Zimbabwe: Supply Chain Costing of Health Commodities
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Zimbabwe: Supply Chain Costing of Health Commodities JULY 2010 This publication was produced for review by the U.S. Agency for International Development. It was prepared by the USAID | DELIVER PROJECT, Task Order 1.


Zimbabwe: Supply Chain Costing of Health Commodities The authors' views expressed in this publication do not necessarily reflect the views of the U.S. Agency for International Development or the United States Government.

USAID | DELIVER PROJECT, Task Order 1 The USAID | DELIVER PROJECT, Task Order 1, is funded by the U.S. Agency for International Development under contract no. GPO-I-01-06-00007-00, beginning September 29, 2006. Task Order 1 is implemented by John Snow, Inc., in collaboration with PATH; Crown Agents Consultancy, Inc.; Abt Associates, Inc.; Fuel Logistics Group (Pty) Ltd.; UPS Supply Chain Solutions; The Manoff Group, Inc.; and 3i Infotech. The project improves essential health commodity supply chains by strengthening logistics management information systems, streamlining distribution systems, identifying financial resources for procurement and supply chain operations, and enhancing forecasting and procurement planning. The project also encourages policymakers and donors to support logistics as a critical factor in the overall success of their health care mandates. Recommended Citation Sarley, David., Elaine Baruwa, and Marie Tien. 2010. Zimbabwe: Supply Chain Costing of Health Commodities. Arlington, Va.: USAID | DELIVER PROJECT, Task Order 1. Abstract A costing analysis was conducted for the USAID | DELIVER PROJECT field office in Harare to compare six different scenarios, based on the Delivery Team Topping Up (DTTU) system and the essential drug system. This report presents the findings of the average supply chain costs of delivering U.S.$1.00 of health commodities by looking at the relationship between average costs and the value of products managed by the supply chain. Cover photo: A logistics worker in Zimbabwe enters data using Auto DRV software on a rugged laptop. USAID | DELIVER PROJECT John Snow, Inc. 1616 Fort Myer Drive, 11th Floor Arlington, VA 22209 USA Phone: 703-528-7474 Fax: 703-528-7480 Email: askdeliver@jsi.com Internet: deliver.jsi.com

Contents
Acronyms ....................................................................................................................................................................... v
Acknowledgments...................................................................................................................................................... vii
Executive Summary...................................................................................................................................................... 1
Introduction................................................................................................................................................................... 7
DTTU and EDS Overview ......................................................................................................................................... 9
Supply Chain Costing Tool ......................................................................................................................................11
EDS Cost Using a Budget-Based Approach .........................................................................................................13
Costing Scenarios and Assumptions......................................................................................................................15
Results for Scenario 1 and 2....................................................................................................................................21
Results for Scenario 3 and 4....................................................................................................................................27
Results for Scenario 5 and 6....................................................................................................................................33
Comparing Results across Scenarios.....................................................................................................................39
Conclusion—Can the DTTU Be Expanded Further? ........................................................................................51
References....................................................................................................................................................................55
Appendices
A. International Comparisons .................................................................................................................................57
B. Summary of the DTTU Partners (Tier 1) and Facilities (Tier 2) and Their Functions Included
in the Supply Chain Costing Study....................................................................................................................61
C. PHC Commodity List ..........................................................................................................................................65
D. Detailed Approach, Assumptions, and Results..............................................................................................67
Figures
1. Comparison of Costing Results (Average Costs)...........................................................................................4
2. Supply Chain Functions and Tiers (illustrative) .............................................................................................12
3. Breakdown of Costs by Supply Chain Function for Scenario 1 and 2.....................................................22
4. Scenario 3 and 4—Comparison of Tier 1 Costs by Partner .....................................................................29
5. Scenario 3 and 4—Comparison of Tier 1 Costs by Function ...................................................................29
6. EDS Cost Results for Scenario 5 ......................................................................................................................33
7. EDS Cost Results for Scenario 6 ......................................................................................................................37
8. Total Supply Chain Cost by Distribution Tier Excluding Procurement Costs......................................41
9. Comparative Average Costs for Different Supply Chain Scenarios (excluding procurement) .........44
10. Average Cost Breakdown by Component for Each Scenario.................................................................48
11. Comparing the Actual Costs of DTTU and EDS .......................................................................................52
12. NatPharm Distribution Network...................................................................................................................71
iii
Tables 1. Summary of Costing Scenarios .............................................................................................................................2 2. Summary of Differences between Cost Scenarios.........................................................................................15 3. Summary Costs of the DTTU Tier 1 Partners—Scenario 1 and Scenario 2 ..........................................21 4. Summary Costs for the DTTU Supply Chain—Tier 1 Partners for Scenario 1 .....................................22 5. Summary Costs for the DTTU Supply Chain—Tier 1 Partners for Scenario 2 .....................................23 6. Comparison of Transportation Costs for Scenario 1 Versus Scenario 2 ................................................23 7. Comparison of Transportation Cost Metrics for Scenario 1 vs. Scenario 2...........................................24 8. Total Tier 2 Costs for Scenarios 1 and 2.........................................................................................................24 9. Tier 1 Supply Chain Costs between Scenarios 2 and 3................................................................................27 10. Summary Costs for Tier 1 for Scenarios 3 and 4 ........................................................................................28 11. Comparison of Transportation Costs between Scenarios 2, 3, and 4 ...................................................30 12. Scenarios 2, 3 and 4—Comparison of Transportation Metrics for Tier 1............................................31 13. Scenarios 3 and 4—Management Costs for Tier 1 .....................................................................................31 14. Total Tier 2 Costs for Scenarios 3 and 4 ......................................................................................................32 15. EDS Annual Cost Results for Scenario 5 .......................................................................................................34 16. Supply Chain Cost per U.S.$1.00 of Commodities Delivered for Scenario 5 ......................................35 17. EDS Annual Cost Results for Scenario 6 .......................................................................................................35 18. Supply Chain Cost per U.S.$1.00 of Commodities Delivered for Scenario 6 ......................................36 19. Scenario Costing Comparisons........................................................................................................................40 20. Comparing Total Tier 1 and Tier 2 Costs by Scenario..............................................................................41 21. Summary of the Costing Comparison Results (total costs)......................................................................43 22. Summary of the Costing Comparison Results (average costs) ................................................................46 23. DTTU and EDS Cost Drivers...........................................................................................................................47 24. Average Supply Chain Costs Divided into Components ...........................................................................48 25. Supply Chain Cost per U.S.$1.00 of Commodities Delivered for Scenario 6 ......................................49 26. Summary of Cost Estimates for Select Countries by Product Group....................................................57 27. Survey: Central Medical Stores Charge for Logistics Services .................................................................59 28. DTTU Commodities and Their Procurement Agents................................................................................69 29. Sampling Framework...........................................................................................................................................69 30. Comparison of Storage Costs between ZNFPC and NatPharm .............................................................70 31. Key Management Assumptions ........................................................................................................................73 32. Transport Assumptions......................................................................................................................................71 33. EDS Supervision Time ........................................................................................................................................72 iv

Acronyms
AC average cost
CAZ Crown Agents, Inc., Zimbabwe
DFID Department for International Development
DPS Department of Pharmaceutical Services
DRV delivery receipt voucher
DTTU Delivery Team Topping Up
ED essential drug
EDL essential drug list
EDS essential drug system
GFATM Global Fund to Fight AIDS, Tuberculosis and Malaria
GOZ Government of Zimbabwe
HIV human immunodeficiency virus
JSI John Snow, Inc.
LMIS logistics management information systems
LSU logistics sub-unit
M&E monitoring and evaluation
MOH Ministry of Health
MOHCW Ministry of Health and Child Welfare
NatPharm National Pharmaceutical Company
NGO nongovernmental organization
NVP nevirapine
PHC primary health care
PMD Provincial Medical Director
PMTCT prevention of mother-to-child transmission
QA quality assurance
RTK rapid test kit
SCCT supply chain costing tool
SCMS Supply Chain Management System project
SDP service delivery point
v
UNFPA United Nations Population Fund UNICEF United Nations Children’s Fund USAID U.S. Agency for International Development ZIP Zimbabwe Informed Push ZNFPC Zimbabwe National Family Planning Council vi
Acknowledgments
The authors would like to thank and express their sincere appreciation to the Zimbabwe USAID |
DELIVER PROJECT staff for the time, expertise, and support they provided for this activity.
Special thanks go to Carol Mashingaidze and Louis Kajawu; they accompanied the team in the field,
traveling with them throughout the data collection process. We are also grateful to the health facility
staff who took time from their busy schedules to provide us with valuable information. This activity
would not have been possible without the support of the Ministry of Health and Child Welfare and
USAID.
viiviii
Executive Summary
The USAID | DELIVER PROJECT field office in Harare is unique among project offices in that it
manages, rather than just provides, technical support to in-country public health supply chains, The
Government of Zimbabwe and donor and implementation partners have acknowledged that the
Zimbabwe National Family Planning Council (ZNFPC)/Delivery Team Topping Up (DTTU)
system achieves high product availability for the 11 contraceptives and health products it carries.
Based on the vendor-managed inventory system used in the commercial soft drinks industry, this
system puts the burden of stocktaking and calculating top-up amounts on delivery teams that serve
as a mobile warehouse, instead of on the already busy medical staff in each facility. The question
often asked is—at what cost? Also, how would those costs change if different products were added
to the delivery routes? How do they compare to a more traditional pull essential drug system (EDS)?
The current study applies a function-based supply chain costing tool (SCCT) to answer these
questions and to guide counterparts with supply change management decision making. Commercial
supply chain costs are often difficult to estimate; this is particularly true of public health supply
chains. Costs occur across multiple functions (procurement, storage, transportation, management),
across different organizations, and at different levels or tiers (central, regional, facility-level, etc.).
The function-based SCCT uses an analytical approach to identify, organize, collect, and estimate
costs, and then analyzes them. After costs are analyzed, they can guide supply chain system design,
help ensure supply chains are properly funded, and improve efficiency so that more funding is
available for necessary products. However, supply chain costing is not a simple accounting exercise.
The tool uses accounting information, where available, but this is supplemented with primary data
collection, including an analysis of the time, effort, and resources needed to complete different
supply chain functions—in Zimbabwe, a combination of key informant interviews and direct
observations also provided rich data.
Cost comparisons were made in a series of different scenarios, which are described in this paper.
Because these scenarios involved different product bundles and volumes, we calculated the average
supply chain cost of delivering U.S.$1.00 of health commodity in each scenario. This enabled us to
look at the relationship between average costs and the value of products managed by the supply
chain to address some of the key management questions summarized in table 1.
1Table 1. Summary of Costing Scenarios
Scenario Commodity Delivery Cost Results Used to Answer the
Bundles Approach Comparisons Following:
Delivered Made
Scenario 1 11 Family planning Delivery — What is the cost of delivering 11 family
Team planning commodities using the
Topping Up bimonthly DTTU system?
(DTTU)
Scenario 2 11 Family planning DTTU Scenario 2 vs. What is the cost impact of moving from
scenario 1 a bimonthly to a quarterly delivery
schedule?
Scenario 3 11 Family planning Integrated Scenario 3 vs. What is the cost impact of adding the
+ 44 primary DTTU scenario 2 44 PHC commodities to the quarterly
health care (PHC) DTTU schedule, when staff are on
project salaries?
Scenario 4 11 Family planning Integrated Scenario 4 vs. What is the cost impact of adding the
+ 44 PHC DTTU scenario 3 44 PHC commodities to the DTTU if
staffed by personnel on public service
salaries only versus the development
partner/project salaries assumed in
scenario 3?
Scenario 5 44 PHC EDS pull — What is the cost of delivering the 44
PHC commodities using the pull EDS on
a quarterly schedule?
Scenario 6 44 PHC + 11 EDS pull Scenario 4 vs. What is the cost of an integrated DTTU
family planning scenario 6 system compared to a pull EDS handling
the same products on a quarterly
schedule?
In estimating the supply chain costs, we adopted two interlinked approaches. First, we used the
function-based costing tool to collect all the transport, management, and storage costs incurred at
the central and branch level for the 11 DTTU commodities. Working with the USAID | DELIVER
PROJECT, Crown Agents, and the ZNFPC offices, we collected information on all the costs
incurred to operate the DTTU. We called these tier 1 costs. The tool was also used to collect facility-
level (tier 2) costs for a cross-section of 29 facilities. This included their management and storage
functions because those facilities did not incur transport costs. Facilities visited covered the main
types of primary and secondary health facilities in urban and, where appropriate, rural settings.
These 2009 costs, estimated under scenario 1, captured how the DTTU operated with a bimonthly
delivery schedule. These cost estimates were then used to calculate three other scenarios—2, 3, and
4—each with different adjustments. In scenario 2, we estimated the costs if the 11 DTTU
commodities were moved to a quarterly delivery schedule. Then, in scenario 3, we added 44 primary
health care commodities to the 11 carried by the DTTU. In scenario 4, we recalculated scenario 3
costs using the government of Zimbabwe per diems and salaries for the truck delivery teams and
other partner-supported salaries from scenario 3.
For the EDS scenarios 5 and 6, we used a budget-style approach to estimate the costs. The lack of
actual EDS information by function meant that the function-based approach used in the earlier
scenarios would require numerous assumptions. Data from scenarios 3 and 4 helped to project out
2what costs would be if the EDS was fully functioning. Discussions with stakeholders in three
workshop/meetings resulted in an agreement on the structure of the EDS scenarios and the
assumptions being made for unit costs and number of staff, and other resources required, similar to
a budget-based approach.
While the cost analysis captures all the in-country supply chain functions, we have not included the
procurement fees in the cost comparisons. As most of the procurement is done offshore, the
procurement fees are included as part of the landed cost of the commodities. This should not be
confused with the logistics sub-unit’s (LSU’s) handling charges to clear products from customs when
costs are incurred in-country and are categorized under the procurement function. National
procurement costs could be estimated for the EDS scenarios, while donor procurement costs vary
considerably from donor to donor.
Before reviewing cost estimates from the different scenarios, it is necessary to understand the
different factors that drive costs for the DTTU and EDS. A key cost driver for the DTTU scenarios
is the amount of time the delivery team needs to spend in the field on their delivery routes. As the
number of products increase, more time is required in the field to count inventory at facilities and
then to pick the products to leave behind. At some point, if the number of products becomes too
large, then the cost of the team time and the cost of their per diem will become too costly. Because
the DTTU operates like a mobile warehouse, there is a limit to the number of products that can be
managed in one drop. For larger numbers of products, it may be less costly to do the picking and
packing in the central or branch warehouse, rather than on a mobile warehouse. DTTU program
management is another important cost driver, but this is likely to decrease as more products are
added. Transport costs may increase.
By comparison, the key cost drivers with the pull EDS are the number of staff to be trained, staff
turnover that requires frequent training, supervision costs, and the time spent by staff managing
their own stock. With 1,404 facilities to be managed, these average costs are substantial for smaller
volumes of products, but the costs decrease as the value and volume of product handled increases.
The cost drivers, described earlier, suggest that for smaller numbers of products, the DTTU
approach will probably have lower average costs than the EDS approach. As the number of
products increase, the average cost of the EDS will decrease and, at some point, will probably be
lower than the costs for the DTTU.
The cost of a DTTU delivery for 11 products on a bimonthly schedule is, on average, U.S.$0.27 to
deliver each $1.00 of commodity carried (see figure 1). This average cost is reduced to $0.252 with a
quarterly schedule because of savings in transport cost. Therefore, a quarterly schedule is a more
efficient approach to product delivery. Adding the 44 PHC commodities to the DTTU increases the
total operating costs by $1.5 million, but this is matched by an increase in the value of the
commodities handled. The average cost for delivering the 55 products decreases to $0.234 on a
quarterly delivery schedule. However, average costs are reduced to $0.197 per $1.00 of delivered
commodity if the Ministry of Health (MOH) salaries and per diems are used instead of project
salaries and per diems.
By comparison, the average cost of delivering product under the two EDS scenarios is higher.
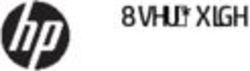
3Figure 1. Comparison of Costing Results (Average Costs)
Scenario 1 Ave rage Cost U.S.$ $0.270
Scenario 2 Ave rage Cost U.S.$ $0.252
Costs lowe r by
Scenario 2 vs Scenario 1
$0.018
Scenario 3 Ave rage Cost U.S.$ $0.234
Costs lower by
Scenario 3 vs Scenario 2
$0.018
Scenario 4 Ave rage Cost U.S.$ $0.197
Costs lower by
Scenario 4 vs Scenario 3
$0.037
Scenario 5 Ave rage Cost U.S.$ $0.300
Costs increase d by
Scenario 5 vs Scenario 4
$0.103
Scenario 6 Ave rage Cost U.S.$
$0.265
Costs lower by
Scenario 4 vs Scenario 6 $0.068
The smaller total volume of products associated with the 44 products results in the highest average
cost of all the scenarios—$0.300. The EDS is designed to handle a larger volume of products. This
is evident in scenario 6 where the average cost for the EDS for the 55 commodities is $0.265. It
should be noted, while only 11 commodities are added, the additional volume and value of products
more than doubles that associated with the 44 PHC commodities.
When the results were discussed with the Ministry of Health and Child Welfare (MOHCW) and
National Pharmaceutical Company (NatPharm) counterparts, and donor partners, a number of key
conclusions were drawn:
A DTTU informed push approach appears to be less costly than a pull system for a smaller
number of commodities that are intended for primary health care facilities.
The DTTU delivery system can add PHC commodities for a similar average cost of delivery with
additional funding for capital and operating costs.
4 The costs of staff time, training, and supervision at the facility level represent most of the pull
EDS costs; these costs need to be funded to ensure that the approach works. Note that medical
staff must take time away from other duties (including seeing patients, in some cases) to perform
the supply chain activities.
For larger numbers of commodities in a fully functioning, traditional, pull EDS supply chain
costs would probably be less costly than trying to manage these products in a DTTU system.
The pull EDS training and supervision costs would be spread over a larger value of commodities
being handled.
Future applications to the Global Fund need to ensure that these facility costs, particularly staff
time, are funded or they will risk system performance problems.
The average delivery cost is a key indicator that should be considered in further supply chain system
design. The present analysis is a benchmark that can improve the efficiency of supply chain
operations: it can make more funding available to ensure that health products are purchased and
reach their intended clients.
56
Introduction
This report presents the results of a supply chain costing exercise conducted in Zimbabwe in
November 2009 and January 2010. The U.S. Agency for International Development (USAID)
funded this work through the USAID | DELIVER PROJECT; it included staff from the USAID |
DELIVER PROJECT and Abt Associates, Inc. The work involved the second field test of the
function-based supply chain costing tool, which the project developed; it followed earlier work by
the same team in Zambia. The work in Zimbabwe differed in a number of important ways from the
analysis in Zambia. Discussions with the project field office identified three key objectives for the
cost work:
Provide project stakeholders with an understanding of the Zimbabwe National Family Planning
Council (ZNFPC)/Delivery Team Topping Up (DTTU) costs.
Undertake some cost comparisons for different supply chain scenarios involving different
bundles of products of primary health commodities and different ways of delivering them.
Develop a tool to guide management decision making that local staff and counterparts could
apply in looking at further system design options.
The DTTU system was implemented in Zimbabwe to ensure the availability of condoms and
contraceptives in public and nongovernmental organization (NGO) facilities. It adapts a supplier-
managed inventory approach—often used in the commercial soft drinks sector—to the public
health system in Zimbabwe. The DTTU systems require that special investments are made to ensure
that reliable vehicles, drivers, technical staff members, or a combination of these, will directly
provide or top up facilities with the health products they need. Under a DTTU system, delivery trucks
are filled with a predetermined quantity of a product—usually based on past consumption
patterns—and the product is driven to health facilities. The drivers or other staff members who are
part of the delivery team calculate current consumption and resupply quantities, and they reconcile
inventories at each facility they visit. Thus, they top up the inventory of each facility with quantities
needed to meet the next period’s requirements.
As the USAID | DELIVER PROJECT’s success story, Delivery Team Topping Up: Bringing
About Reliable Distribution in Difficult Environments, stated, the DTTU has been very successful
in improving product availability.
“An evaluation in 2007 showed remarkable results. Focusing on condoms for HIV and AIDS prevention and
contraceptives, the evaluation found that throughout the nation, the DTTU system has achieved 99 percent of coverage
of all service delivery points—more than 1,200 clinics. On the same national scale, it has achieved more than 95
percent availability of contraceptives and HIV and AIDS condoms.”
To ensure product availability during Zimbabwe’s economic difficulties, donors have invested in
establishing and operating the DTTU. A key question now for donors and the Government of
Zimbabwe (GOZ) is whether the DTTU is still justified as the economy recovers. Is the DTTU
approach more expensive than more traditional approaches, such as the pull essential drug system
(EDS)? What adjustments can be made to the DTTU to reduce cost? How would costs be affected
7if the number of products carried was expanded? Should the National Pharmaceutical Company (NatPharm) and the Ministry of Health consider a version of the DTTU approach as more products are funded by donors, including the Global Fund? To answer these questions requires an understanding of the actual cost of delivering products included in the DTTU and the alternative approaches. A previous analysis (Bunde et al. 2007) looked at the DTTU accounting data to derive an estimated delivery cost of 12 percent of the commodity value. This analysis did not include the Ministry of Health and Child Welfare (MOHCW) costs; it was based only on the DTTU accounting information; it did not include an estimation of the actual costs of the different functions associated with the DTTU. To address the questions listed above requires a fuller understanding of all the costs involved in ensuring that products are delivered. Costs need to be estimated across several implementing partners, including donor and the GOZ-funded entities. It also requires an understanding of costs incurred at different tiers or levels in the supply chain in Zimbabwe. As funding for health commodities in Zimbabwe increases, the Ministry of Health and NatPharm are seeking increased funding for their supply chain. Estimating the cost of a fully functional EDS in Zimbabwe will help ensure that sufficient resources are identified for both NatPharm and the MOHCW to fund the supply chain. Estimating EDS costs will help in the system design and will allow comparisons with the cost of alternate models of delivery, such as the DTTU and Zimbabwe Informed Push (ZIP) models. The DTTU contrasts with the traditional pull EDS where the staff at the facilities are responsible for these calculations and for ordering resupplies. The DTTU more closely resembles an informed push system where pre-determined quantities are delivered, but the quantity size can vary and they are determined or informed by current consumption data collected by the delivery team. The USAID | DELIVER PROJECT developed and applied a supply chain costing tool (SCCT) in Zambia (Baruwa, Tien, and Sarley 2009). Zimbabwe was selected as the second field test for the tool. The SCCT was used directly to cost the DTTU. Discussions with the project office in Harare revealed that the range of different questions to be addressed also required the application of the costing tool using a budget-based approach, which would be applied to estimate costs of the EDS in two different scenarios. The function-based costing tool provides the actual cost of delivering product using the current variations of the DTTU supply chain (scenarios 1–4). A different budget-based version of the costing tool was developed to cost the hypothetical pull EDS (scenarios 5–6). This report includes a synopsis of the DTTU and the EDS, summarizes the costing methodology, then presents six different cost scenarios. See the appendix in this report for more detail on the assumptions behind each scenario. 8
DTTU and EDS Overview
The DTTU has three main characteristics: (1) specially trained ZNFPC team leaders, drivers (or
other accompanying technical staff members), (2) reliable transport, and (3) adequate operating
funds. In situations where options for transport within the public and private sectors are not
available or reliable, this approach means, in practice, that the DTTU will need to acquire and
maintain its own fleet of trucks. This creates a major start-up cost, but, in some fragile state
situations, donors recognize the need and are prepared to cover this expense. The recurrent costs of
fuel, maintenance, and staff travel expenses must also be covered.
The DTTU system is a partnership of the USAID | DELIVER PROJECT and Supply Chain
Management System (SCMS) projects, funded by USAID, Crown Agents, Inc. Zimbabwe (CAZ)
funded by DFID, the Zimbabwe National Family Planning Council (ZNFPC) and the logistics sub
unit (LSU) of the MOHCW AIDS & TB Unit and National Pharmaceutical Company (NatPharm).
Since its implementation in 2004 with condoms and family planning products, several additional
HIV-related products have been added to the system; it has developed a reputation for reliability
despite the challenging social and economic environment.
The project in Zimbabwe supports the DTTU through two of its USAID-funded projects: the
USAID | DELIVER PROJECT (project) and the Supply Chain Management Systems (SCMS)
project. The project in Zimbabwe provides technical support to the DTTU. The project also
employs logistics support, drivers, administrators, and supervision staff; they are seconded to the
MOHCW. They may also be funded by other partners, such as Crown Agents, Inc. (CAZ) or GOZ,
through ZNFPC. Vehicles, maintenance, and fuel are also paid for and managed by the project in
Zimbabwe. The USAID | DELIVER PROJECT procures commodities through the project (male
and female condoms and contraceptives); SCMS procures HIV/AIDS commodities. SCMS funds
the staffing of the LSU, which also funds and manages the procurement of HIV-related products.
The funding source, USAID, is used from this point forward and refers to both the USAID |
DELIVER PROJECT and the SCMS project.
The Department for International Development (DFID) (United Kingdom) supports the DTTU
through its contract with CAZ. This funds the salaries and per diems for drivers and other
supervisory staff of the DTTU. In addition, CAZ quantifies, procures, and funds the pills for family
planning. The ZNFPC is the agency of the GOZ that provides storage facilities for the family
planning commodities and pays the salaries of the team leaders who accompany the delivery vehicles
as part of the DTTU delivery teams (per diems are paid for by CAZ).
The LSU resides physically at the NatPharm site but it is funded by SCMS. The LSU quantifies and
procures HIV-related products and also provides some supervision for the DTTU. The preventing
mother-to-child transmission (PMTCT) and rapid test kit (RTK) commodities are stored at
NatPharm.
Although UNICEF is not a DTTU partner in the current system, UNICEF currently procures the
primary health care (PHC) drugs for the EDS. Their role is modeled in several of the cost scenarios
involving primary health care commodities.
9The DTTU system is a two-tiered system. Goods are procured, stored, and transported by facilities in the first tier (tier 1), which is made up of the DTTU partners discussed earlier in this report. After procurement and in-country delivery, the commodities are stored either at NatPharm or the ZNFPC; the DTTU delivery trucks and teams pick them up and then distribute them directly to the second tier facilities (tier 2) facilities, which include— central/university/provincials/municipal/district/rural hospitals maternity clinics/polyclinics rural health centers and clinics. All the tier 1 facilities, as well as a sample of each type of the tier 2 facilities, were included in the DTTU supply chain costing study. A full list of these facilities is provided in appendix C, including a list of functions performed by each partner and facility, the region where the facility is located, as well as the population density (high/low) of the facility and whether or not it is a rural/urban facility. See appendix D for a list of the 11 products carried by the DTTU and the 44 products carried by the EDS. NatPharm has historically operated a pull order system for essential drugs. Health facilities issue requisition orders for the products needed; they are then sent by post or in person to their district pharmacy manager, which is located at the district hospital. The orders are then processed, checked, and consolidated at the district before transmission to the local NatPharm branch store for fulfillment. The four branch stores then obtain their products from one of the two regional stores. The EDS has suffered in the economic crisis from underfunding and this has contributed to reduced product availability. The UNICEF PHC kits are providing a much-needed supply of products to the system, but a lack of budget for staff training and supervision has slowed the process. 10
Supply Chain Costing Tool
The supply chain costing tool is used to estimate the cost of getting individual commodities from
the port of entry delivered through the supply chain, down to the service delivery point (SDP). It
looks at actual processes, and the time and effort required to complete delivery of the product at
each stage in the supply chain.
The approach used in the supply chain costing tool is to model the supply chain in terms of its
structure and management, and functions; and the quantity of product or commodity that flows
through it. Each of these supply chain characteristics must be described in detail in order for the
tool to determine supply chain costs. These three characteristics determine both the sample of
facilities that must be included in the data collection process and the manner in which the metrics
calculated by the tool may be used to determine the previously described categories of costs.
The core functions of a supply chain costed by the tool include—
procurement
storage
transportation
management (quantification, quality assurance/supervision, logistics management information
systems [LMIS], training and operating costs).
Each function is divided into a labor component, an equipment cost component, and a third other
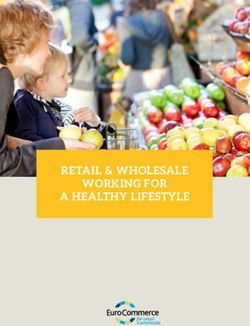
section to capture costs peculiar to the particular function. Figure 2 is adapted from the work of
Raja, Grace, and Chesley (2000) on costing Ghana’s supply chain and it shows how the costs of a
supply chain can be described in terms of both tiers and function.
The total delivered cost in figure 2 is defined as the total cost of delivering a unit of a commodity to
the end user. The unit can be defined in value terms by $1,000 worth of commodities, or
volumetrically as per meter squared (m2), or by weight per kilo (kg) of commodity. The total
delivered cost includes the cost of procuring that unit at each tier of the supply chain, the cost of
storing that unit at every point where the commodities are stored, and the cost of transporting each
commodity unit between each storage point in the supply chain.
11Figure 2. Supply Chain Functions and Tiers (illustrative) The total delivered cost is typically analyzed in terms of the percentage of the value of the good required to deliver the good; e.g., if it costs $200 to deliver $1,000 worth of family planning and HIV commodities, then the delivered cost is 20 percent of the value of the delivered goods. This indicator can help supply chain managers budget sufficient funds for product delivery. This is particularly important when policymakers, planners, and development partners are planning commodity donations and procurement actions because this helps budget the cost of ensuring that essential commodities are delivered to the end user in-country. The total costs by tier in figure 2 refers to the total costs of every function performed by each facility, in each tier; which can be aggregated to estimate the total cost of each tier. This information is typically presented in terms of who is covering these costs so that it can be determined what role different partners are playing. The types and quantities of commodities distributed by the supply chain provide the denominator to determine the various unit or average cost metrics. To use the tool, every commodity in the supply chain must be described, including the price of the commodity at procurement and the volume of each unit of the commodity during each stage of its supply chain journey. Usually, supply chains straddle several administrative and institutional layers and involve multiple players, so that it is common to find that no single organization knows the exact total costs of the supply chain system. Furthermore, because the costs are not recorded by activity, but rather by accounting or budget line; staff salaries and benefits, fuel, office costs, and a walk-through approach interviewing key players is necessary to determine the costs involved in delivering commodities. 12
EDS Cost Using a Budget-Based
Approach
As described above, the costing tool can help determine the cost of the actual inputs for supply
chain systems that are working. In situations where supply chain budgets have been underfunded, a
different approach is required. Where there have been budget constraints, the necessary products
may not be available. Staff may not be funded to undertake all the functions required to ensure
product availability. Other resources for training, supervision, and ordering may also be missing.
This summarizes the constraints the pull EDS has been operating under.
Calculating EDS costs requires a theoretical estimation of the resources needed to operate it. This
will require a top down, or macro, approach to approximate the likely costs that would be incurred if
the EDS was fully functional. Constructing a meaningful model of a functioning EDS will involve
multiple levels of assumptions, all agreed to with the stakeholders.
In this type of modeling exercise, the scope for an assumption error is very large. It is better to focus
on building a simple model with consensus on the general assumptions made rather than attempting
to go into intricate detail on how the EDS might work. As Professor Terry Pohlen stated at the
Council for Supply Chain Management Professionals (CSCMP) 2009 Chicago conference when he
commented on supply chain costing, “It is better to be approximately correct than precisely wrong.”
A proposed EDS costing approach is similar to a budgeting exercise undertaken for a workplan
before the work is undertaken. Typically, the budget will involve estimating the main tasks to get the
work done, making assumptions about the level of effort and other inputs, and assigning average
costs to those inputs. This represents our expectation on what the costs of the activity might be.
Validation by stakeholders of the assumptions will ensure that the budget is approved. As the results
will probably be sensitive to the assumptions made, upper and lower estimates will be made based
on different assumptions for key cost factors.
1314
Costing Scenarios and
Assumptions
Several key cost questions need to be addressed.
What is the cost of using the DTTU to deliver commodities?
Can changes in delivery schedules help reduce this cost?
How would delivery costs change if more products were added to the DTTU system?
How does the cost of the DTTU system compare to that of the EDS, if it was fully operational?
How do these costs compare to the costs of other supply chain systems?
To answer these questions, we developed a series of supply chain cost scenarios. Each scenario
involves different assumptions about the value and volume of products distributed and the way they
are distributed. We estimated the costs for the delivery of different commodity bundles with
different assumptions for delivery intervals, delivery approach, and the average costs being used.
Table 2 summarizes the six scenarios developed and the key assumptions underlying each scenario.
Table 2. Summary of Differences between Cost Scenarios
Scenario Commodity Delivery Delivery Average Cost
Bundles Delivered Interval Approach Assumptions
Scenario 1 11 Delivery Team Bimonthly DTTU Average costs from
Topping Up (DTTU) DTTU, Crown Agents,
commodities and other partners
Scenario 2 11 DTTU commodities Quarterly DTTU Average costs from
DTTU, Crown Agents,
and other partners
Scenario 3 44 primary health care Quarterly Integrated Average costs from
(PHC) commodities DTTU DTTU, Crown Agents,
plus the 11 DTTU and other partners
commodities
Scenario 4 44 PHC commodities Quarterly Integrated MOH salary and per
plus the 11 DTTU DTTU diem costs
commodities
Scenario 5 44 PHC commodities Quarterly EDS pull MOH and NatPharm
system average costs
Scenario 6 44 PHC commodities Quarterly EDS pull MOH and NatPharm
plus the 11 DTTU system average costs
commodities
15For ease of comparison, we focus on the cost of delivery as a percentage of the commodity cost. Comparisons can also be made in terms of the cost per kg or m2 delivered. A comparison of scenarios 1 and 2 will demonstrate whether a bimonthly or quarterly schedule is more cost efficient for the DTTU delivery of its existing 11 products. A comparison between scenarios 2 and 3 can show whether expanding the range of products carried by the DTTU to integrate PHC commodities increases or decreases average costs. While we would expect scenario 4 to cost less than scenario 3, are the cost differences significant? Similarly, comparing scenario 5 and scenario 6 will determine whether expanding the number and volume of commodities covered increases or decreases the estimated EDS costs. Finally, comparing scenario 3 and 4 and scenario 5 and 6 will help gauge whether the integrated DTTU or the pull EDS is the more cost efficient approach to delivering commodities. Scenarios 1 through 4 were all developed using the costing tool. Scenario 5 and 6 used the budget-based approach. It should be noted that we do not attempt to undertake any program effectiveness analysis. This could be considered with the proposed ZIP rollout, as product availability could be considered with cost data. Approach The DTTU system was reviewed as a necessary step before trying to determine the inputs and costs of running the system. Several project reports were reviewed describing the system in detail. The DTTU standard operating procedures manual was also reviewed. Scenario 1 describes the cost of the existing DTTU system based on a bimonthly delivery schedule. Both qualitative and quantitative data was collected to determine the DTTU supply chain costs. Data was collected through interviews with key informants and the review of reports and financial data. The project field office conducted much of the work in advance by working with the MOH, ZNFPC, and NatPharm. Supply chain cost data were collected from a wide range of sources, including logistics reports, transport schedules, expenditure reports, and on-site interviews at each of the facilities sampled. A range of respondents were interviewed to collect information. For facilities in tier 1, at least one person was interviewed in each of the different teams responsible for administrative, financial, logistics/storage, and service delivery functions. For example, the costing team spoke to the logistics advisors that manage transportation and the LMIS to identify the roles played by each partner in the transportation function of the DTTU; and also to obtain all the relevant delivery records required to determine the volume of commodities that flow through the DTTU in a single year. Using the facility’s annual report and payroll documents, the finance and administrative officer for each tier 1 partner was interviewed to determine labor and operating costs. The tool classifies each partner as a facility and then asks the respondent/respondents at each facility which of the three primary functions—procurement, storage, or transportation—does the facility carry out. For example, ZNFPC does not conduct any procurement activities; therefore, the questions focused on ZNFPC’s storage activities. In many tier 2 facilities, very few people actually handled the commodities. Where possible, the data collection team obtaining data from tier 2 facilities followed the schedule of a DTTU delivery route. This enabled direct observation of the delivery team as they worked. To estimate SDP staff time spent on managing DTTU commodities, the SDP staff were asked to estimate the time spent each week or month on supply chain–related tasks. Salary data were then collected or obtained by matching each staff member’s civil service grade to the public service management salary guide, or by asking staff directly. All the SDP facilities’ interviews were completed in less than two hours. 16
A variety of quantitative resources were used; for example, cost data were obtained primarily by
reviewing financial expenditure reports, usually with the facility’s financial or senior administrator.
The JSI/Zimbabwe office and Crown Agents provided information on the quantities of
commodities procured for the entire country and the quantity of commodities delivered to each of
the sampled SDPs. The supply chain costing tool provides pre-programmed surveys to guide
interviews with respondents as they discussed procurement, storage, transportation, operating costs,
and staff time.
After the DTTU cost under scenario 1 was estimated, the next step was to determine all the
assumptions required to estimate the cost of a quarterly DTTU delivery schedule captured in cost
scenario 2. Discussions with DTTU fleet management staff confirmed that a quarterly delivery
schedule would not require any increase in the size of the transport fleet. The key differences were
related to fleet operating costs associated with the new delivery schedules, including the potential
difference in labor and fuel costs that might occur if the schedule was changed.
Comparing scenarios 2, and 3 and 4, was a more complex analysis. Scenarios 3 and 4 involved the
addition of the 44 PHC products. The increased volume would require significant adjustments to the
DTTU system. Delivery schedules had to be adjusted to account for the need to replenish delivery
trucks with commodities during a distribution run. The number of vehicles had to be increased
which, in turn, increased fuel, insurance, and maintenance cost. Finally, all these changes also
affected the number of delivery days for drivers and team leaders. Additional staff also had to be
added to accommodate the inclusion of the 44 PHC commodities under supervision, quantification,
and the LMIS. The staff time at the health facility was also doubled to account for their increased
time to manage the PHC commodities.
A sample of facilities was selected to ensure geographical representation and to ensure that each type
of facility was included. The sample of facilities covered the two largest cities in Zimbabwe—Harare
and Bulawayo. The two sampled provinces included Manicaland, which is the most eastern province,
with the densest population of health facilities; and Matabeleland South, a sparsely populated
southwestern province. Out of approximately 1,404 facilities, the data collection team visited 29.
For scenarios 5 and 6, as a macro budgeting exercise, the EDS costing model estimated the total
costs to run the EDS system nationwide. It considered costs incurred both by NatPharm and the
MOH. The model used a series of linked spreadsheets to describe the costs of different supply chain
components. For each component, key assumptions defined the level of effort and other inputs with
the average cost for each input. These costs were apportioned between the MOH and NatPharm;
and then compared to the estimate commodity value, volume, and, weight handled by the system.
EDS costs were estimated at each level in the system; they require assumptions both on the total
inputs required to operate the EDS and the average costs of those inputs. Costs incurred by both
NatPharm and the MOH were considered. At the central level, this required estimating the total
number of staff involved in the management functions at NatPharm headquarters, the Harare store,
and the MOH. Costs included management time, central storage costs, transportation to regional
stores; and other operational costs, including training, the LMIS, and office costs.
Data were collected from project sources and during meetings with individual stakeholder, who
validated key assumptions to guide the model construction. These assumptions were then discussed
and adjusted during a stakeholder workshop with counterparts from NatPharm and the MOHCW.
An agreement was reached on the number of facilities, staff required, time needed for different
functions, and commodities that could be handled. Agreement was also reached on supervision and
training needed to keep the EDS functional.
17At the Bulawayo and branch level, the inputs and costs of running each store are estimated. This
includes branch storage, picking and packing, and transport costs to the SDPs. Similarly, for SDPs
the average cost incurred at each type of SDP, including staffing and storage, are estimated. To
provide the total cost, these are multiplied by the total number of SDPs of each type. Assumptions
are made on the number of trips, average number of kilometers per trip, and the average cost per
kilometer. With NatPharm and the project office, the estimate of the quantity, value, volume, and
weight of the 44 drugs on the essential drug list (EDL), plus the 11 DTTU commodities, have been
determined.
Assumptions
Scenario 1—Bimonthly Delivery
Because it was not possible to visit every facility and province in Zimbabwe, the costing team had to
make several assumptions to simplify the analysis. The sample of facilities covered the two largest
cities in Zimbabwe; the two sampled provinces included Manicaland and Matabeleland South. The
team assumed that the Matabeleland South was representative of the other less-densely populated
provinces, which we were unable to visit. Although the team visited at least one of each of the more
numerous types of facility commonly found in Zimbabwe, private-for-profit facilities were not
included as part of the sample.
As noted, five of the scenarios being costed were hypothetical and many cost assumptions and
simplifying were required in order to model their costs. These are listed below.
Scenario 2—Quarterly Delivery
Scenario 2 estimates the cost of changing the delivery schedule from a bimonthly to a quarterly
schedule; key assumptions include those listed below:
When the quarterly schedule is introduced, it was assumed that no additional vehicles are
required to deliver the adequate quantity of commodities to each and all facilities. In practice,
this may not be true of Manicaland, which is a densely populated province that may require one
additional short journey to restock the delivery truck.
It is assumed that the additional commodities will not change the amount of time required to make
each delivery, at each site, in any significant manner. In practice, because the number of
commodities being counted will not change, and it may only take a few minutes longer to count the
extra units of each commodity.
No change was made to the useful life of each vehicle, although the overall mileage covered on a
quarterly schedule will decrease with the likely wear and tear of each vehicle. Although, on a
quarterly schedule the vehicles may be in a better condition at the end of five years, several of
them have already been used on a bimonthly schedule. Also, in accounting terms, the book life
of a vehicle follows standard accounting practice, typically a straight line depreciation over three
or four years, irrespective of the actual physical condition of the vehicle.
As the maintenance schedule and costs are determined by the mileage covered by a vehicle
(every 10,000 kilometers for the large delivery trucks), overall maintenance costs were reduced
by one third, which relates to the reduction in annual mileage that results from the change in
schedule.
18Scenario 3 and 4—Adding PHC Products to the DTTU, Quarterly Delivery
Scenario 3 estimates the cost associated with an increase in the number of commodities being
delivered by the DTTU system when 44 PHC commodities are added to the 11 already carried. This
scenario continues to use project salaries for project staff. Assumptions for scenario 3 include—
Four deliveries per annum are added to all the facilities served by the expanded DTTU system.
Additional replenishment miles each quarter to replenish stock in each district are required to
accommodate the addition of the 44 commodities into the expanded DTTU system. This
required—
three additional delivery trucks and three drivers
two additional monitoring and evaluation (M&E) vehicles for the two additional DPS staff
increase in costs for the maintenance, insurance, and tires for additional delivery and M&E
vehicles
per diem for the additional drivers and team leaders.
The total distance to deliver to each facility, not including the replenishment mileage, from
scenarios 1 and 2 remained the same.
The cost of storing six months of stock of PHC commodities at $6.00 per square meter per
month at NatPharm was assumed.
The time spent by staff to perform supply chain tasks at SDPs is doubled to reflect the addition
of the PHC commodities.
The logistics manager’s time for the LMIS function is increased from 30 percent from scenario 1
and 2 to full time.
Two additional data entry clerks are added, for a total of three clerks, to accommodate the
additional 44 commodities handled by the LMIS.
Assume that the PMTCT and RTK team would also quantify the PHC products, increasing their
time from 1.5 days per quarter to 5 days per quarter.
The area coordinators and deputy logistics advisor’s time remained the same.
Two additional Department of Pharmaceutical Services (DPS) logistics officers are added to
make supervision visits for five days every month. The current supervision schedule by four
logistics officers remained the same.
The estimated operating costs at the health facilities is increased from 0.5 percent to 1 percent to
account for the additional space the PHC commodities will occupy in each of the health
facilities.
An assumption of 100 percent of the storage space will be used for the 55 commodities at rural
heath centers, rural hospitals, and clinics; while 25 percent of the storage space will be used for
the 55 commodities at district, provincial, and central hospitals.
19You can also read