Transpositions des gros vaisseaux - Le point du vue du cardiopédiatre Dr Daniela Laux, UE3C - Arcothova
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Transpositions des gros vaisseaux
Le point du vue du cardiopédiatre
Dr Daniela Laux, UE3C
M3C-HML-Centre des Malformations Congénitales Cardiaques complexes
Cardiopathies congénitales humaines Fréquence Incidence Communication interventriculaire (CIV) 30% 1500 Communication interauriculaire (CIA) 8% 400 Sténose pulmonaire (SP) 7% 350 Persistance du canal artériel (PCA) 7% 350 Coarctation de l’aorte (CoA) 6% 300 Tétralogie de Fallot (T4F) 6% 300 Transposition des gros vaisseaux (TGV) 5% 250 Sténose aortique (SA) 5% 250 Canal atrioventriculaire (CAV) 4% 200 Atrésie pulmonaire à septum intact (APSI) 2% 100 Atrésie pulmonaire à septum ouvert (APSO) 2% 100 Atrésie tricuspide (AT) 2% 100 Tronc artériel commun (TAC) 2% 100 Retour veineux pulmonaire anormal (RVPA) 2% 100 Malpositions vasculaires (MV) 1% 50 Syndrome d'hypoplasie du cœur gauche (SHCG) 1% 50 Interruption de l’arc aortique (IAA) 1% 50 Ventricule unique (VU) 1% 50 Anomalie d’Ebstein 1% 50 Discordances AV et VA 1% 50 Autres 6% 300

Transposition des gros vaisseaux Définition: • AP au dessus du ventricule G • Aorte au dessus du ventricule D = discordance ventriculo-artérielle • La TGV n’est qu’une des malpositions vasculaires qui incluent: TGV, VDDI, VGDI, malposition anatomiquement corrigée.
VX NORMOPOSES VX TRANSPOSES
D-TGV
S = solitus Ao
AP
D L
L-TGV
A = antéropostérieur
I = inversus
Courtesy L.Houyel
Rappel embryologique
Nouveau concept de morphogenèse :
second champ cardiaque
Premier champ cardiaque (cardiac crescent) = 1st lineage
Second champ cardiaque (anterior heart field) = 2nd lineage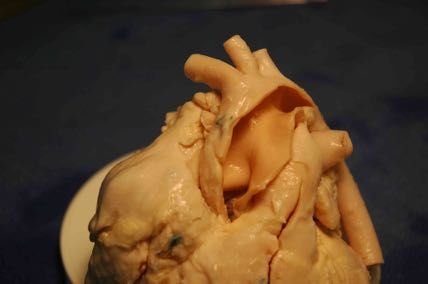
Cœur normal
Ao
AP
Rotation
CT « normale »
O
VD Ao AP
VG
Rotation
« inversée »
TGV
Early looping Convergence Rotation Courtesy L.Houyel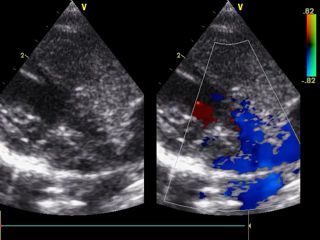
Types anatomiques: simples et complexes • TGV « simple » – 60%: pas d’autre lésion associée • TGV avec communication interventriculaire (CIV) • TGV avec CIV et coarctation • TGV avec CIV et sténose pulmonaire • L-TGV (très rare) • Anomalies des valves AV: – Fente mitrale et straddling mitral – Straddling tricuspide
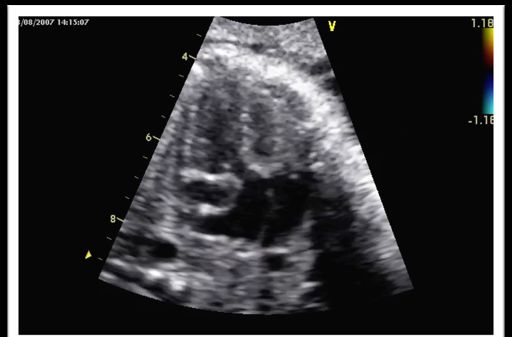
Diagnostic prénatal
Table 3 - Prenatal diagnosis, pregnancy termination, perinatal and early neonatal mortality for selected (isolated) congenital heart anomalies -
Paris Registry of Congenital Malformations, 1983-2000
Etude EPICARD
i) Transposition of Great Arteries
1983 - 1988 1989 - 1994 1995 - 2000
N % 95 % CI* N % 95 % CI* N % 95 % CI* pV
Prenatal Diagnosis 16 12.5 1.6 - 38.3 27 48.1 28.7 - 68.1 40 72.5 56.1 - 85.4 0.001
Pregnancy Termination 17 0 0 - 19.5 27 7.4 0.9 - 24.3 40 0 0 - 8.8 0.62
First Week Mortality 16 18.8 4.0 - 45.6 24 8.3 1.0 - 27.0 39 2.6 0.1 - 13.5 0.04
Perinatal Mortality 17 23.5 6.8 - 49.9 25 12.0 2.5 - 31.2 40 5.0 0.6 - 16.9 0.02
Khoshnood B et al 2012
ii) Hypoplastic Left Heart Syndrome
1983 - 1988 1989 - 1994 1995 - 2000
N % 95 % CI* N % 95 % CI* N % 95 % CI* pV
Prenatal Diagnosis 22 31.8 13.9 - 54.9 29 82.8 64.2 - 94.2 27 88.9 70.8 - 97.6 < 0.001
Pregnancy Termination 22 13.6 2.9 - 34.9 29 72.4 52.8 - 87.3 27 63.0 42.4 - 80.6 < 0.001
First Week Mortality 18 83.3 58.6 - 96.4 8 75.0 34.9 - 96.8 10 50.0 18.7 - 81.3 0.12
Perinatal Mortality 19 84.2 60.4 - 96.6 8 75.0 34.9 - 96.8 10 50.0 18.7 - 81.3 0.10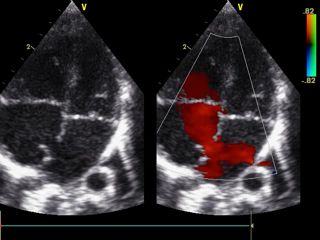
Evolution du diagnostic prénatal et IMG
P+PC = naissances enregistrées à Paris de femmes domiciliées à Paris ou dans la Petite Couronne
P = naissances enregistrées et domiciliées à Paris
Transposition des gros vaisseaux (isolée)
Diagnostic prénatal et interruption médicale de grossesse
1981-84 1985-87 1988-90 1991-93 1994-96 1997-99 2000-02 2003-05 2006-08 2009-11 2012-14
%DPN 3.8 30.0 29.2 61.3 68.1 75.0 76.5 86.5 92.2 82.5 90.3
% IMG 0.0 4.8 4.2 19.4 10.6 15.0 3.9 1.9 3.1 11.1 4.8
Naissances enregistrées à Paris de femmes domiciliées à Paris ou dans la Petite CouronneDiagnostic prénatal ailleurs qu’en France
Escobar-Diaz et al. Ultrasoud Obst Gyn 2015Impact postnatal du diagnostic prénatal (?)
• Mortalité périopératoire: études contradictoires
– Amélioration globale des résultats concomitante
de l’augmentation du DAN partout dans le monde
Bonnet et al. 1999, Khosnood at al. 2017
• Morbidité périopératoire:
– Amélioration des délais opératoires, ventilation
mécanique, acidose Chakraborty et al. 2018, Cloete et al. 2019
• Devenir neurodeveloppemental:
– Association positive DAN démontrée dans la TGV
Calderon 2012It is recommended that a detailed foetal anomaly I C echo
scan be performed by a foetal medicine specialist beca
Because the risk for foetal karyotype abnormality is IIb C are
low in cases of TGA IVS, karyotyping may be
PEC pratique en France
vent
considered on an individual basis where appropriate
After foetal diagnosis, follow-up to term is I C
orga
recommended for early detection of the T
6 development of high-risk features, which may Cardiology in norm
the
require immediate intervention following delivery be o
a
Class of recommendation. to3.3
Recommendation
b
Level of evidence. Classa Levelb and
• DAN TGV -> CPDPN Recommendations for prenatal detection
It is recommended that the obstetric anomaly scan I C
elec
an
typi
3.2 Perinatal management—timing, place and mode of
be performed at 18-22 weeks of gestation sym
righ
• Confirmation par un cardiopédiatre expert To increase prenatal detection, it is recommended
delivery
that outflow tract views, in addition to four-chamber
I C alm
the
duA
Studies
views, be comparing the outcome
included in obstetric of babies with TGA
anomaly scans
• Accompagnement du couple: Itdiagnosed
is recommended
suggest
by a foetalthat
prenatally
that thewith
the rates
cardiology
thosebediagnosed
diagnosis
of preoperative
specialist
confirmed IpostnatallyC
and postoperative
and that parental
sig
pay
is
arte
counselling [9,
mortality should20,also
38,be39]
provided
and by a foetal [19, 40–43]
morbidity asy
feat
information sur la pathologie/PEC/pronostic cardiology
are specialist and other related
lower for babies diagnosed prenatally.
professionals (foetal medicine specialists,
health po
and
3.2.1
obstetricians,Sitepaediatric
and timingcardiacofsurgeons
delivery.and Because babies diam
• Soutien psychologique with TGA
neonatologists)
Itgenerally
is recommended
require
recommended
early treatment
thatfoetal
that a detailed delivery
anomaly
after birth, it is
takesI place Cat or
con
have
ech
com
near
scan be aperformed
tertiary-care
by a foetal paediatric
medicine specialistcardiology and be
coro
Because
paediatricthe risk for foetal
cardiac karyotype
surgery [44, is45].IIbAdhering
abnormality
centre C are
surg
low in cases of TGA IVS, karyotyping may
to this practice enables the neonate to be in optimal be ven
It
• Accouchement déclenché en milieu spécialisé considered on an individual basis where appropriate
condition
After and avoids
foetal diagnosis, follow-upneonatal
to term isretrieval I transport-
C
org
accu
related
recommended for early detection costs
complications and of the [46]. Although the excl
• Cardiopédiatre sur place en SDN delivery
development
majority
must
of women
require immediate
be scheduled
of high-risk features, before
can have
intervention
which may
a vaginal
following
the due date, the
delivery, which
delivery
Innoa
be
is generally recommended [47]. However, a planned to
• Evaluation postnatale hémodynamique immédiateLevel of evidence.
a
Class of recommendation. Reco
caesarean delivery may be indicated if high-risk
b an
maternal or
Recommendations foetal features
for prenatal are identified.
detection ele
Neon
• Décision si Rashkind ou non 3.2 Perinatal management—timing, place and mode of
typ
cru
rig
Echo
delivery
Recommendation Classa Levelb for
the
allo
Studies comparing
It is recommended the outcome
that delivery ofatbabies
takes place or I withCTGA arte
diagnosed prenatally
near a tertiary-care withcardiology
paediatric those diagnosed
and postnatally pa
rele
• Transfert en cardio/SI/ néona suggest
paediatric
mortality
that thesurgery
cardiac
[9, 20,
Vaginal delivery
rates ofcentre
at term
38,is 39]
preoperative and postoperative
recommended in most I[19, 40–43]
and morbidity C
art
Perfo
und
fea
cases, whereas caesarean delivery is recommended
arewhen
lower for babies
high-risk featuresdiagnosed
are identifiedprenatally. an
BAS:
a
a
3.2.1 Site and timing of delivery. Because babies b
dia
Clas
Class of
with recommendation.
TGA require early treatment after birth, it is Leve
b c ha
Level of evidence. Refe
generally recommended that delivery takes place at or
Recommendations for perinatal management com
Reco
near a tertiary-care paediatric cardiology and cor
paediatric cardiac surgery centre [44, 45]. Adhering sur
to this practice enables the neonate to be in optimal
, 1454 31 2 9475 Sarris
7 3 5 /C et0 9D al. City
1 2017
1 C2:53 5 1
4 9 condition
7 . and avoids neonatal retrieval transport- acc
related complications and costs [46]. Although the excfindings on fetal echocardiogram have facilitated more com- of risk assessment that include stratification of patients and spe-
prehensive planning to prevent the intrapartum hemodynamic cific postnatal care recommendations have been reported.571,572 In
AHA Scientific Statement
compromise that may occur with specific high-risk CHD. practice, anticipated postnatal level of care should be assigned by
Disease-specific delivery room care recommendations for the fetal diagnostic team, with concomitant delivery room and
newborns with CHD have been created for neonatologists and neonatal care recommendations made before delivery. Table 19
are well accepted in clinical practice.569,570 For many newborns summarizes risk-stratified level of care assignment and coordi-
with CHD, no specialized care is needed in the delivery room, nating action plans based on reported algorithms.
Diagnosis and Treatment of Fetal Cardiac Disease
and infants can be discharged from the nursery to be seen for
follow-up as outpatients. For all others, delivery care planning Disease-Specific Recommendations for
must define the specialized treatment and follow-up required, Transitional Care
A Scientific Statement From theTransitional
American
Past studies have shown that Heart
Circulation
Association
the fetal diagnosis
the possible need for transport to a specialized cardiac cen-
ter, the likelihood of neonatal catheter intervention or surgery,
of CHD pre-
or the need for intervention in the delivery room in the small vents the postnatal hemodynamic instability that occurs during
Downloaded from http://circ.ahajournals.org/ by guest on October 1, 2017
Endorsed by the American Society of Echocardiography and Pediatric and Congenital Electrophysiology Society
Table 19. Level of Care Assignment and Coordinating Action Plan
The American Institute
LOC
P
ofDefinition
Ultrasound
CHD in which palliative care is
in Example
Medicine CHD
CHD with severe/fatal chromosome
supports the value and
Delivery Recommendations
Arrange for family support/palliative
findings of the statement.*
DR Recommendations
planned abnormality or multisystem disease care services
The Society of Maternal Fetal Medicine supports the Normal statement’s
delivery at local hospital review of the subject matter and
1 CHDbelieve
without predicted it is consistent
risk of VSD, AVSD, mild TOFwith its existing clinical
Arrange cardiology consultation or guidelines.†
Routine DR care
hemodynamic instability in the outpatient evaluation Neonatal evaluation
DR or first days of life Normal delivery at local hospital
Mary T. 2Donofrio,
CHD with minimal riskMD,of
hemodynamic instability in
Chair; Anita
Ductal-dependent lesions,J. Moon-Grady,
including
HLHS, critical coarctation, severe
Consider planned induction
near term
MD;usually Lisa K.in Hornberger,
Neonatalogist DR
Routine DR care, initiate PGE if
MD;
Joshua A. Copel, DRcatheterization/surgery
MD; Mark
but requiring postnatal S. Sklansky,
AS, IAA, PA/IVS, severeMD;TOF Alfred Abuhamad,
Delivery at hospital with neonatologist
and accessible cardiology
MD;
indicated Bettina F. Cuneo, MD;
Transport for catheterization/
James C. Huhta, MD; Richard A. Jonas, MD; Anita consultationKrishnan, MD; surgery Stephanie Lacey, DO;
Wesley
3 Lee,
CHD with MD; Erik
likely hemodynamic
instability in DR requiring
d-TGA C. Michelfelder,
with concerning atrial septum
primum (note: it is reasonable to
PlannedSr, MD;
induction GwenNeonatologist
at 38–39 wk;
consider C/S if necessary to
R. Rempel, RN;
and cardiac specialist
in DR, including all necessary
Norman H. Silverman, MD,
immediate
stabilization
specialtyDSc,
care for FAHA; Thomas
consider all d-TGA
an ASD at risk)
fetuses without L. coordinate
Spray, servicesMD, FAHA;
Delivery at hospital that can execute
equipmentJanette F. Strasburger, MD;
Plan for intervention as indicated by
Wayne Tworetzky, MD; Jack Rychik MD;
Uncontrolled on behalf rapid
arrhythmias
CHB with heart failure
of care, the American
including necessary
stabilizing/lifesaving procedures
Heart Association Adults With
diagnosis
Plan for urgent transport if indicated
Congenital Heart 4Disease Joint Committee
CHD with expected hemodynamic
of the Council
HLHS/severely RFO or IAS
on Cardiovascular
C/S in cardiac facility with necessary
Disease in the Young and
Specialized cardiac care team in DR
Council on Clinical instability
Cardiology,
with placental
separation requiring immediate
Council on Cardiovascular
d-TGA/severely RFO or IAS and
abnormal DA
Surgery and
specialists in the DR usually at
38–39 wk
Anesthesia, and Council on
Plan for intervention as indicated
by diagnosis; may include
catheterization/surgery in DR to
improve chance of survival
Cardiovascular
Obstructed TAPVR
Ebstein anomaly with hydrops
and Stroke Nursing catheterization, surgery, or ECMO
TOF with APV and severe airway
obstruction
Uncontrolled arrhythmias with hydrops
Background—The goal of this statement is to review available literature and to put forth a scientific statement on the current CHB with low ventricular rate, EFE,
and/or hydrops
practice of fetal cardiac medicine, including the diagnosis and management of fetal cardiovascular disease.
5 CHD in which cardiac HLHS/IAS, CHD including List after 35 wk of gestation Specialized cardiac care team in DR
Methods and Results—A writing
transplantationgroup
is planned appointed by the
severe Ebstein American
anomaly, CHD, C/SHeart
when heartAssociation
is available reviewed the available literature pertaining
to topics relevant to fetal cardiac medicine,orventricular including the diagnosis of congenital heart disease and arrhythmias,
cardiomyopathy with severe
dysfunction
assessment
AHA 2014 Donofrio et al.
APV indicates absent pulmonary valve; AS, aortic stenosis; ASD, atrial septal defect; AVSD, atrioventricular septal defect; CHB, complete heart block; CHD, congenitalClinique postnatal
Cyanose réfractaire en salle de naissance
sans détresse respiratoire
= TGV jusqu’à la preuve du contrairePathophysiologie TGV simple
• Cardiopathie cyanogène car
aorte nait du VD !
• Circulation en parallèle
• CA et FOP obligatoire pour un
mixing efficace
VG
VD
• CA shunte Ao-AP à cause des
résistances vasculaires
OG
• FOP shunte G-D à cause des
OD
compliances ventriculaireLe FOP restrictif avant Rashkind
• FOP restrictif ou fermé=
Œdème pulmonaire
• Majoration de la
cyanose
• Majoration de l’acidose
VG
VD
• Mixing inefficace
OD
OG jusqu’au décèsPrise en charge médicale néonatale • Rashkind – Mixing – Déprécharge le VG • PGE1 – Effets secondaires: apnée, douleur, fièvre – Précharge le VG • Surveillance glycémies • Surveillance alimentation entérale: risque d’entéropathie/entérocolite • Risque théorique d’AVC en cas de KTC: VD-aorte- cerveau
and mitral valve anomalies. In particular, the delaying intervention for TGA IVS results in decon- life [93].
babies diameters of the main pulmonary artery and the aorta ditioning of the left ventricle, rendering the patient a In Europe,
h, it is haveClinical
to be measured; the location of
guidelines for the managementthe valve of patients
potentially with for a primary ASO.
poor candidate have undergon
ce at or commissures and also the origin and course of the Centres have reported early repair [86], primary of life [90]. It
y and transposition
coronary arteries must beofdescribed
the great arteries
carefully before withrepair
intact
as lateventricular
as age 3 months,septum
late single-stage repair few hours of
dhering surgery. with postoperative mechanical circulatory support [94, 95]. This
optimal ItThe
has been
Taskshown that echocardiography
Force on Transposition facilitates
of the Great Arteries
and two-stage of the
repair European
(i.e. pulmonary artery banding controversial.
nsport- accurate evaluation of
Association theCardio-Thoracic
for coronary artery pattern and
Surgery with or without
(EACTS) and aortopulmonary
the Association shunt placement Also, the u
ugh the exclusion of other relevant malformations [49, 50]. followed by an ASO in 7–14 days) [86, 87] with TGA IVS ca
ate, the for European Paediatric and Congenital
In addition, echocardiography facilitates imaging for Cardiology (AEPC)
acceptable results. undertake a p
, which age, whereas
planned Authors/Task Force Members: George E. Sarris* (Chairperson) (Greece), Christian Balmer (Switzerland), Pipina 1 month of ag
gh-risk Recommendation a
LevelbdaRef
ClassEduardo
Bonou (Greece), Juan V. Comas (Spain),
c
Cruz (USA), Luca Di Chiara (Italy), Roberto M. Di Donato groups have el
Recommendation Classa Levelb presenters (u
(United Arab Emirates), José Fragata (Portugal), Tuula Eero Jokinen (Finland), George Kirvassilis (USA), Irene
Neonatal pulse oximetry screening is I C 51 postoperative
Lytrivi (USA), Milan Milojevic (Netherlands), Gurleen Sharland (UK), Matthias
Immediately Siepe
after (Germany),
birth, IV infusionJoerg
of PGEI Stein
is I C
crucial for timely diagnosis of TGA
(Austria), Emanuela Valsangiacomo
Echocardiography is the modality of choice I
Büchel (Switzerland)
B 49, 50
and Pascal R. Vouhé
recommended (France)
to maintain ductal patency until 96–99], and
a
Levelb for diagnosing TGA postnatally and
the comprehensive series of postnatal postoperative
EACTS
allows Clinical
accurate Guidelines
evaluation Committee Members: Miguel Sousa-Uva
of the coronary (Chairperson)is(Portugal),
echocardiograms complete andUmberto
all sites of few outliers un
Benedetto (UK), Giuseppe Cardillo (Italy), Manuel Castella (Spain),intercirculatory
Martin Czerny mixing have been
(Germany), evaluated
Joel Dunning
C artery pattern and exclusion of other Avoidance of elective intubation of infants on PGE1 I C
age have bee
(UK),
relevant Mark Hazekamp
malformations in most(Netherlands),
cases Stuart Head (Netherlands), Neil J. Howell (UK), Matthias Thielmann infants older t
(Germany) andshould
TómasbeGudbjartsson (Iceland) during transport is recommended. The decision to
Performance of BAS considered, IIa B 52–54 intubate prior to transport must be individualized mass/end-dias
C under echocardiographic guidance An individualized management strategy for low I C orient toward
Keywords: Transposition of the great arteries (TGA); Arterial switch operation (ASO); Jatene operation
birth weight and premature infants is
BAS: balloon atrial septostomy; TGA: transposition of the great arteries. recommended, taking into account patient and
a
Class of recommendation. institutional factors. Management options include
b
Level of evidence. primary repair as late as 3 months of age, late
c Recommendatio
Table of Contents
References single-stage repair with postoperative VAD or
Recommendations for postnatal diagnosis ECLS support and two-stage repair It is recommende
ABBREVIATIONS AND ACRONYMS………………………3 A primary ASO may be considered the preferred IIb C in neonates with
1 PREAMBLE 3 management strategy for low-birth-weight and performed from
2 BACKGROUND 5 premature infants and can be performed with 3 weeks of life
3 DIAGNOSIS 5 acceptable but increased early and mid-term risk
C2:53 5 1 2 9475 5 5 C 5 1D19 12 5 1 31 2 9475 7 3 5 5 A primary ASO s
3.1 Prenatal diagnosis 5
3.1.1 Prenatal detection 5 up until 60 days
ASO: arterial switch operation; ECLS: extracorporeal life support; IV:
3.1.2 Counselling following prenatal detection 5 intravenous; PGE1: prostaglandin E1; VAD: ventricular assist device. ASO: arterial switc
3.1.3 Further prenatal management 5 a
Class of recommendation. intact ventricular s
3.2 Perinatal management—timing, place and mode of delivery 6 b a
3.2.1 Site and timing of delivery 6 Level of evidence. Class of recommen
b
3.3 Postnatal diagnosis 6 Recommendations for perinatal management in a neonatal intensive care unit Level of evidence.
c
References.
Sarris et al. City 2017
3.3.1 Postnatal detection 6
3.3.2 Further diagnostic steps 6 Recommendations
4 PERINATAL MANAGEMENT 7 5. Surgery for Transposition of The Great
4.1 Monitoring and immediate care 7 Arteries With Intact Ventricular SeptumManœuvre de Rashkind (1966)
Manœuvre de Rashkind : sous scopie ou écho
Rashkind: effet hémodynamique immédiat
Ballon gonflé dans l’OG
Procédure réalisée dans 70% à la naissance ou dans les premiers joursPreoperative Brain Injury in Transposition of the Great Arteries Is
Associated With Oxygenation and Time to Surgery, Not Balloon
Atrial Septostomy
Christopher J. Petit, MD, Jonathan J. Rome, N=MD, 26Gil
NN avec switch
Wernovsky, MD,dont 14 avec
Stefanie Rashkind;
E. Mason,
BS, David M. Shera, ScD, Susan C. Nicolson, MD, Lisa M. Montenegro, MD, Sarah Tabbutt,
Petit et al. Petit
MD,etPhD,
al. Circ 2009 A. Zimmerman, MD,
Robert
10/26 J.avaient
and Daniel
Page 11 une leucomalacie préopératoires
Licht, MD
Petit et al. Page 12
Division of Cardiology, Department of Pediatrics (C.J.P., J.J.R., G.W., S.T.); Division of Critical Care
Medicine, Department of Anesthesia and Critical Care Medicine (G.W., S.T.); Division of Neurology,
Department of Pediatrics (S.E.M., D.J.L.); Division of Biostatistics and Epidemiology (D.M.S.);
NIH-PA Author Manuscript
Division of Cardiothoracic Anesthesia, Department of Anesthesia and Critical Care Medicine
(S.C.N., L.M.M.); and Department of Radiology (R.A.Z.), The Children’s Hospital of Philadelphia
and the University of Pennsylvania School of Medicine, Philadelphia, Pa
Abstract
Background—Preoperative brain injury is an increasingly recognized phenomenon in neonates
with complex congenital heart disease. Recently, reports have been published that associate
preoperative brain injury in neonates with transposition of the great arteries with the performance of
balloon atrial septostomy (BAS), a procedure that improves systemic oxygenation preoperatively. It
is unclear whether BAS is the cause of brain injury or is a confounder, because neonates who require
NIH-PA Author Manuscript
BAS are typically more hypoxemic. We sought to determine the relationship between preoperative
brain injury in neonates with transposition of the great arteries and the performance of BAS. We
hypothesized that brain injury results from hypoxic injury, not from the BAS itself.
Methods and Results—Infants with transposition of the great arteries (n=26) were retrospectively
included from a larger cohort of infants with congenital heart disease who underwent preoperative
brain MRI as part of 2 separate prospective studies. Data collected included all preoperative pulse
Figure 3.
A daily mean P 2 was calculated for the PVL and no-PVL groups. Repeated-measures ANOVA
O
oximetry recordings, all values from preoperative arterial blood
demonstrated gas measurements,
a significant and the
difference in mean daily P 2 between
O
BAS
PVL group (dashed line)
and the no-PVL group (solid line; P=0.02). The PVL group never achieved a mean daily P 2
O
procedure data. MRI scans were performed on the day >40ofmm surgery,
Hg. before the surgical repair. Of the
26 neonates, 14 underwent BAS. No stroke was seen in the entire cohort, whereas 10 (38%) of 26Check liste écho pré op • CIA large ou restrictive et CA ouvert ou fermé • Equilibre des ventricules – Petit VD : risque de coarctation – Petit VG : vérifier la voie pulmonaire • Anatomie de la valve mitrale – Fente non commissurale • Cardiopathies associées (CIV, caorctation aortique) • Valve pulmonaire (futur aortique) • Discongruence aortopulmonaire ? • Malalignement commissural ? • Anatomie des artères coronaires ?
La question du VG depréparé
• < 3 semaines: switch artériel
• > 3 semaines: évaluation forme du VG,
présence CA/CIA/CIV, calcul de masse VG
• Deux stratégies
– Switch avec ECMO postopératoire
– Préparation du VG: cerclage + Blalock 7-10
jours puis switch
• Masse VG minimale : > 35 g/m2 calculée en F. Lacour-Gayet et al. / European Journal of Cardio-thoracic Surgery 20 (2001) 824–829
TM Table 1 cular septum with a ‘banana’ LV shape at 2D
LV Mass (ASE) ¼ 1.04 * (LVED d 1 LVPW d 1 IVS d) 3 2 LVED d 3a
graphy.
Indexed LV Mass (G/m 2 ¼ [0.8 * (LV Mass) to 0.6] / BSA Two patients had some degree of LVOT ob
systolic gradient less than 20 mmHg. All p
a
LVED d, left ventricle end diastolic diameter; LVPW d, left ventricle ASD that was judged 2001
small in 5 patients. Eig
posterior wall thickness; IVS d, left ventricle interventricular thickness; Lacour-Gayet
a previous Rashkind septostomy. One patien
ASE, American Society of Echography. Sarrris et al. City 2017
ductus arteriosus.Vaisseaux parallèles: grand axe
TGV en souscostal: vaisseaux parallèles
Ao
Ao
AP
AP
AP
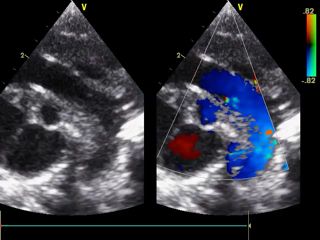
AoCIA post-RSK
Canal artériel
Congruence aortopulmonaire
Position en D-TGV: aorte ant/AP post
Ao
APAlignement commissural
AO
Ao
Ao AP
AP
APCoronaires Type A: CG
Coronaires Type A: CD
TGV avec CIV d’outlet
Classification de Yacoub
Type A Type B Type C Type D
PA PA
PA
R PA C
A C R A R A
R A
A A A C A
Type E
PA PA
C
A A
C
R A R AAnatomie coronaire • « normale » : 60% • boucle antérieure et/ou postérieure : 35% • entre gros vaisseaux (intramurale) : 5%
Les lésions coronaires après switch artériel
Comment les détecter?
ECG et échographie (IM!!!)
Coroscanner si signe d’ischémie
Coronarographie si doute
Test d’ischémie (scintigraphie)
Coroscanner systématique à 5 ans
Que faire ?
Rappeler votre chirurgien…Devenir
Mortalité postopératoire
• TGV simple: 1-5% FdR de décès:
Anatomie coronaire
• TGV + CIV: 3-6% complexe
• TGV+CIV+ Coa: 6-10%
Villafañe et al. Fricke et al. 2012 Page 27
NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript Villafane JACC 2014
NIH-PA Author Manuscript
TABLE 2
Outcome and predictors of early mortality of the arterial switch operation for TGA with IVS publications during the last decade.
Villafañe et al.
Author, year Inclusive years n % IVS Early 5 Year Survival% 10 Year Survival% Coronary anatomic risk Other predictors of early mortality
Survival For factors
TGA IVS %
Sarris, 2006* 1998–2000 613 70 97 NA NA Single coronary (univariate Open sternum
analysis only)
Lalezari, 2011 1977–2007 332 60.8 88.6 85.8† 85.2† Not a risk factor for early Technical problems with coronary transfer
J Am Coll Cardiol. Author manuscript; available in PMC
mortality
Fricke, 2012 1983–2009 618 64 98.2 98 97 Not a risk factor for early Weight < 2.5 kg ECMO
mortality
Khairy, 2013 1983–1999 400 59.5 93.5† NA 92.7† Single right coronary Postoperative heart failure
artery
Cain, 2014 2000–2011 70 100 98.6 NA NA None identified No predictors of early mortality but earlier
repair < 4 days of age was associated with
decrease resource utilization
Anderson, 2014 2003–2012 140 75 98.6 NA NA None identified No predictors of early mortality but earlier
NIH-PA Author M
repair < 4 days of age was associated with
decrease resource utilization
*
Multicenter study of early results only from the European Congenital Heart Surgeons Association.
†
Results include outcome of all patients undergoing the arterial switch operation and are not confined to those with intact ventricular septum.
Villafane JACC 2014
ECMO = extracorporeal membrane oxygenation; IVS = intact ventricular septum; TGA = transposition of the great arteries with intact septum.
Figure 5. Neonatal ASO and postoperative mortalityMorbidité du switch artériel
• Coronaires
• Coronaire intra-murale
• Coronaire unique
• Voie droite (patch et Lecompte)
• IA sur néo-valve aortique, dilation Ao
• HTAP primitive:
• 1/200 TGV soit 100 fois plus fréquente que
dans la population générale
• Étiologie inconnue
• Traitement médical………PottsSwitch artériel entre 1988-1999
cantly lower in the late repair group in comparison
with the early repair group. The mean postoperative
Associations Between Age at Arterial body weight z score for the early repair group was
–1.2±0.95 and –1.9±1.3 for the late repair group.
Switch Operation, Brain Growth, and
There was no difference in brain–to–body weight ra-
tio between the 2 groups (early repair=0.11±0.02 ver-
Figure 4. Freq
sus late repair=0.12±0.02). Change in body weight z
Development in Infants With Transposition score trended toward an inverse correlation with age
IVS indicates in
ies; and VSD, v
Lim et al of the Great Arteries Lim et al
Age at ASO and Brain Growth inCirculation.
Infants With2019;139:2728–2738.
TGA Age at ASO and Brain Growth in Infants With TGA
DOI: 10.1161/CIRCULATIONAHA.118.037495
Lim et al Age at ASO and Brain Growth in Infants With TGA
Editorial, see p 2739 Table 3. Bayley-III Composite Scores
Jessie Mei Lim, BSc*
ORIGINAL RESEARCH
Composite
Table 3. Bayley-III Composite Scores
Prashob Porayette, MD*
Score
P Value Early Repair Late Repair
ORIGINAL RESEARCH
ARTICLE
Cognitive 106±9 100±10 0.13
Composite
BACKGROUND: Brain injury, impaired brain growth, and long-term Davide Marini, MD
ORIGINAL RESEARCH
Language 98±13 90±20 0.50
Score Early Repair Late Repair P Value
neurodevelopmental problems are common in children with transposition of Motor 104±13 102±12Vann Chau,
0.76 MD
ARTICLE
Cognitive 106±9 100±10 0.13 Bayley-III scores in early vs late repair groups. Stephanie H. Au-Young,
the great arteries. We sought to identify clinical risk factors for brain injury
ARTICLE
Language 98±13 90±20 0.50
and poor brain growth in infants with transposition of the great arteries PhD
When analyzing for possible predictors of neurode-
Motor undergoing
104±13 the arterial switch
102±12 0.76operation, and to examine their relationship
velopmental outcome, we found that Amandeep
age at surgery Saini, RN
with
Bayley-III scores in early vs lateneurodevelopmental
repair groups. outcome.
(R2=0.21, P=0.03) and days of open Linh G.
chest (RLy,
2
MD
=0.21,
P=0.03) were associated with lower language scores,
whereas the length of stay (R2=0.22, SusanP=0.02)Blaser,
was as- MD
METHODS: The brains of 45 infants with transposition of the sociated great with arteries
lower cognitive scores Manohar Shroff, MD
on the Bayley-III
When analyzing for possible predictors of neurode- (Figure 5). When patients with preoperative complica-
undergoing surgical repair were imaged pre- and postoperatively tions (ECMO using or NEC) were excluded Helen
from theM. Branson, MD
analysis,
velopmental outcome, we found that age at surgery
magnetic resonance imaging. Brain weight z scores were calculated based
the inverse relationship between age Renee Sananes,
at surgery and PhD,
(R2=0.21, P=0.03) and days of open chest (R2=0.21, language development remained significant (R2=0.18,
on brain with volume andlanguage
autopsy reference CPsych
scores, data. Brain injury scores P=0.05).were
Downloaded from http://ahajournals.org by on July 20, 2019
P=0.03) were associated lower Composite cognitive scores were lower in the
determined as2 previously described. Neurodevelopment was
whereas the length of stay (R =0.22, P=0.02) was as-
lateassessed
repair group,atalthough 18 this didEdward J. Hickey, MBBS
not reach statisti-
cal significance (P=0.13). There wasJ.noWilliam correlation Gaynor,
be- MD
sociated with lower months using scores
cognitive the Bayley-III
on the scoresBayley-IIIof infant development. The tweenrelationships
brain weight z score and neurodevelopmental
between clinical variables, brain injury, perioperative brain growth, outcome. and Glen Van Arsdell, MD
(Figure
Figure 5).weight
3. Brain When patients
z score with
comparisons. preoperative complica-
A, tions Lim
brainet al18-month Bayley-III scores wererepairanalyzed.
Steven P. Miller, MD† Age at ASO and Brain Growth
(ECMO
Postoperative or NEC)
weight were
z score excluded
comparison from
in the early andthe
late analysis,
groups and in those with TGA/IVS and TGA/VSD. B, Change in brain weight z score
between pre- and postoperative scans in early and late repair groups and in those with TGA/IVS and TGA/VSD. IVS indicates DISCUSSION intact ventricular septum; Mike TGA, trans-Seed, MBBS†
the inverse relationship betweenseptal agedefect.
at surgery and
position of the great arteries;RESULTS: On preoperative
and VSD, ventricular imaging, moderate or severe white Thematter
main newinjury findings of our study are the associa-
language development remained significant (R2=0.18, tions between older age at repair and the presence
Downloaded from http://ahajournals.org by on July 20, 2019
was present in 10 of 45 patients, whereas stroke was seen inof4aof 45. A similar
theP=0.05).
other 13 Composite
patients cognitive
(29%) with scores
a medianwere age lower of in the at surgery, although this did VSD with impaired perioperative brain growth in
notunable reach statistical signifi-
prevalence of injury was seen on 17
postoperative imaging, and we
infants werewith TGA. Older to age at repair was also asso-
late repair
(14–54) days. group,
Table There although
3.identify
wereBayley-III
no this Composite
did not
significant reachScores
differences statisti-
in cance (R 2
=0.05, P=0.14).
ciated with slower language development. In humans
any clinical risk factors for brain injury. Brain weight zdeveloping scores decreased
anycalofsignificance (P=0.13).between
the clinical variables There was theno correlation
2 groups, withbe- under normal conditions, the early weeks
ORIGINAL RESEARCH
tween brain weight
perioperatively
z score and
in 35 of 45 patients.
neurodevelopmental
The presence of a ventricular septallifedefect
of postnatal coincide with the maximal rate of
the exceptionCompositeof hospital length of stay, which was lon- brain growth and development and may represent a
geroutcome. (P=0.009) and older
in the late repair group. 6 of 32 (19%) patients in
age at surgery Neurodevelopment
(P=0.007) were associated with impaired
period of special vulnerability to the consequences of
Scoreperioperative brain Early
growth.Repair When patients LatewereRepair
divided into those P Value
nutritional undergoing
growth restriction.22 Abnormalities of adult
the early repair group had a VSD versus 5 of 13 (38%) Twenty-four patients brain (18 structure
from the early repair
and function group
surgery during the first 2 weeks of life (32/45) versus those being repaired later have been produced in
ARTICLE
in the late repair group
Cognitive (Table 1). There were
106±9 no other and 6 from
100±10 the late repair
animal group)
models by returned
0.13
modest growth for the
restriction Bay-
during this
DISCUSSION (13/45), infants
clinical variables associated with older age at surgery. repaired later had significantly
ley-III worse
test at 18 perioperative
months.brain spurt.
The brain
23
mean growth
Chronic hypoxemia at this stage results
composite cognitive,
in hypomyelination attributable to the arrest of preoli-
(late repair postoperative brain weight zlanguage, = –1.0±0.90 and versus
motor early
scores repair
were z 105±10
= and (mean scoregrowth
The main new Languagefindings of our study 98±13
are the associa- 90±20 godendrocyte 0.50 maturation reduced cortical
–0.33±0.64; P=0.008). Bayley-III testingpercentile scores fellof within
59), the
97±15normal
associated
(mean range
with for
diminished
score populations of neural stem
percentile of 44),
Associations
tions between Between older age at Age repairat and
Surgery the presence
Downloaded from http
cells. 24–27
Similar findings have been*Drs observed in human
Lim and Porayette contributed
all patients, although age at repair (P=0.03) and days of open chest (P=0.03)
Downloaded from h
of a VSD Motor
with impaired perioperative 104±13
brain growth in and 104±12
102±12 (mean score
newborns percentile
0.76with of
congenital 56),heartrespectively.
disease (CHD) at au-
and Brain Growth were associated with a lower composite language score, andtopsy length andand ofbrain-imaging
on stay
late was studies.
equally.
Impaired
re- brain Figure
infants with TGA. Older age at repair was also asso- A comparison of thegrowth early repair groups
27–30
5. Linear regression of Bayley-III scores with clinical predictor
persists into infancy in patients †Drsfollowing
Miller and repair variables.
Seed contributed
We comparedBayley-III brainassociated
growth in
scores in the
with early
a and
lower late
composite
early vs lateIn repair repair cognitive
groups. score (P=0.02).
vealed no statistically significant differences in equally.
Bayley-III A and B, Composite language scores were negatively correlated with age at
ciated with slower language development. humans of TGA, when reductions in white matter volume are surgery (A) and days of open chest (B). C, Composite cognitive scores were
groups defined above. The mean preoperative brain
weeks scores between the 2 groups. In the early repair group,
associated with delayed speech. 9,31
Suboptimal brain negatively correlated with length of stay.
developing underCONCLUSIONS: normal conditions, the early
Surgery beyond
weight z scores were not statistically different between2 weeks of age is associated
growth with has beenimpairedassociated with poor neurodevelop-
Key Words: arterial switch operation
of postnatal life coincide with the maximal rate of the mean compositemental scores for cognitive,
outcomes in children undergoing language,
◼ brain ◼ staged
growth pal- increased risk of white matter injury with increasing in-
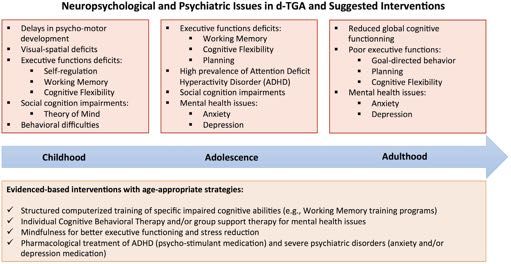
& developmentDevenir neurodevelopmental
• TGV= une des cardiopathies le mieux exploré en
neuropsychologie
• Intelligence (sub)normale (IQ-testing)
• Altération des fonctions cognitives supérieures: « theory of
mind », visualisation temporo-spatiale etc.
• ADHS >> population de contrôle
Kasmi et al. Neuropsychological and Psychiatric Outcomes in D-TGA
Kalfa et al. 2017
Kasmi et al 2017
Calderon et al. 2010
Calderon et al. 2012
Calderon et al. 2014
FIGURE 1 | Neuropsychological and psychiatric issues in dextro-transposition of the great arteries (D-TGA) by age group and suggested
interventions.You can also read

















































