A CME/CE-certified Activity - Jointly provided by
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
A CME/CE-certified Activity
Jointly provided by: In collaboration with: This activity is supported by an educational
grant from Lilly. For further information
concerning Lilly grant funding visit
and www.lillygrantoffice.com.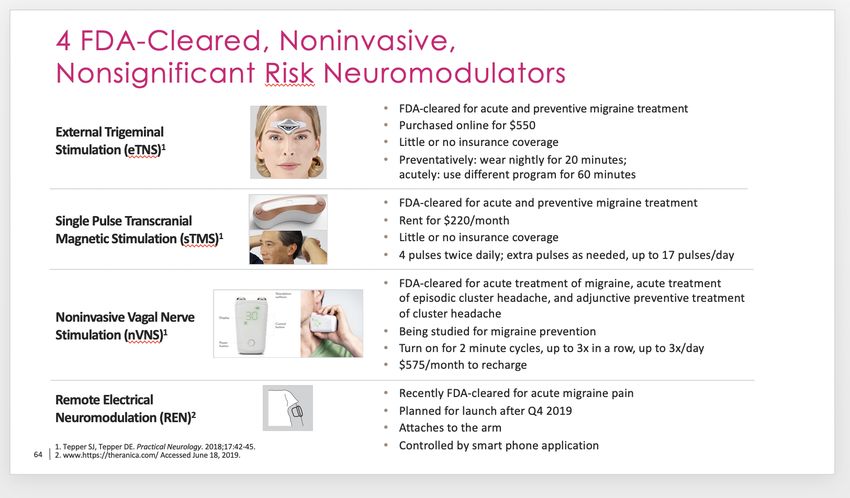
Steering Committee Jack Schim, MD Co-Director The Headache Center of Southern California Carlsbad, CA Christina Treppendahl, FNP-BC, AQH, MHD Founder and Director The Headache Center and the Headache Center Institute Ridgeland, MS
Disclosures
Faculty and Steering Committee Disclosures
The faculty and steering committee reported the following relevant financial relationships that they or their spouse/partner have
with commercial interests:
Jack Schim, MD: Consultant: Acorda, Alder, Allergan, Amgen, Avanir, Depomed, ElectroCore, Lilly, Novartis, Pernix,
Promius, Supernus, Teva Pharmaceuticals, Upsher-Smith; Speaker: Acorda, Allergan, Amgen, Avanir, Depomed, ElectroCore,
Lilly, Novartis, Pernix, Promius, Supernus, Teva Pharmaceuticals, Upsher-Smith; Grants/Research Support: Alder, Allergan,
Amgen, ElectroCore, Lilly, Teva Pharmaceuticals
Christina Treppendahl, FNP-BC, PA-C: Consultant: Eli Lilly; Advisory Board: Eli Lilly; Speaker: Eli Lilly
Non-faculty Disclosures
Non-faculty content contributors and/or reviewers reported the following relevant financial relationships that they or their
spouse/partner have with commercial interests:
Chad Williamson, MS, MBA, CMPP; Blair St. Amand; USF Health CPD Staff; Martin Myers, MD: Nothing to disclose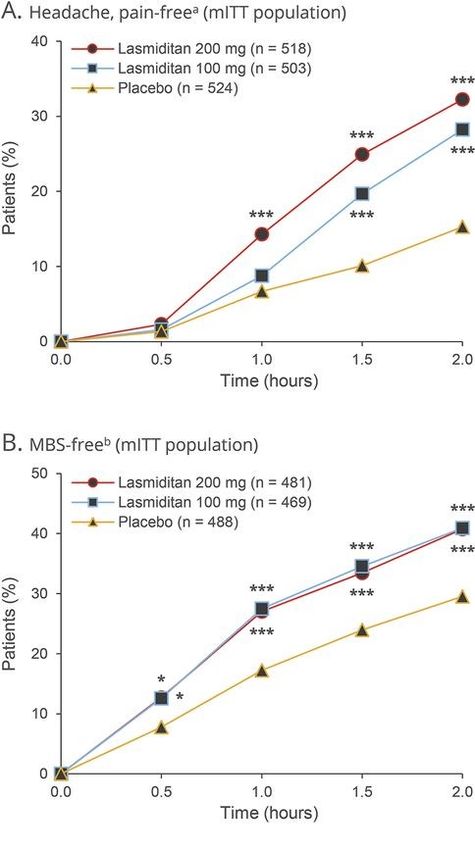
Educational Objectives • Utilize diagnostic criteria to differentiate migraine from other headache disorders • Discuss the pathophysiology of migraine, including the role of calcitonin gene-related peptide (CGRP) • Develop an individualized migraine treatment plan using pharmacologic, nonpharmacologic, and preventive therapies • Examine the efficacy/safety data from clinical trials of new and emerging therapeutic agents for the prevention of migraine

Agenda • Welcome and Introduction • Differentiating Migraine from Other Types of Headache • The Pathophysiology and Role of CGRP in Migraine • Treating Migraine: Current, New, and Emerging Therapies • Q & A Session and Concluding Remarks

Polling Question 1 Please rate your confidence in your ability to differentiate migraine from other types of headache: 1. Not confident 2. Slightly confident 3. Confident 4. Highly confident 5. Expert
Several Types of Headaches (HAs)
Primary Examples Secondary Examples
• Migraine • Infectious (meningitis, sinusitis)
• Tension type • Space occupying lesion (abscess, mass)
• Cluster • Bleeding (SAH)
• Vascular (cerebral venous thrombosis, cervical artery
dissection)
• Rheumatologic (GCA)
Our focus today will be • Ophthalmological (angle-closure glaucoma, optic neuritis)
migraine. • Neurological (trigeminal neuralgia, post-herpetic neuralgia)
• Idiopathic intracranial hypertension
• Others (acute hypertension, CO poisoning)
Rizzoli P, Mullally WJ. Am J Med. 2018;131:17-24.
Impact and Epidemiology of Migraine
• One in five US adults has migraine1
– 38 million persons have migraine each year in the US
• Prevalence
– Women 25% (lifetime); Men 8% (lifetime)
– ~ 70% of migraineurs have positive family history in first-degree relative
• From the 2016 Global Burden of Disease Study
– Migraine is 2nd-leading cause of disability worldwide after low back pain and the leading
cause of disability for people less than age 502,3,4
• 5-9 million PCP office visits per year in US due to migraine2
– 5th-leading cause of annual emergency department visits1
• Associated with ~$17 billion/year in direct and indirect healthcare costs1
1. Migraine.com/migraine-statistics. 2. Global Burden of Disease Study 2016. Lancet Neurol. 2018;17:954-976.
3. Saylor D, Steiner TJ. Semin Neurol. 2018;38:182-190. 4. Steiner TJ et al. J Headache Pain. 2018;19:17.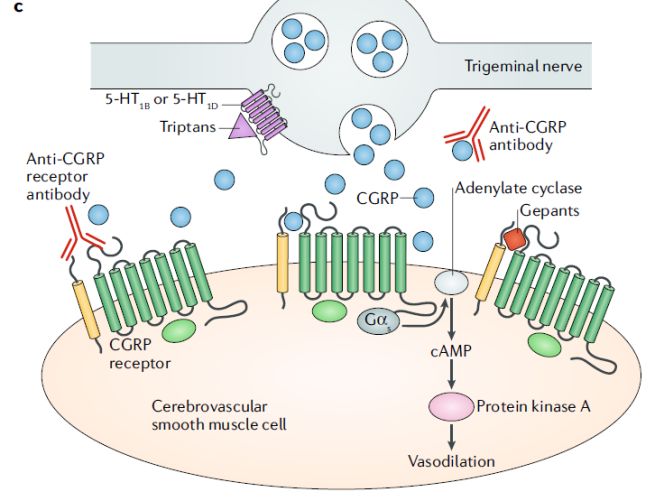
Leslie: A 35-year-old Mother • Asks you for help with her sinus headaches; she has been getting them for several years, but they are occurring almost daily now • Predominantly frontal and maxillary in location; not throbbing • She takes acetaminophen almost daily, along with pseudoephedrine preparations and occasional loratadine when she has watery eyes and nasal congestion • What else do you need to know to help Leslie? • What treatments could be offered?
Differentiating Migraine from Other Headache Disorders
Basics of the History and Physical Exam
Headache Screening
Inquire about: Evaluate:
• Timing/frequency/duration • Patient walking, body language
• Exacerbating factors/triggers • Perform fundoscopic exam
– By activity or movement, or • Assess symmetry of CN, motor,
– Causing avoidance of activities sensory, coordination, DTRs
• Location: Front, back occipital, right/left, • Palpate head, arteries, trigger points
side-locked, neck • Examine neck for stiffness and ROM
• Character: Stabbing, imploding, pulsating, • Examine oral cavity/TMJ
throbbing, dull, sharp
• Associated symptoms: GI, visual, sensory,
language, motor deficits, nausea, photo-,
phono-, and osmophobia
Diagnosis and Treatment of Headache. Bloomington, MN: Institute for Clinical Systems Improvement (ICSI); 2009.Episodic Migraine (EM) Recognition by ICHD Criteria
Migraine without Aura (1.1) Migraine with Aura (1.2.1-6)
At Least FIVE Attacks with: At Least TWO Attacks with:
• At least 2 of the following • At least 1 fully reversible symptom without motor
– Unilateral – Visual + and/or -
– Pulsating – Sensory + and/or -
– Moderate to severe pain – Speech or language dysfunction
– Aggravated by or avoidance • At least 2 of the following
of routine physical activity – At least one aura symptom develops gradually
• At least 1 of the following over ³5 min or different symptoms occur in
– Nausea and/or vomiting succession over ³5 min
– Photo and phonophobia – Each symptom lasts ³5 and £60 min
• No organic disease • 1.1 begins with aura or in £60 min
• No organic disease
ICHD = International Classification of Headache Disorders. International Headache Society. Cephalalgia. 2018;38:1-211.Polling Question 2 What is the single most frequent symptom identifier for migraine? 1. Photophobia 2. Nausea/Upset stomach 3. Sinus pain 4. Pulsating pain on one side of the head 5. Eye pain
ID Migraine™ – A Validated Screener
Closing the HA Diagnosis Gap
Choose Yes or No
• When you have an HA, do you feel nauseated or sick to your stomach?
• When you have an HA, does light bother you (a lot more than when you don’t have an HA)?
• During the last 3 months, have your HAs limited your ability to work, study, or do what you
needed to do?
2/3 Yes for migraine: Positive predictive value of
• Sensitivity: 0.81 =
• Specificity: 0.75 93% in primary care setting
Nausea is the single most important symptom identifier for migraine
Lipton RB et al. Neurology. 2003;61:375-382.Chronic Daily Headache
Chronic Migraine (CM) Medication Overuse Headache (MOH)
• Headache ≥15 days/month AND duration • >15 d/mo with HA
≥4 hours/day x > 3 mo • Regular acute drug use >10 d/mo (>15 d for
• ≥8 days/month are migrainous simple analgesics) for >3 mo
• Not just “more” episodic migraine! • HA worsens over time of overuse
• Evolves as complication of EM (2.5%/year) • HA resolves or reverts to previous pattern within
• More disabling with higher costs 2 mo of overuse elimination
• Risk factors include: • A secondary headache, but often co-morbid
with Chronic Migraine
– Comorbidities (anxiety, depression, obesity)
– Iatrogenic factors (medication type and
• ANY abortive medication can cause
frequency of use) medication overuse headache!
• Can be reversed; goal is revert back to episodic migraine
Natoli JL et al. Cephalalgia. 2010;30:599-609. Buse DC et al. J Neurol Neurosurg Psychiatry. 2010;81:428-432. Link to app for identifying CM
Blumenfeld AM et al. Cephalalgia. 2011;31:301-315. International Headache Society. Cephalalgia. 2018;38:1-211.
CDCP. Census projections request (http://wonder.cdc.gov/population-projections.html). Accessed 10/9/17.
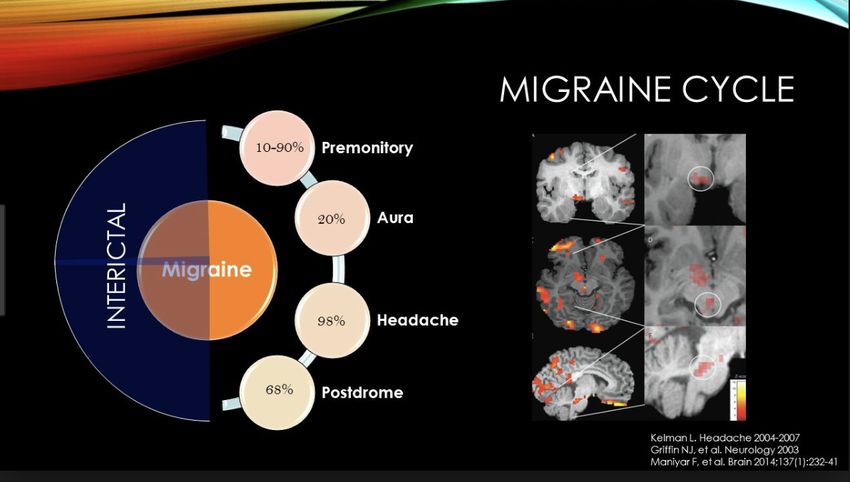
American Headache Society. www.americanheadachesociety.org/assets/1/7/Stephen Silberstein - Medication Overuse Headache.pdf.Understanding the Chronology of Migraine Kelman L. Headache. 2004;44:865-872. Kelman L. Headache. 2007;47:1228-1229. Maniyar F et al. Brain. 2014;137:232-241.
Diagnostic Testing: Indications
Red Flags Green Flags
• Systemic symptoms: fever, weight loss, BP/2o risk: • Stable pattern >6 months
cancer HIV • Long-standing HA history
• Neurologic symptoms or signs • Family history of similar HA
• Onset: new, sudden, abrupt, or split-second • Normal neurologic and fundoscopic
• Older: especially >50 years exams
• Pattern change/prior HA or worsening • Consistently triggered by
• Papilledema/pulsatile tinnitus – Hormonal cycle
• Preciptated by valsalva (space occupying lesion) – Specific sensory input
• Pregnancy – Weather changes
• Positional/postural Diagnostic testing NOT indicated if
Diagnostic testing indicated if ANY red flags only green flags present
are present
Dodick D. Adv Stud Med. 2003;3(6C):S550-S555. Negro A et al. J Headache Pain. 2017;18:106.If Indicated, Which Diagnostic Test?
• CT or MRI? With or without contrast?
– Yield minimal without neurologic signs:Another Look at Leslie
• Further history: she used to have more typical migraine headaches as a
teen; these changed over time to less intense, daily “sinus” type headaches
– In two studies, 86%-88% of self- or physician-diagnosed "sinus" headaches
met ICHD* criteria as migraine or probable migraine1,2
– Autonomic symptoms are common in migraine
• Based on diary review, 94% of headaches that prompt a visit to the PCP
are migraine type headaches3
• You diagnose Leslie with migraine; the appropriate treatments you provide
help reduce her headache occurrence toMultiple Manifestations of Migraine
Current Management ApproachesRichard A 36-year-old Financial Accountant • Has history of very occasional migraines since his early 20s; naproxen and/or a triptan usually provided relief • Started new job 6 months ago, requiring him to work long hours • Headaches have increased and now occur several days a week, especially on most weekend days for the last few months • He is now taking an abortive medication most days a week
Treatments for Headache • Education! • Acute (abortive): taken after attack has begun to relieve pain and disability and to stop progression • Preventive: taken to reduce attack frequency, severity, and duration of attacks • Non-pharmacologic (behavioral, neuromodulation, complementary/alternative) • Combining pharmacotherapy and behavioral therapy is more effective than either as monotherapy Mayo Clinic. www.mayoclinic.org/diseases-conditions/migraine-headache/diagnosis-treatment/drc-20360207. Puledda F, Shields K. Neurotherapeutics. 2018;15:336-345. Holroyd KA et al. BMJ. 2010;1-12. Smitherman TA et al. Headache. 2018;58:1052-1059.
Principles of Management for the Patient
• Establish realistic expectations
– ≈50% reduction with prevention
– ≥70% relief with acute treatment
– There is no cure!
• Encourage patients to participate in their care
– Keep a headache diary, identify triggers
– Educate regarding nuisance vs dangerous side-effects
– Optimize behavioral management
– Acute: administer treatment early; do not use more than 2-3x/week or 10 days/month
– Prevention: follow guidelines for drug/devices/complementary/alternative treatments
– Regular patient follow-up with dose/drug/combination changes as needed
Silberstein SD. Continuum (Minneap Minn). 2015;21(4 Headache):973-989.
Stanford Healthcare. https://stanfordhealthcare.org/medical-conditions/brain-and-nerves/headache/diagnosis/headache-diary.html.
American Headache Society. Headache. 2019;59:1-18.Behavioral Strategies for Managing Migraine
1. Sleep – 6 to 8 hours, consistent within 1 hour to bed/rise (even weekends!)
2. Exercise – Any better than none; aerobic > nonaerobic
3. Stress management – Biofeedback/relaxation, cognitive-behavioral, mindful
therapy, time management
4. $Substance use – Taper caffeine to maximum 1-6 oz cup – Eliminate
artificial sweeteners, decongestants
5. Eat – Fresh, non-processed, small, frequent healthy meals/snacks
Keeping a headache diary can reduce medication overuse headaches
Buse DC et al. Mayo Clin Proc. 2009;84:422-435.Acute (Abortive) Migraine Medications1
Non-specific New Formulations (FDA-approved)
• NSAIDs • Breath-powered intranasal sumatriptan dry powder2
• Combination analgesics • New sumatriptan autoinjectors3
• Neuroleptics/antiemetics
• Sumatriptan nasal spray with permeation enhancer
• Corticosteroids
Specific New Formulations and Classes (In development)
• Triptans • Microneedle array skin patch (zolmitriptan)
• Ergotamine/DHE • New DHE intranasal deliveries: HFA propellant, dry powder
• Gepants
CHOOSING WISELY • 5-HT1F receptor agonist (lasmiditan)4
Don’t recommend prolonged or frequent
use of OTC pain meds for headache • New combinations: meloxicam-rizatriptan;
promethazine-sumatriptan
1. Silberstein S. ExpertNSAID = non-steroidal
Opin Pharmacother. antiinflammatory drug; DHE
2012;13:1961-1968. = dihydroergotamine.
2. Tepper SJ. Headache.2016;56:817.
3. Munjal S et al. J Headache Pain. 2017;18:17. 4. Tepper SJ et al. Headache. 2015;55:621-635.Polling Question 3
When should preventive strategies be initiated in a patient with
migraine?
1. Overuse of acute medications (>2 times per week)
2. Presence of uncommon migraine conditions
(e.g. hemiplegic migraine, prolonged aura)
3. Headaches interfere with patient’s daily life
4. Patient request or preference
5. All of the aboveMigraine Prevention Therapy
Guidelines for Initiation
• Goals: decrease attack frequency, reduce disability and medication overuse
• Many migraineurs qualify for prevention, few are offered it
• Institute preventive strategies if:
– 2 attacks or 1 day of disability/month (≥4 HA days/month, per 2018 AHS Consensus)
– Recurring HA significantly interfering with patient’s daily routine despite acute Rx
– Presence of uncommon migraine conditions: hemiplegic migraine, prolonged aura,
migrainous infarction
– Patient preference, cost considerations, med intolerance
– Acute medications overused >2 d/wk, ineffective, intolerable side effects, or contraindicated
Silberstein SD. Continuum (Minneap Minn). 2015; 21(4 Headache):973-989. Silberstein SD et al. Neurology. 2012;78:1337-1345.
American Headache Society Consensus Statement. Headache. 2019;59:1-18.Challenges Remain in the Use of
Preventive Therapy
80%
40% of migraine patients could benefit
from preventive therapy1
of patients who initiated
a trial of oral migraine
preventive medicines
were no longer taking
preventive treatmentLevel B: Medications are Level U: Inadequate or
Level A: Medications probably effective (1 Level C: Medications conflicting data to Other: Medications that are
with established are possibly effective established as possibly or
AHS efficacy (≥ Class I trials)
Class I or 2 Class II
studies)
(1 Class II study)
support or refute
medication use
probably ineffective
Guidelines Antiepileptic drugs
Divalproex sodium*
Antidepressants
Amitriptyline
ACE inhibitors
Lisinopril
Carbonic anhydrase inhib.
Acetazolamide
Established as not effective
Antiepileptic drugs
Migraine Sodium valproate Venlafaxine Angiotensin rec blockers Antithrombotics Lamotrigine
Topiramate* b-Blockers Candesartan Acenocoumarol Probably not effective
Preventive b-Blockers Atenolola a-Agonists Coumadin Clomipraminea
Therapies Metoprolol Nadolola Clonidinea Picotamide Possibly not effective
Propranolol* Triptans (MRMb) Guanfacinea Antidepressants Acebutolola
Timolola* Naratriptanb Antiepileptic drugs Fluvoxaminea Clonazepama
Triptans (MRMb) Zolmitriptanb Carbamazepinea Fluoxetine Nabumetonea
Frovatriptanb Oxcarbazepine
b-Blockers Antiepileptic drugs
Telmisartan
Nebivolol Gabapentin
Pindolola TCAs
Antihistamines Protriptylinea
Cyproheptadine b-Blockers
Bisoprolola
Calcium blockers
*Highlighted red boxes in left column only indicate FDA-approved medications Nicardipine, Nifedipine
a
Classification based on original guideline and new evidence not found for this report Nimodipine, Verapamil
b For short-term prophylaxis of menstrually-related migraine.
Muscle relaxants
Silberstein SD. Continuum (Minneap Minn). 2015;21(4 Headache):973-989. CyclandelateTreatment for Chronic Migraine
Institute Behavioral Strategies and Prevention Medications
• Specific FDA-approved medication:
OnabotulinumtoxinA
– Approved for prophylaxis of chronic migraine
(≥15 headache days/month)
– 8-9 fewer HA compared to 6-7 with placebo
– 31 injection sites into head/neck Q 3 mo
– Boxed warning re: possibility for spread causing
weakness in distant area(s)
• OnabotulinumtoxinA blocks the presynaptic release
of neurotransmitters, as an endopeptidase that
interrupts the vesicle docking process
Linsenmeyer TA. J Spinal Cord Med. 2013;36:402-419.Migraine Pathophysiology New Insights and Awareness
Martha: A 38-year-old Female • Headaches began when she was 14 • Currently adherent with topiramate 50 mg BID; uses an oral triptan as needed • In the last 3 months, her headaches have increased from 1x/wk to 2-3 days/wk despite optimal lifestyle management and trigger avoidance; they are not always relieved despite prompt triptan use
Polling Question 4
Given Martha’s worsening migraine pattern despite compliance
with behavioral and medication strategies, which of the following
would be an appropriate next step?
1. Increase topiramate dose to 100 mg BID
2. Add gabapentin to the patient’s treatment regimen
3. Add lamotrigine to the patient’s treatment regimen
4. Add a calcitonin gene-related peptide (CGRP) antagonist
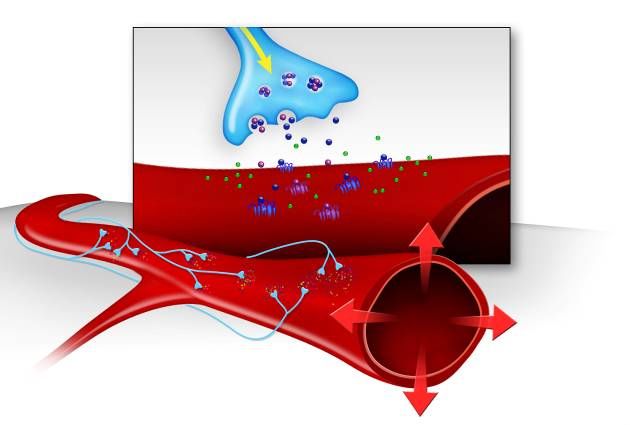
to the patient’s treatment regimenCalcitonin Gene Related Protein (CGRP) First Identified
as a Potential Mediator of Trigeminal Inflammation
Nociceptor
• First discovered as a potent vasodilator
• Initially considered important in migraine because of its
CGRP
receptor
potential peripheral actions
– Vasodilation
Substance – Neuroinflammation
P receptor
• Belongs to calcitonin family (calcitonin, amylin,
adrenomedullin, intermedin) in humans, α-CGRP and
β-CGRP isoforms
CGRP
Substance P
NO
Brain et al. Nature. 1985;313:354.
Edvinsson L, Uddman R. Brain Res Brain Res Rev. 2005;48:438-456.
McCulloch J et al. Proc Natl Acad Sci USA. 1986;83:5731-5735.
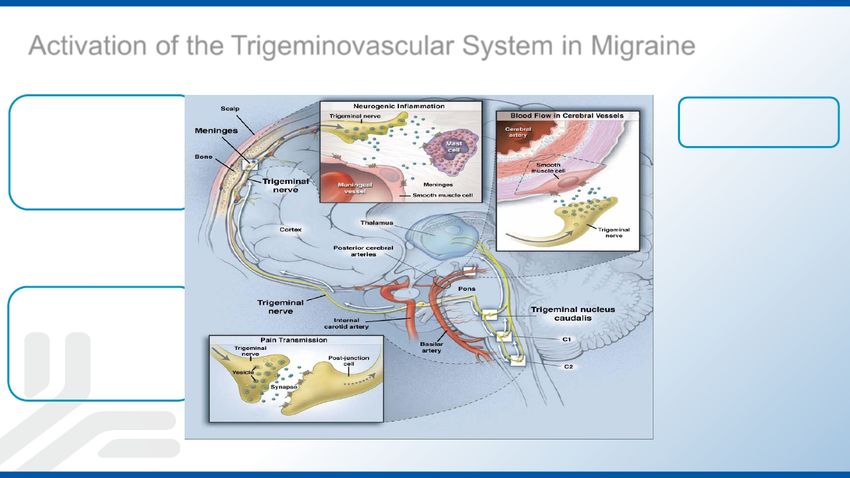
Moskowitz MA. Neurol Clin. 1990;8:801-815.Migraine
Pathogenesis
Meninges
• Inflammation
Meninges
• Vasodilation
Brainstem
• Pain processing
• Central sensitization
CNS = central nervous system.
Adapted from Durham PL.
N Engl J Med. 2004;350:1073-1075.CGRP-Targeted Therapies for Headache Disorders
Three Different Targets of Action
2. Anti-CGRP
antibody
1. Anti-CGRP Onabot-A
receptor
antibody 3. CGRP
receptor
antagonist
Adapted from: Edvinsson L et al. Neurology. 2018;14:338-350.Treating Migraine Headaches
New, Emerging, and
Alternative ApproachesPolling Question 5
Which of the following is true regarding the role of CGRP in
migraine?
1. Serum CGRP levels are elevated in chronic migraine
2. CGRP is a potent vasoconstrictor of cerebral arteries
3. CGRP is released into the ophthalmic vein during migraine
4. Anti-CGRP-receptor monoclonal antibody activity is
likely central
5. All of the aboveThe Role of CGRP in Migraine
• Modulates pain pathways
• Potent vasodilator of cerebral arteries
• Released into jugular venous system during migraine
• Serum CGRP levels elevated in CM
• CGRP infusion evokes migraine
• Small-molecule CGRP-receptor antagonists (gepants) effectively abort migraine
attacks
• Large molecule anti-CGRP and anti-CGRP-receptor monoclonal antibodies (mAbs)
prevent EM and CM
– Because of large size, potential to cross blood brain barrier limited
– mAb activity likely peripheral
Adapted from AHS CMEP. Edvinsson L et al. Neurosci Lett. 1985;58:213-217. McCulloch J et al. Proc Natl Acad Sci USA. 1986;83:5731-5735.
Edvinsson L et al. Ann Neurol. 1987;21:431-437. Lassen LH et al. Cephalalgia. 2002;22:54-61.
Goadsby PJ, Edvinsson L. Brain. 1994;117:427-434. Olesen J et al. N Engl J Med. 2004;350:1104-1110.
Ho TW et al. Neurology. 2008;70:1304-1312. Voss T et al. Cephalalgia. 2016;36:887-898.Small Molecule Approach to Migraine Treatment
CGRP-Receptor Antagonists: The Gepants
• Development of older gepants stopped because of liver toxicity
• Newer, safer gepants in development:
– For acute treatment of episodic migraine
§ BI 44370 TA (oral): effective vs placebo in phase II
§ Rimegepant: effective vs placebo in phase III
§ Ubrogepant: effective vs placebo in phase III; submitted to the FDA in March 2019
– For preventive treatment of episodic migraine
§ Atogepant: effective vs placebo in phase II; will proceed to phase III
§ Rimegepant: phase III in progress
– Gepants have NEVER failed on EFFICACY
Olesen J et al. N Engl J Med. 2004;350:1104-1110. Diener HC et al. Cephalalgia. 2011;31:573-584. Ho TW et al. Lancet. 2008;372:2115-2123. Marcus R et al. Cephalalgia. 2014;34:114-125.
Voss T et al. Cephalalgia. 2016;36:887-898. Allergan press release. June 11, 2018. www.allergan.com/news/news/thomson-reuters/allergan-s-oral-cgrp-receptor-antagonist-atogepant.aspx.
Allergan press release. March 11, 2019. www.allergan.com/news/news/thomson-reuters/allergan-announces-fda-acceptance-of-new-drug-appl.Rimegepant1 and Ubrogepant2,3 Phase III Studies – Abortives • These studies included adults aged 18-65, rarely older. Complicated patients, such as those with numerous comorbidities, autoimmune diseases, and poorly controlled depression, were not included in the studies. Thus, generalizability should be considered.1-3 • The most common adverse events with rimegepant were nausea and urinary tract infections.1 • The most common adverse events with ubrogepant (>5%) were nasopharyngitis, upper respiratory tract infection, sinusitis, urinary tract infection, and influenza2,3 • With both medications, no liver related issues have been seen, and overall safety profiles have been consistent with placebo1-3 1. Lipton et al. Presented at AHS 2018. 2. Dodick D et al. AHS 2018. Presentation IOR01LB. 3. Lipton RB et al. AHS 2018. Poster PS111LB.
Polling Question 6 Which of the following FDA-approved CGRP antagonists are dosed monthly by a subcutaneous route? 1. Erenumab 2. Eptinezumab 3. Galcanezumab 4. Fremanezumab 5. 1, 3, and 4 6. 2, 3, and 4 7. All of the above
Large Molecule Approach to Migraine Treatment
Four Monoclonal Antibodies to CGRP or Its Receptor Approved or in Development
Erenumab-aooe Fremanezumab-vfrm Galcanezumab-gnlm Eptinezumab
(fully humanized) (fully humanized) (humanized) (humanized)
Studied for EM, CM EM, CM, eCH, cCH EM, CM, eCH, cCH EM, CM
Monthly or quarterly SC; 225 Monthly SC; 240 mg loading
Route and Monthly subq
mg monthly, or 675 mg Q3 dose, then 120 mg SC Q3 months IV
Dosing 70, 140 mg
months monthly thereafter
Target CGRP receptor CGRP peptide or ligand CGRP peptide or ligand CGRP peptide or ligand
FDA approved FDA approved 9/26/18 for Submitted BLA to FDA
Regulatory FDA approved 9/14/18 for
5/17/18 for migraine migraine prevention and 2/22/19 for migraine
Status migraine prevention
prevention 6/4/19 for eCH prevention
CM = chronic migraine; cCH= chronic cluster headache; eCH = episodic cluster headache; EM = episodic migraine; SC= subcutaneous; BLA= biologic license application
Tepper SJ. Headache. 2018;58 (S3):238-275. Tepper SJ. Headache. 2018; 58(S3):276-290. Edvinnson L. Headache. 2018;58(S1):33-47.
Lilly press release. March 5, 2019. AIMOVIG® (erenumab-aooe) injection prescribing information. Amgen Inc., Thousand Oaks, CA. Revised: 03/2019.
EMGALITYTM (galcanezumab-gnlm) injection prescribing information. Eli Lilly and Company, Indianapolis, IN. Revised: 6/1/2019.
AJOVY® (fremanezumab-vfrm) injection prescribing information. Teva Pharmaceuticals USA, Inc. North Wales, PA, Revised 1/2019.
Alder press release. February 22, 2019; https://www.globalnewswire.com/news-release/2019/02/22/1740250/0/en/Alder-BioPharmaceuticals-Submits-Biologics-License-
Application-to-the- U-S-Food-And-Drug-Administration-for-Eptinezumab.html. Accessed April 5, 2019;Episodic Migraine and CGRP Monoclonal Antibodies
Phase III Results
70 *PmAbs to CGRP or the CGRP Receptor
How are they different than our current migraine preventive medications?
• mAbs for the most part do not cross the blood-brain barrier1,2
• mAbs are eliminated by the reticuloendothelial system – so far, hepatotoxicity has not been seen1,3,4 lgG1 Monoclonal
• Because they work, it is likely that peripheral anti-CGRP action is sufficient to prevent migraine Antibody ~150 kDa
Are they an improvement?3,4 All 4 Small
• Prevent episodic migraine, chronic migraine, medication-overuse headache; Molecule
~0.2-1 kDa
galcanezumab also prevents episodic cluster headache
• Have shown quick onset: separate from placebo within 1 week
• Have led to a clinically meaningful response by 1 month
• Have shown unprecedented responder rates of ≥75%
• Have shown safety and tolerability similar to placebo
• Decrease acute medication use days; improve impact, disability, and/or quality of life
1. Yu YJ, Watts RJ. Neurotherapeutics. 2013;10:459-472. 2. Lipton RB et al. US Neurology. 2018;14 (suppl 4):S3-S10.
3. Tepper SJ. Headache. 2018;58 (suppl 3):238-275. 4. Tepper SJ. Headache. 2018;58 (suppl 3):276-290.A New Abortive Recently Approved
Lasmiditan – Serotonin1F Receptor Agonist
• Lasmiditan, FDA approved for PRIMARY ENDPOINT 100 mg (n=503) 200 mg (n=518) Placebo (n=524)
acute migraine Oct 2019 with
warning not to engage in % of Subjects Pain-free1 at 2h 28.2% 32.2% {38.8%} 15.3% {21.3%}
potentially hazardous activities Odds ratio (95% CI) 2.2 (1.6 – 3.0) 2.6 (2.0 – 3.6)
for at least 8 hours
P-valueNew Abortives in Development “ditans” – Serotonin1F Receptor Agonists • Lasmiditan, positive in Phase III (Samurai and Spartan) studies as abortive • Oral tablet 50-400 mg • AEs: dizziness, drowsiness, paresthesias • Does not constrict vessels These studies included adults aged 18-65, rarely older. Complicated patients, such as those with numerous comorbidities, autoimmune diseases, and poorly controlled depression, were not included in the studies. Thus, generalizability should be considered. *P
Sandra: A 50-year-old Female
• Diagnosed with episodic migraines more than 20 years ago
• History of CAD for past 5 years and has decided to embrace a
“clean” lifestyle
– Patient no longer wants to use naproxen or a triptan
– Began an aerobic exercise regimen and her sleeping schedule has
improved
– However, she continues to experience headaches 5 times a month
• She asks you if there are any non-pharmacologic therapies that
she could use to reduce her migraines?Four FDA-Cleared, Noninvasive,
Nonsignificant Risk Neurostimulators
External Trigeminal Single Pulse Transcranial Non-invasive Vagal Nerve Remote Electrical
Stimulation (eTNS) 1 Magnetic Stimulation (sTMS) 1 Stimulation (nVNS)1 Neuromodulation (REN)2
• FDA-cleared for acute and • FDA-cleared for acute and • FDA-cleared for acute treatment • Recently FDA-cleared for
preventive migraine treatment preventive migraine treatment of migraine, acute treatment of acute migraine pain
• Purchased online for $550 • Rent for $220/month episodic cluster headache, and
• Planned for launch after
adjunctive preventive treatment
• Little or no insurance • Little or no insurance Q4 2019
of cluster headache
coverage coverage • Attaches to arm
• Being studied for migraine
• Preventively: Wear nightly for • 4 pulses twice daily, with extra • Controlled by smart phone
prevention
20 minutes pulses as-needed up to 17 application
• Acutely: Use different pulses/day • Turn on for 2-minute cycles, up to
program for 60 minutes 3x in a row, up to 3x/day
• $575/month to recharge
1. Tepper SJ, Tepper DE. Practical Neurology. 2018;17:42-45. 2. www.https://therancia.com/ Accessed June 18, 2019.Single-Pulse Transcranial Magnetic Stimulation (sTMS)
Approved for Acute and Preventive Treatment
ESPOUSE Prevention Study
4 pulses twice/day; 3 pulses up to 3 times for acute HA
1
0.5 Performance Goal
Mean Reduction of Headache Days
(PG)
0
-0.5
-0.63 BL BL
Full Analy sis Set
from Baseline
-1 Days Days (FAS; mean reduction
= 9.06 = 9.07 in HA days)
-1.5
Per Protocol (PP;
-2 mean reduction in
acute med use)
Rental – $150/month -2.5 -2.73 -2.98
* PTranscutaneous Supraorbital Neurostimulator (tSNS)
• Device covers the supratrochlear and supraorbital nerves
• FDA approved: for acute1 and preventive2 migraine treatment
• 67-patient RCT; turn it on and wear it 20 minutes/day
0.5 0.3
45
0 40 38.2
35 50% responder rates
–0.5 Change in HA days (NS) 30
–1.0 P=0.054 25 P=0.023
20
–1.5 15 12.1
–2.0 10
–2.1 5
–2.5 0
Active Sham
Active Sham
• Cost: $400 to buy, can return for money back within 60 days,
$25 q2-3 mos. for replacement electrodes
This study included adults aged 18-65, rarely older. Complicated patients, such as those with numerous comorbidities, autoimmune
diseases, and poorly controlled depression, were not included in the study. Thus, generalizability should be considered.
1. www.prnewswire.com/news-releases/fda-releases-cefaly-for-acute-treatment-of-migraine-attacks-300523385.html.
2. https://migraine.com/pro/fda-approves-cefaly.
Schoenen J et al. Neurology. 2013;80;697-704. Tepper D. Headache. 2014;54:1415-1416.Non-invasive Vagal Nerve Stimulator (nVNS)
• Handheld, patient-controlled device that:
– Preferentially activates vagal afferents, not vagal efferent
pathways that cause bradycardia and bronchoconstriction1,2
– Inhibits rat CSD,3 central trigeminovascular, and
thalamocortical pathways4-6
• Approved in US for acute treatment of migraine, as well as
episodic cluster headache
• No serious AEs, minimal-risk device
These studies included adults aged 18-65, rarely older. Complicated patients, such as those with numerous comorbidities, autoimmune
diseases, and poorly controlled depression, were not included in these studies. Thus, generalizability should be considered.
CSD = cortical spreading depression
1. Schoenen J et al. AAN, 2016: Abstract I3.006. 2. Mourdoukoutas et al. AAN 2016. 3. Chen SP et al. Pain. 2016;157:797-805.
4. Hawkins et al. AAN 2016. 5. Akerman et al. AAN, 2016. 6. Nonis R et al. AAN,2016.Remote Electrical Neuromodulation (REN)
• Modulates descending tracts in the brain RESPONSE AT 2 HOURS
Response at 2 hours post-treatment
POST-TREATMENT
• Small, simple, smartphone controlled PComplementary and Alternative Considerations • Riboflavin • Tai Chi • Magnesium • Melatonin • Acupuncture • Hypnotherapy • Spinal/osteopathic manipulation • Cold therapy • Physical therapy • Massage • Exercise • Homeopathy • Yoga • Coenzyme Q10 Millstine D et al. BMJ. 2017;357:j1.
Key Highlights • Recurring HA with disability is migraine until proven otherwise • Patients should institute acute therapies as soon a possible after headache onset • Use of acute meds >9 days/month can lead to medication overuse or transformation to chronic migraine • Preventive treatment should be offered early to reduce adverse outcomes • Newer modalities, such as CGRP antagonists, neuromodulators, and complementary options, may supplement the therapeutic benefits offered by traditional therapies
Migraine and Management:
The Impact of Decision Making with PCPs
©HEALTH UNION, LLC. 5Meeting People Where They Are ©HEALTH UNION, LLC. 5
Patient Doctor Relationships & Migraine Management
Opportunity to improve the
patient experience with
treatment
v Only half reported being
satisfied with care from HCP
v Only half reported having an
HCP who regularly discussed
QoL on current treatment plan
N= 4,356
Source: Health Union – Migraine In America Survey 2018Perceptions of the HCP Relationship
58%* 46%* 39%*
My HCP clearly explains My HCP regularly My HCPs communicate
treatment options discusses my QOL with effectively with each other about
my current treatment plan my condition/health concerns
N= 3,975. *Top 2 Strongly Agree/Agree
Source: Health Union – Migraine In America Survey 2018Listening to the
Migraine
Community
©Health Union, LLC | Confidential
Health Union, LLC.Post-activity Survey
Post-Activity Question 1 What is the single most important symptom identifier for migraine? 1. Photophobia 2. Nausea 3. Sinus pain 4. Pulsating pain on one side of the head 5. Eye pain
Post-Activity Question 2
When should preventive strategies be initiated in a patient with
migraine?
1. Overuse of acute medications (>2 times per week)
2. Presence of uncommon migraine conditions (e.g.
hemiplegic migraine, prolonged aura)
3. Headaches interfere with patient’s daily life
4. Patient request or preference
5. All of the abovePost-Activity Question 3
Given Martha’s worsening migraine pattern despite compliance
with behavioral and medication strategies, which of the following
would be an appropriate next step?
1. Increase topiramate dose to 100 mg BID
2. Add gabapentin to the patient’s treatment regimen
3. Add lamotrigine to the patient’s treatment regimen
4. Add a calcitonin gene-related peptide (CGRP) antagonist
to the patient’s treatment regimenPost-Activity Question 4
Which of the following is true regarding the role of CGRP in
migraine?
1. Serum CGRP levels are elevated in chronic migraine
2. CGRP is a potent vasoconstrictor of cerebral arteries
3. CGRP is released into the ophthalmic vein during migraine
4. Anti-CGRP-receptor monoclonal antibody activity is likely
central
5. All of the abovePost-Activity Question 5 Which of the following FDA-approved CGRP antagonists are dosed monthly by a subcutaneous route? 1. Erenumab 2. Eptinezumab 3. Galcanezumab 4. Fremanezumab 5. 1, 3, and 4 6. 2, 3, and 4 7. All of the above
Q & A Session and Concluding Remarks
Thank you for joining us today!
Please remember to complete your
EVALUATION.
Your participation will help shape future CME activities.You can also read

















































