Volumetry of the left atrial appendage in healthy cats by two-dimensional and three-dimensional echocardiography
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria 108 (2021)
Small Animal Hospital1, Department of Biometry, Epidemiology and Information Processing2,
University of Veterinary Medicine Hannover, Foundation, Hannover, Germany; Tiergesundheits-
zentrum Hungerbühler, Tierärztliche Klinik für Kleintiere Salzgitter3, Salzgitter, Germany
Volumetry of the left atrial appendage in healthy
cats by two-dimensional and three-dimensional
echocardiography
J. RAUCH1*, M. FEHR1, M. BEYERBACH2 and S.O. HUNGERBUEHLER3
received October 7, 2020
accepted April 26, 2021
Keywords: left atrial appendage, Schlüsselwörter: linkes Herzohr,
volumetry, RT3DE, RTTPE, mono- Volumetrie, RT3DE, RTTPE, mo-
plane, echocardiography. noplan, Echokardiographie.
Summary Zusammenfassung wurden noch keine Studien zu LAAV
Messungen bei Katzen publiziert.
Introduction Volumetrie des linken
We studied whether monoplane, Aurikulums bei herzgesunden Material und Methoden
triplane and real-time three-dimen- Katzen mittels zwei- und dreidi- In die Studie wurden 50 gesunde
sional echocardiography are feasi- mensionaler Echokardiographie Katzen unterschiedlicher Rassen
ble for volumetric measurement of einbezogen. Das linksatriale (LA)
the left atrial appendage (LAA) in Einleitung Maximalvolumen (LAMax), das LA
healthy cats to establish a founda- Das linke Aurikulum (LAA) scheint Minimalvolumen (LAMin), die Ejek-
tion for further studies on cats with ein noch stark unterschätzter pro- tionsfraktion (EF) und das Schlag-
heart disease. gnostischer Faktor für feline Kardio- volumen (SV) wurden mit eindimen-
pathien zu sein. LAA Dilatation und sionaler, monoplanarer Simpson
Materials and Methods dadurch verursachte Reduktion der Scheibchensummations-methode
The study included 50 healthy Blutflussgeschwindigkeit im LAA er- (SMOD), Real-time triplane echo-
cats of various breeds. Left atri- höhen nachweislich das Risiko für cardiography (RTTPE) und Real-
al (LA) maximum volume (LAMax), Thrombose bei Menschen und time 3D echocardiography (RT3DE)
LA minimum volume (LAMin), ejec- Katzen. An Katzen konnte gezeigt mit TomTec® Software gemes-
tion fraction (EF) and stroke vol- werden, dass verringerte maxi- sen. SMOD wurde im linksapikalen
ume (SV) were calculated based male LAA Blutflussgeschwindigkeit Zweikammerblick angewendet. Alle
on the one-dimensional monoplane (≤ 0,25 m/s) als unabhängiger Parameter wurden zusätzlich inklu-
Simpson method of discs (SMOD) Marker mit Dilatation des linken sive LAA gemessen. Die Volumina
volumetry, as well as on triplane Atriums (LA), LA Funktionsreduktion, exklusive LAA wurden anschlie-
echocardiography (RTTPE) and on linksventrikulärer diastolischer Dys- ßend von den Messungen inklu-
real-time three-dimensional echo- funktion, Thrombose und auch mit sive LAA subtrahiert, um das LAA
cardiography (RT3DE) using the kongestivem Herzversagen in Zu- Volumen zu erhalten.
TomTec® software. Monoplane sammenhang steht. Bei Menschen
SMOD was applied in the left api- mit paroxysmalem Vorhofflimmern Ergebnisse
cal two-chamber view. All parame- konnte sogar in Phasen mit physio- Gemessen mit SMOD (0,97 ml)
ters were also measured including logischem Sinusrhythmus ein re- war der Mittelwert für LAAMax circa
the left atrial appendage (LAA) and duziertes maximales LAA Volumen doppelt so hoch wie mit RTTPE
the volumes of the LA excluding the (LAAV) gemessen werden. Bisher (0,61 ml) und circa dreimal so hoch
*E-Mail: nina.rauch@hotmail.com
131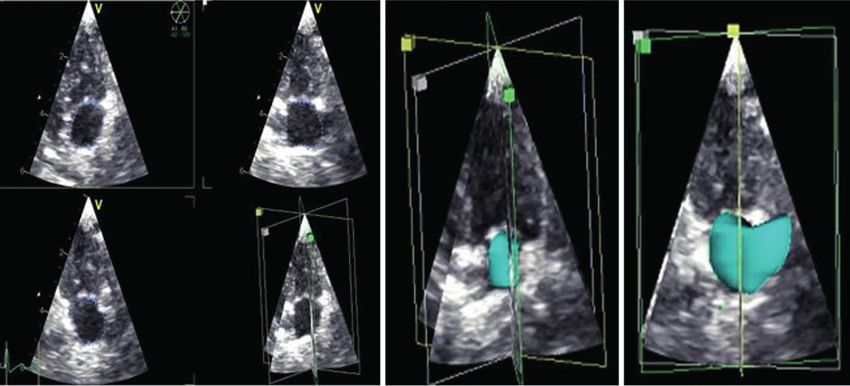
Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria
LAA subtracted from the volumes of the LA including the wie mit RT3DE (0,31 ml). Alter, Geschlecht und Gewicht
LAA to obtain the volumes of the LAA (LAAV). der Katzen hatten keinen signifikanten Einfluss auf die
Ergebnisse.
Results
The monoplane SMOD mean volume for LAAMax Schlussfolgerung
(0.97 ml) was nearly twice as high as the value obtained Es konnte zum ersten Mal gezeigt werden, dass
with the RTTPE (0.61 ml) and three times as high as die Volumetrie des linken Herzohres bei gesunden
that given by the 4D-TomTec™ (0.31 ml). Age, sex and Katzen mit zweidimensionalen und dreidimensionalen
weight had no influence on the results. Methoden zwar möglich, aber noch nicht praktikabel ist.
Diese Ergebnisse liefern eine Basis für weitere Studien
Conclusion an Katzen mit Kardiopathien um herauszufinden, ob es
We have shown the feasibility of monoplane, tri- möglich ist, ein cut-off Volumen für den Start mit anti-
plane and real-time three-dimensional echocardiogra- thrombotischer Therapie zu finden und das Risiko für fa-
phy for LAA volumetry in healthy cats. 4D-TomTec™ is talen Thromboembolismus zu senken.
the least suitable method, whereas monoplane SMOD
and RTTPE appear promising. The results provide the
groundwork for further studies in cats with cardiopa-
thies to determine a LAAV cut-off value to commence
antithrombotic treatment and reduce the risk of aortic
thromboembolism.
Abbreviations: 1D = one-dimensional; 1DE = one-dimensional echocardiography; 2D = two-dimensional; 2DE = two-dimensional echocardi-
ography; 3D = three-dimensional; 3DE = three-dimensional echocardiography; cCT = cardiac computer tomography; cMRI = cardiac magnetic
resonance imaging; CV = coefficient of variation; ECG = echocardiogram; EDV = end-diastolic volume; EF = ejection fraction; ESV = end-systolic
volume; fps = frames per second; L2 = left apical two-chamber view; L3 = left apical three chamber-view; L4 = left apical four chamber-view; LA =
left atrium; LAA = left atrial appendage; LAAMax = left atrial appendage maximum volume; LAAMin = left atrial appendage minimum volume; LA/
AO = proportion of the left atrial diameter to the aortic valve; LAAV = left atrial appendage volume; LAD = Left Atrial Diameter; LAMax = left atrial
maximum volume; LAMin = left atrial minimum volume; LAV = left atrial volume; LV = left ventricle; MD = mean difference; MMode = motion mode;
R4 = right parasternal four-chamber view; R4AL = right parasternal four-chamber view calculated with area/length formula; RT3DE = real-time 3D
echocardiography; RTTPE = real-time triplane echocardiography; SD = standard deviation; SMOD = Simpson method of discs; SV = stroke volume
Introduction as well as reduced early ventricular filling (HOIT et al.,
1993).
The left atrial appendage (LAA) used to be dismissed In humans, LAA mouth diameter and LAA volume en-
as an unimportant left atrial (LA) attachment and is largement correlate with certain types of atrial fibrilla-
still excluded from standard echocardiographic meas- tion (IMANISHI et al., 2015; TANG et al., 2015). Patients
urements in veterinary medicine. However, there is in- with atrial fibrillation and asymptomatic patients with si-
creasing evidence that LAA has multiple functions and nus rhythm have low or absent LAA blood flow, which
has an important prognostic role in human and in feline represents a predisposing factor for thromboembolism.
cardiopathies. The LAA is more elastic than the LA and This provides an explanation for cardio-embolic events
can therefore compensate for a pressure increase in in asymptomatic patients with sinus rhythm (POZZOLI
the LA (HOIT and WALSH, 1992; ITO et al., 1998). The et al., 1991). During non-rheumatic atrial fibrillation,
Frank-Starling mechanism sets in earlier and results more than 90 % of thrombi form in the LAA (MÜGGE
in a regulatory function of the appendage (HOIT and et al., 1994), so appendectomy and appendage clo-
GABEL, 2000). An increase of left ventricular (LV) pres- sure are increasingly common surgeries in human
sure led to the dilatation of both the LA and the LAA medicine. Prior to the procedure, exact LAA measure-
in 66 cats (SCHOBER et al., 2007). LAA dilatation sig- ment is necessary. The LAA has a complex, individu-
nificantly increases the risk of thrombosis in both cats al and highly asymmetrical structure. Little is known in
and humans (FATKIN and FENELEY, 1996; KAMP et al., animals but various types of asymmetrical LAA mor-
1999; SCHOBER and MAERZ, 2006). Pathological dil- phology have been described in humans (WANG et
atation leads to decreased blood flow in the LAA, with al., 2010), although all shapes have approximately the
velocities below 0.25 meters per second (m/s) signifi- same volume (SHIMADA et al., 2020). Diameter meas-
cantly increasing the activation of platelets and clotting urements are quick and easy to perform but carry a
factors (SCHOBER and MAERZ, 2006). Cardiopathy- high risk of failure to detect dilatation, which can occur
induced thrombosis is not a common disorder in dogs. asymmetrically in all directions. Simple LAA mouth dia-
Nonetheless, an experimental study including 12 dogs meter measurements have been used but two-dimen-
revealed that left appendectomy results in significant- sional (2D) and three-dimensional (3D) measurements
ly decreased left atrial reservoir and conduit function of the complex asymmetric structure have a clear ad-
132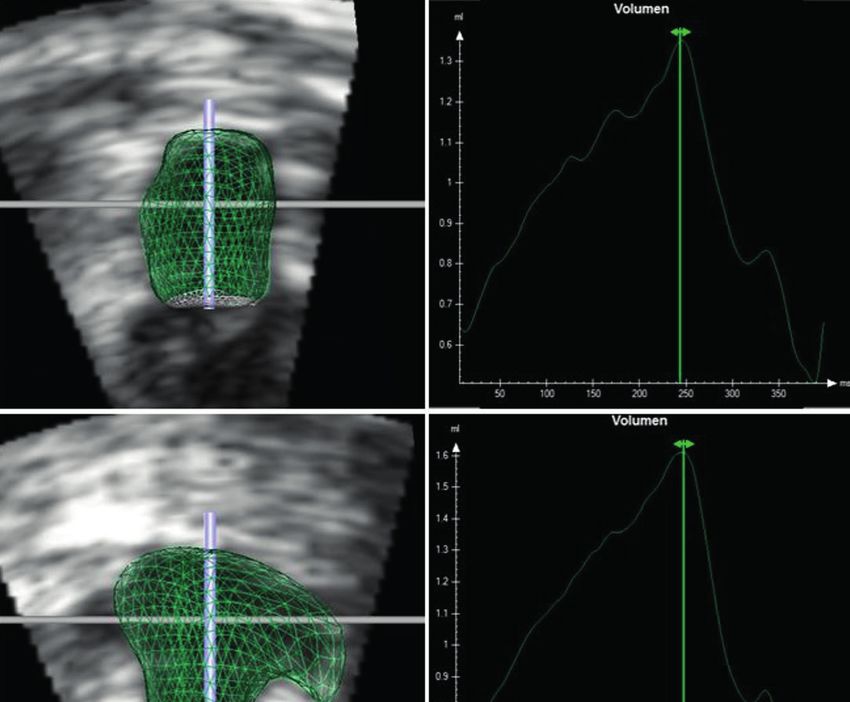
Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria 108 (2021)
Echocardiography
vantage (MÜGGE et al., 1994; TANAKA et al., 2014; AL-
KASSOU et al., 2016; BAI et al., 2017; PINTO TEIXEIRA All 50 cats were examined by the same veterinarian. The ultra-
et al., 2017; HOZAWA et al., 2018). 3D measurements sound unit Vivid E9 was equipped with a GE12S-D Phased Array
show a good correlation to the gold standard cardiac probe for 1DE and 2DE ultrasonography (4–12 MHz) and a GE 3V
computed tomography (cCT) in humans (BAI et al., Matrix Array probe for 3D examination (2.5–3.6 MHz). The cats were
2017). While we are the first to measure left atrial ap- restrained in right lateral recumbency for the right parasternal long
pendage volume (LAAV) in cats, human studies have and short axis view and in left lateral position for left apical two-,
three- and four-chamber view. An ECG was recorded during the
shown the advantages of cardiac computer tomogra-
whole procedure. The examination steps were carried out in ac-
phy and 3D model printing of LAA over RT3D echocar- cordance with recommendations for cardiac chamber quantification
diography (OTTON et al., 2015; OBASARE et al., 2018). by echocardiography of the American Society of Echocardiography
In humans, transoesophageal echocardiography and (LANG et al., 2015). Three consecutive heartbeats were recorded for
cCT are the examination methods of choice (WANG et each plane and saved for offline analysis. All data were transferred
al., 2010; NUCIFORA et al., 2011; OTTON et al., 2015; AL- to a workstation for offline analysis.
KASSOU et al., 2016; BAI et al., 2017; OBASARE et al.,
2018; STREB et al., 2019). As these techniques require Measurement of left atrial diameter (LAD) and LA/AO to classify
healthy animals
general anaesthesia in cats, they are far from suitable
The LAD was measured as described for the reference value of
for everyday practice. We have measured the volume
1.6 cm (SCHOBER and MAERZ, 2005; SCHOBER et al., 2014).
of the left atrial appendage with monoplane two-dimen- The diameter was measured in ventricular end systole, defined
sional echocardiography (2DE), real time triplane echo- as the moment immediately before mitral valve opening (LAMax).
cardiography (RTTPE) and real time three-dimensional The ‘Swedish method’ was used for LA/AO measurement with a
echocardiography (RT3DE). We aimed to test the fea- described limit value of 1.4 (HANSSON et al., 2002; ABBOTT and
sibility and repeatability of volumetric LAA measure- MACLEAN, 2006). The inner edge to inner edge measurement was
ments in healthy cats, to assess the correlation of the performed in the frame immediately after closure of the aortic valve.
methods and to provide a reference for further studies
Volumetry
in cats with cardiac pathologies. We also tested the in-
Left atrial maximum volume (LAMax) and left atrial appendage
fluence of age, sex and weight on LAAV. We did not maximum volume (LAAMax) were measured immediately before the
aim to find the most accurate method, as this would re- opening of the mitral valve, in ventricular end systole, the frame after
quire a comparison to cardiac magnetic resonance im- the ECG’s T wave. Left atrial minimum volume (LAMin) and left atrial
aging (cMRI) or cCT, which would involve not only high appendage minimum volume (LAAMin) were measured immediately
costs and anaesthetic risk but also a substantially low- after closing of the mitral valve at the end of LV diastole, the frame
er heart frequency than in awake animals, which could after the ECG’s P wave.
blur the comparison with regular echocardiography.
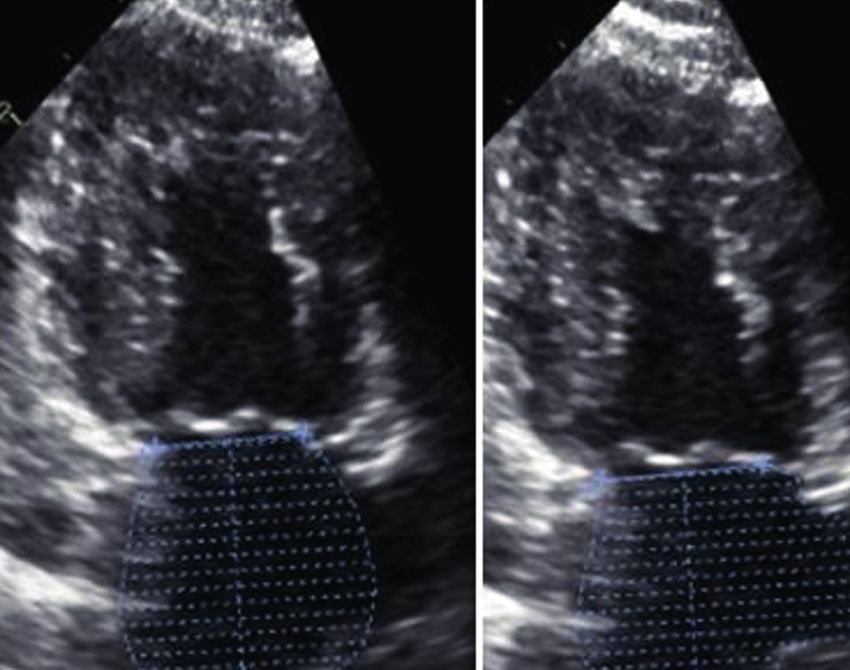
Monoplane examination
We chose the left apical two-chamber axis (L2) view for mono-
plane LA and LAA volumetry and used the 12S-D Phased Array
Materials and Methods probe (Fig. 1). The program calculated end diastolic volume (EDV
equals LAMax), end systolic volume (ESV equals LAMin), ejection
The study was approved by the Ethical Committee of the fraction (EF) and stroke volume (SV), defined as the output during
University of Veterinary Medicine Hannover and was not classified one systole in millilitres (ml). EF marks the percentage of blood vol-
as an animal experiment as data were collected during regular car- ume ejected by the left atrium during one heartbeat. Three consecu-
diac examinations. tive heartbeats were measured and averaged for statistical analysis.
The steps were repeated after monoplane LA measurement, includ-
Animals ing the left atrial appendage.
Fifty privately owned cats were included (26 male, 24 female, Real time triplane echocardiography (RTTPE)
6.48 ± 3.05 years, 48 European Shorthair, 1 Maine Coon and 1 The RTTPE combines measurements in three planes to calculate
Burmese, median weight 4.42 ± 1.41 kg). All animals were presented a dynamic three-dimensional (3D) reconstruction. The GE 3V probe
to the Small Animal Hospital of the University of Veterinary Medicine was used in the left apical four-chamber (L4) axis. Simultaneously,
Hannover for cardiac examination. Cats were not sedated during left apical two- and three-chamber axes (L2 and L3) were displayed
physical examination, blood pressure measurement and the subse- on the screen with LA and LAA visible (Fig. 2). Width and depth
quent echocardiography. The animals were classified as healthy and were modified as needed to reach frame rates above 40 frames per
included in the study when the following criteria were met: 1: there second (fps). Loops of three consecutive heart beats were recorded
was no history of cardiac pathologies, hypertonia, syncope or dys- and saved for offline analysis. In the LAMax frame, the endocardial
pnoea; 2: the clinical examination was clear of pathological findings; border was traced from the septal to the parietal mitral valve annulus
3: the blood pressure did not exceed 160 mmHg; 4: the echocardiog- in all three planes. The start and endpoint were automatically con-
raphy and echocardiogram (ECG) did not show any abnormalities; 5: nected at the mitral valve level. These steps were repeated in the
the anteroposterior diameter of the left atrium, measured in the right LAMin phase and a dynamic three-dimensional LA reconstruction
parasternal long axis, was below 1.6 cm; and 6: the LA/AO ratio was for the whole heart cycle was generated based on the six measure-
below 1.4 in the right parasternal short axis. ments. Additionally, LAMax, LAMin, EF and SV were calculated. The
process was repeated including LAA.
133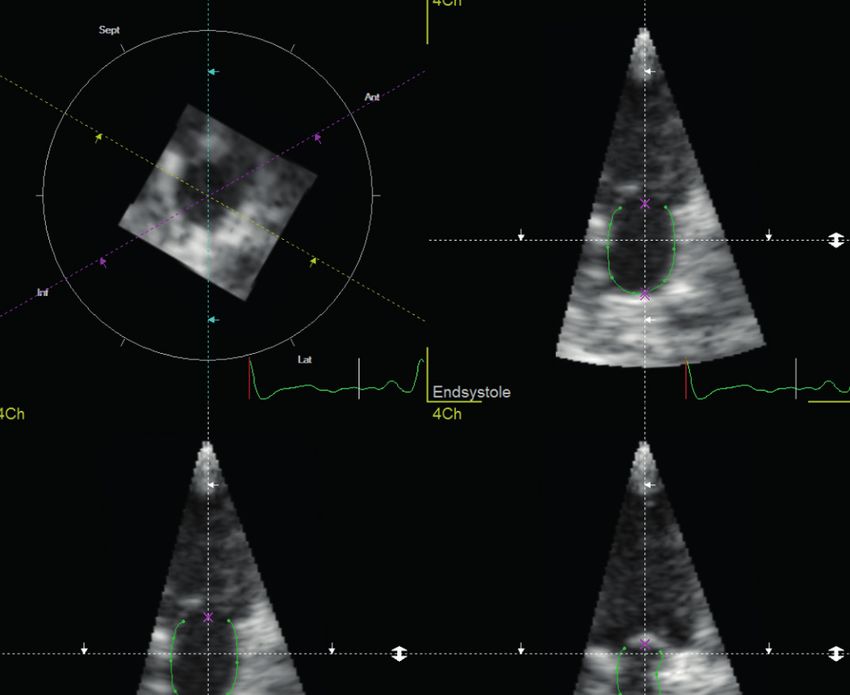
Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria
small size of the LA and the LAA, it was pos-
sible to acquire legitimate real-time 3D data
and no fusion of subvolumes was necessary.
We used the 4D-TomTec™ program for offline
analysis (Fig. 3, 4). The program is designed
to quantify ventricles, so the end-diastole and
end-systole of the ventricle were detected
automatically based on the ECG. One axis
at a time with both end-systole and end-dias-
tole were manually corrected to LAMax and
LAMin. The program automatically detected
the borders for the whole heart cycle. Manual
correction was performed where necessary
before generating the dynamic 3D body and
the volume curve. Based on the volume curve,
LAMax and LAMin were expressed in millili-
tres (ml). SV and EF were also calculated and
all steps were repeated including the LAA.
Time for measurements
The measurement of every method, in-
cluding and excluding LAA, was timed using
a stopwatch. Timing started when data sets
were opened for analysis and stopped as
Fig. 1: Left atrium (LA) and left atrial appendage (LAA) volume measurement using mono- soon as the results were calculated.
plane Simpson method of discs (SMOD): Representative images of left atrial maximum
volume (LAMax) measurement in a healthy cat with SMOD in left apical two-chamber view Statistical analysis
(left) and left apical two-chamber view including volumetry of the left atrial appendage (right)
/ Volumen Messung von linkem Atrium (LA) und linkem Herzohr (LAA) mit monoplanarer Statistics and graphs were calculated
Simpson Scheibchensummationsmethode (SMOD): Repräsentatives Bild von linksatrialem with commercially available software (SAS,
Maximalvolumen bei einer gesunden Katze mit SMOD im linksapikalen Zweikammerblick (links) GraphPadPrism). All measurements were
und linksapikalen Zweikammerblick inklusive Volumetrie des linken Herzohres (rechts) performed three times and averaged for
statistical analysis. Normal distribution was
verified with the Shapiro-Wilk method. Three
additional measurements were performed
and averaged in every L2 views (monoplane,
RTTPE, RT3DE), including the left atrial ap-
pendage but excluding the inlet of the pulmo-
nary veins. The volumes of the LA excluding
the LAA (LAV) were subtracted from the vol-
umes of the LA including the LAA to calculate
the left atrial appendage volume (LAAV). The
percentage increase of LAMax when includ-
ing the LAA was calculated for each method
with the following formula:
Volume Increase (%) = LAAV/LAV*100.
Fig. 2: Left atrium (LA) and left atrial appendage (LAA) volume measurement using Real-time
LAAMax, LAAMin, EF and SV were ex-
triplane echocardiography (RTTPE): Representative images of left atrial maximum (LAMax)
pressed as mean ± standard deviation (SD).
volumetry in a healthy cat with RTTPE (left). The atrium is displayed concurrently in all three
Bland-Altman graphs were created to vis-
angles. The analysis results are shown as three-dimensional dynamic reconstructions of the LA
ualize the relationships between different
excluding (centre) and including the left atrial appendage (right). / Volumetrie des linken Atriums measurement methods for LAAMax (Fig. 5).
(LA) und des linken Herzohres (LAA) mittels triplanarer real time Echokardiographie (RTTPE): Descriptive statistics were calculated for age,
Repräsentatives Bild von linksatrialem Maximalvolumen bei einer gesunden Katze mittels body weight and sex. The influence of age
RTTPE (links). Das Atrium ist gleichzeitig in allen drei Winkeln abgebildet. Die Ergebnisse wer- and weight on the left atrial volume including
den als dreidimensionale Rekonstruktion des LA ohne (Mitte) und mit linkem Herzohr (rechts) and excluding the LAA was calculated with
dargestellt. the coefficient of determination R2. We used
a simple t test to determine whether the
Real-time three-dimensional echocardiography with border detection LA+LAA volumes differ between genders, cal-
The RT3DE generates a 3D body based on true border detection culating the increase of volume from female to male left appendage
algorithms on the entire data set of six measurements. This ena- with the formula:
bles the program to create a volume curve for the entire heartbeat. Mean Difference
LAAV Difference (%) = ( )*100.
RT3DE loops were recorded as described for RTTPE. Due to the LAAV Female
134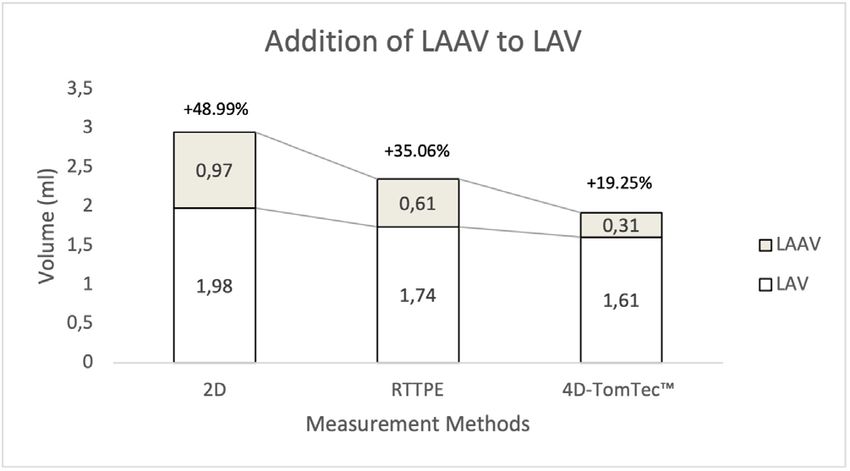
Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria 108 (2021)
Fig. 3: Left atrium (LA) volume measurement including and exclud-
Fig. 4: Left atrium (LA) volume measurement including and exclud-
ing the left atrial appendage (LAA) using Real-time three-dimensional
ing the left atrial appendage (LAA) using Real-time three-dimensional
echocardiography (RT3DE) with 4D-TomTec™ as evaluation pro-
echocardiography (RT3DE) and 4D-TomTec™ as evaluation program:
gram. Representative images of LA volumetry in a healthy cat with
Representative RT3DE analysis of the left atrium in a healthy cat. The
RT3DE. The atrium is displayed concurrently in dynamic short axis
dynamic 3D model of LA and the time volume curve are displayed. Top =
view, left apical four-chamber view, left apical two-chamber view and
excluding appendage; bottom = including appendage / Linksatriale (LA)
left apical three-chamber view. / Linksatriale (LA) Volumetrie inklu-
Volumetrie inklusive und exklusive linkem Herzohr (LAA) mittels dreidi-
sive und exklusive linkes Herzohr (LAA) mittels dreidimensionaler
mensionaler Echtzeit Echokardiographie (RT3DE) und der 4D-TomTec™
Echtzeit Echokardiographie (RT3DE) und der 4D-TomTec™ Software:
Software: Repräsentative RT3DE LA Analyse bei einer gesunden Katze.
Repräsentative Bilder der LA Volumetrie bei einer gesunden Katze mit
Das dynamische dreidimensionale LA Modell und die Volumenkurve
RT3DE. LA ist gleichzeitig und dynamisch dargestellt in Kurzachse,
sind dargestellt. Oben: Exklusive LAA, Unten: Inklusive LAA
linksapikalem Vierkammerblick, linksapikalem Zweikammerblick und
linksapikalem Dreikammerblick.
Tab. 1: Overview of left atrial volumes (LAV) excluding appendage, left atrial volumes including the left ap-
For group comparison, we used pendage and left appendage volumes in healthy cats (n = 50) measured with different methods. Data are
single factor variance analysis and presented as mean ± standard deviation in millilitre (ml) for Max, Min and SV and in percentage (%) for EF. /
a paired t test for multiple pairwise Überblick zum linksatrialen Volumen (LAV) exklusive und inklusive linkem Herzohr (Appendage) sowie zum
comparisons of the normally dis- Herzohrvolumen von gesunden Katzen (n = 50). Gemessen wurde mit drei verschiedenen Methoden. Die
tributed data. All measuring times Daten sind als Mittelwert ± Standardabweichung in Milliliter (ml) angegeben.
were normally distributed and are
therefore specified with mean ± LAV excluding appendage Max Min EF SV
SD. We evaluated the min. and L2 1.98±0.63 0.77±0.24 60.93±8.26 1.22±0.44
max. inter- and intraobserver var-
iability for the measurements of
RTTPE 1.74±0.52 0.68±0.23 60.17±8.96 1.06±0.38
LAV and LAAV by the coefficient of 4D-TomTec™ 1.61±0.52 0.68±0.32 57.41±13.60 0.93±0.38
variation (CV) for all methods. The LAV including appendage
intraobserver CV was calculated
as the standard deviation divided
L2 2.96±0.74 1.10±0.45 63.23±9.60 1.86±0.53
by the mean and expressed as RTTPE 2.35±0.63 0.85±0.32 63.85±8.65 1.51±0.47
a percentage. To assess inter- 4D-TomTec™ 1.92±0.63 0.78±0.39 58.63±15.38 1.14±0.50
observer variability, five patients
Appendage
were independently measured by
two different observers. CV was L2 Appendage 0.97±0.52 0.33±0.32 67.10±26.08 0.64±0.34
then calculated as the standard RTTPE Appendage 0.61±0.25 0.17±0.16 73.66±21.04 0.45±0.22
deviation of the mean difference
4D-TomTec™ Appendage 0.31±0.20 0.10±0.10 63.51±29.96 0.22±0.19
between the two data sets divided
by the total mean, multiplied by Abbreviations: Max = left atrial/appendage maximum volume, Min = left atrial/appendage minimal volume,
100. For all analysis, a p value EF = ejection fraction, SV = stroke volume, L2 = left apical two-chamber view for Simpson method of discs,
of less than 0.05 was considered RTTPE = Real-time triplane echocardiography, 4D-TomTec™ = real-time three-dimensional analysing software.
statistically significant. / Abkürzungen: Max = Maximalvolumen, Min = Minimalvolumen, EF = Ejektionsfraktion, SV = Schlagvolumen,
L2 = linksapikaler Zweikammerblick für monoplanare Simpson Scheibchensummationsmethode, RTTPE =
Triplanare Echtzeit Echokardiographie, 4D-TomTec™ = Dreidimensionale Echtzeit Analysesoftware
135Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria
Sources of supply:
4D-AutoLVQ™: EchoPAC PC, GE Healthcare, Horten, Norway;
4D-TomTec™: 4D LV-Function™ 2.2, TomTec Imaging Systems
GmbH, Unterschleißheim; GE 3V Matrix Array probe, GE 12S-D
Phased Array probe, GE Healthcare, Horten, Norway; GraphPad
Prism, Version 5.00 for Windows: GraphPad Software, San Diego,
Calif., USA; SAS version 9.3: SAS Institute, Cary, NC, USA; ultra-
sound unit: Vivid E9, GE Healthcare, Horten, Norway; workstation:
EchoPAC PC, 108.1.4 Version 110.x.x, GE Healthcare, Horten
Norway
Results
The LAV results were discussed in a separate pa-
per (RAUCH et al., 2020). They served as the basis for
LAAV acquisition and interpretation for the present
manuscript.
Image acquisition
Of 72 data sets, only 50 were suitable for complete
data acquisition. Poor 3DE loop quality prohibited ex-
act LAV measurements and led to the exclusion of 20
patients. The ECG of two patients was incomplete and
prohibited correct analysis. No case was excluded be-
cause of problems with the LAA measurements.
Technically, the ultrasound unit Vivid E9 is able to
create a volume block by using multiple subvolumes of
consecutive ECG-triggered R-R cycles to attain higher
frame rates and therefore better resolution. As it is pro-
grammed for human patients, the software could not
Fig. 5: Bland-Altman plots comparing three methods to quantify left sufficiently recognise the low amplitude of the cat´s R
atrial appendage maximum volume (LAAMax). The methods are: mono- peaks and produced irregular R-R distances. No viable
plane Simpson method of discs (2D), Real-time triplane echocardio- fusion of subvolumes was reached.
graphy (RTTPE) and 4D-TomTec™ analysing software. / Vergleich von
drei Methoden der Messung von Maximalvolumen des linken Herzohres Volumetry
(LAA) mittels Bland-Altman Plots: Die Methoden sind die zweidimen-
sionale monoplanare Simpson Scheibchensummationsmethode,
Left atrial appendage maximum volume
Echtzeit triplanare Echokardiographie (RTTPE) und 4D-TomTec™
Analysesoftware.
The LAAMax results can be summarized as decreas-
ing with an increasing number of measurement planes.
The monoplane SMOD mean volume (0.97 ml) was
Tab. 2: Mean maximum volume of the left atrium (LAV) and the left atri- nearly twice as high as RTTPE (0.61 ml) and three
al appendage (LAAV) in 50 healthy cats, measured with monoplane
times as high as 4D-TomTec™ (0.31 ml). The results
Simpson left apical 2-chamber view (l2), Real-time triplane echocar-
are summarized in Table 1. The monoplane LA volume
diography (RTTPE) and 4D-TomTec™. The mean data are present-
ed in millilitres (ml). The volume increase when including the LAA is
is increased by nearly 50 % (48.99 %) when adding the
presented as a percentage (%). / Mittelwert des Maximalvolumens LAAV. The increase was 35 % for RTTPE. The lowest
von linkem Atrium (LAV) und linkem Herzohr (LAAV) von 50 herzge- LAAV was measured with 4D-TomTec, adding 19 % to
sunden Katzen. Gemessen wurde mit zweidimensionaler Simpson the regular LAV. The results are summarized in Table
Scheibchensummationsmethode im linksapikalen Zweikammerblick 2 and Figure 6.
(L2), Triplanarer Echtzeit Echokardiographie (RTTPE) und 4D-TomTec™
Analysesoftware. Die Werte sind in Milliliter (ml) dargestellt. Die Left atrial appendage minimum volume
Volumenzunahme durch die Addition von linkem Herzohr zu linkem Similarly, LAAMin decreased with an increas-
Atrium wird in Prozent (%) dargestellt. ing number of planes. The mean value was 0.33 ml
Method LAV (ml) LAAV (ml) Increase (%) for monoplane SMOD, 0.17 ml for RTTPE and
0.10 ml for 4D-TomTec™. For both LAV (p=0.9260)
L2 1.98 0.97 48.99
and LAV+LAAV (p=0.2977), there was a significant dif-
RTTPE 1.74 0.61 35.06
ference between RTTPE and 4D-TomTec™ results.
4D-TomTec™ 1.61 0.31 19.25
136Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria 108 (2021)
Ejection Fraction
The EF was highest in RTTPE (73.66 %), followed
by monoplane SMOD (67.10 %) and was lowest in
4D-TomTec™ (63.51 %). For all methods, EF was high-
er in LAA than in LA. Monoplane SMOD values were
significantly different to RTTPE and 4D-TomTec™ re-
sults in both LAV and LAV+LAAV.
Stroke Volume
The calculated stroke volumes ranged from 0.22
ml to 0.64 ml, with standard deviations of ± 0.19 ml
Fig. 6: Comparison of left atrial (LAV) and left atrial appendage (LAAV) to ± 0.34 ml. As expected, SV was highest in monoplane
maximum volumes in 50 healthy cats measured with 2D monoplane SMOD, followed by RTTPE and 4D-TomTec™. The differ-
Simpson method of discs in the left apical two-chamber view (L2), ences were not significant between any of the methods.
Real-time triplane echocardiography (RTTPE) and 4D-TomTec™ ana-
lysing software. Data are presented as volume in millilitres (ml) and in- Influence of age, sex and weight
crease of LAV when adding LAAV in percentage (%). / Vergleiche von
Messungen des Maximalvolumens des linken Atriums (LA) und linken The influence of age and weight on LA volume, in-
Herzohres (LAA) bei 50 herzgesunden Katzen mit zweidimensionaler cluding and excluding the LAA, was assessed using
Simpson Scheibchensummationsmethode aus dem linksapikalen Zwei-
the coefficient of determination R2. Since R2 was < 0.25
kammerblick (L2), Echtzeit triplanarer Echokardiographie (RTTPE)
(for age: 0.003–0.22 and for weight: 0.002–0.14), we
und 4D-TomTec™ Analysesoftware. Die Daten werden präsentiert als
Volumen in Milliliter (ml) und die Volumensteigerung durch die Addition
concluded that age and weight had no influence on LA
von LAAV zu LAV in Prozent (%). volume. The results are summarized in Tables 3 and 4.
The mean difference (MD) of the LAV, including and
Tab. 3: Coefficient of determination (R2) to show the influence of weight Tab. 4: Coefficient of determination (R2) to show the influence of age
on left atrial volumes excluding and including the left atrial appendage on left atrial volumes excluding and including the left atrial appendage
/ Determinationskoeffizient (R2) zur Bewertung des Einflusses des / Determinationskoeffizient (R2) zur Bewertung des Einflusses des
Tiergewichts auf das linksatriale Volumen inklusive und exklusive linkem Tieralters auf das linksatriale Volumen inklusive und exklusive linkem
Herzohr Herzohr
Method LAMax LAMin EF SV Method LAMax LAMin EF SV
L2 0.1206 0.1321 0.0126 0.0658 L2 0.1534 0.1589 0.0105 0.0876
RTTPE 0.0816 0.0590 0.0024 0.0642 RTTPE 0.1793 0.1044 0.0101 0.1580
4D-TomTec™ 0.0348 0.0080 0.0120 0.0307 4D-TomTec™ 0.1473 0.0361 0.0186 0.1242
L2+LAA 0.1389 0.1056 0.0221 0.0639 L2+LAA 0.2180 0.1093 0.0028 0.1476
RTTPE+LAA 0.0585 0.1017 0.0000 0.0738 RTTPE+LAA 0.0906 0.2151 0.0021 0.1897
4D-TomTec™+LAA 0.0342 0.0054 0.0129 0.0289 4D-TomTec™+LAA 0.2136 0.0317 0.0368 0.1882
Coefficient of determination (R2) to show the influence of weight on Coefficient of determination (R2) to show the influence of age on left
left atrial (LA) maximum (LAMax) and minimum (LAMin) volume and atrial (LA) maximum (LAMax) and minimum (LAMin) volume and on
on the ejection fraction (EF) and stroke volume (SV) in 50 healthy cats the ejection fraction (EF) and stroke volume (SV) in 50 healthy cats
measured with 3 echocardiographic methods excluding and includ- measured with three echocardiographic methods excluding and inclu-
ing the left atrial appendage (LAA): 2D monoplane Simpson method ding the left atrial appendage (LAA): 2D monoplane Simpson method
of discs in the left apical two-chamber view (L2), Real-time triplane of discs in the left apical two-chamber view (L2), Real-time triplane
echocardiography (RTTPE), 4D-TomTec™ analysing software, L2 in- echocardiography (RTTPE), 4D-TomTec™ analysing software, L2 in-
cluding the left atrial appendage (L2+LAA), RTTPE including the LAA cluding the left atrial appendage (L2+LAA), RTTPE including the LAA
(RTTPE+LAA), 4D-TomTec™ including the LAA (4D-TomTec™+LAA). (RTTPE+LAA), 4D-TomTec™ including the LAA (4D-TomTec™+LAA) /
/ Determinationskoeffizient (R2) zur Evaluation des Einflusses von Determinationskoeffizient (R2) zur Evaluation des Einflusses von Tieralter
Tiergewicht auf das linksatriale (LA) maximale (LAMax) und mini- auf linksatriales (LA) maximales (LAMax) und minimales (LAMin)
male (LAMin) Volumen, sowie auf die Ejektionsfraktion (EF) und das Volumen, sowie auf die Ejektionsfraktion (EF) und das Schlagvolumen
Schlagvolumen (SV) in 50 herzgesunden Katzen. Gemessen wurde (SV) in 50 herzgesunden Katzen. Gemessen wurde mit 3 Methoden
mit 3 Methoden inklusive und drei Methoden exklusive Herzohr (LAA): inklusive und drei Methoden exklusive Herzohr (LAA): zweidimen-
zweidimensionale Simpson Scheibchensummationsmethode im links- sionale Simpson Scheibchensummationsmethode im linksapikalen
apikalen Zweikammerblick (L2), Triplanare Echtzeit Echokardiographie Zweikammerblick (L2), Triplanare Echtzeit Echokardiographie (RTTPE),
(RTTPE), 4D-TomTec™ Analysesoftware, L2 inklusive Herzohr 4D-TomTec™ Analysesoftware, L2 inklusive Herzohr (L2+LAA), RTTPE
(L2+LAA), RTTPE inklusive Herzohr (RTTPE+LAA) und 4D-TomTec™ inklusive Herzohr (RTTPE+LAA) und 4D-TomTec™ inklusive LAA
inklusive LAA (4D-TomTec™+LAA). (4D-TomTec™+LAA).
137Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria
Tab. 5: Comparison of left atrial volumes excluding and including the left atrial appendage of healthy male (n = 26) and female (n = 24) cats / Vergleich
von linksatrialem Volumen exklusive und inklusive linkem Herzohr gesunder männlicher (n = 26) und weiblicher (n = 24) Katzen
LAMax LAMin
Male Female MD ml MD % Male Female MD ml MD %
Excluding appendage
L2 2.14 1.81 0.33 18.01 0.83 0.70 0.13 18.76
RTTPE 1.84 1.63 0.21 12.88 0.73 0.62 0.11 17.74
4D-TomTec™ 1.69 1.53 0.16 10.46 0.72 0.65 0.07 10.77
Including appendage
L2 3.14 2.75 0.39 14.24 1.20 0.99 0.20 20.55
RTTPE 2.51 2.19 0.32 14.61 0.92 0.77 0.15 19.48
4D-TomTec™ 2.03 1.80 0.23 12.78 0.83 0.73 0.10 13.70
Comparison of left atrial maximum and minimum volumes (LAMax/LAMin) in male (n = 26) and female (n = 24) healthy cats measured with 3 echocardi-
ographic methods excluding and including the left atrial appendage (LAA): 2D monoplane Simpson method of discs in the left apical two-chamber view
(L2), Real-time triplane echocardiography (RTTPE), 4D-TomTec™ analysing software, L2 including the left atrial appendage (L2+LAA), RTTPE includ-
ing the LAA (RTTPE+LAA), 4D-TomTec™ including the LAA (4D-TomTec™+LAA). Mean difference (MD) of LAV between male and female was eval-
uated with a t test. Significant differences (pWiener Tierärztliche Monatsschrift – Veterinary Medicine Austria 108 (2021)
Tab. 7: Comparison of measurement time in seconds / Vergleich der
Discussion Messzeiten pro Methode in Sekunden
Volumetry Analysis Time Mean SD Min Max
L2 22.03 1.85 18.36 28.47
Our major finding is that measuring the LAAV with
2DE and 3DE in healthy cats is challenging but pos- RTTPE 39.66 1.64 37.21 43.11
sible. To determine the LAAV, the LAV is subtracted 4D-TomTec™ 85.29 9.80 76.62 106.48
from the volume of the LA including the LAA. This
L2+LAA 24.25 4.12 22.69 32.57
step is necessary because outlining the LAA alone
is possible in monoplane SMOD but not in 3DE RTTPE+LAA 41.36 3.03 39.95 51.85
methods. This insight provides a good foundation
4D-TomTec™+LAA 87.95 10.02 76.92 112.82
for further studies with cCT and cMRI as well as in
cats with cardiac pathologies. Mean, standard deviation (SD), minimum (Min) and maximum (Max)
duration in seconds for left atrial and left appendage volumetry in
50 healthy cats were measured with 3 echocardiographic methods
Monoplane SMOD
excluding and including the left atrial appendage (LAA): 2D monopla-
Only the left apical two-chamber view is suitable for ne Simpson method of discs in the left apical two-chamber view (L2),
monoplane LAA measurements. The minimal angle Real-time triplane echocardiography (RTTPE), 4D-TomTec™ analy-
deviation of the probe results in foreshortening and an sing software, L2 including the left atrial appendage (L2+LAA), RTTPE
imprecise starting situation. This is particularly prob- including the LAA (RTTPE+LAA), 4D-TomTec™ including the LAA
lematic due to the very small size of the structure and (4D-TomTec™+LAA). There was a significant difference between the
the very low LAAV (mean 0.97 ml). The individual LAA durations of measurement for the three methods (p≤0.005) / Mittelwert
outlines of each cat caused an issue in monoplane (Mean), Standardabweichung (SD), Minimale (Min) und Maximale
SMOD. The cross section of the LAA is a flat oval but (Max) Messdauer in Sekunden für die Volumetrie des linken Atriums
the formula assumes a circular shape. The method can und Herzohres von 50 herzgesunden Katzen. Gemessen wurde mit
3 Methoden inklusive und drei Methoden exklusive Herzohr (LAA):
therefore only provide an approximation of the true vol-
zweidimensionale Simpson Scheibchensummationsmethode im links-
ume and most likely overestimates the LAAV.
apikalen Zweikammerblick (L2), Triplanare Echtzeit Echokardiographie
In cats with cardiac pathologies, the volume of the (RTTPE), 4D-TomTec™ Analysesoftware, L2 inklusive Herzohr (L2+
LAA increases in all directions and the shape is round- LAA), RTTPE inklusive Herzohr (RTTPE+LAA) und 4D-TomTec™ in-
ed. This implies an easier depiction and possibly out- klusive LAA (4D-TomTec™+LAA). Es gab signifikante Differenzen
comes that are closer to the true volume. No veteri- zwischen den Messdauern aller Methoden (p≤0.005).
nary studies have been published on this topic but
our findings provide future projects with a solid foun-
dation. SMOD LAA volumetry is especially interesting In cats with cardiac pathologies, the LAV and the
for everyday practice, as it can be performed with any LAAV increase and the LAA is not emptied properly. The
echocardiography machine and does not require ex- reduced blood flow increases the risk of thrombus for-
pensive probes and separate software. mation (SCHOBER and MAERZ, 2005, 2006). This im-
In human medicine, 2DE is only used to measure plies that LAAMin increases disproportionally more than
the LAA orifice, which it underestimates in compari- LAAMax and the values converge. We speculate that
son to 3DE and CT (AL-KASSOU et al., 2016; BAI et a particular LAAV mean value could serve as indica-
al., 2017). The orifice measurements are required prior tor for LAA enlargement and a higher risk of thrombo-
to closure surgeries, which are not undertaken in cats. sis. In healthy cats, the difference between LAAMin and
The LAAV is currently measured with transoesopha- LAAMax is clearer but only comes up to approximately
geal RT3DE or CT (WANG et al., 2010; NUCIFORA et 0.5 ml. The current recommendation for antithrombotic
al., 2011; OTTON et al., 2015; AL-KASSOU et al., 2016; treatment depends mainly on the LA size and not on the
BAI et al., 2017; OBASARE et al., 2018; STREB et al., LAA volume (LUIS FUENTES et al., 2020).
2019). The large SD can be explained by the very small In summary, monoplane SMOD is the most practica-
volumes, where minor variation has major impact. SD ble method but probably overestimates LAAV and has
may be lower in cats with enlarged LAA. This sugges- the highest standard deviation of all methods tested.
tion requires confirmation in future studies. Our results provide a solid foundation for future stud-
The frame rate for SMOD was approximately 60 ies with cCT, cMRI and cats with cardiac pathologies.
fps and the cats’ heart rate approximately 180 beats
per minute (three beats per second). This means that Triplane echocardiography
every heartbeat was recorded with about 20 frames. In The RTTPE was originally designed for LV volume-
cases with higher heartrates, the number of frames is try and the automatically generated discs are circular,
correspondingly less. Low fps come with the risk that as in SMOD. This may overestimate the variable con-
the maximum and minimum LAAV cannot be correctly tours of the LAA. The advantage of RTTPE is the pres-
distinguished. Monoplane SMOD had the highest fps ence of three measured planes, which produces a more
of all the methods. realistic LAA contour that is also seen in the automati-
139Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria
cally created dynamic three-dimensional model (Fig. 2). but its numerous downsides make it unsuitable for
We conclude that RTTPE gives values that are lower everyday practice. Not only is the low frequency spe-
than those of SMOD because they are closer to the real cial probe 2.5–3.6 MHz expensive, it also creates a low
LAAV. However, in a concrete comparison between the image quality. This is particularly concerning in view of
methods, the difference in LAAMax was roughly 0.4 ml, the very low volume of the LAA, the high heart rates
again highlighting how small the LAAV is and how a mi- and the awake patients. The agitated endocardial bor-
nor deviation in volume has a major impact on the SD. der seems broadened, which leads to a poor quality
There has been no comparable volumetry study in vet- of the semi-automatic detection of the endocardial bor-
erinary or human medicine. It would be interesting to un- der. It was possible to choose the amount of border
dertake a clinical study in cats with cardiac pathologies detection and we always measured with the same me-
or arterial thromboembolic events to assess whether dium level. Many manual corrections were necessary
LAA volumetry could distinguish between the cases and throughout the heart cycle and border detection did not
provide a cut-off value as an indication for antithrombot- work at all in several patients. Manual implementation
ic therapy. During decompensation, the LAA volume in- always poses the risk of error, especially on blurred
creases and the shape alters, which could probably be borders. All of these issues became particularly clear in
seen well with RTTPE. Recording videos with RTTPE the volume curves, which often showed little difference
requires practice but the process itself is fast. Cats with between LAAMax and LAAMin. In many patients we
severe left-sided congestive cardiopathies cannot lie in had to measure multiple loops to produce viable data.
lateral recumbency for long and are not stable in general The temporal resolution of RT3DE was as low as that
anaesthesia. This makes RTTPE a suitable method for of RTTPE. Automatic border detection is only precise
the examination of cats with clinical symptoms, where- when based on as many frames per second as possi-
as cMRI, cCT and transoesophageal echocardiography ble, which is challenging in animals with high heartrate,
are unsuitable. We have to assume that there will nev- such as cats. Having only approximately 13 pictures
er be an LAAV gold standard with cMRI or cCT for cats per heart cycle limits the precision of the method. We
with cardiac pathologies. presume that these reasons are why RT3DE produced
While we performed 2D methods with a high fre- the lowest LAA volumes of all methods.
quency probe 4–12 MHz, the spectrum of the 3D probe Poor 3DE loop quality was the main reason to exclude
was lower 2.5–3.6 MHz. As a result, the manual detec- patients from the study. The amount of manual corrections
tion of the border was more difficult than with mono- led to the longest measurement duration of all the meth-
plane measurements. RTTPE has inferior spatial res- ods. In addition to the costly probe, a separate program is
olution to 2DE but superior to RT3DE. The frame rate required for the offline analysis. This additional expense
was above 40 fps in both 3DE methods but above 60 makes the use of RT3DE in everyday practice even more
fps in 2DE. Forty fps for a heart rate of roughly 180 unrealistic.
beats per minute means that every heart cycle is re- Humans have much lower heart frequencies and high-
corded in approximately 13 pictures; the number of er LAA volumes, so RT3DE is suitable for use in humans.
frames is correspondingly lower for higher heart rates. There have been no comparable studies on LAA volume-
This could be an issue in cats with cardiopathies, as try in veterinary or human medicine. In human LA volum-
their heart rates are higher to compensate for the re- etry, RT3DE correlates extremely well with cMRI but usu-
duced stroke volume. ally gives larger volumes than 2DE (MADDUKURI et al.,
The high costs of the special GE 3V Matrix Array probe 2006; CASELLI et al., 2010; LANG et al., 2015). In a re-
and the special software limit the suitability of RTTPE for cent study on the LAA orifice diameter in humans, RT3DE
small veterinary practices. However, RTTPE has the ad- measurement gave better agreement with the implanted
vantage of a fast retrograde measurement, which takes occluders and had less inter- and intraobserver variability
only twice as long as monoplane and half the time of than 2DE (STREB et al., 2019). 4D-TomTec™ also gives
RT3DE. lower volumes than 2DE methods for LA and LV volume-
In summary, LAA volumetry with RTTPE is feasible in try in dogs (MEYER et al., 2013; LEBLANC et al., 2016a).
healthy cats. It presumably provides more realistic re- However, our findings show that the method is far from
sults than monoplane SMOD but is not yet suitable for practicable or reliable for LAA volumetry in cats.
the average veterinary practice. The results provide a
solid foundation for future studies with cCT, cMRI and Influence of age, sex and weight
cats with cardiac pathologies.
The coefficient of determination R2 was below 0.25
Real-time three-dimensional echocardiography with all methods for age (range of 0.003–0.22) and for
We managed to create real-time 3D models of the weight (range of 0.002–0.14). We saw no clear differ-
LAA in healthy cats with 4D-TomTec™ (Fig. 4). The ence between the results of LA including and excluding
LAA structure is highly asymmetrical but can be rec- LAA. We thus conclude that LAAV does not depend on
ognized well in the real-time 3D reconstruction. The age or weight. Our findings are in agreement with work
method can potentially capture the most realistic LAAV in human medicine, where age also has no effect on
140Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria 108 (2021) the LAAV of healthy patients (ILERCIL et al., 2001). Our ommended when the cat is “at risk of aortic thrombo- study population had a very narrow weight range (4.42 embolism”. The risk is not clearly defined but based on ± 1.41 kg), which could explain the lack of influence on multiple indicators that leave room for subjective inter- the LAAV. Including more large-breed cats would maybe pretation (LUIS FUENTES et al., 2020). We aimed to have altered the result (e.g. Maine Coons). provide a foundation for further studies in cats with car- We found significant differences (p
Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria
so an indirect calculation was required. 4D-TomTec™ that can be used to commence antithrombotic treat-
is the least suitable of the methods for use in cats, ment and reduce the risk of aortic thromboembolism.
whereas monoplane SMOD and RTTPE appear more
promising. The results of monoplane SMOD proba- Acknowledgements
bly deviate the most from the true LAAV but the meth- The LAV results of a previous study by the same au-
od is fast and easy to perform with regular echocardi- thors served as a basis for LAAV acquisition and interpre-
ography machines in everyday practice. The RTTPE tation (RAUCH et al., 2020). The article had been pub-
technique has the best potential but requires a special lished open-access, so the copyright is retained by the
probe, which limits its applicability. Age and weight had authors. The article is licensed under a Creative Commons
no significant influence on the results and we found no Attribution 4.0 International License. http://creativecom-
significant difference between male and female cats. mons.org/licenses/by/4.0/. Data and figures were extend-
The results provide the basis for further studies in cats ed but not changed.
with cardiopathies to determine a LAAV cut-off value
Fazit für die Praxis
Unsere Studie hat gezeigt, dass Volumetrie des linken Herzohres bei gesunden Katzen mit zweidimensi-
onalen und dreidimensionalen Methoden zwar möglich, aber noch nicht praktikabel ist. Diese Ergebnisse
liefern eine Basis für weitere Studien an Katzen mit Kardiopathien um herauszufinden, ob es möglich
ist, ein cut-off Volumen für den Start mit antithrombotischer Therapie zu finden und das Risiko für fatalen
Thromboembolismus zu senken.
References HOIT, B.D., WALSH, R.A. (1992): Regional atrial distensibility.
American J Physiol 262, H1356–H1360.
ABBOTT, J., MACLEAN, H. (2006): Two-dimensional echocardio- HOIT, B.D., SHAO, Y., TSAI, L.M., PATEL, R., GABEL, M., WALSH,
graphic assessment of the feline left atrium. J Vet Intern Med 20, R.A. (1993): Altered left atrial compliance after atrial appendec-
111–119. tomy. Influence on left atrial and ventricular filling. Circ Res 72,
AL-KASSOU, B., TZIKAS, A., STOCK, F., NEIKES, F., VÖLZ, A., 167–175.
OMRAN, H. (2016): A comparison of two-dimensional and real HOIT, B.D., GABEL, M. (2000): Influence of left ventricular dysfunc-
time 3D transesophageal echocardiography and angiography tion on the role of atrial contraction: An echocardiographic-hemo-
for assessing the left atrial appendage anatomy for sizing a left dynamic study in dogs. J Am Coll Cardiol 36, 1713–1719.
atrial appendage occlusion system – impact of volume loading. HORN, P.S., PESCE, A.J. (2003): Reference intervals: An update.
EuroIntervention 12, 2083–2091. Clin Chim Acta 334, 5–23.
BAI, W., CHEN, Z., TANG, H., WANG, H., CHENG, W., RAO, L. HOZAWA, M., MORINO, Y., MATSUMOTO, Y., TANAKA, R.,
(2017): Assessment of the left atrial appendage structure and NAGATA, K., KUMAGAI, A., TASHIRO, A., DOI, A., YOSHIOKA,
morphology: comparison of real-time three-dimensional trans- K. (2018): 3D-computed tomography to compare the dimensions
esophageal echocardiography and computed tomography. Int J of the left atrial appendage in patients with normal sinus rhythm
Cardiovasc Imaging 33, 623–633. and those with paroxysmal atrial fibrillation. Heart Vessels 33,
CASELLI, S., CANALI, E., FOSCHI, M.L., SANTINI, D., 777–785.
ANGELANTONIO, E., PANDIAN, N.G., CASTRO, S. (2010): ILERCIL, A., KONDAPANENI, J., HLA, A., SHIRANI, J. (2001):
Long-term prognostic significance of three-dimensional echocar- Influence of age on left atrial appendage function in patients with
diographic parameters of the left ventricle and left atrium. Eur J nonvalvular atrial fibrillation. Clin Cardiol 24, 39–44.
Echocardiogr 11, 250–256. IMANISHI, J., TANAKA, H., SAWA, T., MOTOJI, Y., MIYOSHI, T.,
FATKIN, D., FENELEY, M.P. (1996): Patterns of Doppler-measured MOCHIZUKI, Y., FUKUDA, Y., TATSUMI, K., MATSUMOTO, K.,
blood flow velocity in the normal and fibrillating human left atrial OKITA, Y., HIRATA, K.I. (2015): Association of left atrial boost-
appendage. Am Heart J 132, 995–1003. er-pump function with heart failure symptoms in patients with se-
FRIEDRICHS, K.R., HARR, K.E., FREEMAN, K.P., SZLADOVITS, vere aortic stenosis and preserved left ventricular ejection fraction.
B., WALTON, R.M., BARNHART, K.F., BLANCO-CHAVEZ, J. Echocardiography 32, 758–767.
(2012): ASVCP reference interval guidelines: Determination of de ITO, T., SUWA, M., KOBASHI, A., YAGI, H., HIROTA, Y., KAWAMURA,
novo reference intervals in veterinary species and other related K. (1998): Influence of Altered Loading Conditions on Left Atrial
topics. Vet Clin Pathol 41, 441–453. Appendage Function In Vivo. Am J Cardiol 81, 1056–1059.
HANSSON, K., HÄGGSTRÖM, J., KVART, C., LORD, P. (2002): Left KAMP, O., VERHORST, P.M.J., WELLING, R.C., VISSER, C.A.
atrial to aortic root indices using two-dimensional and M-mode (1999): Importance of left atrial appendage flow as a predictor of
echocardiography in cavalier King Charles spaniels with and with- thromboembolic events in patients with atrial fibrillation. Eur Heart
out left atrial enlargement. Vet Radiol Ultrasound 43, 568–575. J 20, 979–985.
142Wiener Tierärztliche Monatsschrift – Veterinary Medicine Austria 108 (2021)
LANG, R.M., BADANO, L.P., MOR-AVI, V., AFILALO, J., Appendage Closure Guided by Personalized 3D-Printed Cardiac
ARMSTRONG, A., ERNANDE, L., FLACHSKAMPF, F.A., FOSTER, Reconstruction. JACC Cardiovasc Interv 8, 1004–1006.
E., GOLDSTEIN, S.A., KUZNETSOVA, T., LANCELLOTTI, P., PINTO TEIXEIRA, P., MARTINS OLIVEIRA, M., RAMOS, R., RIO,
MURARU, D. (2015): Recommendations for Cardiac Chamber P., SILVA CUNHA, P., DELGADO, A.S., PIMENTA, R., CRUZ
Quantification by Echocardiography in Adults: An Update from FERREIRA, R. (2017): Left atrial appendage volume as a new
the American Society of Echocardiography and the European predictor of atrial fibrillation recurrence after catheter ablation. J
Association of Cardiovascular Imaging. J Am Soc Echocardiogr Interv Card Electrophysiol 49, 165–171.
28, 1–39. POZZOLI, M., FEBO, O., TORBICKI, A., TRAMARIN, R.,
LEBLANC, N., SCOLLAN, K., SISSON, D. (2016a): Quantitative CALSAMIGLIA, G., COBELLI, F., SPECCHIA, G., ROELANDT,
evaluation of left atrial volume and function by one-dimensional, J.R. (1991): Left Atrial Appendage Dysfunction: A Cause of
two-dimensional, and three-dimensional echocardiography in a Thrombosis ? Evidence by Transesophageal Echocardiography –
population of normal dogs. J Vet Cardiol 18, 336–349. Doppler Studies. J Am Soc Echocardiogr 4, 435–441.
LEBLANC, N., SCOLLAN, K., SISSON, D. (2016b): Quantitative RAUCH, J., FEHR M., BEYERBACH, M., HUNGERBUEHLER, S.O.
evaluation of left atrial volume and function by one-dimensional, (2020): Comparative assessment of left atrial volume in healthy
echocardiography in a population of normal dogs. J Vet Cardiol cats by two-dimensional and three-dimensional echocardiography.
18, 336–349. BMC Vet Res 16, 263.
LUIS FUENTES, V., ABBOTT, J., CHETBOUL, V., CÔTÉ, E., FOX, SCHOBER, K.E., MAERZ, I. (2005): Doppler echocardiographic as-
P.R., HÄGGSTRÖM, J., KITTLESON, M.D., SCHOBER, K., sessment of left atrial appendage flow velocities in normal cats. J
STERN, J.A. (2020): ACVIM consensus statement guidelines for Vet Cardiol 7, 15–25.
the classification, diagnosis, and management of cardiomyopa- SCHOBER, K.E., MAERZ, I. (2006): Assessment of left atrial ap-
thies in cats. J Vet Intern Med 34, 1062–1077. pendage flow velocity and its relation to spontaneous echocardi-
MADDUKURI, P.V., VIEIRA, M.L., DECASTRO, S., MARON, M.S., ographic contrast in 89 cats with myocardial disease. J Vet Intern
KUVIN, J.T., PATEL, A.R., PANDIAN, N.G. (2006): What Is the Med 20, 120–130.
Best Approach for the Assessment of Left Atrial Size ? Comparison SCHOBER, K.E., MAERZ, I., LUDEWIG, E., STERN, J. (2007):
of Various Unidimensional and Two-dimensional Parameters with Diagnostic accuracy of electrocardiography and thoracic radio-
Three-dimensional Echocardiographically Determined Left Atrial graphy in the assessment of left atrial size in cats: comparison with
Volume. J Am Soc Echocardiogr 19, 1026–1032. transthoracic 2-dimensional echocardiography. J Vet Intern Med
MEYER, J., WEFSTAEDT, P., DZIALLAS, P., BEYERBACH, M., 21, 709–718.
NOLTE, I., HUNGERBÜHLER, S.O. (2013): Assessment of left SCHOBER, K.E., WETLI, E., DROST, W.T. (2014): Radiographic and
ventricular volumes by use of one-, two-, and three-dimensional Echocardiographic Assessment of Left Atrial Size in 100 Cats With
echocardiography versus magnetic resonance imaging in healthy Acute Left-Sided Congestive Heart Failure. Vet Radiol Ultrasound
dogs. Am J Vet Res 10, 1223–1230. 55, 359–367.
MÜGGE, A., KÜHN, H., NIKUTTA, P., GROTE, J., LOPEZ, J.A., SHIMADA, M., AKAISHI, M., KOBAYASHI, T. (2020): Left atrial ap-
DANIEL, W.G. (1994): Assessment of Left Atrial Appendage pendage morphology and cardiac function in patients with sinus
Function by Biplane Transesophageal Echocardiography in rhythm. J Echocardiogr 18, 117–124.
Patients with Nonrheumatic Atrial Fibrillation: Identification of a STREB, A.W., MITRĘGA, K., PODOLECKI, T. (2019): Two-
Subgroup of Patients at Increased Embolic Risk. J Am Coll Cardiol dimensional versus three-dimensional transesophageal echocar-
23, 599–607. diography in percutaneous left atrial appendage occlusion. Cardiol
NUCIFORA, G., FALETRA, F.F., REGOLI, F., PASOTTI, E., J 26, 687–695.
PEDRAZZINI, G., MOCCETTI, T., AURICCHIO, A. (2011): TANAKA, K., KOGA, M., SATO, K., SUZUKI, R., MINEMATSU, K.,
Evaluation of the left atrial appendage with real-time 3-dimen- TOYODA, K. (2014): Three-dimensional analysis of the left atrial
sional transesophageal echocardiography implications for cathe- appendage for detecting paroxysmal atrial fibrillation in acute is-
ter-based left atrial appendage closure. Circ Cardiovasc Imaging chemic stroke. Int J Stroke 9, 1045–1051.
4, 514–523. TANG, B., ZHANG, H., JIANG, L. (2015): The correlation between
OBASARE, E., MAINIGI, S.K., MORRIS, D.L., SLIPCZUK, L., the mouth diameter of left atrial appendage and stroke risk score
GOYKHMAN, I., FRIEND, E., RODRIGUEZ ZICCARDI, M., in patients with atrial fibrillation. Eur Rev Med Pharmacol Sci 19,
PRESSMANN, G.S. (2018): CT based 3D printing is superior to 790–794.
transesophageal echocardiography for pre-procedure planning in WANG, Y., DI BIASE, L., HORTON, R.P., NGUYEN, T., MORHANTY,
left atrial appendage device closure. Int J Cardiovasc Imaging 34, P., NATALE, A. (2010): Left atrial appendage studied by computed
821–831. tomography to help planning for appendage closure device place-
OTTON, J., SPINA, R., SULAS, R., SUBBIAH, R., JACOBS, ment. J Cardiovasc Electrophysiol 21, 973–982.
N., MULLER, D., GUNALINGAM, B. (2015): Left Atrial
143You can also read

















































