Therapierefraktäre Angina Pectoris - PD Dr. med. Florim Cuculi Co-Chefarzt Kardiologie Leiter Interventionelle Kardiologie und Akutkardiologie ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Therapierefraktäre Angina Pectoris
PD Dr. med. Florim Cuculi
Co-Chefarzt Kardiologie
Leiter Interventionelle Kardiologie und
Akutkardiologie
Herzzentrum, Luzerner Kantonsspital
Inhalt
• Diagnose der KHK
– Wann welcher Test? Sensitivität- und Spezifität der
verschiedenen diagnostischen Möglichkeiten
• Medikamentöse Therapie der Angina pectoris
Neue Möglichkeiten der Angina Therapie
• Pro- und Kontra einer frühen invasiven Abklärung
– Orbita Studie
• Fallbeispiele
Patienten mit einem akuten Myokardinfarkt profitieren eindeutig von einer invasiven Therapie
Diagnosis and management of patients with stable ischemic heart disease
Make diagnosis and
assess prognostic factors
Provide appropriate Initiate medical
follow-up care treatment
Consider
revascularization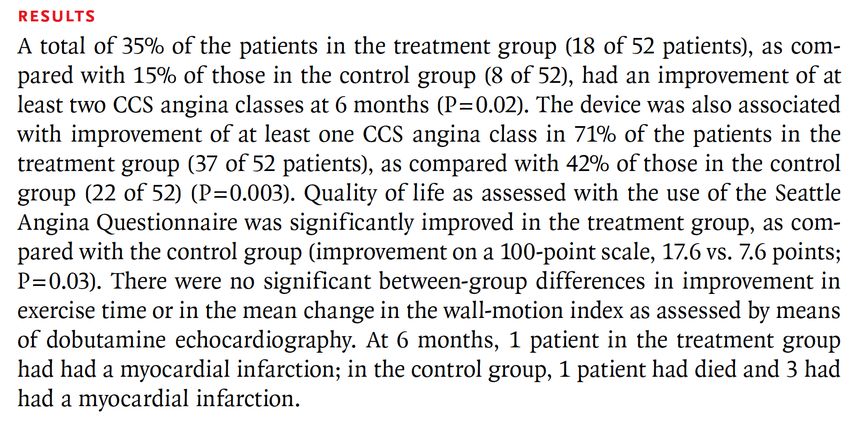
Pretest likelihood of CAD as detected by invasive angiography in symptomatic patients according to age and
sex (Combined Diamond Forrester and CASS Data).
A low pretest risk of CAD is considered < 10% (green) and a high pretest risk is considered > 90% (red). All others are at
intermediate risk (yellow).
Chest Pain Criteria:
1. Sub-sternal chest discomfort with characteristic quality and duration
2. Provoked by exertion or emotional stress
3. Relieved promptly by rest or nitroglycerin
Non-anginal Chest Pain Atypical Angina Typical Angina
1 of 3 Criteria 2 of 3 Criteria 3 of 3 Criteria
Age Male Female Male Female Male Female
30 – 39 4% 2% 34% 12% 76% 26%
40 - 49 13% 3% 51% 22% 87% 55%
50 - 59 20% 7% 65% 33% 93% 73%
60 – 69 27% 14% 72% 51% 94% 86%
Adapted from Diamond et al NEJM 1979;300:1350-58 and Weiner et al NEJM 1979;301:230-5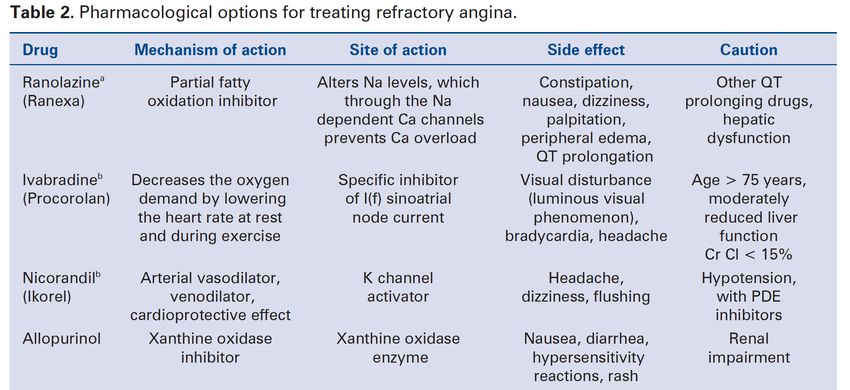
Summary Estimates of Pooled Sensitivity and Specificity (with 95% confidence
intervals) for Non-Invasive Cardiac Tests for the Diagnosis of Coronary Artery Disease
Technology Sensitivity Specificity
Exercise Treadmill 0.68 (0.23-1.0) 0.77 (0.17-1.0)
Attenuation Corrected SPECT 0.86 (0.81-0.91) 0.82 (0.75-0.89)
Gated SPECT 0.84 (0.79-0.88) 0.78 (0.71-0.85)
Traditional SPECT 0.86 (0.84-0.88) 0.71 (0.67-0.76)
Contrast Stress Echocardiography (wall motion) 0.84 (0.79-0.90) 0.80 (0.73-0.87)
Exercise or Pharmacologic Stress Echocardiography 0.79 (0.77-0.82) 0.84 (0-.82-0.86)
Cardiac Computed Tomographic Angiography 0.96 (0.94-0.98) 0.82 (0.73-0.90)
Positron Emission Tomography 0.90 (0.88-0.92) 0.88 (0.85-0.91)
Cardiac MRI (perfusion) 0.91 (0.88-0.94) 0.81 (0.75-0.87)
Adapted from Gianrossi et al Circulation 1989; 80:87-98, Medical Advisory Secretariat 2010; 10:1-40,
and McArdle et al J Am Coll Cardiol 2012;60:1828-37
Chronic Management of Anginal Symptoms
Recommendation Strength of Level of
recommendation evidence
We suggest that beta-blockers be used as first-line therapy for symptom relief, with the dose titrated Conditional Moderate
to reach a target resting heart rate of 55 to 60 bpm quality
We suggest that beta-blockers or long-acting calcium channel blockers be used for chronic stable Conditional Moderate
angina in uncomplicated patients quality
We suggest the addition of a long-acting nitrate when initial treatment with a beta-blocker and/or Conditional Moderate
long acting calcium channel blocker is not tolerated or contraindicated or does not lead to adequate quality
symptom control
We recommend avoiding non-dihydropyridine calcium channel blockers in conjunction with beta- Strong High quality
blockers if there is risk of AV block or excessive bradycardia
We suggest that chelation therapy, allopurinol, magnesium supplementation, coenzyme Q10, suxiao Conditional Moderate
jiuxin wan or shenshao tablets and testosterone should not be used to attempt to improve angina or quality
exercise tolerance
We recommend that implementation and optimization of medical therapy should be achieved within Strong High quality
12 to 16 weeks of an initial evaluation suggesting presence of SIHD without high risk features during
which adequacy of symptom control and quality of life can be assessed prior to consideration of
revascularization therapy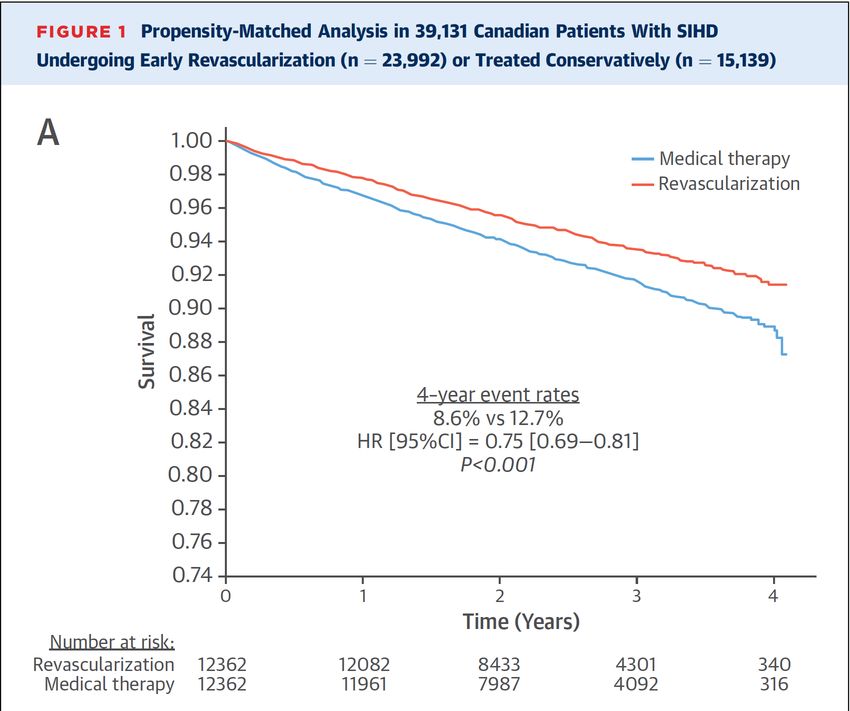
Consideration of Revascularization Therapy
Recommendation Strength of Level of
recommendation evidence
We recommend that coronary angiography be considered early in patients who are Strong High quality
identified to have high risk non-invasive test features
We recommend that patients who develop medically refractory symptoms or Strong High quality
inadequate CV quality of life on medical therapy should undergo elective coronary
angiography in anticipation of possible revascularization procedures
Medikamentöse Therapie der Angina pectoris I

Medikamentöse Therapie der Angina pectoris II
Pro- und Kontra: Revaskularisation • Der Benefit einer PTCA/Stenting bei Patienten mit stabiler KHK ist umstritten. • Gewisse Patienten-Populationen profitieren von einer invasiven Therapie.
Fundamental prognostic factors for assessing stable
ischemic heart disease.
Anatomical burden and Ischemic burden
distribution of disease of disease
LV ejection fraction and wall
motion abnormalitiesOrbita-Studie
Mein Kommentar bzgl. Orbita-Studie • Ausgebaute medikamentöse Therapie kann auch bei hochgradigen Stenosen die Patienten symptom-frei machen. • Orbita war eine kleine Studie mit kurzem Follow-up keine prognostische Aussage. • Pragmatisches Vorgehen angezeigt: nicht bei allen Stenosen einen Stent implantieren!
Hauptstamm-Stenose • 66 jährige Frau mit typischer Angina pectoris CCS III • Pathologische Ergometrie • Zugewiesen für eine Koronarangiographie
• Die Patientin wurde aus prognostischen Gründen chirurgisch revaskularisiert • Wahrscheinlich wäre eine Kontrolle der Symptome mit medikamentöser Therapie schwierig gewesen.
Subtotale Stenosen in grossen Gefässen • 60 jähriger Mann mit Angina pectoris CCS II • CCS 3 CCS 2 mit Nebilet 5 mg 1-0-0 und Nitroderm TTS 10 tagsüber • Ist sehr sportlich, Müdigkeit seit Beta-Blocker- Therapie, Ruhepuls neu 50/min. • Perkutane Behandlung mit Stents
PCI to RCA
32Rotablation
Koronarangiographie nach 18 Monaten (atypische Symptome)
35Schwere KHK • 87 jährige Dame mit typischer Angina pectoris CCS III- IV • Wohnt noch zuhause, kann Haushalt nicht mehr machen. • Hospitalisation, Ausbau medikamentöse Therapie mit Bisoprolol 7.5 mg, Amlodipin 5 mg (BD tief). • Revaskularisation RIVA, konservative Therapie für RCA und RCX aktuell CCS 1-2 und zufrieden mit medikamentöser Therapie.
37
Patient nach Bypass-Operation • 72 jähriger Mann mit Angina pectoris CCS III. • Vor 2 Jahren Diagnose schweren 3-Gefäss-KHK • Bypass-Operation, seit 3 Monaten erneut AP wie vor der OP: Venengraft auf RCA zu. • RCA in komplexer Intervention mit Stents versorgt. Patient beschwerdefrei.
Schlussbemerkungen I • Nach der Diagnose der KHK (mit oder ohne Koronarangiographie) sollte eine medikamentöse Therapie implementiert werden (Beta-Blocker +/- Amlodipin +/- Nitraten).
Schlussbemerkungen II
• Erreicht man Symptomfreiheit und hat der
Patient eine gute Leistungsfähigkeit in der
Ergometrie bzw. keine induzierbare Ischämie
kann konservativ vorgegangen werden.
• Relevante Ischämie (keine Symptomfreiheit,
induzierbare Ischämie)
Koronarangiographie +/- PTCA +/- CABG.Fragen?
You can also read