TIPS FOR PAIN MANAGEMENT IN THE ED - DR. EMILY AUSTIN UHN EMERGENCY MEDICINE CONFERENCE - MYCONFERENCE SUITE
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Tips for
Pain Management in the ED
(that don’t involve an opioid)
Dr. Emily Austin
St. Michael’s Hospital; Ontario Poison Centre
UHN Emergency Medicine Conference
November 8, 2018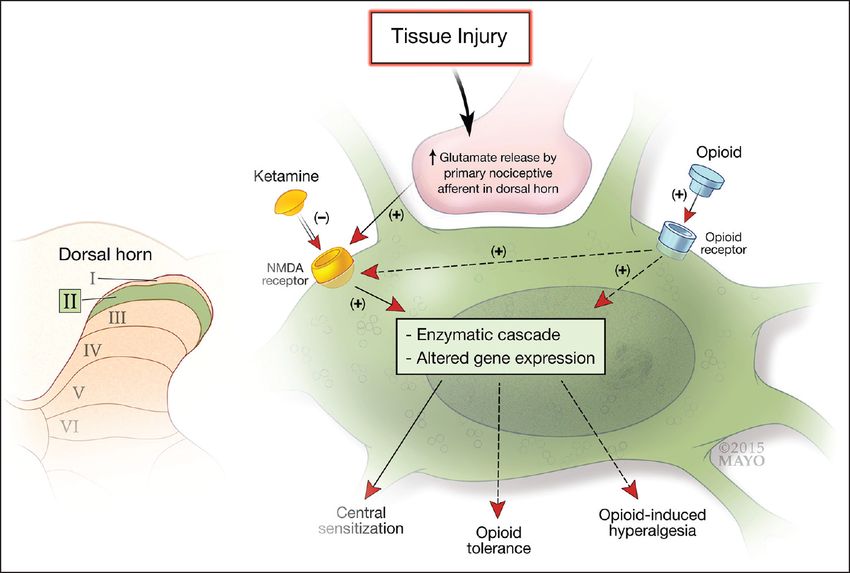
Pain is a chief complaint in > 50%
of ED presentations
(Cordell AM J EM 2002)
https://www.aliem.com/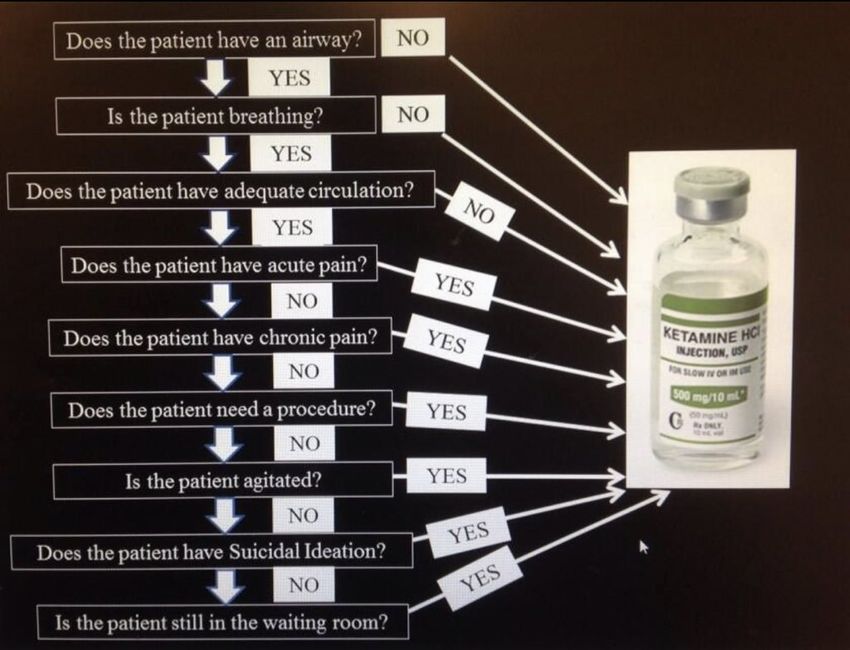
Non-pharmacologic strategies
Ann Emerg Med. 2017;70:446-448.
Patient-centered communication
Physical interventions
Ice, heat
Topical coolant sprays
Recommendations for activity, exercise
Relaxation techniques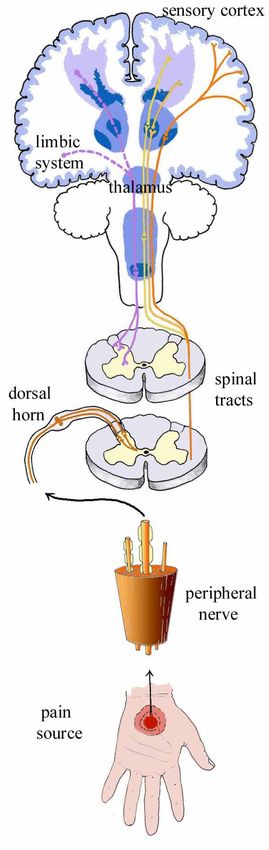
Opioids
Adverse effects
Respiratory depression
Hypotension
Bradycardia
Nausea, vomiting
Oversedation
https://www.poison.org/
Outline
4 cases of acute pain in the ED:
Sub-dissociative dose ketamine
NSAIDs
Regional nerve blocks
Haloperidol
https://smhttp-ssl-41526.nexcesscdn.net
Case 1
40 yo F
“10/10” RUQ pain x 3 hours
HR 105 BP 130/85 Afebrile
https://www.aliem.com/
Preserved airway reflexes
Hemodynamic stability
https://www.magneticmag.com
https://twitter.com/painfreeED/media

Ketamine is an NMDA
receptor antagonist
*other receptor interactions as well
https://encrypted-tbn0.gstatic.com
http://www.perioperativepain.com
http://www.joacp.org/articles/2016/32/
Analgesic: 0.1-0.3 mg/kg
Partially dissociated: 0.4 - 0.8 mg/kg
Dissociated: > 0.7 mg/kg
http://emupdates.comStudies on
sub-dissociative dose Ketamine
for ED analgesia
Motov 2018 Ahmadi 2014
Bowers 2017 Andolfatto 2013
Motov 2017 Richards 2013
Sin 2017 Ahern 2013
Beik 2016 Yeaman 2013
Motov 2015 Jennings 2012
Ahern 2015 Jennings 2011
Miller 2015 Lester 2010
Beaudoin 2014 Johansson 2009
Ahern 2014 Galinski 2007
Golster 2014 Gurnani 2006
https://twitter.com/painfreeED/
June 9, 2018Studies on
sub-dissociative dose Ketamine
for ED analgesia
Motov 2018 Ahmadi 2014
Sub-dissociative dose
Bowers 2017
Motov 2017
Andolfatto 2013
Richards 2013
ketamine is safe and
Sin 2017
Beik 2016
Ahern 2013
Yeaman 2013
effective for analgesic
Motov 2015
Ahern 2015
Jennings 2012
Jennings 2011
use in EDs.
Miller 2015
Beaudoin 2014
Lester 2010
Johansson 2009
Ahern 2014 ACEPAnnPolicyGalinski
statement 2007
EM 2018; 71: e35
Golster 2014 Gurnani 2006Ketamine Adverse Effects
Adverse effects are minor and transient when
sub-dissociative doses given
EMERGENCE REACTION
Nausea and vomiting
Dysphoria
Hallucinations
Dizziness
Headaches
Laryngospasm
Apnea
Hypersalivation
https://i2-prod.mirror.co.uk/Emergency providers should
disclose that SDK may trigger
minor and transient
adverse effects, including
nausea and temporary dysphoria.
ACEP Policy statement
Ann EM 2018; 71: e35Ketamine for analgesia
Analgesic Dose: 0.15-0.3 mg/kg
Short Infusion Continuous
IV Push Infusion
Over 10 - 15
Over 2 minutes minutes
0.15 mg/kg/hr, increase
2-5 mg PRN q30 min
Lowest rates of adverse effects
Motov AJEM 2017One absolute contraindication
*Patients with psychiatric illness are generally excluded from
studies.Geriatric population
Motov et al. Am J EM 2018.
Good analgesia, but more adverse events than morphine 0.1 mg/kg.
https://ubisafe.orgPregnant population
Excluded from ED studies.
Category C: Animal studies have shown adverse effects
https://vectortoons.com/Summary
Analgesic Dose: 0.15-0.3 mg/kg IM or IV over 10 minutes
Low-dose ketamine is safe and effective for analgesia in the ED.
Inform patient about unpleasant side effects.Case 2
55 yo M
“10/10” left flank pain x 2 hours
Remote hx of PUD
https://www.aliem.com/NSAIDs
Analgesia
Anti-Inflammatory
Anti-pyretic
http://www.previcox.com/http://www.perioperativepain.com http://www.joacp.org/
Adverse effects limit use
GI Bleed
Acute kidney injury
Platelet dysfunction
Hypersensitivity
Drug-Drug interactions
Cardiovascular eventsNSAIDs have an analgesic ceiling
There is a dose beyond which there
is no additional analgesic benefit.
* there is no anti-inflammatory ceiling dose
https://images.slideplayer.com/33/9421732/slides/slide_18.jpgNSAIDs have an analgesic ceiling
There is a dose beyond which there
is no additional analgesic benefit.
* there is no anti-inflammatory ceiling dose
https://images.slideplayer.com/33/9421732/slides/slide_18.jpgNSAIDs have an analgesic ceiling
Ibuprofen 400 mg PO
Ketorolac 10 mg IV Motov Ann Emerg Med 2017
There is no analgesic benefit to taking a higher
dose, but more risk of adverse events.
* there is no anti-inflammatory ceiling doseGeriatric Population
Caution!
GI Bleed, renal injury, MI, DDI.
Topical NSAIDs
Screen for underlying GI, renal disease, CV risk factors
Lowest dose, < 5 days.
Advise patient of warning signs
https://ubisafe.orgPregnant population
Not in T1, T3.
https://vectortoons.com/Summary
Minimize harms by dosing NSAIDS within analgesic ceiling:
Ibuprofen 400 mg PO TID
Ketorolac 10 mg IVCase 3
32 yo F
“10/10” pounding right-sided headache 10 mg IV
No relief despite acetaminophen, maxeran and ketorolac
https://www.aliem.com/Regional nerve blocks
Directed analgesia
Less systemic side effects
Decreased length of stay
Decreased morbidity (delirium)Sphenopalatine ganglion block
for headaches
Cotton-tipped applicator + Lidocaine or bupivicaine + 15 minutes
https://www.aliem.com/Sphenopalatine ganglion block
for headaches
Cotton-tipped applicator + Lidocaine or bupivicaine + 15 minutes
https://www.aliem.com/Sphenopalatine ganglion block
for headaches
Non-invasive, well tolerated
Geriatric
Pregnancy
Not first line
https://www.aliem.com/Summary Sphenopalatine ganglion block can be a useful adjunct for migraine pain management.
Case 4
44 yo M, T1 DM
“10/10” diffuse abdominal pain, multiple episodes vomiting
Many previous admissions for similar presentation
https://www.aliem.com/Haloperidol
Antipsychotic
Dopamine inhibition in brain & chemoreceptor trigger zone
(?other complicated mechanisms)Haloperidol 5 mg IM or IV
Ramirez AJEM 2017
Lower rates of hospital admission
Lower opioid dosingHaloperidol 5 mg IM or IV
Migraine Gaffigan JEM 2015
Gastroparesis Ramirez AJEM 2017, Roldan AEM 2017
Cannabinoid hyperemesis syndrome Hickey AJEM 2013
Opioid tolerant patients Richards JEM 2011, StrayerSummary
Haloperidol 5 mg IV or IM for analgesia in select
clinical settings.Take-Home Points
Sub-dissociative dose Ketamine for analgesia
0.15-0.3 mg/kg IM or IV over 10 minutes
Minimize harms by dosing within analgesic ceiling:
Ibuprofen 400 mg PO TID
Ketorolac 10 mg IV
Sphenopalatine ganglion block can be a useful adjunct for migraine pain
management.
Haloperidol 5 mg IV or IM for analgesia in select clinical settings.Acknowledgments
Anne Sylvestre
Dr. Reuben StrayerYou can also read