Transient Global Amnesia - Diffusion-Weighted Imaging Lesions and Cerebrovascular Disease
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Transient Global Amnesia
Diffusion-Weighted Imaging Lesions and Cerebrovascular Disease
Christian Enzinger, MD; Felix Thimary, MD; Peter Kapeller, MD; Stefan Ropele, PhD;
Reinhold Schmidt, MD; Franz Ebner, MD; Franz Fazekas, MD
Background and Purpose—A hypoxic-ischemic origin of transient global amnesia (TGA) has been suggested on the basis
of the observation of infarctlike diffusion-weighted imaging (DWI) abnormalities in some affected individuals. We
tested this hypothesis by comparing vascular risk factors, magnetic resonance imaging (MRI) markers of cerebral
small-vessel disease, and other evidence of a cerebrovascular disorder between TGA patients with (DWI⫹) and without
(DWI⫺) DWI lesions and normal community-based controls.
Methods—We retrospectively identified 86 patients hospitalized for TGA (mean⫾SD age, 65.9⫾10.9 years; 62% female).
Brain MRI at 1.5 T was assessed for DWI lesions exhibiting restricted diffusion (ie, DWI⫹), white-matter
hyperintensities, lacunes, and chronic infarcts (median time lag to clinical onset, 66.6⫾54.6 hours). Vascular risk factors
and findings from duplex sonography, ECG, and echocardiography were recorded. A 1:2 age- and sex-matched sample
of 172 elderly subjects (mean⫾SD age, 65.6⫾9.3 years; 62% female) free of neuropsychiatric disease served for
comparison.
Results—DWI lesions were observed in 10 patients with TGA (11.5%; mean⫾SD age, 68.3⫾5.4 years; 8 women). They
were all small and located in the mesiotemporal region (9 left hemisphere, 5 right hemisphere). The vascular risk profile
of TGA patients and concomitant changes on brain MRI were comparable with those of healthy controls and did not
show significant differences between DWI⫹ and DWI⫺ subjects. A comprehensive diagnostic workup also provided
no evidence for a higher rate of cerebrovascular disorder–related abnormalities in either the total group of TGA patients
or TGA DWI⫹ patients.
Conclusions—These findings do not support a cerebrovascular etiology of TGA, even in those individuals showing acute
DWI lesions. Other pathophysiologic mechanisms need to be explored. (Stroke. 2008;39:2219-2225.)
Key Words: transient global amnesia 䡲 amnestic syndrome 䡲 magnetic resonance imaging 䡲 diffusion-weighted
imaging 䡲 risk factors
T ransient global amnesia (TGA) is characterized by an-
terograde memory disturbance of sudden onset that lasts
for 1 to 24 hours.1 Orientation in space and time is impaired
jugular vein incompetency, have been implicated in the
pathophysiology of TGA. (For reviews, see Sander and
Sander,3, Pantoni et al,4 and Quinette et al.5) However, almost
while consciousness remains undisturbed. From a defined 5 decades after Fisher and Adams coined this term,6 consen-
population, the minimum annual incidence of TGA has been sus on its etiology and pathogenesis is still lacking. Concep-
estimated to be 3.4 per 100 000 in 1 study.1 TGA is tually, cerebral ischemia, epileptic discharge, and migraine
commonly considered a benign syndrome because complete constitute the main pathogenic hypotheses.
restitution occurs in most cases after a few hours, although a Diffusion-weighted imaging (DWI) has become a powerful
remaining amnesic gap may persist.2 tool in the evaluation of patients with suspected stroke owing
A variety of mechanisms and eliciting events such as to its high sensitivity and specificity, even for small areas of
paradoxical embolism, vertebral angiography, physical exer- acute ischemia, and thereby DWI often provides important
cise, sexual intercourse, emotional stress, arterial thrombo- etiologic hints.7,8 Consequently, this method has also been
embolism, hyperextension of the neck, psychologic distur- applied to TGA to gain further insights into the pathophysi-
bances, migraine, cerebral small-vessel disease, venous ology of this enigmatic condition.9 Indeed, some authors
ischemia due to Valsalva-like maneuvers and, more recently, observed DWI lesions in the mesiotemporal region that were
Continuing medical education (CME) credit is available for this article. Go to http://cme.ahajournals.org to take the quiz.
Received October 29, 2007; final revision received December 14, 2007; accepted January 8, 2008.
From the Department of Neurology (C.E., S.R., R.S., F.F.) and the Section of Neuroradiology (C.E., F.T., F.E.), Department of Radiology, Medical
University of Graz, Graz; and the Department of Neurology (P.K.), Villach, Austria.
The first 2 authors contributed equally to this work.
Correspondence to Christian Enzinger, MD, Department of Neurology and Section of Neuroradiology, Medical University of Graz, Auenbruggerplatz
22, A-8036 Graz, Austria. E-mail chris.enzinger@meduni-graz.at
© 2008 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.107.508655
2219
Downloaded from http://stroke.ahajournals.org/ by guest on October 30, 20152220 Stroke August 2008
Table 1. Clinical, Demographic, and Paraclinical Data of TGA Patients Compared With Age- and Sex-Matched Controls, Stratified by
the Finding of a DWIⴙ Lesion in Patients
TGA Patients Healthy Controls DWI⫹ TGA Patients DWI⫺ TGA Patients
(n⫽86) (n⫽172) P Value (n⫽10) (n⫽76) P Value
Age, y 65.9⫾10.9 (25.6–84.8) 65.6⫾9.3 (41–83) 0.77 68.3⫾5.4 (62.0–77.3) 65.3⫾11.4 (25.6–84.8) 0.24
Female sex, n (%) 53 (61.6) 107 (62.2) 1.00 8 (80.0) 45 (59.2) 0.30
Arterial hypertension, n (%) 51 (59.3) 101 (58.7) 0.80 6 (60.0) 45 (59.2) 0.49
Diabetes, n (%) 6 (7.0) 17 (9.9) 0.49 0 (0) 6 (7.8) 0.46
Systolic BP, mm Hg 142.4⫾16.7 (110–177) 142.3⫾22.7 (87–212) 0.98 138.2⫾14.7 (112–170) 140.4⫾16.7 (110–177) 0.97
Diastolic BP, mm Hg 80.9⫾8.8 (63–98) 84.4⫾10.0 (52–110) 0.03 81.2⫾7.9 (68–98) 80.9⫾8.3 (63–98) 0.70
Cholesterol, mg/dL 212.1⫾46.9 (86–360) 237.0⫾52.0 (136–523) 0.001 222.1⫾46.9 (86–267) 234.4⫾68.2 (127–360) 0.66
HDL, mg/dL 59.1⫾13.5 (30–92) 56.18⫾16.2 (28–136) 0.16 58.6⫾15.7 (40–86) 59.1⫾13.3 (30–92) 0.92
LDL, mg/dL 127.6⫾42.9 (48–278) 150.7⫾35.2 (68–244) 0.001 134.1⫾28.0 (86–164) 126.8⫾44.5 (48–278) 0.63
Triglycerides, mg/dL 136.5⫾61.0 (50–345) 149.1⫾140.0 (41–1285) 0.44 120.4⫾49.2 (50–202) 138.5⫾62.3 (57–345) 0.40
Fibrinogen, mg/dL 307.6⫾70.8 (198–550) 316.9⫾82.1 (33–661) 0.37 333.5⫾53.8 (247–399) 304.0⫾72.4 (198–550) 0.22
Atrial fibrillation, n (%) 2 (2.3) 11 (6.4) 0.23 0 (0) 2 (2.6) 0.78
ICA stenosis, n (%)
Normal (0%) 25 (29.1) 27 (15.7) 3 (30) 22 (28.9)
Mild (1–29%) 54 (62.8) 144 (83.7) 7 (70) 47 (61.8)
Moderate (30–69%) 6 (7.0) 1 (0.6) 䡠䡠䡠 6 (7.9)
Severe (70–99%) 1 (1.2) 䡠䡠䡠 䡠䡠䡠 1 (1.3)
Occluded (100%) 䡠䡠䡠 䡠䡠䡠 0.001§ 䡠䡠䡠 䡠䡠䡠 0.79§
Cardiac abnormalities, * † ‡
n (%)
TTE normal 31 (70.5) 142 (82.6) 4 (66.7%) 27 (71.1)
Valve insufficiency I 11 (25.0) 24 (14.0) 2 (33.3%) 9 (23.7)
Valve insufficiency II 䡠䡠䡠 5 (2.9) 䡠䡠䡠 䡠䡠䡠
Valve insufficiency III 1 (2.3) 䡠䡠䡠 䡠䡠䡠 1 (2.6)
Valve stenosis 1 (2.3) 1 (0.6%) 0.05§ 䡠䡠䡠 1 (2.6) 0.73§
BP indicates blood pressure; ICA, extracranial section of the internal carotid artery; TTE, transthoracic echocardiography; and valve insufficiency, aortic, mitral,
and/or tricuspidal valve insufficiency (degrees I–III). Data on cardiac abnormalities are from subcohorts of 44 (*), 6 (†), and 38 (‡) subjects. Values are given as
mean⫾SD (range) or as denoted.
§P value assessed by the Kruskal-Wallis H test.
mostly punctuate and showed signal characteristics consistent TGA by first assessing the frequency of acute DWI⫹
with focal cerebral ischemia.10 –19 This created new arguments ischemic lesions in patients with TGA and then comparing
for a vascular etiology of TGA. However, a recent careful the vascular risk factor profile and other evidence for a
serial magnetic resonance imaging (MRI) study with a cerebrovascular disorder between TGA patients with and
dedicated imaging protocol demonstrated that the temporal without DWI lesions, also in relation to a cohort of sex- and
dynamics of DWI lesion evolution are distinct from “classic” age-matched population-based normal controls.
acute focal cerebral ischemia, and those authors proposed
delayed ischemia as a possible underlying mechanism.10 Subjects and Methods
Although clinical follow-up has not shown an increased risk Patients
for stroke in the overall group of individuals with TGA,1,20,21 We retrospectively identified patients hospitalized for an acute
it could be speculated that cerebrovascular disease (CVD) episode of TGA at the Department of Neurology, Medical University
might exist at least in those who show acute DWI lesions in Graz, within the time period January 2002 to December 2006, in
the context of this disorder.5 This would have important whom an MRI of the brain including DWI was available. This
implications regarding diagnostic workup and preventive yielded a cohort of 86 patients with a mean⫾SD age of 66⫾10 years
(53 females, 44 males; Table 1). According to existing criteria,1 a
therapeutic measures. At present, however, other evidence for diagnosis of TGA was reserved for witnessed attacks of definite
a cerebrovascular disorder has not yet been fully analyzed in amnesia without disturbance of consciousness, focal neurologic
DWI⫹ patients, and conclusions are also limited by a report symptoms, or epileptic features in patients who did not have active
of this finding from mostly smaller series of patients,12,14 – epilepsy, who had not sustained a recent head injury, and that
16,22–24 except for a few larger studies with up to 41
resolved within 24 hours.
Apart from a careful neurologic examination and medical history,
patients.10,11,13 patients underwent repeated blood pressure measurements (n⫽86),
We therefore wished to further test the “vascular hypoth- ECGs (n⫽86), transthoracic echocardiography (n⫽44), duplex
esis” in a large, unselected cohort of patients hospitalized for sonography of the extracranial cerebral arteries (n⫽86), electroen-
Downloaded from http://stroke.ahajournals.org/ by guest on October 30, 2015Enzinger et al DWI Lesions in TGA and CVD 2221
cephalography (EEG; n⫽83), chest x-ray (n⫽86), and a routine blinded experts (E.C., S.R.) as described previously27 as absent
laboratory workup including measurements of cholesterol, triglycer- (grade 0), punctate (grade 1), early confluent (grade 2), and confluent
ides, and fibrinogen (n⫽86). EEG findings were mostly normal (grade 3).
(n⫽57, 66.3%) or nonspecific (n⫽11, 12.8%). Regional slowing of
electrical activity was observed in 13 patients (15.1%). Only 2 Plotting of DWI Lesions
subjects in the TGA group demonstrated EEG signs compatible with To visualize both the topographic distribution and overlap of DWI⫹
epileptogenic foci (2.3%), and these individuals were DWI⫺. This lesions in the TGA cohort, all DWI⫹ lesions were plotted into
distribution of EEG findings (normal, nonspecific regional slowing standard space (MNI 152 averaged standard brain). First, DWI
of electrical activity, and epileptic foci) did not differ significantly lesions were outlined manually in a magnified view of the diffusion-
between DWI⫹ and DWI⫺ TGA patients (P⫽0.065). Vascular risk weighted images, and corresponding lesion masks were produced.
factors were defined as reported previously.25,26 Four patients had a These masks then were transferred into standard space by using the
history of migraine (4.6%), and 3 patients (3.4%) reported that they transformation matrix that was defined by prior registration of the
had experienced symptoms suggestive of a TGA previously (without individual diffusion-weighted scans to standard space. Registration
confirmation by medical doctors). was done with an affine 12-parameter model with a correlation
ratio– based cost function and trilinear interpolation (FLIRT, part of
Healthy Controls the FMRIB software library FSL; available at www.fsl.ox.ac.uk). A
A sample of 172 elderly subjects (mean⫾SD age, 66⫾9 years; 107 probabilistic map for lesion occupancy was produced by calculating
women and 65 men) was randomly drawn in consecutive order with the relative frequency from all registered masks.
the investigator unaware of clinical and (if present) MRI findings
from the register of the Austrian Stroke Prevention Study (ASPS) to Statistical Analyses
obtain a 1:2 age- and sex-matched control group for comparison of The Statistical Package for the Social Sciences (PC⫹, version 14.01;
clinical, demographic, and paraclinical variables and risk factors SPSS Inc, Chicago, Ill) was used for data analysis. Categorical
(Table 1). MRI of the brain was performed in subcohorts of the variables were tested by Pearson’s 2 test or by 2⫻2 Fisher’s exact
ASPS and was available for 92 individuals with a mean age of 67⫾9 test in case of contingency tables containing ⬍5 cases. Fulfilment of
years. The ASPS is a single-center, prospective, follow-up study on or deviation from normal distribution of continuous variables was
the cerebral effects of vascular and genetic risk factors in the normal tested by Kolmogorov-Smirnov statistics with a significance level
elderly population of Graz, Austria. Within the ASPS, individuals after Lilliefors and additional inspection of histograms. Normally
are excluded if they have a history of neuropsychiatric disease, distributed continuous variables were compared with Student t test or
including previous cerebrovascular attacks and dementia, or an 1-way ANOVA. The Mann–Whitney U test and the Kruskal-Wallis
abnormal neurologic examination determined on the basis of a test were used as analog nonparametric tests. Spearman’s rank
structured clinical interview and a physical and neurologic exami- correlation coefficients were calculated. The level of significance
nation. The design of the study, selection and sampling procedures was set at 0.05 in all cases. Data are quoted as mean⫾SD unless
for ASPS participants, and a detailed description of the assessment of otherwise stated.
risk factors within the setting of the ASPS have been given
elsewhere.25,26 Results
Magnetic Resonance Imaging MRI Findings
MRI of the brain was performed with 1.5-T scanners (Siemens In the TGA cohort, 14 punctate lesions with restricted
Symphony, Siemens Erlangen, Germany; Philips Gyroscan NT and diffusivity (DWI⫹) were observed in 10 subjects (11.5%;
Gyroscan ACS, Philips, Eindhoven, the Netherlands). Patients un- mean⫾SD age, 68.3⫾5.4 years; 8 women; Figure 2). As
derwent scanning according to a standard protocol used for the shown in the lesion plot in Figure 3, DWI⫹ lesions were seen
workup of patients with suspected stroke at our clinic. This included
an axial T2-weighted spin-echo sequence (repetition time/echo time exclusively in the mesiotemporal region, with a peak of lesion
[TR/TE]⫽2700 ms/120 ms), an axial fluid-attenuated inversion probability in the hippocampus (alveus, body, and head).
recovery sequence (TR/TE/inversion time⫽6000 ms/130 ms/1900 Other anatomic areas affected were the collateral eminence,
ms), a sagittal T1-weighted spin-echo sequence (TR/TE⫽612 ms/13 the gyrus dentatus and cornu ammonis, and the parahip-
ms), and a diffusion-weighted, single-shot echo-planar imaging pocampal gyrus (T3; anatomic designations according to the
sequence (TR/TE⫽4600 ms/80 ms, isotropic diffusion weighting, b
value⫽0 and 1000 s/mm 2 , field of view⫽250 mm, ma- Duvernoy atlas).28 Nine lesions were located in the left
trix⫽128⫻128, 2 averages) with 20 axial slices (thickness⫽5.0 mm, hemisphere, and 5 lesions lay in the right hemisphere. Four
slice gap⫽1 mm). Apparent diffusion coefficient (ADC) maps were subjects demonstrated 2 lesions, which were bilateral in 2 of
calculated from the reference scan (b⫽0) and the diffusion-weighted them. The size of lesions ranged between 3 and 6 mm. The
scan. The time lag between clinical onset of TGA and imaging was interval between symptom onset and MRI was not signifi-
0 to 24 hours in 10 patients (11.6%), ⬎24 but ⬍48 hours in 20
patients (23.3%), ⬎48 but ⬍115 hours in 36 patients (41.9%), and cantly different between DWI⫹ and DWI⫺ subjects
ⱖ115 hours in 20 patients (23.3%). The MRI protocol for the control (63.3⫾30.1 hours [median, 65.6 hours; range, 22.8 to 116.3
subjects included a dual-echo spin-echo sequence (TR/TE⫽2000 to hours] vs 88.0⫾57.2 hours [median, 70.2 hours; range, 3.6 to
2500 ms/30 and 90 ms) in axial orientation and a sagittal T1- 289.7 hours]; P⫽0.23). The proportion of subjects with a
weighted spin-echo sequence (TR/TE⫽600 ms/30 ms). The ASPS DWI⫹ lesion was not significantly different between TGA
MRI protocol did not include DWI.
patients scanned ⬎48 hours after symptom onset (n⫽4/30,
Rating of Scans 13.3%) and subjects scanned ⱕ48 hours (n⫽6/56, 10.7%;
All scans were rated by consensus by 2 blinded experts (T.F., K.P.) P⫽0.7). The duration of the TGA episode also did not differ
for the presence of lesions with focal restriction of diffusivity significantly between the DWI⫹ and the DWI⫺ patient
(DWI⫹) of ⬎3-mm diameter (which had to be confirmed by a groups (DWI⫹, 4.8⫾3.3 hours vs DWI⫺, 6.2⫾5.7 hours;
concomitant ADC reduction; Figure 1) and for clinically silent P⫽0.54).
ischemic infarcts and lacunes (defined as focal lesions involving the
basal ganglia, the internal capsule, the thalamus, or the brain stem Markers of cerebral small-vessel disease such as early
and not exceeding a maximum diameter of 10 mm). According to our confluent or confluent WMHs were seen in one third of TGA
scheme, white-matter hyperintensities (WMHs) were rated by 2 subjects (Table 2). Thirteen TGA patients (15.1%) showed
Downloaded from http://stroke.ahajournals.org/ by guest on October 30, 20152222 Stroke August 2008
Figure 1. Typical DWI⫹ lesion in a TGA patient.
Representative axial slices from a 66-year-old
male TGA patient (time interval between clinical
onset and imaging was 20 hours). Note that axial
T2- (A) and fluid-attenuated inversion recovery
sequence–weighted (B) images are inconspicuous,
but a punctuate lesion (C) confirmed by a concom-
itant ADC reduction (D) is clearly shown in the left
hippocampus on DWI sequences (images are
shown in radiologic convention).
cerebral lacunes. Clinically silent territorial infarcts were grades of carotid artery stenosis (⬎30%) were in the DWI⫺
observed in 2 DWI⫺ patients, 1 in the area of the posterior group. Cardiac abnormalities as evidenced by echocardiog-
cerebral artery and 1 in the cerebellum. Regarding the raphy were also infrequent in TGA patients and, if present,
distribution and frequency of WMHs, lacunes, and clinically mild. Cases with more severe changes of the heart valves (an
silent infarcts, no significant differences were found between 83-year-old woman with mitral insufficiency III and 1 56-
DWI⫹ and DWI⫺ TGA subjects or between the entire TGA year-old man with a mitral stenosis of 1 cm2 orifice area) or
group and matched controls (n⫽92). a patent foramen ovale (n⫽4) were found in the DWI⫺ group.
As shown in Table 1, the distribution and frequency of
Cerebrovascular Risk Factors and Other Evidence cerebrovascular risk factors within the entire cohort of TGA
for a CVD patients were not significantly different from an age- and
The cerebrovascular risk factor profiles between DWI⫹TGA sex-matched population-based sample of normal elderly in-
subjects and DWI⫺ subjects did not show significant differ- dividuals. With regard to some factors like diastolic blood
ences. As shown in Table 1, TGA patients with DWI pressure, serum cholesterol, and HDL levels, the TGA cohort
abnormalities had a similar frequency of arterial hypertension even demonstrated a more favorable risk profile. Further-
and demonstrated similar mean values for systolic and dia- more, the proportion of subject with no or only minor cardiac
stolic blood pressures and for total cholesterol, HDL, LDL, abnormalities was similar between TGA patients (95.5%) and
and triglyceride levels than those without DWI lesions, and normal individuals (96.6%). Carotid artery abnormalities
there were also no differences in comparison to the control were more frequent in TGA patients compared with normal
population. None of the 6 subjects with diabetes mellitus and individuals, but this difference was driven by the 6 TGA
none of the 2 subjects with atrial fibrillation was in the DWI⫹ subjects with moderate stenosis.
group. In the entire TGA cohort, the degree of atherosclerosis
of the extracranial cerebral vessels assessed by sonography in Discussion
general was low (92% of subjects either showed a normal Our analyses of a series of 86 patients with TGA at our
finding or had only a mild stenosis). All 7 patients with higher institution confirmed the presence of small, focal, hyperin-
Downloaded from http://stroke.ahajournals.org/ by guest on October 30, 2015Enzinger et al DWI Lesions in TGA and CVD 2223
Figure 2. DWI⫹ TGA patients. Selected slices from the 10 TGA subjects, demonstrating lesions with focal restriction of diffusivity
(arrows and insets). Nine lesions were located in the left hemisphere, and 5 lesions lay in the right hemisphere (only 3 are shown). Four
subjects demonstrated 2 lesions, which were bilateral in 2 of them. Lesion size ranged between 3 and 6 mm. Images are shown in
radiologic convention.
tense lesions on DWI in some of the affected individuals. To earlier reports,1,20 there also was no difference in vascular risk
the best of our knowledge, this study represents the largest factors compared with an age- and sex-matched group of
single-center MRI-based investigation on a consecutive series normal elderly controls drawn from the ASPS.
of TGA patients who underwent DWI.10 –16,22–24 The signal The presence of infarctlike abnormalities on DWI in some
abnormalities observed were associated with reduced diffu- patients with TGA10 –19 has revived the discussion regarding a
sivity, as indicated by the ADC maps, a finding that otherwise cerebrovascular etiology for such abnormalities in at least
is regarded as rather specific for acute ischemic infarction.7,8 some individuals. Along these lines, a higher prevalence of
When looking at evidence for a coexisting cerebrovascular atherosclerosis, as indicated by a higher intima-media thick-
disorder, however, we found no difference between TGA ness and substantial vascular risk factors in DWI⫹ patients,
patients with and without DWI lesions. In confirmation of has been reported.12 This would imply the need for an
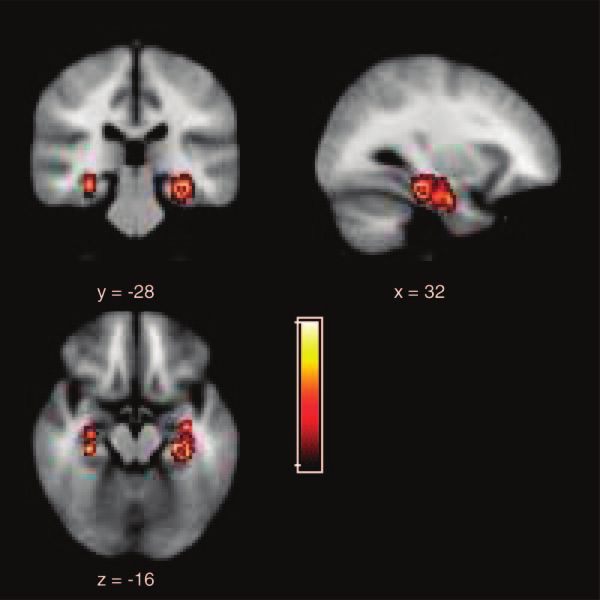
Figure 3. Probabilistic lesion distribution map of
the cohort of DWI⫹ TGA patients. DWI lesions
were located exclusively in mesiotemporal brain
structures relevant for memory (brighter values on
the hot metal scale indicate greater lesion proba-
bility; coordinates refer to MNI standard space).
Note the preponderance of lesions in the dominant
(left) hemisphere (right-hand image in the upper
panel).
Downloaded from http://stroke.ahajournals.org/ by guest on October 30, 20152224 Stroke August 2008
Table 2. MRI Findings of TGA Patients Compared With Age- and Sex-Matched Controls, Stratified by the Finding of a DWIⴙ Lesion
in Patients
TGA Patients Healthy Controls DWI⫹ TGA Patients DWI⫺ TGA Patients
(n⫽86) (n⫽92) P Value (n⫽10) (n⫽76) P Value
WMHs
Score 0 (absent), n (%) 19 (22.1) 31 (33.7) 1 (10.0) 18 (23.7)
Score 1 (punctuate), n (%) 38 (44.2) 26 (28.3) 6 (60.0) 32 (42.1)
Score 2 (early confluent), n (%) 18 (20.9) 22 (12.8) 2 (20.0) 16 (21.1)
Score 3 (confluent), n (%) 11 (12.8) 13 (14.1) 0.13 1 (10.0) 10 (13.2) 0.69
Lacunes, n (%) 13 (15.1) 12 (13.0) 0.83 2 (20.0) 11 (14.5) 0.64
Clinically silent infarcts, n (%) 2 (2.3) 2 (2.2) 0.80 䡠䡠䡠 2 (2–6%) 0.60
extensive vascular workup and long-term therapeutic strate- sole explanation for the low rate of DWI⫹ lesions in the
gies as indicated for the secondary prevention of stroke. present study.
Whereas avoidance of and correction for vascular risk factors Although our results strongly argue against an association
are certainly appropriate in any individual, our data do not between CVD and TGA, the true etiology of DWI⫹ lesions
suggest a specific preponderance of cerebrovascular disor- in the context of TGA still remains speculative. Interestingly
ders, neither in the entire group of TGA patients nor in those and in line with previous studies (for a review, see Sander and
with a DWI lesion, when compared with community-based Sander3), mapping of lesions consistently pointed to the
controls. There was no evidence for an increased rate or involvement of the same brain regions relevant to memory
intensity of cerebrovascular risk factors, and there was no function, with a predominance for the left hemisphere.
indirect evidence for an increased rate of microangiopathy, as Because the hippocampal artery supplies an internal anasto-
indicated by higher grades of WMHs and lacunes. Early mosis between an upper and a lower artery, some have
confluent and confluent WMHs have been associated with suggested this to be a particularly hypoxia-susceptible water-
microangiopathy,29 and their prevalence was similar in TGA shed area (the so-called sector of Sommer).30 The similarity
subgroups as well as in comparison with ASPS participants. between DWI abnormalities in TGA and areas of acute
Other diagnostic workup procedures, including ECG, ex- ischemia is intriguing, but the consistency of lesion size and
tracranial duplex sonography, and echocardiography, also did the absence of other DWI lesions argue against ischemic
not provide more direct evidence for a cerebrovascular infarction per se. In this context, it is particularly interesting
etiology. that the few existing longitudinal studies also did not docu-
This retrospective analysis showed acute DWI lesions in
ment persistent abnormal signal changes in the hippocampus
only 11% of individuals with TGA. This is relatively low
after TGA, which would have been compatible with postis-
compared with some previous reports.10 –13 In a review of
chemic structural damage.11,14 Indeed, in addition to cerebral
existing MRI studies on acute TGA, 52 of the published 99
ischemia, ADC reductions have also been observed after
patients had DWI abnormalities, corresponding to a rate of
cortical spreading depression, ischemic depolarizations, sta-
DWI positivity of 52%.3 In a careful serial study, a frequency
tus epilepticus, and hypoglycemia.31–35 A DWI lesion thus
of DWI lesions of even 84% was observed.10 This suggests
has to be considered a nonspecific finding with several
that higher rates of lesion detection might be achieved with
possible underlying mechanisms, probably all leading to focal
repeated scanning at later time intervals, dedicated protocols,
or higher field strengths. As a consequence, it could be argued energy failure. Recently, a combined study with single-
that in our study, some individuals might have been falsely photon emission computed tomography and transcranial mag-
labeled as DWI⫺, and this might have obscured the compar- netic stimulation suggested a relation between hypoperfusion
ison between TGA subgroups. Although this cannot be ruled in several brain areas (in the thalami, and also in the temporal
out, our main conclusions are supported by the fact that even lobes in a subset of patients) and reduced activity in inhibi-
those patients who were definitely DWI⫹ did not show any tory circuits.36 Conceptually, studies in TGA patients would
difference in regard to cerebrovascular risk factors or MRI thus appear to benefit from a combination of DWI with
findings suggestive of small-vessel disease when compared perfusion-weighted MRI, but to date, this approach has been
with population-based controls. It has also been speculated used only in a case study, which yielded negative results.37
that the incongruence between imaging findings could be Unfortunately, both the design of our study and the small
explained by the delayed detectability of DWI lesions in TGA numbers of migraneurs and subjects with pathologic EEG
compared with stroke.10 In this context, it is interesting that in findings prohibit us from drawing further conclusions on
our study, DWI⫺ and DWI⫹ TGA patients did not show some of these alternative hypotheses. Clearly, pathophysio-
significant differences in the interval between the onset of logic mechanisms other than focal ischemia from CVD need
TGA and MRI scanning, and there were also no significant to be explored further as causes of a temporal dysfunction in
differences in the rate of lesion detection between subjects memory-relevant structures, as indicated by more recent
scanned within or beyond 48 hours in this study. Differences reports on hemodynamic disturbances in venous flow patterns
in the timing of scanning therefore cannot be regarded as the in TGA.38 – 40
Downloaded from http://stroke.ahajournals.org/ by guest on October 30, 2015Enzinger et al DWI Lesions in TGA and CVD 2225
Acknowledgment 20. Zorzon M, Antonutti L, Mase G, Biasutti E, Vitrani B, Cazzato G.
Transient global amnesia and transient ischemic attack: natural history,
We thank Erich Flooh, PhD, for help with database management.
vascular risk factors, and associated conditions. Stroke. 1995;26:
1536 –1542.
Disclosures 21. Pantoni L, Bertini E, Lamassa M, Pracucci G, Inzitari D. Clinical
None. features, risk factors, and prognosis in transient global amnesia: a
follow-up study. Eur J Neurol. 2005;12:350 –356.
References 22. Huber R, Aschoff AJ, Ludolph AC, Riepe MW. Transient global amnesia.
J Neurol. 2002;249:15–20.
1. Hodges JR, Warlow CP. The aetiology of transient global amnesia: a
23. Greer DM, Schaefer PW, Schwamm LH. Unilateral temporal lobe stroke
case-control study of 114 cases with prospective follow-up. Brain.
1990;113 (pt 3):639 – 657. causing ischemic transient global amnesia: role for diffusion-weighted
2. Hodges JR, Oxbury SM. Persistent memory impairment following imaging in the initial evaluation. J Neuroimaging. 2001;11:317–319.
transient global amnesia. J Clin Exp Neuropsychol. 1990;12:904 –920. 24. Gass A, Gaa J, Hirsch J, Schwartz A, Hennerici MG. Lack of evidence of
3. Sander K, Sander D. New insights into transient global amnesia: recent acute ischemic tissue change in transient global amnesia on single-shot
imaging and clinical findings. Lancet Neurol. 2005;4:437– 444. echo-planar diffusion-weighted MRI. Stroke. 1999;30:2070 –2072.
4. Pantoni L, Lamassa M, Inzitari D. Transient global amnesia: a review 25. Schmidt R, Fazekas F, Kapeller P, Schmidt H, Hartung HP. MRI white
emphasizing pathogenic aspects. Acta Neurol Scand. 2000;102:275–283. matter hyperintensities: three-year follow-up of the Austrian Stroke Pre-
5. Quinette P, Guillery-Girard B, Dayan J, de la Sayette V, Marquis S, vention Study. Neurology. 1999;53:132–139.
Viader F, Desgranges B, Eustache F. What does transient global amnesia 26. Enzinger C, Fazekas F, Matthews PM, Ropele S, Schmidt H, Smith S,
really mean? review of the literature and thorough study of 142 cases. Schmidt R. Risk factors for progression of brain atrophy in aging:
Brain. 2006;129:1640 –1658. six-year follow-up of normal subjects. Neurology. 2005;64:1704 –1711.
6. Fisher CM, Adams R. Transient global amnesia. Trans Am Neurol Assoc. 27. Schmidt R, Enzinger C, Ropele S, Schmidt H, Fazekas F, the Austrian
1958;83:143–146. Stroke Prevention Study. Progression of cerebral white matter lesions:
7. Gass A, Ay H, Szabo K, Koroshetz WJ. Diffusion-weighted MRI for the 6-year results of the Austrian Stroke Prevention Study. Lancet. 2003;14:
‘small stuff’: the details of acute cerebral ischaemia. Lancet Neurol. 2046 –2048.
2004;3:39 – 45. 28. Duvernoy H. The Human Brain: Surface, Three-Dimensional Sectional
8. Fisher M, Albers GW. Applications of diffusion-perfusion magnetic res- Anatomy With MRI, and Blood Supply. Vienna/New York: Springer-
onance imaging in acute ischemic stroke. Neurology. 1999;52: Verlag; 1999.
1750 –1756. 29. Fazekas F, Kleinert R, Offenbacher H, Schmidt R, Kleinert G, Payer F,
9. Tong DC, Grossman M. What causes transient global amnesia?: new Radner H, Lechner H. Pathologic correlates of incidental MRI white
insights from DWI. Neurology. 2004;62:2154 –2155. matter signal hyperintensities. Neurology. 1993;43:1683–1689.
10. Sedlaczek O, Hirsch JG, Grips E, Peters CNA, Gass A, Wohrle J, 30. Erdem A, Yasargil G, Roth P. Microsurgical anatomy of the hippocampal
Hennerici M. Detection of delayed focal MR changes in the lateral arteries. J Neurosurg. 1993;79:256 –265.
hippocampus in transient global amnesia. Neurology. 2004;62: 31. Sotak CH. Nuclear magnetic resonance (NMR) measurement of the
2165–2170. apparent diffusion coefficient (ADC) of tissue water and its relationship
11. Bartsch T, Alfke K, Stingele R, Rohr A, Freitag-Wolf S, Jansen O, to cell volume changes in pathological states. Neurochem Int. 2004;45:
Deuschl G. Selective affection of hippocampal CA-1 neurons in patients 569 –582.
with transient global amnesia without long-term sequelae. Brain. 2006; 32. Smith JM, Bradley DP, James MF, Huang CLH. Physiological studies of
129:2874 –2884. cortical spreading depression. Biol Rev. 2006;81:457– 481.
12. Winbeck K, Etgen T, von Einsiedel HG, Rottinger M, Sander D. DWI in 33. Miyasaka N, Nagaoka T, Kuroiwa T, Akimoto H, Haku T, Kubota T, Aso
transient global amnesia and TIA: proposal for an ischaemic origin of T. Histopathologic correlates of temporal diffusion changes in a rat model
TGA. J Neurol Neurosurg Psychiatry. 2005;76:438 – 441. of cerebral hypoxia/ischemia. AJNR Am J Neuroradiol. 2000;21:60 – 66.
13. Lee HY, Kim JH, Weon YC, Lee JS, Kim SY, Youn SW, Kim SH. 34. Hasegawa Y, Formato JE, Latour LL, Gutierrez JA, Liu K-F, Garcia JH,
Diffusion-weighted imaging in transient global amnesia exposes the CA1 Sotak CH, Fisher M, Brayden JE. Severe transient hypoglycemia causes
region of the hippocampus. Neuroradiology. 2007;49:481– 487. reversible change in the apparent diffusion coefficient of water. Stroke.
14. Cianfoni A, Tartaglione T, Gaudino S, Pilato F, Saturno E, Tonali PA, Di 1996;27:1648 –1656.
Lazzaro V. Hippocampal magnetic resonance imaging abnormalities in 35. Szabo K, Poepel A, Pohlmann-Eden B, Hirsch J, Back T, Sedlaczek O,
transient global amnesia. Arch Neurol. 2005;62:1468 –1469. Hennerici M, Gass A. Diffusion-weighted and perfusion MRI demon-
15. Felix MM, Castro LH, Maia AC Jr, da Rocha AJ. Evidence of acute strates parenchymal changes in complex partial status epilepticus. Brain.
ischemic tissue change in transient global amnesia in magnetic resonance 2005;128:1369 –1376.
imaging: case report and literature review. J Neuroimaging. 2005;15: 36. Nardone R, Buffone EC, Matullo MF, Tezzon F. Motor cortex excit-
203–205. ability in transient global amnesia. J Neurol. 2004;251:42– 46.
16. Ay H, Furie KL, Yamada K, Koroshetz WJ. Diffusion-weighted MRI 37. Budson AE, Schlaug G, Briemberg HR, Furie KL, Ay H. Perfusion- and
characterizes the ischemic lesion in transient global amnesia. Neurology. diffusion-weighted magnetic resonance imaging in transient global
1998;51:901–903. amnesia. Neurology. 1999;53:239.
17. Matsui M, Imamura T, Sakamoto S, Ishii K, Kazui H, Mori E. Transient 38. Chung CP, Hsu HY, Chao AC, Chang FC, Sheng WY, Hu HH. Detection
global amnesia: increased signal intensity in the right hippocampus on of intracranial venous reflux in patients of transient global amnesia.
diffusion-weighted magnetic resonance imaging. Neuroradiology. 2002; Neurology. 2006;66:1873–1877.
44:235–238. 39. Sander D, Winbeck K, Etgen T, Knapp R, Klingelhofer J, Conrad B.
18. Jeong Y, Kim GM, Min Song Y, Na DL. A tiny hippocampal ischemic Disturbance of venous flow patterns in patients with transient global
lesion associated with transient global amnesia. Cerebrovasc Dis. 2003; amnesia. Lancet. 2000;356:1982–1984.
16:439 – 442. 40. Schreiber SJ, Doepp F, Klingebiel R, Valdueza JM. Internal jugular vein
19. Di Filippo M, Calabresi P. Ischemic bilateral hippocampal dysfunction valve incompetence and intracranial venous anatomy in transient global
during transient global amnesia. Neurology. 2007;69:493. amnesia. J Neurol Neurosurg Psychiatry. 2005;76:509 –513.
Downloaded from http://stroke.ahajournals.org/ by guest on October 30, 2015Transient Global Amnesia: Diffusion-Weighted Imaging Lesions and Cerebrovascular
Disease
Christian Enzinger, Felix Thimary, Peter Kapeller, Stefan Ropele, Reinhold Schmidt, Franz
Ebner and Franz Fazekas
Stroke. 2008;39:2219-2225; originally published online June 26, 2008;
doi: 10.1161/STROKEAHA.107.508655
Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 2008 American Heart Association, Inc. All rights reserved.
Print ISSN: 0039-2499. Online ISSN: 1524-4628
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://stroke.ahajournals.org/content/39/8/2219
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.
Once the online version of the published article for which permission is being requested is located, click
Request Permissions in the middle column of the Web page under Services. Further information about this
process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Stroke is online at:
http://stroke.ahajournals.org//subscriptions/
Downloaded from http://stroke.ahajournals.org/ by guest on October 30, 2015You can also read