
Questions I ask every patient as they start MAT
Have you ever overdosed? Ever given Narcan?
How old were you when you first became addicted?
How did you start? – with what agents?
Did either of your parents have a problem with ... ?
Does your partner have trouble with drugs or alcohol?
Are you presently working?
Do you use Marijuana? For how long?
Do you smoke or chew tobacco? For how long?
12How Did the Epidemic Start?
▶ Addiction is an medical state or condition that
is partially Doctor induced.
▶ 91,000,000 Rx in 1991 to
▶ 219,000,000 Rx in 2011 to
▶ 300,000,000 Rx in 2017
In 2017 the US experienced a 12% drop in
prescription Opioid dosage volume, which was the
steepest annual decline in 25 years
I ask every patient I see how and when they first
realized they were addicted and how. The answers
will surprise everyone.
13Canada Leads North America
There are a number of items/programs that Canada
is ahead of the US in:
▶ In March of 2016, the Canada made the overdose-
reversal drug naloxone a non-prescription agent!
▶ In BC, naloxone is available at no cost through
community agencies and pharmacies. Basis of need
▶ Led by BC, Canada now facilitates the development
of medically supervised injection facilities.
▶ BC now funds publicly available anonymous drug-
testing services i.e. users can test before using.
▶ Education must apply to all health care providers
14Risk Factors for Opioid Abuse
▶ Use
of Prescription controlled opiate agents and/or
Benzodiazepines
▶ Use of Alcohol and Tobacco
▶ History of Sexual Abuse female > male
▶ Familyhistory of Substance Abuse or a Psychiatric
disease diagnosis
▶ Age 16 – 45 years and male > female
15The Opioid Risk Tool (ORT)
1. Family Hx of Substance Abuse F M
Alcohol ☐1 ☐3
Illegal Drugs ☐2 ☐3
Prescription Meds ☐4 ☐4
2. Personal Hx of Substance Abuse
Alcohol ☐3 ☐3
Illegal Drugs ☐4 ☐4
Prescription Meds ☐5 ☐5
3. Age between 16 and 25 ☐1 ☐1
4. Hx of Adolescent Sexual Abuse ☐3 ☐0
5. Psychological Disease
ADD, OCD, BiPolar, Schizoph ☐2 ☐2
Depression ☐1 ☐1
16Addiction Statistics - 2016
Estimates on the Number of Deaths
▶ Opiates 62,000 >1/3 in age 25-34 years
▶ Alcohol 80,000
▶ Tobacco 440,000
Probability of ‘Addiction’ after the First Use
▶ Tobacco 32%
▶ Heroin 23%
▶ Cocaine 17%
▶ Alcohol 15%
▶ Cannabis 9%
17Cigarette Smoking
Smoking two packs of cigarettes daily is
linked to an almost fivefold risk of stroke.
18 August 05The Addiction of Smoking
90% of smokers start in their teens with the
average age of Starting at 13-15 Years old
Why?
▶ Advertising
▶ Endorsement
▶ Product Placement
▶ Special Tobacco Formula
▶ To be ‘cool’
▶ Because my friend does it
▶…
19Must Really be “Cool” to Smoke
A
20Believe it or not
21The End-Result of Nicotine Use
“Nicotine addiction is the second-
leading cause of death worldwide.”
The important causes of smoking-
related mortality are atherosclerotic
cardiovascular disease, cancer, and
chronic obstructive pulmonary disease
(COPD).
Forewarned is Forearmed
Ref: www.CDC.gov
22What to you get for your money??
Bad Breath
Lung Problems
▶ Emphysema
▶ COPD
Marked increase in Heart Disease (#1 Killer)
Marked increase in Cancer
▶ Lung
▶ Throat
▶ Mouth
▶ Stomach
▶ Intestinal
And on and on… every part of your body.
23Recommended Office Poster
Marijana / Marihuana
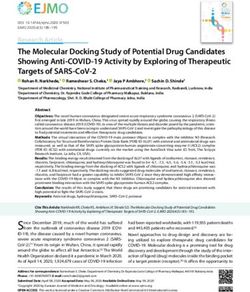
25 August 05Cannabis is a lot more than THC
The Cannabis plant includes more than 400 different
chemicals, of which about 70 are cannabinoids.
▶ Typical government-approved medications contain
only one or two chemicals.
▶ The number of active chemicals in cannabis is one
reason why treatment with cannabis is difficult
A 2014 review stated that the variations in ratio of
CBD-to-THC in botanical and pharmaceutical
preparations determines the therapeutic vs
psychoactive effects (CBD attenuates THC's
psychoactive effects) of cannabis products
26Cannabinoids
Pharmacologically active ingredients
THC: Δ9-Tetrahydrocannabinol
▶ Euphoria and psychosis
▶ Marinol® to improve appetite
Cannabidiol (CBD)
▶ Not Psychoactive
▶ POSSIBLE Antianxiety & Antipsychotic
Therapeutic effects vary greatly
▶ Depend on [THC]
▶ Ratio of THC:Cannabidiol
ü Cannabidiol can mitigate psychoactive effects of THC
27Legal status of Marijuana
A
Ref:
28.
29Use of Drugs leading to SUD
What agents started an individual down the path of
wanting and using illicit drugs (study of 2.8M with SUD)
▶ Marijuana 70.3%
▶ Pain Relievers 12.5%
▶ Inhalants 6.3%
▶ Tranquilizers 5.2%
▶ Stimulants 2.7%
▶ Hallucinogens 2.6%
▶ Sedatives, Cocaine 0.3%
30Once Medically Available ...
The argument against legalization
▶ Addictive nature is such that 10% of users are likely
to develop dependence - increasing HC costs.
▶ Health concerns - The brain, the heart, the lungs,
and mental health. This is not to be taken lightly.
▶ After effects such as a distorted perception triggering
accidents or as a gateway/start to more serious drugs.
▶ Safety of children who get into almost anything
around the house or on the street +/- supervision
▶ Unintended consequences is when added to
‘candy’, an “overdose” is considerably more likely
31Marijuana Candy and Gummies
Is this what you want your kids to consume?
32The Result of Legal Marijuana
A
33Methamphetamine 34 August 05
Methamphetamine
Also called Chalk, Crystal, Glass, Ice, Meth, Speed ...
▶ This is a very addictive stimulant.
▶ It is a pill, powder, crystal that can be ingested,
snorted, injected or smoked in a small glass pipe.
The METH rush and good feelings get soon replaced by
edginess, excitement, anger, fear. “Addiction” follows
quickly with increased body temperature, BP, HR, Itching,
emotional problems and a big problem in decision making
METH and MDMA (2,4 methyldioxyMeth (ecstacy)
has a strong relationship to ‘high-risk’ sexual behavior
in HIV/AIDS due to judgment Lapses
It has been added to Marijuana to the surprise of users
35The Drug / Opioid Epidemic
36 August 05Yes, Opioid Addiction is Serious
Opioid dependence affects nearly 5 million people in
the US and leads to almost 64,000 deaths annually
(2016).
According to the CDC, the death rate from overdose tripled
from 6.1/100,000 in 1999 to
19.8/100,000 in 2016.
Number of fatal overdosing from Fentanyl and other synthetic
opiates more than doubled from 2015 (9K) to 2016 (19K)
Half of the deaths due to drug overdose are related to Rx.
80% of Heroin users report misusing prescription
opioids prior to heroin.
37“Addiction” Starts in Many Ways
Individuals who have an “addiction” to:
▶ Alcohol are 2 times...
▶ Marijuana are 3 times...
▶ Cocaine are 15 times...
▶ Pain Reliever Meds are 40 times...
... More likely to get addicted to Heroin than others
It is said that 4 of 5 heroin users started out being
prescribed opioid pain medications
38For Every Problem, A Solution
▶ Too Many Prescriptions - in 2015 enough was prescribed to
cover every American for 3 weeks – 640 MME per person
Fewer Prescriptions - use only when benefits likely to
outweigh the risk. Consider Non Opioid and/or PT...
▶ Too Many Days Rx - more than 3 months increases the risk of
addiction 15 times
Fewer Days of Rx - consider 3-4 days and taper
▶ Too High a Dose – Doses > 50 MME per day doubles the risk of
Overdose. Doses at 90 MME Increase the risk 10 times
Lower Dosage Rx – Use lowest effective dose of
immediate release agents. Avoid a daily dose of 90 MME
or more or taper to a safer dose
39New Prescribing Rules (MD, DO, PA)
1. No more than 7 day Rx on First Prescription (Rx)
2. No more than 5 day Rx for minors + parent consent
3. No excess of the days supply unless patient
records clearly document a valid reason
4. Total MED of Rx cannot exceed avg. 30 MED/day
5. Limits do not apply to opioids Rx for cancer,
palliative care, end of life/hospice care or ...
In addition, on the RX there must be at least 4 of the 7
ICD-10 code digits for the Diagnosis or Procedure and
the number of days supply - actually written on the Rx
40ICD-10 Codes typically used
F11.20 Opioid dependence, uncomplicated ✔
F11.21 Opioid dependence, in remission ✔
F12.19 Cannabis abuse with unspecified cannabis-Anxiety
F12.92 Cannabis use, unspecified with intoxication
F14.90 Cocaine use, unspecified, uncomplicated
F15.10 Other stimulant abuse, uncomplicated (METH, Amph)
F17.201 Nicotine dependence, cigarettes, uncomplicated
F41.9 Anxiety Disorder, unspecified
F43.10 Post-traumatic stress disorder, unspecified
N94.3 Premenstrual Tension syndrome
O09.33 Tobacco use (smoking) during pregnancy, childbirth..
B19.2 Unspecified viral hepatitis C
41Where to Individuals Get Opioids
The source of the most recent Opioid:
▶ 54% Given, bought, or taken from a friend or
Relative
▶ 36% By a Rx or stolen from a Health Care
Provider
▶ 5% Bought from a Dealer or Stranger
▶ 5% other than the above
Ref: SAMSA 2015
42Drug Source relationship
A
Ref: SAMHSA, cited in Tetrault, Butner, 2015
43What are the Common Opiates?
.
methadone
Dolophine
heroin
hydromorphone
Dilaudid
Morphine Buprenorphine
MS Contin Suboxone/Subutex
Bunavail/ Zubsolv hydrocodone
Vicodin
Codeine
Tylenol # 3
oxycodone
Oxycontin &
Percocet
44And then there is Fentanyl +
Fentanyl and fentanyl analogues include the following:
▶ Fentanyl* (65% of T) ▶ despropionyl-fentanyl
▶ acetylfentanyl ▶ furanyl-fentanyl
▶ butyrylfentanyl ▶ Norfentanyl
▶ Carfentanil ▶ 3-methylfentanyl
Many of these show up when least expected and OD
deaths from Fentanyl is considered and advertisement
Keep in mind that even metabolites can be active:
▶ Dihydrocodeine
▶ Monoacetylmorphine
▶ Norbuprenorphine
45Fentanyl !!!
▶ TheOMHAS has issued an advisory (21Feb18) on
the marked increase of “fentanyl-related OD deaths
when non-opioids are known to be involved
▶ One of the 20+ forms of Fentanyl has been found in
▶ Heroin
▶ Cocaine - (powdered Crack)
▶ Marijuana
▶ Methamphetamine
▶ MDMA - (powdered Estacy)
▶ Rx? opioids, sedatives, and hypnotics
We now administer naloxone in all drug overdoses
as the Liklihood of Fentanyl is that high!
46Opioid Potency
Fentanyl & Carfentanil
often in Marijuana èè
47How Bad is the Opioid Epidemic?
This “Epidemic” has been called the worst drug
crisis in American and Canadian History with deaths
now rivaling those from AIDS in the 1990s
▶ In ‘99 there was more than twice as many motor
vehicle deaths as fatal drug overdoses.
▶ These numbers flipped in 2008 and by 2014 there
was almost 40 percent more deaths from overdoses
(47,055) than car crashes (29,230)
▶ Cocaine used to be the leading killer but now Heroin
and prescription opioids lead. *
▶ By 2014 Opioid deaths were up 369% and
Heroin deaths were up 439%
48Some Surprises from the CDC
A
49▶P
Age-adjusted drug overdose
Death rates by state, 2016
50Rx / 100 Persons in US
A
199 MME in 1999
640 MME by 2015
51▶
Age-adjusted drug overdose
Death rates by Province, 2016
52Canada Leads North America
There are a number of items/programs that Canada
is ahead of the US in:
▶ In March of 2016, the Canada made the overdose-
reversal drug naloxone a non-prescription agent!
▶ In BC, naloxone is available at no cost through
community agencies and pharmacies. Basis of need
▶ Led by BC, Canada now facilitates the development
of medically supervised injection facilities.
▶ BC now funds publicly available anonymous drug-
testing services i.e. users can test before using.
▶ Education must apply to all health care providers
53Age adjusted Death Rates
▶P
54OD Death Rates by Age group
55Overdose kills
Actual case in 2016
56“You are not alone”
Over 800,000 people in the US are dependent on
heroin or other opiates. The number in Canada is a
similar percentage of the population as in the US
For an overdose (OD) there is naloxone* (Narcan,
Evzio), 0.4-2 mg iv/im/subq not to exceed 10 mg
which is available in several forms:
▶ Narcan - 4mg/actuation non aerosol spray
▶ naloxone - 0.4 mg/ml soln. or 1.0 mg/ml syringe
▶ Evzio - 0.4 mg/0.4 ml auto-injector, 2.0 mg/0.4 ml
*Available in Canada without a Prescription/OTC
57Treatment / Management of
Drug Addiction
58 August 05Medicated Assisted Treatment
▶ MAT is the use of medications, in combination with
counseling and behavioral therapies, to provide a
“whole patient” approach to the treatment of SUD
▶ The combination of meds and therapy is successful
in treating those struggling with addiction.
▶ MAT is used primarily for the treatment of addiction
to opioids (Heroin and Rx pain meds with opioids)
The meds normalize brain chemistry and block
the euphoric effects, relieve physiologic craving,
and normalize body functions without the negative
effects.
59Drug Abuse Treatment Act (DATA)
When prescribing buprenorphine et al TO TREAT
ADDICTION, a physician must have a DATA 2000
Waiver, also called an “X-DEA number” à
Ref: 21 U.S.C. 823(g)
DATA 2000 Waiver can be obtained by any physician
by taking an 8-hour online course and passing a test.
You can treat 30 patients/yr. with buprenorphine et al in
year 1, and 100 patients/yr. starting in year 2, and from
Aug 2016 275 Patients/yr. from year three on.
Ref: http://www.samhsa.gov/medication-assisted-treatment
As of 14Feb18 there are only 46,500 waivered docs
Ref: MedPage Today February 14, 2018
60Certified Physicians by Waiver Level
DEA
As ofCertified MD/DO (n=41,170)
March 2018
30 (28,068) 100 (9,110) 275 (3,992)
10%
22%
68%
Capacity: 2,850,840
March 2018
61Clinical Opiate Withdrawal Scale
To determine the withdrawal state prior to Rx
▶ Resting Heart Rate ▶ GI Upset
▶ Sweating ▶ Tremor
▶ Restlessness ▶ Yawning
▶ Pupil size ▶ Anxiety or Irritability
▶ Bone or Joint aches ▶ Goose Flesh skin
▶ Runny nose or tearing
Total score ______
5-12=mild, 13-24=moderate, 25-36=moderately severe, >36=wow
62Use of Buprenorphine
Buprenorphine blocks other opiates and prevents
physical craving for those opiates. Many people
describe feeling “normal” or “energized” when
they take their buprenorphine regularly.
▶ Buprenorphine: is an opiate that acts to fill up the
brains opiate mu receptors without causing
sleepiness or “high” feelings. It has a low risk of
overdose.
▶ Naloxone: a drug that is not absorbed orally but
helps persuade people to not inject Suboxone in a
vein as it causes instant withdrawal.
63Buprenorphine Knowledge
▶ BUP is a semisynthetic, highly lipophilic thebaine
derivative, which is a Partial µ-agonist but >
naloxone and an antagonist at the kappa receptors
▶ Mu-opioid receptor activity produces the analgesic
effects of BUP, which is 25-50 times more potent
than morphine.
▶ BUP is metabolized through the CYP3A4 system so
attention must be paid to the potential for significant
drug interactions among other meds that are
substrates, inhibitors, or inducers of his system.
64Buprenorphine (BUP) Products
Buprenorphine is a unique opioid analgesic that comes
in many dosage formulations - most transmucosal use
1. Suboxone® - BUP/Naloxone - sl film, 2/.5, 4/1, 8/2, 12/3 mg
2. Buprenorphine/Naloxone - (generic) - sl tablet, 2/.5, 8/2 mg
3. Bunavail® - BUP/Nalox - buccal film, 2.1/.3, 4.2/.7, 6.3/1 mg
4. Zubsolv® - BUP/Nalox - sl tablet 1.4/.36, 5.7//1.4 mg
5. Buprenorphine - BUP (generic) – sl tablet 2, 8 mg
6. Subutex® - BUP - sl tablet, 2, 8 mg
7. Buprenex® - BUP – iv, im, 0.3 mg/ml
8. Sublocade® - BUP - subq injection/month, 300 mg, then 100 mg
9. Probuphine® - BUP - an implant, 74.2 (80) mg X 4
65The half-life is around 36 hours i.e.
taken once a day it takes a week for
maximum effect or to be eliminated
66How to take tablet or the strips (film)*
Plan on 35-40 minutes of “Quiet Time” alone
Do not smoke for 20-30 minutes prior to taking the
medication as tobacco is a vaso-constrictor thus inhibiting
absorption.
Rinse your mouth with warm water (vasodilator) prior to
taking the dose, which promotes absorption
After placing the tablet or strip under your tongue, to
ensure absorption of the agent (Buprenorphine) you
need, for 15-20 Minutes you must:
▶ Not drink anything
▶ Not smoke or use any form of tobacco
▶ Not swallow the tablet remains or your saliva
67Screening Tests Each Visit
Systems vary but the following are tested regularly
▶ BUP -Buprenorphine ▶ OPI- Opiates
▶ AMP -Amphetamine ▶ MOP -Heroin
▶ MET -Methamphetamine ▶ COC -Cocaine
▶ BZO -Benzodiazepine ▶ BAR -Barbiturates
▶ OXY -Oxycodone ▶ THC -Marijuana
▶ TCA -Tricyclic Antidepress. ▶ MTD -Methadone
On Further testing? ng/ml on above plus surprises
▶ Norbuprenorphine ▶ MDMA (estacy)
▶ Gabapentin
▶ Pregablin
▶ Fentanyl !!!
68Meds NOT to be taken with BUP
Benzodiazepine’s top the list:
▶ Valium (diazepam)
▶ Ativan et al (lorazepam)
▶ Xanax et al (alprazolam)
▶ Klonopin (clonazepam)
▶ Celexa (citalopram)
▶ Ambien et al (zolpidem)
▶ Adderall (amph/dextroamph)
▶ Catapress et al (clonidine)
▶ Cymbalta (duloxetine)
▶ Flexeril (cyclobenzaprine)
A total of 1047 drugs (5868 brand and generic names)
have been fund to interact with Buprenorphine
69Along with Buprenorphine
Stopping the Physical craving is just the beginning
Changing thinking followed by the behaviors
associated with the SUD is the process of “Recovery”
Recovery process requires Psychological and
Psychiatric Counseling/therapy. Group counseling has
the advantage as the patient sees beyond her/himself
Individual Counseling plus Group-therapy may be the
only way to learn to cope with the pain, blame and
shame linked to addiction. It is a safe and tested way to
treat depression or to face abuse that may have occurred
in the patients past.
70Now You Know
Thank you for listening
In the US- FDA = 800-332-1088
Health Canada = 866-234-2345
http://Dr.Pierce1.net
Charles@Pierce1.net
71Selected References
▶ American Society of Addiction Medicine Opioid Addiction (2016) Facts & Figures
http://www.asam.org/docs/default-source/advocacy/opioid-addiction-
disease-facts-figures.pdf
▶ Dowell D, Haegerich TM, Chou R. (2016) CDC Guideline for Prescribing Opioids
for Chronic Pain - United States, 2016. MMWR Recomm Rep 2016;65(No.
RR-1):1–49. DOI: http://dx.doi.org/10.15585/mmwr.rr6501e1
▶ National Institute on Drug Abuse (NIDA) https://www.drugabuse.gov/
▶ Rebecca Voelker, MSJ (2018,) Monthly Buprenorphine Injection Approved for
Opioid Use Disorder,. JAMA. 2018;319(3):220. doi:10.1001/jama.2017.20647
▶ Physician Clinical Support System (PCSS)-National Mentor for Physicians
Treating Opiate Dependence. http://www.PCSSmentor.org
▶ Joshi V, Suchin, V, Lim, J, (2017), Smoking Cessation: Barriers, Motivations and
the role of Physicians - A Survey of Physicians and patients, Sing Health Center
for Health Serv. Res.
▶ Pierce, CH, (2018) The Pre-Menstrual (PMS) Treatment is Unmasked and it is
Simple and Safe. Arch Clin Med Case Rep.; 2(1):1-4 doi: 10.26502/acmcr.016
72Selected References
▶ Hedegaard H, Warner M, Miniño AM. (2017) Drug overdose deaths in the United
States, 1999-2016. NCHS Data Brief, no 294. Hyattsville, MD: National Center for
Health Statistics
▶ Rudd RA, Seth P, David F, Scholl L. (2016) Increase in drug and Opioid-involved
overdose deaths-United States, 2010-2015. MMWR Morbidity Wkly Rep
65:1445-52
▶ CDC. Increases in Drug and Opioid Overdose Deaths — United States, 2000–
2015. CDC (2016). https://www.cdc.gov/mmwr/volumes/65/wr/mm655051e1.htm.
▶ American Psychiatric Association. (2013) Diagnostic and Statistical Manual of
Mental Disorders, Fifth Edition. Washington, DC: American Psychiatric
Association; 541-46
▶ National report: Apparent opioid-related deaths in Canada (December 2017)
https://www.canada.ca/en/public-health/services/publications/healthy-living/
apparent-opioid-related-deaths-report-2016-2017-december.html
▶ Zoorob, R, Kowalchuk, A, Mejia de Grubb, M, (2018) Buprenorphine Therapy for
Opioid Use Disorder; American Family Physician, 97(5), p 313-320
73Selected References
▶ Dowell D, Haegerich TM, Chou R. CDC (2016), Guideline for Prescribing Opioids
for Chronic Pain - United States, MMWR Recomm Rep 2016;65(No. RR-1):1–49.
doi: http://dx.doi.org/10.15585/mmwr.rr6501e1
▶ Medication Assisted Treatment
http://www.samhsa.gov/medication-assisted-treatment
▶ National Institute on Drug Abuse (NIDA) https://www.drugabuse.gov/
▶ SchuckitMA. (2016) ,Treatment of Opioid Use Disorders. NEJM 375(4), 357
http://www.nejm.org/doi/full/10.1056/NEJMra1604339#t=article
▶ Substance Abuse and Mental Health Services Administration. (2017), Opioid Use
in the Older Population. Rockville, MD
▶ Substance Abuse and Mental Health Services Administration. (2011), Managing
Chronic Pain in Adults With or in Recovery From Substance Use Disorders.
Treatment Improvement Protocol (TIP) Series 54. HHS Publication No. (SMA)
12-4671. Rockville, MD:
▶ EmergencyDepartment Data Show Rapid Increases in Opioid Overdoses –
Wake-up call to the fast-moving opioid overdose epidemic; CDC VitalSigns 2017
74Selected References
▶Gomes T, Greaves S, Martins D, et al (2017) Latest trends in Opioid-
Related Deaths in Ontario: 1991-2015. Ontario Drug Policy Research
Network, Toronto, ON
▶British
Columbia Coroners service. (2017) Illicit Drug overdose Deaths in
BC. January 1, 2007-March 31, 2017. British Columbia Coroners Service,
Burnaby, BC
▶Wood E, MD, PhD, (2018) Strategies for Reducing Opioid-Overdose
Deaths Lessons from Canada. N Engl J Med, 378:1565-1567 doi:
10.1056/NEJMp1800216
▶Buprenorphine Information: www.buprenorphine.samhsa.gov
▶Waiver Training: http://pcssnow.org
▶Waiver information: http://bit.ly/docwaiver
▶The Pharmacology of MAT http://bit.ly/tip63mat
75You can also read