2022 Definition Updates - MTQIP
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

2022 Definition Updates
Key
Indicator Meaning
Yellow Highlight New change
Red Text Variability compared to NTDS
Strike Deleted verbiage
Vendor flag
Key
Indicator Meaning
Yellow Highlight New change
Red Text Variability compared to NTDS
Strike Deleted verbiage
Vendor flag
Key
Indicator Meaning
Yellow Highlight New change
Red Text Variability compared to NTDS
Strike Deleted verbiage
Vendor flagKey
Indicator Meaning
Yellow Highlight New change
Red Text Variability compared to NTDS
Strike Deleted verbiage
Vendor flagAdded to Additional Information: In-house traumatic injuries sustained
after ED/hospital arrival and before discharge at the index hospital (the
NTDS PATIENT INCLUSION CRITERIA
hospital reporting data), and all data associated with that injury event,
are excluded from NTDS Inclusion Criteria.
Rational – NTDS update
2021 2022
PATIENT INCLUSION CRITERIA PATIENT INCLUSION CRITERIA
Description Description
To ensure consistent data reporting across States into the National To ensure consistent data reporting across States into the National
Trauma Data Standard, a trauma patient is defined as a patient Trauma Data Standard, a trauma patient is defined as a patient
sustaining a traumatic injury within 14 days of initial hospital encounter sustaining a traumatic injury within 14 days of initial hospital encounter
and meeting the following criteria: and meeting the following criteria*:
Additional Information Additional Information
• ** Acute Care Hospital is defined as a hospital that provides • * In-house traumatic injuries sustained after ED/hospital arrival and
inpatient medical care and other related services for surgery, acute before discharge at the index hospital (the hospital reporting data),
medical conditions or injuries (usually for a short-term illness or and all data associated with that injury event, are excluded from
condition). NTDS Inclusion Criteria.
• Patients entered into the trauma registry will then be selected for • If an inpatient rehabilitation, geropsychiatry, or similar unit
analysis using TQIP and/or MTQIP inclusion and exclusion criteria. are separately licensed facilities from your hospital, then it’s
not considered an in-house trauma.
• If an inpatient rehabilitation, geropsychiatry, or similar unit
are part of the hospital (i.e., under the same license), then it
would qualify as an in-house trauma.
• ** Acute Care Hospital is defined as a hospital that provides
inpatient medical care and other related services for surgery, acute
medical conditions or injuries (usually for a short-term illness or
condition).
• Patients entered into the trauma registry will then be selected for
analysis using ACS TQIP and/or MTQIP inclusion and exclusion
criteria.ALL ELEMENTS Definition changed to Description. Rational – NTDS update 2021 2022 CASE NUMBER CASE NUMBER Definition Description Registry number from commercial registry software. Registry number from commercial registry software. Element Values Element Values • Relevant value for data element. • Relevant value for data element. Additional Information Additional Information • This number is automatically assigned by the registry program. • This number is automatically assigned by the registry program. • We will use only the initial admission (xxxxxx.000) record. • We will use only the initial admission (xxxxxx.000) record. Resources Resources Codebook Codebook Source: MTQIP Source: MTQIP Data Base Column Name: TRAUMA_NUM Data Base Column Name: TRAUMA_NUM Type of Element: Numeric Type of Element: Numeric Length: 30 Length: 30 Report: #1-8 Report: #1-8
Added to Additional Information: Reporting of null values and
EMS PATIENT CARE REPORT UNIVERSALLY UNIQUE IDENTIFIER (UUID)
information on NEMSIS technology.
Rational – NTDS update
2021 2022
EMS PATIENT CARE REPORT UNIQUE IDENTIFIER (UUID) EMS PATIENT CARE REPORT UNIQUE IDENTIFIER (UUID)
Description Description
The patient’s universally unique identifier (UUID) as assigned by the The patient’s universally unique identifier (UUID) as assigned by the
emergency medical service (EMS) agency transporting the patient emergency medical service (EMS) agency transporting the patient
from the scene of injury to your hospital. from the scene of injury to your hospital.
Additional Information Additional Information
• A sample UUID is: e48cd734-01cc-4da4-ae6a-915b0b1290f6 • A sample UUID is: e48cd734-01cc-4da4-ae6a-915b0b1290f6
• Consistent with NEMSIS v3.5.0. • Automated abstraction technology provided by registry product
• Assigned by the transporting EMS agency in accordance with the providers/vendors must be used for this data element. In the
IETF RFC 4122 standard. absence of automated technology, report the null value "Not
• The null value “Not Applicable” must be reported for all patients Known/Not Recorded.”
where Interfacility Transfer is Element Value “1. Yes”. • Consistent with NEMSIS v3.5.0.
• The null value “Not Known/Not Recorded” should be reported if the • The null value "Not Known/Not Recorded" must be reported if the
UUID is not documented on the EMS Run Report or if the EMS UUID is not documented on the EMS Run Report. The UUID will not be
provider is not NEMSIS v3.5.0 compliant. documented on EMS Run Reports until NEMSIS version 3.5.0 is
• The null value “Not Applicable” must be reported for all patients released. In collaboration with NEMSIS, the ACS will communicate
where Transport Mode is Element Values “4. Private/Public when NEMSIS 3.5.0 is released.
Vehicle/Walk-in”, “5. Police”, “6. Other” or if patient is not • Assigned by the transporting EMS agency in accordance with the
transported from the scene of injury by EMS. IETF RFC 4122 standard.
• For patients with multiple modes of transport from the scene of injury, • The null value “Not Applicable” must be reported for all patients
report the UUID assigned by the EMS agency that delivered the where Interfacility Transfer is Element Value “1. Yes”.
patient to your hospital. • The null value “Not Applicable” must be reported for all patients
where Transport Mode is Element Values “4. Private/Public
Vehicle/Walk-in”, “5. Police”, “6. Other.”
• For patients with multiple modes of transport from the scene of injury,
report the UUID assigned by the EMS agency that delivered the
patient to your hospital.
• If Transport Mode is Element Value "1. Ground Ambulance", "2.
Helicopter Ambulance" or "3. Fixed Wing Ambulance" but the
patient was not transported from the scene of injury, report the null
value "Not Known/Not Recorded."Added to Diagnostic & Therapeutic Imaging: Diagnostic imaging
ICD-10 HOSPITAL PROCEDURES interventions on the total body, Plain radiography of whole body, and
Plain radiography of whole skeleton.
Rational – NTDS update
2021 2022
ICD-10 HOSPITAL PROCEDURES ICD-10 HOSPITAL PROCEDURES
Description Description
Operative and selected non-operative procedures conducted during Operative and selected non-operative procedures conducted during
hospital stay. Operative and selected non-operative procedures are hospital stay. Operative and selected non-operative procedures are
those that were essential to the diagnosis, stabilization, or treatment of those that were essential to the diagnosis, stabilization, or treatment of
the patient’s specific injuries or complications. The list of procedures the patient’s specific injuries or complications. The list of procedures
below should be used as a guide to desired non-operative procedures below should be used as a guide to desired non-operative procedures
that should be provided to NTDB. that should be provided to NTDB.
Diagnostic & Therapeutic Imaging Diagnostic & Therapeutic Imaging
Computerized tomographic Head *, †, ‡ Computerized tomographic Head *, †, ‡
Computerized tomographic Brain *, †, ‡ Computerized tomographic Brain *, †, ‡
Computerized tomographic Chest * Computerized tomographic Chest *
Computerized tomographic Abdomen * Computerized tomographic Abdomen *
Computerized tomographic Pelvis * Computerized tomographic Pelvis *
Computerized tomographic C-Spine * Computerized tomographic C-Spine *
Computerized tomographic T-Spine * Computerized tomographic T-Spine *
Computerized tomographic L-Spine * Computerized tomographic L-Spine *
Diagnostic ultrasound (includes FAST) * Doppler ultrasound of extremities *
Doppler ultrasound of extremities * Diagnostic ultrasound (includes FAST) *
Angiography Angioembolization
Angioembolization Angiography
IVC filter *, † IVC filter *, †
REBOA REBOA
Diagnostic imaging interventions on the total body
Plain radiography of whole body
Plain radiography of whole skeletonChanged description to: The patient had a written request to limit life-
sustaining treatment that restricted the care for the patient during this
patient care event. Clarified Additional Information to: The written
ADVANCED DIRECTIVE LIMITING CARE request was signed or dated prior to arrival. Added to Additional
Information: Report Element Value "2. No" for patients with Advanced
Directives that did not limit life-sustaining treatments during this patient
care event.
Rational – NTDS update
2021 2022
ADVANCE DIRECTIVE LIMITING CARE ADVANCE DIRECTIVE LIMITING CARE
Description Description
The patient had a written request limiting life sustaining therapy, or The patient had a written request to limit life-sustaining treatment that
similar advance directive. restricted the scope of care for the patient during the patient care
event.
Element Values
Advance Directive Limiting Care (NTDS 13) Element Values
Advance Directive Limiting Care (NTDS 13)
Additional Information
• Present prior to arrival at your center. Additional Information
• The verbiage “present prior to arrival at your center” is not limited to • The written request was signed or dated by the patient and/or
documentation in hand or scanned from a previous admission. his/her designee prior to arrival at your center.
“Present prior to arrival at your center” is defined as the medical • Do not report for patients with Advanced Directives that did not limit
record indicates the patient has an advanced directive that limits life-sustaining treatments during this patient care event.
care completed prior to arrival at your center. • The verbiage “prior to arrival at your center” is not limited to
• This includes documentation that indicates to withhold life sustaining documentation in hand or scanned from a previous admission.
measures when a specified set of parameters are present (i.e., a “prior to arrival at your center” is defined as the medical record
documentation indicating to withhold life sustaining measures if a indicates the patient has an advanced directive that limits care
persistent vegetative state or other circumstances occur). completed prior to arrival at your center.
Resources Resources
Codebook Codebook
Source: NTDS Source: NTDS
Data Base Column Name: A_COMORCODE Data Base Column Name: A_COMORCODE
Type of Element: String Type of Element: String
Length: Length:
Report: #4 Report: #4Added to Additional Information: A diagnosis of angina including
microvascular angina, Prinzmetal's angina, stable angina, unstable
ANGINA PECTORIS
angina and variant angina, must be documented in the patient's
medical record.
Rational – NTDS update
2021 2022
ANGINA PECTORIS ANGINA PECTORIS
Description Description
Chest pain or discomfort due to coronary heart disease. Usually causes Chest pain or discomfort due to coronary heart disease. Usually causes
uncomfortable pressure, fullness, squeezing or pain in the center of the uncomfortable pressure, fullness, squeezing or pain in the center of the
chest. Patient may also feel the discomfort in the neck, jaw, shoulder, chest. Patient may also feel the discomfort in the neck, jaw, shoulder,
back or arm. Symptoms may be different in women than men. back or arm. Symptoms may be different in women than men.
Element Values Element Values
• Angina Pectoris (NTDS 32) • Angina Pectoris (NTDS 32)
Additional Information Additional Information
• Present prior to injury. • Present prior to injury.
• A diagnosis of angina including microvascular angina, Prinzmetal’s
Resources angina, stable angina, unstable angina, and variant angina must be
documented in the patient’s medical record.
Codebook
Source: AHA, NTDS Resources
Data Base Column Name: A_COMORCODE
Type of Element: String Codebook
Length: Source: AHA, NTDS
Report: #4 Data Base Column Name: A_COMORCODE
Type of Element: String
Length:
Report: #4Added to Additional Information: Only report on patients ≤18 years-of-
CONGENITAL ANOMALIES age. Added to Additional Information: The null value "Not Applicable"
must be reported for patients > 18-years-of-age.
Rational – NTDS update
2021 2022
CONGENITAL ANOMALIES CONGENITAL ANOMALIES
Description Description
Documentation of a cardiac, pulmonary, body wall, CNS/spinal, GI, Documentation of a cardiac, pulmonary, body wall, CNS/spinal, GI,
renal, orthopedic, or metabolic congenital anomaly. renal, orthopedic, or metabolic congenital anomaly.
Element Values Element Values
• Congenital Anomalies (NTDS 6) • Congenital Anomalies (NTDS 6)
Additional Information Additional Information
• Present prior to injury. • Present prior to injury.
• Include anomalies that have been operatively fixed prior to injury. • Only report on patients < 18 years-of-age.
• Include anomalies that have been operatively fixed prior to injury.
Resources • The null value “Not Applicable” must be reported for patients > 18
years-of-age.
Codebook
Source: NTDS Resources
Data Base Column Name: A_COMORCODE
Type of Element: String Codebook
Length: Source: NTDS
Report: #4 Data Base Column Name: A_COMORCODE
Type of Element: String
Length:
Report: #4Changed description to "Cancer that has spread to one or more sites in
addition to the primary site AND in the presence of multiple metastases
indicates the cancer is widespread, fulminant, or near terminal.”
DISSEMINATED CANCER Changed additional information to ” Another term describing
disseminated cancer is “metastatic cancer.” Changed additional
information to A diagnosis of cancer that has spread to one or more
sites must be documented in the patient’s medical record.
Rational – NTDS update
2021 2022
DISSEMINATED CANCER DISSEMINATED CANCER
Description Description
Patients who have cancer that has spread to one site or more sites in Cancer that has spread to one or more sites in addition to the primary
addition to the primary site and in whom the presence of multiple site and in the presence of multiple metastases indicates the cancer is
metastases indicates the cancer is widespread, fulminant, or near widespread, fulminant, or near terminal.
terminal.
Element Values
Element Values • Disseminated Cancer (NTDS 12)
• Disseminated Cancer (NTDS 12)
Additional Information
Additional Information • Present prior to injury.
• Present prior to injury. • Another term describing disseminated cancer is “metastatic
• Other terms describing disseminated cancer include "diffuse," cancer.”
"widely metastatic," "widespread," "carcinomatosis.” • A diagnosis of cancer that has spread to one or more sites must be
• Common sites of metastases include major organs (e.g., brain, lung, documented in the patient’s medical record.
liver, meninges, abdomen, peritoneum, pleura, bone). • Report Acute Lymphocytic Leukemia (ALL), Acute Myelogenous
• Report Acute Lymphocytic Leukemia (ALL), Acute Myelogenous Leukemia (AML), and Stage IV Lymphoma under this variable.
Leukemia (AML), and Stage IV Lymphoma under this variable. • Do not report Chronic Lymphocytic Leukemia (CLL), Chronic
• Do not report Chronic Lymphocytic Leukemia (CLL), Chronic Myelogenous Leukemia (CML), Stages I through III Lymphoma, or
Myelogenous Leukemia (CML), Stages I through III Lymphoma, or Multiple Myeloma as disseminated cancer.
Multiple Myeloma as disseminated cancer.
Resources
Resources Examples
Examples
Codebook
Codebook Source: NSQIP, NTDS
Source: NSQIP, NTDS Data Base Column Name: A_COMORCODE
Data Base Column Name: A_COMORCODE Type of Element: String
Type of Element: String Length:
Length: Report: #4
Report: #4Changed description to: History of persistent elevated blood pressure
HYPERTENSION
requiring antihypertensive medication.
Rational – NTDS update
2021 2022
HYPERTENSION HYPERTENSION
Description Description
History of a persistent elevated blood pressure requiring medical History of persistent elevated blood pressure requiring antihypertensive
therapy with antihypertensive medication. medication.
Element Values Element Values
• Hypertension (NTDS 19) • Hypertension (NTDS 19)
Additional Information Additional Information
• Present prior to injury. • Present prior to injury.
• A diagnosis of Hypertension must be documented in the patient's • A diagnosis of Hypertension must be documented in the patient's
medical record. medical record.
• Exclude if documentation reports medication noncompliance. • Exclude if documentation reports medication noncompliance.
• Exclude hypertension controlled only with diet or exercise. • Exclude hypertension controlled only with diet or exercise.
Resources Resources
• Drug search • Drug search
Codebook Codebook
Source: NTDS Source: NTDS
Data Base Column Name: A_COMORCODE Data Base Column Name: A_COMORCODE
Type of Element: String Type of Element: String
Length: Length:
Report: #4 Report: #4Changed description to: "Regular administration of oral or parenteral
STEROID USE corticosteroid medications within 30 days prior to injury for a chronic
medical condition."
Rational – NTDS update
2021 2022
STEROID USE STEROID USE
Description Description
Patients that required the regular administration of oral or parenteral Regular administration of oral or parenteral corticosteroid medications
corticosteroid medications within 30 days prior to injury for a chronic within 30 days prior to injury for a chronic medical condition.
medical condition.
Element Values
Element Values • Steroid Use (NTDS 24)
• Steroid Use (NTDS 24)
Additional Information
Additional Information • Examples of oral or parenteral corticosteroid medications are
• Examples of oral or parenteral corticosteroid medications are prednisone and dexamethasone.
prednisone and dexamethasone. • Examples of chronic medical conditions are Chronic Obstructive
• Examples of chronic medical conditions are COPD, asthma, Pulmonary Disease (COPD), asthma, rheumatologic disease,
rheumatologic disease, rheumatoid arthritis, inflammatory bowel rheumatoid arthritis, inflammatory bowel disease.
disease. • Exclude topical corticosteroids applied to the skin or corticosteroids
• Exclude topical corticosteroids applied to the skin or corticosteroids administered by inhalation or rectally.
administered by inhalation or rectally.
Resources
Resources • Drug search
• Drug search
Codebook
Codebook Source: NSQIP, NTDS
Source: NSQIP, NTDS Data Base Column Name: A_COMORCODE
Data Base Column Name: A_COMORCODE Type of Element: String
Type of Element: String Length:
Length: Report: #4
Report: #4Removed from Description: Must have occurred during the patient's
HOSPITAL EVENTS - INTRODUCTION initial stay at your hospital. Added to Additional Information: Onset of
symptoms began after arrival to your ED/hospital.
Rational – NTDS update
2021 2022
INTRODUCTION INTRODUCTION
Description Description
Any medical complication that occurred during the patient's stay at Any medical complication that occurred.
your hospital.
Element Values
Element Values Relevant value for data element.
Relevant value for data element.
Additional Information
Additional Information • Onset of symptoms began after arrival to your ED/hospital.
• The patient's stay begins on arrival to the emergency department. • Do not include reported complications that are present prior to
• Do not include reported complications that are present prior to arrival. For example, a patient arrives with a urinary tract infection as
arrival. For example, a patient arrives with a urinary tract infection as indicated by symptoms present in documentation obtained on
indicated by symptoms present in documentation obtained on arrival and a culture obtained on arrival.
arrival and a culture obtained on arrival. • Do not report contaminants that did not require treatment for
• Do not report contaminants that did not require treatment for infectious events. For example, a patient has a BAL or blood culture
infectious events. For example, a patient has a BAL or blood culture that demonstrates contaminant and therapy is not provided. If a
that demonstrates contaminant and therapy is not provided. If a provider documents a contaminant, but treatment is provided the
provider documents a contaminant, but treatment is provided the event is reported.
event is reported. • For hospitals with an inpatient hospice service/unit without transition
• For hospitals with an inpatient hospice service/unit without transition indicators in the EMR (e.g., new encounter/visit number, discharge
indicators in the EMR (e.g., new encounter/visit number, discharge order, discharge summary, new admit order, new hospice service
order, discharge summary, new admit order, new hospice service assignment, new hospice specific attending provider, etc.) to signal
assignment, new hospice specific attending provider, etc.) to signal the end of the patient’s stay, the end of stay occurs when the acute
the end of the patient’s stay, the end of stay occurs when the acute phase of care ends. This does not include comfort care status
phase of care ends. This does not include comfort care status during the acute phase of care or transfer to medicine services
during the acute phase of care or transfer to medicine services during the acute phase of care.
during the acute phase of care. • The null value "Not Applicable" should be used for patients with no
• The null value "Not Applicable" should be used for patients with no complications.
complications.
Resources
Resources
Codebook
Codebook Source: NTDS
Source: NTDS Data Base Column Name: Not applicable
Data Base Column Name: Not applicable Type of Element: Not applicable
Type of Element: Not applicable Length: Not applicable
Length: Not applicable Report: #6
Report: #6Added to Additional Information: "EXCLUDE: Patients with a planned
UNPLANNED ADMISSION TO ICU ICU stay post-operative. INCLUDE: patients who required ICU care due
to an event that occurred during surgery or in the PACU."
Rational – NTDS update
2021 2022
UNPLANNED ADMISSION TO ICU UNPLANNED ADMISSION TO ICU
Description Description
Patients admitted to the ICU after initial transfer to the floor, and/or Patients admitted to the ICU after initial transfer to the floor, and/or
patients with an unplanned return to the ICU after initial ICU discharge. patients with an unplanned return to the ICU after initial ICU discharge.
Element Values Element Values
Unplanned Admission to ICU (NTDS 31) Unplanned Admission to ICU (NTDS 31)
Additional Information Additional Information
• Exclude patients in which ICU care was required for postoperative • Exclude patients with a planned post-operative ICU stay.
care of a planned surgical procedure. • Include patients who required ICU care due to an event that
• Include patients who deteriorate in the post-anesthesia care unit occurred during surgery or in the PACU.
(PACU) or intra-operatively with new resultant requirement for ICU
admission. Resources
Resources Codebook
Source: NTDS
Codebook Data Base Column Name: A_TCODE, A_TCODE_AS_TEXT
Source: NTDS Type of Element: String
Data Base Column Name: A_TCODE, A_TCODE_AS_TEXT Length:
Type of Element: String Report: #6
Length:
Report: #6UNPLANNED VISIT TO THE OPERATING ROOM Added exclusion of: Non-urgent tracheostomy and gastrostomy tube.
Rational – NTDS update
2021 2022
UNPLANNED VISIT TO THE OPERATING ROOM UNPLANNED VISIT TO THE OPERATING ROOM
Description Description
Patients with an unplanned operative procedure OR patients returned Patients with an unplanned operative procedure OR patients returned
to the operating room after initial operation management of a related to the operating room after initial operation management of a related
previous procedure. previous procedure.
Element Values Element Values
• Unplanned Visit to OR (NTDS 40) • Unplanned Visit to OR (NTDS 40)
Additional Information Additional Information
• Unplanned is defined as an acute clinical deterioration requiring • Unplanned is defined as an acute clinical deterioration requiring
operative intervention. operative intervention.
• Exclude pre-planned, staged and/or procedures for incidental • Exclude non-urgent tracheostomy and gastrostomy tube.
findings. • Exclude pre-planned, staged and/or procedures for incidental
• Exclude operative management related to a procedure that was findings.
initially performed prior to arrival at your center. • Exclude operative management related to a procedure that was
• Example 1: Patient is having difficulty weaning for the ventilator. initially performed prior to arrival at your center.
Patient is scheduled and undergoes a tracheostomy. Do not report • Example 1: Patient is having difficulty weaning for the ventilator.
as an Unplanned Visit to the Operating Room. Patient is scheduled and undergoes a tracheostomy. Do not report
• Example 2: Patient has an acute loss of airway requiring emergent as an Unplanned Visit to the Operating Room.
tracheostomy in the OR for airway establishment. Report an • Example 2: Patient has an acute loss of airway requiring emergent
Unplanned Visit to the Operating Room. tracheostomy in the OR for airway establishment. Report an
Unplanned Visit to the Operating Room.
Resources
Resources
Codebook
Source: NTDS Codebook
Data Base Column Name: A_TCODE, A_TCODE_AS_TEXT Source: NTDS
Type of Element: String Data Base Column Name: A_TCODE, A_TCODE_AS_TEXT
Length: Type of Element: String
Report: #6 Length:
Report: #6Added to Additional Information: Element Value "5. None" is reported
VENOUS THROMBOEMBOLISM PROPHYLAXIS TYPE
for patients who refuse VTE prophylaxis.
Rational – NTDS update
2021 2022
VENOUS THROMBOEMBOLISM PROPHYLAXIS TYPE VENOUS THROMBOEMBOLISM PROPHYLAXIS TYPE
Description Description
Type of first dose of venous thromboembolism prophylaxis or treatment Type of first dose of venous thromboembolism prophylaxis or treatment
administered to patient at your hospital. administered to patient at your hospital.
Additional Information Additional Information
• Must be administered, not just ordered. • Must be administered, not just ordered.
• Report heparin, LMWH, direct thrombin inhibitor and Xa inhibitor • Element Value “5. None” is reported if the patient refuses venous
class agents regardless of the indication when it is administered first. thromboembolism prophylaxis.
• Report Coumadin and ‘other’ agents when the indication of VTE • Report heparin, LMWH, direct thrombin inhibitor and Xa inhibitor
prevention is identified in the medical record documentation. class agents regardless of the indication when it is administered first.
• Exclude non-prophylactic dosing of agents, such as heparin • Report Coumadin and ‘other’ agents when the indication of VTE
administered for line clearance purposes. prevention is identified in the medical record documentation.
• Use drug search for agents and dosing outside these parameters to • Exclude non-prophylactic dosing of agents, such as heparin
determine class and/or indicated use. administered for line clearance purposes.
• Venous Thromboembolism Prophylaxis Types which were retired • Use drug search for agents and dosing outside these parameters to
greater than 2 years before the current NTDS version are no longer determine class and/or indicated use.
listed under Element Values above, which is why there are • Venous Thromboembolism Prophylaxis Types which were retired
numbering gaps. Refer to the NTDS Change Log for a full list of greater than 2 years before the current NTDS version are no longer
retired Venous Thromboembolism Prophylaxis Types. listed under Element Values above, which is why there are
• Exclude sequential compression devices. numbering gaps. Refer to the NTDS Change Log for a full list of
retired Venous Thromboembolism Prophylaxis Types.
• Exclude sequential compression devices.PATIENT’S FIRST NAME Clarification to report the legal name of the patient.
Rational – MTQIP Member request
2021 2022
PATIENT’S FIRST NAME PATIENT’S FIRST NAME
Description Description
The first name of the patient. The first name of the patient.
Element Values Element Values
• Relevant value for data element. • Relevant value for data element.
Additional Information Additional Information
• Report the legal name provided by the patient.
Resources
Resources
Codebook
Source: MTQIP Codebook
Data Base Column Name: PAT_NAME_F Source: MTQIP
Type of Element: String Data Base Column Name: PAT_NAME_F
Length: Type of Element: String
Report: #1 Length:
Report: #1PATIENT’S LAST NAME Clarification to report the legal name of the patient.
Rational – MTQIP Member request
2021 2022
PATIENT’S LAST NAME PATIENT’S LAST NAME
Description Description
The last name of the patient. The last name of the patient.
Element Values Element Values
• Relevant value for data element. • Relevant value for data element.
Additional Information Additional Information
• Report the legal name provided by the patient, including suffix if
Resources applicable.
Codebook Resources
Source: MTQIP
Data Base Column Name: PAT_NAME_L Codebook
Type of Element: String Source: MTQIP
Length: Data Base Column Name: PAT_NAME_L
Report: #1 Type of Element: String
Length:
Report: #1PATIENT’S MIDDLE INITIAL Clarification to report the legal initial of the patient.
Rational – MTQIP Member request
2021 2022
PATIENT’S MIDDLE INITIAL PATIENT’S MIDDLE INITIAL
Description Description
The first name of the patient. The first name of the patient.
Element Values Element Values
• Relevant value for data element. • Relevant value for data element.
Additional Information Additional Information
• Report the legal name first initial provided by the patient.
Resources
Resources
Codebook
Source: MTQIP Codebook
Data Base Column Name: PAT_NAME_MI Source: MTQIP
Type of Element: String Data Base Column Name: PAT_NAME_MI
Length: Type of Element: String
Report: #1 Length:
Report: #1Clarified reporting as the final level of ED care documented. Clarified
ED TRAUMA RESPONSE
reporting of patients directly admitted to the hospital.
Rational – MTQIP validation feedback
2021 2022
ED TRAUMA RESPONSE ED TRAUMA RESPONSE
Description Description
Enter the final level of response being provided to the patient in the The final level of response listed on the trauma flowsheet or similar
Emergency Department (ED) by trauma. documentation.
Element Values Element Values
1. Full activation 1. Full activation
2. Partial activation 2. Partial activation
3. Trauma consult 3. Trauma consult
4. None 4. None
Additional Information Additional Information
• Trauma is called by the ED to see a patient in the ED and a provider • Trauma is called by the ED to see a patient, report as consult.
from the service sees the patient, report as consult. • Patient arrives as a full activation, but is downgraded to a partial
• Patient arrives as a full activation, but is downgraded to a partial activation, report as a partial activation.
activation, report as a partial activation. • Patient arrives as partial activation, but is upgraded to a full
• Patient arrives as partial activation, but is upgraded to a full activation, report as a full activation.
activation, report as a full activation. • Include patients with an order entered. For example, an ED provider
• Include patients with an order entered. For example, an ED provider enters a consult order for trauma consultation, report as trauma
enters a consult order for trauma consultation, report as trauma consult.
consult. • Report direct admits (e.g., no ED care provision) as 4. None.
Resources Resources
Codebook Codebook
Source: MTQIP Source: MTQIP
Data Base Column Name: ED_TTA_TYPE, ED_TTA_TYPE_AS_TEXT Data Base Column Name: ED_TTA_TYPE, ED_TTA_TYPE_AS_TEXT
Type of Element: Numeric, String Type of Element: Numeric, String
Length: 1,8 Length: 1,8
Report: #1 Report: #1Corrected logic error. Null value vendor mapping requested in 2021
TRAUMA SURGEON ARRIVAL TIME
updates.
Rational – MTQIP Member request
2021 2022
TRAUMA SURGEON ARRIVAL TIME TRAUMA SURGEON ARRIVAL TIME
Description Description
The time the first trauma surgeon arrived at the patient’s bedside. The time the first trauma surgeon arrived at the patient’s bedside.
Element Values Element Values
• Relevant value for data element. • Relevant value for data element.
Additional Information Additional Information
• Collected as HHMM military time. • Collected as HHMM military time.
• Limit reporting to the 24 hours after ED/Hospital arrival. • Limit reporting to the 24 hours after ED/Hospital arrival.
• The trauma surgeon leads the trauma team and is responsible for • The trauma surgeon leads the trauma team and is responsible for
the overall care of trauma patient, including coordinating care with the overall care of trauma patient, including coordinating care with
other specialties and maintaining continuity of care. other specialties and maintaining continuity of care.
• The null value “Not Applicable” is reported for those patients who • The null value “Not Applicable” is reported for those patients who
were not evaluated by a trauma surgeon within 24 hours of were not evaluated by a trauma surgeon within 24 hours of
ED/Hospital arrival. ED/Hospital arrival.
• The null value “Not Applicable” is reported if the data element • Report for all full and partial activations. Trauma center discretion
Highest Activation is reported as Element Value “2. No.” for consults.
• Report for all full and partial activations. Trauma center discretion
for consults. Resources
Resources Codebook
Source: NTDS
Codebook Data Base Column Name: EDP_A_TIME01
Source: NTDS Type of Element: Time (HH:MM Format)
Data Base Column Name: EDP_A_TIME01 Length:
Type of Element: Time (HH:MM Format) Report: #1
Length: Vendor mapping: Map partial activations to null value “Not
Report: #1 Applicable” for NTDS submission.
Vendor mapping: Map partial activations to null value “Not
Applicable” for NTDS submission.INITIAL ED/HOSPITAL GCS-EYE Clarified inclusion of the word “alert” for reporting as GCS – Eye of 4. Rational – MTQIP Member request 2021 2022 INITIAL ED/HOSPITAL GCS-EYE INITIAL ED/HOSPITAL GCS-EYE Description Description First recorded Glasgow Coma Score (Eye) in the ED/hospital within 30 First recorded Glasgow Coma Score (Eye) in the ED/hospital within 30 minutes or less of ED/hospital arrival. minutes or less of ED/hospital arrival. Element Values Element Values 1. No eye movement when assessed 1. No eye movement when assessed 2. Opens eyes in response to painful stimulation 2. Opens eyes in response to painful stimulation 3. Opens eyes in response to verbal stimulation 3. Opens eyes in response to verbal stimulation 4. Opens eyes spontaneously 4. Opens eyes spontaneously Additional Information Additional Information • If a patient does not have a numeric GCS score recorded, but • If a patient does not have a numeric GCS score recorded, but written documentation closely (or directly) relates to verbiage written documentation closely (or directly) relates to verbiage describing a specific level of functioning within the GCS scale, the describing a specific level of functioning within the GCS scale, the appropriate numeric score may be listed. E.g., the chart indicates: appropriate numeric score may be listed. E.g., the chart indicates: "opens eyes spontaneously," an Eye GCS of 4 may be recorded, IF "opens eyes spontaneously,” or “alert,” an Eye GCS of 4 may be there is no other contradicting documentation. recorded, IF there is no other contradicting documentation. • Please note that first recorded/hospital vitals do not need to be from • Please note that first recorded/hospital vitals do not need to be from the same assessment. the same assessment. • The provider evaluation time, staff arrived time, and similar • The provider evaluation time, staff arrived time, and similar assessment time should be used when the specified provider’s note assessment time should be used when the specified provider’s note documents this assessment. documents this assessment. • The null value “Not Known/Not Recorded” is reported if Initial • The null value “Not Known/Not Recorded” is reported if Initial ED/Hospital GCS 40 – Eye is documented. ED/Hospital GCS 40 – Eye is documented. • The null value “Not Known/Not Recorded” is reported if the patient’s • The null value “Not Known/Not Recorded” is reported if the patient’s Initial ED/Hospital GCS - Eye was not measured within 30 minutes or Initial ED/Hospital GCS - Eye was not measured within 30 minutes or less of ED/hospital arrival. less of ED/hospital arrival. • If the patient has a cardiopulmonary arrest prior to arrival or within 15 • If the patient has a cardiopulmonary arrest prior to arrival or within 15 minutes of arrival, and no GCS is ever able to be obtained then minutes of arrival, and no GCS is ever able to be obtained then report this GCS variable as 1. report this GCS variable as 1.
INITIAL ED/HOSPITAL GCS-EYE Clarified inclusion of the word “alert” for reporting as GCS 40 – Eye of 4.
Rational – MTQIP Member request
2021 2022
INITIAL ED/HOSPITAL GCS 40 – EYE INITIAL ED/HOSPITAL GCS 40 – EYE
Description Description
First recorded Glasgow Coma Score 40 (Eye) in the ED/hospital within First recorded Glasgow Coma Score 40 (Eye) in the ED/hospital within
30 minutes or less of ED/hospital arrival. 30 minutes or less of ED/hospital arrival.
Element Values Element Values
0. Not Testable 0. Not Testable
1. None 1. None
2. To Pressure 2. To Pressure
3. To Sound 3. To Sound
4. Spontaneous 4. Spontaneous
Additional Information Additional Information
• If a patient does not have a numeric GCS score recorded, but • If a patient does not have a numeric GCS score recorded, but
written documentation closely (or directly) relates to verbiage written documentation closely (or directly) relates to verbiage
describing a specific level of functioning within the GCS 40 scale, describing a specific level of functioning within the GCS 40 scale,
the appropriate numeric score may be listed. E.g., the chart the appropriate numeric score may be listed. E.g., the chart
indicates: "patient's eyes open spontaneously," an Eye GCS 40 of 4 indicates: "patient's eyes open spontaneously” or “alert” an Eye GCS
may be recorded, IF there is no other contradicting documentation. 40 of 4 may be recorded, IF there is no other contradicting
• Report Element Value “0. Not Testable” if unable to assess (e.g., documentation.
swelling to eye(s)). • Report Element Value “0. Not Testable” if unable to assess (e.g.,
• The provider evaluation time, staff arrived time, and similar swelling to eye(s)).
assessment time should be used when the specified provider’s note • The provider evaluation time, staff arrived time, and similar
documents this assessment. assessment time should be used when the specified provider’s note
• The null value “Not Known/Not Recorded” is reported if Initial Field documents this assessment.
GCS – Eye is reported. • The null value “Not Known/Not Recorded” is reported if Initial Field
• The null value “Not Known/Not Recorded” is reported if the patient’s GCS – Eye is reported.
Initial ED/Hospital GCS 40- Eye was not measured within 30 minutes • The null value “Not Known/Not Recorded” is reported if the patient’s
or less of ED/hospital arrival. Initial ED/Hospital GCS 40- Eye was not measured within 30 minutes
or less of ED/hospital arrival.INTRODUCTION PRE-EXISTING CONDITIONS Clarified recommended data resources.
Rational – MTQIP Member request
2021 2022
INTRODUCTION INTRODUCTION
Description Description
Pre-existing co-morbid factors present before patient arrival at the Pre-existing co-morbid factors present before patient arrival at the
MTQIP ED/hospital. MTQIP ED/hospital.
Element Values Element Values
Relevant value for data element. Relevant value for data element.
Additional Information Additional Information
• The null value "Not Applicable" is used for patients with no known co- • The null value "Not Applicable" is used for patients with no known co-
morbid conditions. morbid conditions.
• Check all that apply. • Check all that apply.
• Comorbidities should be submitted using numeric or alpha-numeric • Comorbidities should be submitted using numeric or alpha-numeric
code under each variable. code under each variable.
• Recommended data resources for reporting include but are not
Resources limited to electronic medical record (EMR), emergency medical
Codebook services (EMS) run sheet, and Care Everywhere.
Source: NTDS, MTQIP
Data Base Column Name: A_COMORCODE Resources
Type of Element: String Codebook
Length: Source: NTDS, MTQIP
Report: #4 Data Base Column Name: A_COMORCODE
Type of Element: String
Length:
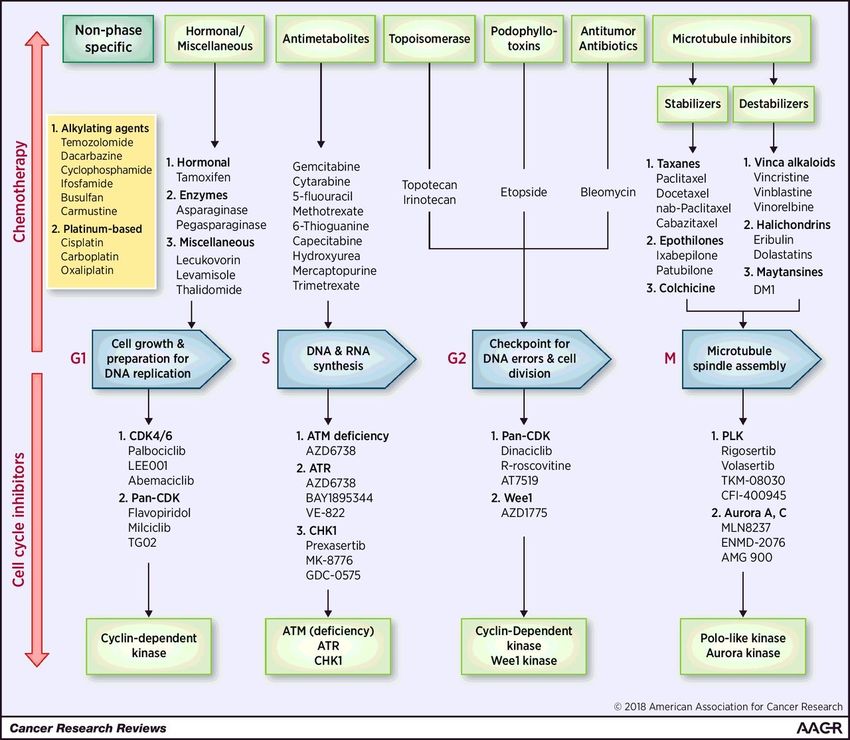
Report: #4Clarified the exclusion of cell cycle inhibitors and added an infographic
CHEMOTHERAPY FOR CANCER
hyperlinked resource.
Rational – MTQIP Member request
2021 2022
CHEMOTHERAPY FOR CANCER CHEMOTHERAPY FOR CANCER
Description Description
A patient who is currently receiving chemotherapy treatment for A patient who is currently receiving chemotherapy treatment for
cancer. cancer.
Element Values Element Values
Chemotherapy for Cancer (NTDS 5) Chemotherapy for Cancer (NTDS 5)
Additional Information Additional Information
• Prior to injury. • Prior to injury.
• Chemotherapy may include, but is not restricted to, oral and • Chemotherapy may include, but is not restricted to, oral and
parenteral treatment with chemotherapeutic agents for parenteral treatment with chemotherapeutic agents for
malignancies such as colon, breast, lung, head and neck, and malignancies such as colon, breast, lung, head and neck, and
gastrointestinal solid tumors as well as lymphatic and hematopoietic gastrointestinal solid tumors as well as lymphatic and hematopoietic
malignancies such as lymphomas, leukemia, and multiple myeloma. malignancies such as lymphomas, leukemia, and multiple myeloma.
• Exclude if treatment consists solely of hormonal therapy. • Exclude if treatment consists solely of hormonal therapy or cell cycle
inhibitors.
Resources
• Drug search Resources
• Drug search
Codebook • Therapy Types
Source: NTDS
Data Base Column Name: A_COMORCODE Codebook
Type of Element: String Source: NTDS
Length: Data Base Column Name: A_COMORCODE
Report: #4 Type of Element: String
Length:
Report: #4Therapies that target the cell cycle.
Christopher C. Mills et al. Cancer Res 2018;78:320-325
©2018 by American Association for Cancer ResearchClarified exclusion of disease processes not in the peripheral
PERIPHERAL ARTERIAL DISEASE (PAD)
vasculature.
Rational – MTQIP Member request
2021 2022
PERIPHERAL ARTERIAL DISEASE (PAD) PERIPHERAL ARTERIAL DISEASE (PAD)
Description Description
The narrowing or blockage of the vessels that carry blood from the The narrowing or blockage of the vessels that carry blood from the
heart to the legs, present prior to injury. It is primarily caused by the heart to the legs, present prior to injury. It is primarily caused by the
buildup of fatty plaque in the arteries, which is called atherosclerosis. buildup of fatty plaque in the arteries, which is called atherosclerosis.
Element Values Element Values
• Peripheral Arterial Disease (NTDS 35) • Peripheral Arterial Disease (NTDS 35)
Additional Information Additional Information
• PAD can occur in any blood vessel, but it is more common in the • PAD can occur in any blood vessel, but it is more common in the
legs than the arms. legs than the arms.
• Include peripheral vascular disease (PVD) which is used • Include peripheral vascular disease (PVD) which is used
interchangeably with PAD unless vein-only disease is specified. interchangeably with PAD unless vein-only disease is specified.
• Exclude disease processes not caused by atherosclerosis such as • Exclude disease processes not caused by atherosclerosis such as
Raynaud’s and Buerger’s disease. Raynaud’s and Buerger’s disease.
• Exclude disease processes not in the peripheral vasculature such as
Resources coronary artery disease.
Codebook Resources
Source: CDC, NTDS
Data Base Column Name: A_COMORCODE Codebook
Type of Element: String Source: CDC, NTDS
Length: Data Base Column Name: A_COMORCODE
Report: #4 Type of Element: String
Length:
Report: #4STROKE/CVA Clarified logic with use of circles.
Rational – MTQIP Member request, ACS TQIP clarification in algorithms
2021 2022
STROKE/CVA STROKE/CVA
Description Description
A focal or global neurological deficit of rapid onset and NOT present on admission. The patient A focal or global neurological deficit of rapid onset and NOT present on admission.
must have at least one of the following symptoms:
• Duration of neurological deficit ≥24 h
• Change in level of consciousness,
• Hemiplegia, AND
• Hemiparesis,
• Numbness or sensory loss affecting one side of the body, The patient must have at least one of the following symptoms:
• Dysphasia or aphasia,
• Hemianopia • Change in level of consciousness,
• Amaurosis fugax, • Hemiplegia,
• Or other neurological signs or symptoms consistent with stroke • Hemiparesis,
• Numbness or sensory loss affecting one side of the body,
AND • Dysphasia or aphasia,
• • Hemianopia
Duration of neurological deficit ≥24 h • Amaurosis fugax,
• Or other neurological signs or symptoms consistent with stroke
OR
• Duration of deficitUNPLANNED VISIT TO THE OPERATING ROOM Clarified with examples of events without acute clinical deterioration.
Rational – MTQIP Member request and z-score trending
2021 2022
UNPLANNED VISIT TO THE OPERATING ROOM UNPLANNED VISIT TO THE OPERATING ROOM
Description Description
Patients with an unplanned operative procedure OR patients returned Patients with an unplanned operative procedure OR patients returned
to the operating room after initial operation management of a related to the operating room after initial operation management of a related
previous procedure. previous procedure.
Element Values Element Values
• Unplanned Visit to OR (NTDS 40) • Unplanned Visit to OR (NTDS 40)
Additional Information Additional Information
• Unplanned is defined as an acute clinical deterioration requiring • Unplanned is defined as an acute clinical deterioration requiring
operative intervention. operative intervention.
• Exclude non-urgent tracheostomy and gastrostomy. • Exclude non-urgent tracheostomy and gastrostomy.
• Exclude pre-planned, staged and/or procedures for incidental • Exclude pre-planned, staged and/or procedures for incidental
findings. findings.
• Exclude operative management related to a procedure that was • Exclude operative management related to a procedure that was
initially performed prior to arrival at your center. initially performed prior to arrival at your center.
• Example 1: Patient is having difficulty weaning for the ventilator. • Inclusion Example
Patient is scheduled and undergoes a tracheostomy. Do not report • Patient has an acute loss of airway requiring emergent
as an Unplanned Visit to the Operating Room. tracheostomy in the OR for airway establishment.
• Example 2: Patient has an acute loss of airway requiring emergent • Exclusion Example
tracheostomy in the OR for airway establishment. Report an • Patient is having difficulty weaning for the ventilator. Patient
Unplanned Visit to the Operating Room. is scheduled and undergoes a tracheostomy.
• Patient is initially managed non-operatively for a fracture.
Pain control is unable to be achieved with non-operative
management. Patient is scheduled and undergoes an
ORIF.
• Patient is initially managed non-operatively for a fracture.
Post-ambulation imaging to confirm stability demonstrates
increased malalignment. Patient is scheduled and
undergoes an ORIF.HOSPITAL DISCHARGE DISPOSITION Clarified reporting of care/plan arranged at time of discharge. Rational – MTQIP validation feedback 2021 2022 HOSPITAL DISCHARGE DISPOSITION HOSPITAL DISCHARGE DISPOSITION Description Description The disposition of the patient when discharged from the hospital. The disposition of the patient when discharged from the hospital. Additional Information Additional Information • Element value = 6, "home" refers to the patient's current place of • Element value = 6, "home" refers to the patient's current place of residence (e.g., prison, Child Protective Services etc.). residence (e.g., prison, Child Protective Services etc.). • Element values based upon UB-04 disposition coding. • Element values based upon UB-04 disposition coding. • Disposition to any other non-medical facility should be coded as 6. • Disposition to any other non-medical facility should be coded as 6. • Disposition to any other medical facility should be coded as 14. • Disposition to any other medical facility should be coded as 14. • The null value "Not Applicable" is reported if ED Discharge Disposition • The null value "Not Applicable" is reported if ED Discharge Disposition = 5 (Deceased/expired). = 5 (Deceased/expired). • The null value "Not Applicable" is reported if ED Discharge Disposition • The null value "Not Applicable" is reported if ED Discharge Disposition = 4,6,9,10, or 11. = 4,6,9,10, or 11. • Hospital Discharge Dispositions which were retired greater than 2 • Hospital Discharge Dispositions which were retired greater than 2 years before the current NTDS version are no longer listed under years before the current NTDS version are no longer listed under Element Values above, which is why there are numbering gaps. Element Values above, which is why there are numbering gaps. Refer to the NTDS Change Log for a full list of retired Hospital Refer to the NTDS Change Log for a full list of retired Hospital Discharge Dispositions. Discharge Dispositions. • Report the actual disposition of the patient as arranged and • Report the actual disposition of the patient as arranged and documented by discharge planning or case management. If no documented by discharge planning or case management at time discharge planning or case management provided, report the final of discharge. If no discharge planning or case management disposition order. provided, report the final disposition order.
Clarified common documentation practices of a normal examination
INITIAL ED/HOSPITAL PUPILLARY RESPONSE
that correlate with reactive pupils.
Rational – MTQIP Member request
2021 2022
INITIAL ED/HOSPITAL PUPILLARY RESPONSE INITIAL ED/HOSPITAL PUPILLARY RESPONSE
Description Description
Physiological response of the pupil size within 30 minutes or less of Physiological response of the pupil size within 30 minutes or less of
ED/hospital arrival. ED/hospital arrival.
Element Values Element Values
1. Both Reactive 1. Both Reactive
2. One Reactive 2. One Reactive
3. Neither Reactive 3. Neither Reactive
Additional Information Additional Information
• Please note that the first recorded hospital vitals do not need to be • Please note that the first recorded hospital vitals do not need to be
from the same assessment. from the same assessment.
• The provider evaluation time, staff arrived time, and similar • The provider evaluation time, staff arrived time, and similar
assessment time should be used when the specified provider’s note assessment time should be used when the specified provider’s note
documents this assessment. documents this assessment.
• If a patient does not have a listed element value recorded, but • If a patient does not have a listed element value recorded, but
there is documentation related to their pupillary response such as there is documentation related to their pupillary response such as
PERRL “Pupils Equal Round Reactive to Light”, both cranial nerves II & PERRL “Pupils Equal Round Reactive to Light”, both cranial nerves II &
III intact, or no cranial nerve deficit submit element value 1. Both III intact, no cranial nerve deficit, no focal deficit, or neuro exam
reactive IF there is no other contradicting documentation. WNL submit element value 1. Both reactive IF there is no other
• Documentation of a “blown pupil” indicates a non-reactive pupil. contradicting documentation.
• The null value “Not Known/Not Recorded” should be reported if this • Documentation of a “blown pupil” indicates a non-reactive pupil.
information is not documented or if assessment is unable to be • The null value “Not Known/Not Recorded” should be reported if this
obtained due to facial trauma and/or foreign object in the eye. information is not documented or if assessment is unable to be
• Element value 2. One reactive should be reported for patients who obtained due to facial trauma and/or foreign object in the eye.
have a prosthetic eye. • Element value 2. One reactive should be reported for patients who
• The null value “Not Applicable” is reported for patients who do not have a prosthetic eye.
meet the reporting criterion. • The null value “Not Applicable” is reported for patients who do not
meet the reporting criterion.BETA BLOCKER TREATMENT Clarified the original intent of reporting after arrival to index hospital. Rational – MTQIP Member request 2021 2022 BETA BLOCKER TREATMENT BETA BLOCKER TREATMENT Reporting Criterion Reporting Criterion Report on patients with at least one injury in AIS head region, excluding Report on patients with at least one injury in AIS head region, excluding patients with isolated scalp abrasion(s), scalp contusion(s), scalp patients with isolated scalp abrasion(s), scalp contusion(s), scalp laceration(s) and/or scalp avulsion(s). Exclude injuries where the code laceration(s) and/or scalp avulsion(s). Exclude injuries where the code is not included in the AIS head region of the AAAM book such as is not included in the AIS head region of the AAAM book such as isolated asphyxiation/suffocation injuries. isolated asphyxiation/suffocation injuries. Description Description Report patients who receive scheduled administration of parenteral or Report patients who receive scheduled administration of parenteral or oral beta blocker medication within 48 hours of admission time to the oral beta blocker medication within 48 hours after admission to the index hospital. index hospital. Element Values Element Values • Yes (Y) • Yes (Y) • No (N) • No (N) Additional Information Additional Information • Exclude patients who receive prn or intermittent administration of • Exclude patients who receive prn or intermittent administration of beta blocker treatment. beta blocker treatment. • Example: Patient has one or intermittent orders for metoprolol 5 mg • Example: Patient has one or intermittent orders for metoprolol 5 mg IV Q 15 min x 3. Report as “No.” IV Q 15 min x 3. Report as “No.”
You can also read

















































