Abstract Past, Present, and Future of Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Ovarian Cancer
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Open Access Review
Article DOI: 10.7759/cureus.15563
Past, Present, and Future of Hyperthermic
Intraperitoneal Chemotherapy (HIPEC) in
Ovarian Cancer
Mona Mishra 1 , Nilanchali Singh 2 , Prafull Ghatage 3
1. Obstetrics and Gynecology, Maulana Azad Medical College, New Delhi, IND 2. Obstetrics and Gynecology, All India
Institute of Medical Sciences, New Delhi, IND 3. Gynecology and Oncology, Tom Baker Cancer Center, Calgary, CAN
Corresponding author: Nilanchali Singh, nilanchalisingh@gmail.com
Abstract
Hyperthermic intraperitoneal chemotherapy (HIPEC), along with optimal cytoreductive surgery, has been
debated to be a viable option for the treatment of advanced epithelial ovarian cancer with peritoneal
carcinomatosis. HIPEC is associated with a direct and improved penetration of chemotherapy drugs into the
affected tissue and is associated with fewer systemic side effects. There is no standard protocol for the use of
HIPEC in advanced ovarian cancer. Hence, there is controversy over the timing, dose, duration, and efficacy
of HIPEC. In this review, the history, technique, current evidence, recommendations, and future directions
of HIPEC are discussed.
Categories: Obstetrics/Gynecology, Oncology
Keywords: hipec, hyperthermic intraperitoneal chemotherapy, ovarian cancer, clinical trials, technique
Introduction And Background
Ovarian malignancy is the most lethal of all gynecological cancers. The standard of care for ovarian cancer is
surgery in early stages and platinum-based chemotherapy followed by interval debulking surgery in
advanced cases. With this norm followed, the five-year survival is less than 30% and recurrence rates are
high. Ovarian cancer is known for local spread to the peritoneum, hence, local therapy seems promising.
Intraperitoneal (IP) chemotherapy was developed with this idea, and a systemic review found its results
promising, with increased survival time and reduced risk of mortality by 12% with each cycle of
intraperitoneal therapy [1]. However, the therapy could not gain popularity due to the higher incidence of
adverse events. Lately, increased temperature of the chemotherapy agent used intra-peritoneally is being
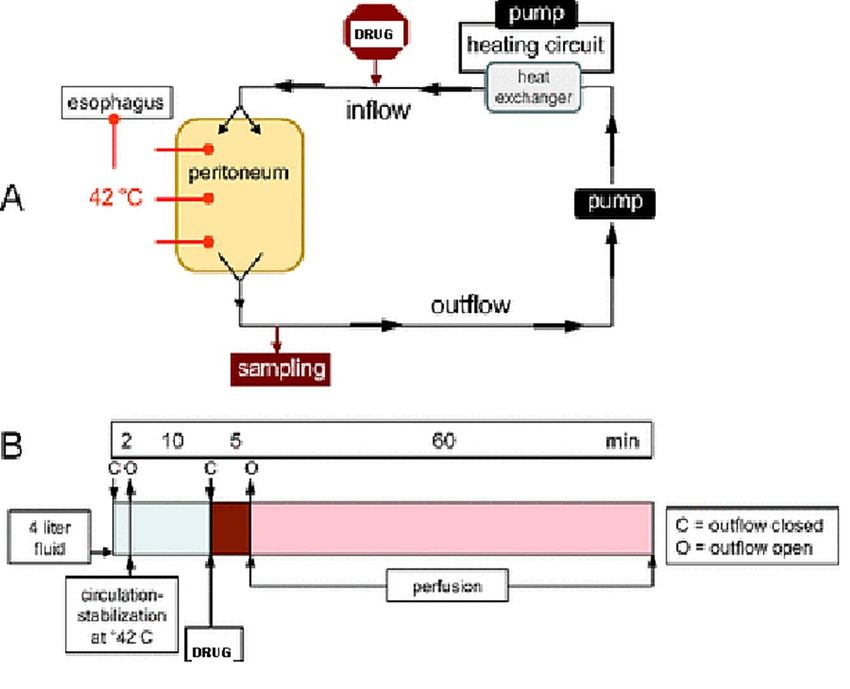
evaluated for its efficacy in ovarian malignancy. Hyperthermic intraperitoneal chemotherapy, popularly
called hyperthermic intraperitoneal chemotherapy (HIPEC), is a technique for delivering a chemotherapeutic
agent, in which a heated solution of chemotherapy agent is perfused throughout the peritoneal space
(Figure 1). It has been used for the treatment of advanced peritoneal malignancies, including
gastrointestinal (colorectal and appendiceal) and advanced ovarian cancers. The aim is to target residual
Review began 05/19/2021
disease after cytoreductive surgery (CRS) by directly acting on the cancer cells present on the peritoneal
Review ended 06/01/2021 surface. The blood peritoneal barrier limits systemic absorption of the chemotherapy agent, hence reducing
Published 06/10/2021 its side effects and toxicity. HIPEC has a controversial role in the management of ovarian cancers. This
© Copyright 2021
review deals with the historical aspects, current role, and future perspective of HIPEC.
Mishra et al. This is an open access article
distributed under the terms of the
Creative Commons Attribution License
CC-BY 4.0., which permits unrestricted
use, distribution, and reproduction in any
medium, provided the original author and
source are credited.
How to cite this article
Mishra M, Singh N, Ghatage P (June 10, 2021) Past, Present, and Future of Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Ovarian
Cancer. Cureus 13(6): e15563. DOI 10.7759/cureus.15563FIGURE 1: Diagrammatic representation of HIPEC
HIPEC: hyperthermic intraperitoneal chemotherapy
Review
Rationale of hyperthermia
Hyperthermia has a multi-fold effect on cancer cells. Firstly, heat encompasses a direct cytotoxic effect on
cancer cells by the increased production of lysosomes. Secondly, heat has a synergistic effect with certain
anti-mitotic agents (cisplatin, paclitaxel, oxaliplatin, and mitomycin) and potentiates their action [2].
Thirdly, heat improves the penetration of chemotherapy, leading to the increased sensitivity of tumor cells
to chemotherapy and interrupting deoxyribonucleic acid (DNA) repair [3-5]. Hyperthermia also helps in
reducing resistance to cisplatin by decreasing the mechanisms of cellular resistance [6]. Lastly, it has an
immunomodulatory role and improves the immune response against tumor cells by inducing heat shock
proteins (HSP), activating antigen-presenting cells, and lymphocyte migration [7].
Although the rising body temperature is associated with significant risks, various methods have been
developed for raising the temperature of the intraperitoneal cavity with a minimal increase in the
temperature of the rest of the body. During HIPEC, heat is applied loco-regionally and the body’s core
temperature is controlled. The anesthesia team aids in core temperature control by applying ice packs in the
neck and groin regions. Moreover, automated pumps are available, which are specifically designed for
temperature-regulated continuous drug delivery and monitoring of the infusion process.
History
The history of HIPEC is interesting. Egyptian doctors treated tumors with heat around 5000 BC. The Greeks
too realized the importance of thermal energy in some form of medical treatment. The most ancient texts of
the Law of Moses mention hot springs as having medicinal values. While grazing donkeys, Anah discovered
the hot and medicinal springs in the desert, a rare and valuable finding. The techniques in the past have
utilized fever-causing microbial extracts or hot water baths for the induction of hyperthermia to treat
various ailments [8]. However, both approaches are difficult to monitor. The use of hyperthermia in cancer
treatment is first documented by De Kizowitz from France, in 1779. He assessed the effect of fever caused by
malaria on malignant tumors. In 1866, Busch in Germany reported the remission of a facial sarcoma in a
patient with a high fever due to erysipelas [9]. William Coley, a surgeon from New York Memorial Cancer
Hospital, developed the “Coley toxin” in the 1800s, which is a mixture of bacterial culture. It was used to
induce hyperthermia in cancer patients. It was the first specialized bacterial antitumor pyrogen [10]. He
managed to treat 38 patients with cancers, who had a high-grade fever: 12 patients had complete regression
of tumors while 19 patients improved. In 1898, Westermark used total-body hyperthermia with hot baths to
treat inoperable cervical cancer and found promising results [11].
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 2 of 14In the twentieth century, localized heat was used in the form of galvanocautery to treat cervical and uterine
cancers [12]. It was found that cancer cells were more sensitive to heat than normal tissues of the body.
These findings were reproduced by others as well. Immersion in heated water is another method evaluated.
This was used to achieve localized hyperthermia of the limbs or of the entire body. This was used for
disseminated tumors.
Luk et al. (1980) investigated hyperthermia with radiotherapy as a treatment modality in patients with
advanced cancers not responding to conventional treatment. It was found that hyperthermia achieved by
microwave combined with radiotherapy was found to have a higher tumor regression rate as compared to
either modality alone. Luk’s study was a pilot study in which a temperature average of 42.5 degrees was
induced by microwave diathermy to treat superficial cancers. The response of recorded tissue temperatures,
either alone or in combination with radiation therapy, was evaluated. The treatment was well-tolerated by
patients with only a few side effects [13].
HIPEC was first introduced by John Spratt in 1980 [14]. He treated a pseudomyxoma peritonei patient with
intraperitoneal thiotepa followed by hyperthermic intraperitoneal methotrexate. Koga et al. confirmed the
role of combined hyperthermia and intraperitoneal chemotherapy in the treatment of implanted peritoneal
cancer in rats [15]. He showed that optimal control of peritoneal metastasis was achieved not by heat or
chemotherapy alone but by a combination of hyperthermia with chemotherapy. Yonemura and Kanazawa
established the role of this treatment in the prevention of gastric cancer peritoneal disease and for the
treatment of established disease [16]. The role of HIPEC in improving survival outcomes in peritoneal
disease is slowly being established in interval debulking surgery, following neoadjuvant chemotherapy,
secondary cytoreductive surgery, and, most recently, in the setting of primary cytoreductive surgery.
Candidates for HIPEC
Women with primary and recurrent stage IIIc ovarian cancer are most commonly recruited in various
observational and interventional studies evaluating the role of HIPEC. Studies performed in ovarian
malignancy stages Ic to IIIc have reported better survival outcomes with the use of HIPEC [17]. Evidence of
the use of HIPEC in recurrent ovarian cancer is limited to a single trial and a few retrospective studies [18].
There is no consensus regarding the chemotherapeutic drug to be used, the protocol for agent delivery, and
postoperative therapy for HIPEC in recurrent ovarian cancer.
Technique
After resection of all gross disease, the abdominal cavity is initially irrigated with normal saline to remove
all particulate matter that may block the outflow circuit and to ensure that there is adequate hemostasis
prior to HIPEC delivery. Enteric reconstruction can be carried out prior to or after HIPEC therapy.
Hyperthermia can be generated by various perfusion systems that are available. These systems include
closed circuit pumps, which deliver heated chemotherapy drugs through inflow catheters with drainage
accomplished via outflow catheters. HIPEC can be performed using two techniques, the open or coliseum
technique and the closed technique.
Open Technique
In the open technique, a big, nonporous synthetic mesh is sewed to the edges of the skin incision, and the
abdomen is tented up using retractors. The surgeon manually stirs the perfusate in the abdomen for even
distribution and adequate exposure of organs to heated chemotherapy. Inflow and outflow catheters are
located on the lateral abdominal wall. The advantages and disadvantages of the open technique are listed in
Table 1.
Advantages of the open technique Disadvantages of the open technique
Even distribution of heated chemotherapy throughout the abdominal cavity Risk of exposure
Risk of spillage
Time-consuming
Accelerated heat loss
TABLE 1: Advantages and disadvantages of the open technique
[19]
At our center, HIPEC is done as an ‘open coliseum technique.’ A small Bookwalter retractor is used and the
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 3 of 14skin is sutured to the frame. The frame is fixed about 3 to 4 inches above the abdomen. This ensures that
there is no spillage of the drug. Once sutured, the abdomen is closed with a clear X-ray cassette dressing
with a small opening made in the dressing so as to allow for mixing of the drug(s). The technician heats the
circulating fluid using D5W to 40⁰C to 42⁰C before injecting the chemotherapy drug.
Closed Technique
In the closed technique, after cytoreduction, the inflow and outflow catheters are introduced into the
abdominal cavity through the midline incision. The abdominal incision is sutured ensuring a watertight
closure. The abdomen is then instilled with the carrier solution following which perfusion begins. Once the
goal temperature of 40⁰C-42⁰C is reached, the chemotherapy drug is filled in the reservoir and perfused for
30 to 120 minutes. During the procedure, the abdominal wall may be agitated to facilitate even drug
distribution throughout the abdominal cavity. After the perfusion cycle is complete, the chemotherapy drug
is drained through the outflow catheter and the abdomen is then irrigated with normal saline. The
advantages and disadvantages of the closed technique are mentioned in Table 2.
Advantages of the closed technique Disadvantages of the closed technique
Minimal heat loss Unequal intra-abdominal distribution of chemotherapy drugs
Higher concentration of drug in the blood, leading to
Easy achievement of intraperitoneal goal temperature
myelosuppression
Reduced chance of spillage and exposure to chemotherapy
drugs
Less time consuming
The theoretical benefit of improved drug penetration
TABLE 2: Advantages and disadvantages of the closed technique
[19]
Chemotherapy drugs used for HIPEC
An ideal chemotherapy drug to be used for HIPEC should be cell-cycle non-specific, water-soluble, having a
synergistic effect with heat, with a high molecular weight and proven cytotoxic effect. There has been
no consensus in terms of the choice of chemotherapy drug, its dosage, dwell time, goal temperature, and
duration of perfusion. These parameters vary widely across various studies conducted until now as shown in
Table 3.
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 4 of 14Study Design Inclusion criteria Drugs Results
Randomized controlled
trial: HIPEC+
5-year progression-free survival (p =
cytoreductive surgery
Lim Primary ovarian cancer Cisplatin 75 mg/m2, 90 0.569): HIPEC: 20.9%, Control: 16%;
(CRS) + systemic
2017 [20] stages 3 and 4 min at 41.5⁰C 5-year overall survival (p = 0.574):
chemotherapy (n = 92),
HIPEC: 51%, Control: 49.4%
CRS + systemic
chemotherapy (n = 92)
Stage III ovarian cancer Progression[Ns1]-free survival:
Multicentric randomized patients who have received HIPEC: 14.2 months, Control: 10.7
Van Driel controlled trial: CRS + neoadjuvant chemotherapy Cisplatin 100 mg/m2, months; Median overall survival:
2018 [21] HIPEC (n = 122), CRS with carboplatin and 90 min at 40⁰C HIPEC: 45.7 months, Control: 33.9
alone (n= 123) paclitaxel with stable months Adverse events of grade 3
disease after 3 cycles and 4: 25% and 27%
Cisplatin 100 mg/m2,
Primary or recurrent
Paclitaxel 175 mg/m2,
Ansaloni peritoneal carcinomatosis Recurrence rate 59%; Mean
Open prospective phase 2 Doxorubicin 35 mg/m2,
et al. with ovarian cancer; recurrence time 14.4 months; Mean
study 90 min at 41.5⁰C, 66%
2012 [22] Primary (n=9), Recurrent hospital stay 23.8 days
received cisplatin +
(n=30)
doxorubicin.
TABLE 3: Studies describing the role of HIPEC in primary ovarian cancer
HIPEC: hyperthermic intraperitoneal chemotherapy
In general, cisplatin is the most commonly used chemotherapy drug used for HIPEC in gynecological
malignancies and is recommended by the National Comprehensive Cancer Network (NCCN) guidelines.
Other commonly used drugs in HIPEC include paclitaxel, liposomal doxorubicin, either alone or in various
combinations. In the setting of primary ovarian cancer, Lim et al. and Van Driel described the use of
intraperitoneal cisplatin while Ansaloni et al. used intraperitoneal cisplatin, paclitaxel, and doxorubicin in
doses described in Table 3 [20-22]. There has been no consensus in terms of the ideal chemotherapy drug
regimen in women receiving HIPEC for the treatment of recurrent ovarian cancer. Fagotti described the use
of oxaliplatin while Bakrin et al. used cisplatin alone or along with mitomycin C or doxorubicin [17-18].
Spiliotis et al. used cisplatin and paclitaxel in platinum-sensitive women while doxorubicin and paclitaxel
or mitomycin C was given to platinum-resistant women [23]. Large randomized controlled trials are needed
in the future to address this. Table 4 and Table 5 show various chemotherapeutic agents used in HIPEC and
their mean peak peritoneal activity, respectively.
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 5 of 14Drug Dosage
Cisplatin 50 -75 mg/m2
Doxorubicin 30- 75 mg/m2
Gemcitabine 1000 mg/m2
Paclitaxel 60 -175 mg/m2
Oxaliplatin 360 – 480 mg/m2
Caelyx 20 – 50 mg/m2
5FU 600 mg/m2
Docetaxel 40 – 150 mg/2
Carboplatin AUC 5-6
TABLE 4: Drugs used for HIPEC and their dosage
HIPEC: hyperthermic intraperitoneal chemotherapy; AUC: area under the curve
Carboplatin 18
Cisplatin 20
5FU 298
Paclitaxel 1000
Doxorubicin 494
Mephalan 94
Caelyx 600 – 1000
Gemcitabine 500 – 800
TABLE 5: Mean peak peritoneal cavity: plasma concentration ratio of various chemotherapy
agents used in HIPEC
HIPEC: hyperthermic intraperitoneal chemotherapy
Timing of HIPEC
Intraperitoneal chemotherapy is usually performed immediately after cytoreduction. There is uncertainly on
whether the complications are increased if done after any gastrointestinal anastomosis. At our center, HIPEC
is preferably performed just prior to closure (after bowel anastomosis, etc). Concerns about the
inconveniences of delivery and toxicities associated with postoperative intraperitoneal chemotherapy
motivated researchers to work out whether HIPEC could improve safety and quality of life.
Temperature
The synergistic effect of hyperthermia and intraperitoneal chemotherapy is observed from a temperature of
39°C and thereafter increases linearly. However, bowel tissue tolerance to temperature limits the upper limit
of heat administered intraperitoneally. A study conducted by Shimizu et al. found that heat administered
intra-abdominally in rats was safe at a temperature of 39°C. However, the application of heat at a
temperature of 46°C or 45°C leads to a mortality of 100% and 90%, respectively. Also, 100% survival was
found at 44°C [24]. Retrospective studies in humans show that an intra-abdominal temperature above 42°C
is associated with a higher complication rate [25]. Keeping these data in mind, most surgical oncologists
have reached a general consensus of 41°C-43°C as the desired level of intra-abdominal hyperthermia.
Duration
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 6 of 14The duration of HIPEC varies from 30 minutes to 120 minutes depending on the institutional protocol and
other factors like the pharmacokinetics of chemotherapy drugs, patients' cell count, and renal function.
Role of HIPEC in primary ovarian cancer
The role of HIPEC in the management of primary ovarian carcinoma is still debatable. Most of the studies
have not shown any benefit. However, there are a few studies that have shown good results with HIPEC in
primary ovarian cancer. Ansaloni et al. (2012) conducted a prospective phase 2 study recruiting 39 patients
with primary or recurrent peritoneal carcinomatosis. Seventy-seven percent (77%) of patients had recurrent
carcinomatosis and 23% had a primary tumor. Cytoreductive surgery was performed in these patients after
which HIPEC was performed. The procedure was performed for 90 minutes, with an intraperitoneal
temperature of 41.5°C. Fifty-nine percent (59%) of patients had recurrence with the mean recurrence time
being 14.4 months [22].
Lim et al. in 2017 conducted a randomized controlled trial in women with stages 3 and 4 primary ovarian
cancer. There was no significant difference found in progression-free survival (PFS) in the HIPEC versus
control groups (43.2% vs. 43.5% at 2 years and 20.9% vs. 16.0% at 5 years; P= 0.569). Five-year OS was also
found to be similar in both groups [20].
Van Driel et al. conducted a multicentric, prospective randomized controlled trial in women with stage 3
ovarian cancer who had stable disease after receiving three cycles of neoadjuvant chemotherapy. It was a
landmark trial in which 245 patients, who underwent interval cytoreductive surgery (CRS) with or without
HIPEC, were recruited. A total of 122 patients were randomly assigned to receive intraperitoneal cisplatin
(100 mg/m2) after an intra-peritoneal temperature of 40°C was achieved with heated saline. One-hundred
twenty-three (123) women underwent CRS without HIPEC. Patients received an additional three cycles of
adjuvant chemotherapy. The median overall survival rate was 33.9 months and 45.7 months in the surgery
and surgery with HIPEC groups, respectively. The median recurrence-free survival rate was 10.7 months in
the surgery group and 14.2 months in the surgery with HIPEC group. Grades 3 and 4 toxicities were similar in
both groups (25% vs 27% in the surgery and surgery with HIPEC groups, respectively). The drawbacks of this
study include the exclusion of stage 4 ovarian cancer [21].
Forty (40) patients with advanced ovarian malignancy, who were planned for upfront cytoreductive surgery
along with HIPEC, were enrolled in a phase II, non-randomized, single-arm study. Patients received
adjuvant chemotherapy with bevacizumab after surgery. Complete cytoreduction was achieved in all the
cases. Early complications were observed in 23 patients, which included hematological toxicity, pleural
effusion requiring a drain, relaparotomy for hemorrhage, and bowel anastomosis dehiscence. Eight patients
had major complications (pleural effusion with drain and bowel anastomosis dehiscence). Overall, the data
suggested that the safety of HIPEC in the upfront treatment of advanced ovarian cancer is reasonable [26].
The major complications reported in this study were pleural effusion requiring a drain in five patients and
bowel anastomosis dehiscence in three patients. The reported late complications were mild and related to
kidney failure. No postoperative death was reported in the series.
In a recent trial from China, survival outcomes were compared between primary cytoreductive surgery (PCS)
with HIPEC versus PCS alone for patients with stage III epithelial ovarian cancer. Four-hundred twenty-five
(425; 72.8%) underwent PCS with HIPEC and 159 (27.2%) underwent PCS alone. The median survival time
was 49.8 (95%CI, 45.2-60.2) months for patients undergoing PCS with HIPEC and 34.0 (95%CI, 28.9-41.5)
months for patients undergoing PCS alone, and the three-year overall survival rate was 60.3% (95%CI,
55.3%-65.0%) for patients undergoing PCS with HIPEC and 49.5% (95%CI, 41.0%-57.4%) for patients
undergoing PCS alone. Subgroup analysis was further done in the complete and incomplete surgery
subgroups. Patients in the PCS with HIPEC group had significantly better survival than those in the PCS
group, except for the three-year overall survival rate in the incomplete subgroup. Among those who
underwent complete surgical procedures and comparing those who received PCS with HIPEC vs those who
received PCS alone, the median survival time and the three-year overall survival rate were better in the
HIPEC group (P = .04). In this study, the PCS with HIPEC treatment approach was associated with better
long-term survival [27].
A randomized phase 3 trial showed a significant benefit in recurrence‐free and overall survival when HIPEC
was added to interval cytoreductive surgery (CRS) in patients who were not eligible for primary surgery
because of the extent of their disease (OVHIPEC trial; NCT00426257). The trial showed no important
differences in toxicity or patient‐reported outcomes between the study groups. The extent of surgery and
the number of bowel resections were also similar between the two study groups, and the effect of HIPEC was
homogeneous across the levels of predefined and post hoc subgroups. Nevertheless, the design and results
of the OVHIPEC trial were critically assessed, and this resembles the reluctance to adopt the positive results
of earlier intraperitoneal chemotherapy studies [28].
Role of HIPEC in recurrent ovarian cancer
There is no clear consensus as to the usefulness and the protocol most suitable for HIPEC in women with
recurrent ovarian cancer. In 2012, in a case-control study conducted by Fagotti et al., performing HIPEC led
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 7 of 14to a significant reduction in secondary recurrence and mortality of women having recurrent platinum-
sensitive ovarian cancer [17].
In a retrospective multicentric study of recurrent or persistent ovarian cancer(n= 246 ), treated by
cytoreductive surgery and HIPEC in two French centers, Bakrin et al. (2012) found no significant difference
in overall median survival rate in platinum-resistant and platinum-sensitive disease (48 months in
platinum-resistant disease and 52 months in platinum-sensitive disease, respectively; p=0.568) [18]. In
another retrospective case-control study conducted by Le Brun (2014) recruiting women with first ovarian
cancer relapse, significantly improved overall survival was observed in women receiving CRS followed by
HIPEC [29].
A case-control study conducted by Safra et al. (2014) in women with recurrent epithelial ovarian cancer also
suggested significant improvement in five-year survival and progression-free survival in women undergoing
surgery with HIPEC as compared to those receiving systemic chemotherapy alone. Treatment outcome
according to the patients' breast cancer gene (BRCA) status was also compared. Fifty-one point two percent
(51.2%) women in controls and 51.9% women in the HIPEC group were BRCA gene mutation carriers. BRCA
gene mutation carriers were also found to have significantly improved survival on adding HIPEC after CRS
(in BRCA gene mutation carriers, progression-free survival was 20.9 months in the HIPEC group and 12.6
months in the chemotherapy alone group, respectively; p=0.048) [30]. An observational study by Classe and
Petrillo also showed favorable survival rates in women with recurrent ovarian cancer receiving CRS followed
by HIPEC [31-32].
In 2015, Spiliotis et al. conducted the first randomized controlled trial recruiting 120 women with stages IIIc
and IV disease who had recurrence after initial treatment with debulking surgery followed by systemic
chemotherapy. Group A comprising 60 women was treated with secondary debulking surgery followed by
HIPEC and systemic chemotherapy. Thirty-four (34) patients were platinum-sensitive with 26 who were
platinum-resistant. Intraperitoneal cisplatin 100 mg/m2 and paclitaxel 175 mg/m2 was administered for 60
minutes at 42.5°C in women with platinum-sensitive disease. Doxorubicin 35 mg/m2 and either paclitaxel
175 mg/m2 or mitomycin 15 mg/m2 was delivered for 60 minutes at 42.5°C. In 40 women, the open
technique was used while in 20 women, the closed technique was used. Women in Group B underwent
debulking surgery followed by systemic chemotherapy alone. The mean overall survival rate was found to be
significantly higher in group A compared to group B (26.7 versus 13.4 months; P0.66, 95% confidence interval 0.54-0.82; P < .001). DESKTOP III is the first prospectively randomized trial
showing an OS benefit of debulking surgery in recurrent ovarian cancer. SOC-3 (Surgery and Niraparib in
Secondary Recurrent Ovarian Cancer) is an ongoing multicenter, randomized controlled, phase II trial of
secondary cytoreduction followed by chemotherapy and niraparib (PARP-inhibitor) maintenance versus
chemotherapy and niraparib maintenance in patients with platinum-sensitive, second relapsed ovarian
malignancy. With the above-mentioned completed trials, the role of secondary cytoreduction is well-proven.
The addition of HIPEC with secondary cytoreduction needs further validation [37].
Various trials are ongoing in this field including the HORSE (Chemotherapy (HIPEC) in Ovarian Cancer
Recurrence) and CHIPOR (Hyperthermic Intra-Peritoneal Chemotherapy (HIPEC) in Relapse Ovarian Cancer
Treatment) trials [38-39]. The HORSE trial was a multicentric randomized controlled trial in which
progression-free survival will be compared between women having first ovarian cancer recurrence, receiving
surgery plus HIPEC versus surgery alone [38]. Similarly, in the CHIPOR trial, 444 patients with ovarian
cancer recurrence were recruited and randomized to either undergo surgery with HIPEC or surgery alone
[39]. Table 6 describes the role of HIPEC in recurrent ovarian cancer.
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 9 of 14Study Design Inclusion criteria Drugs Results
Case-control study:
Platinum-sensitive Secondary recurrence 66.6% in
Fagotti 30 cases CRS + Oxaliplatin 460 mg/m2, 41.5⁰C for
recurrent ovarian cases, 100% in controls
2012 [17] HIPEC, 37 controls 30 min, closed technique
cancer (P=0.001)
CRS alone
Recurrent and
persistant ovarian
cancer treated with 95.5% received cisplatin alone or in Overall median survival: 48
Retrospective
Bakrin optimal CRS + HIPEC; combination with mitomycin C or months in platinum-resistant and
multicentric study
2012 [18] Platinum-resistant doxorubicin, 90 minutes at 44⁰C- 52 months in platinum-sensitive
(n=246)
persistant (n=62); 46⁰C, open and closed technique (P=0.568)
Platinum-sensitive
recurrent (n=184)
Randomized
Platinum-sensitive: cisplatin 100
controlled trial:
Stage IIIc & IV ovarian mg/m2 + paclitaxel 175 mg/m2;
Secondary CRS +
cancer with recurrence Platinum-resistant: doxorubicin 35 Mean overall survival: HIPEC:
Spiliotis HIPEC + systemic
after debulking surgery mg/m2 + paclitaxel 175 mg/m2 or 26.7 months, No HIPEC: 13.4
2015 [23] chemotherapy (n=
followed by systemic mitomycin 15 mg/m2 60 min at months (Panastomotic leaks, intra-abdominal hemorrhage, and sepsis. Toxicities specific to HIPEC are mainly
hematological and renal. Transient bone marrow suppression, anemia, leukopenia, and thrombocytopenia
are the frequently reported hematological complications. Acute kidney injury is the most common toxicity in
patients undergoing HIPEC with cisplatin. Cisplatin-associated nephrotoxicity can be prevented by using
nephroprotectants such as sodium thiosulphate although larger studies are needed to determine the choice
of and the optimal dose of nephroprotectants. Other adverse effects are specific to the chemotherapy drugs
used. Oxaliplatin is associated with bleeding complications. HIPEC with cytoreductive surgery is associated
with higher chances of toxicity as compared to cytoreduction alone. However, recent studies have shown
that the toxicity rate of HIPEC alone and HIPEC combined with cytoreduction are similar. In the multicentric
RCT conducted by Van Driel, the grade 3-4 toxicity rate was similar in both the groups (25% versus 27% in
cytoreduction alone and cytoreduction with HIPEC, respectively) [20]. In the retrospective study conducted
by Bakrin, overall morbidity was 31% and mortality was 0.5%. Leukopenia, intra-abdominal hemorrhage,
and an anastomotic leak occurred in 11.6%, 3%, and 2.4% respectively [18].
ERAS in HIPEC
Enhanced Recovery After Surgery (ERAS) Society recommendations, 2020, have provided guidelines for
ERAS in cytoreductive surgery with and without HIPEC (CRS±HIPEC) [43]. It is recommended that
preoperative counseling should be indicated routinely to improve quality of life, somatic symptoms, and
psychological outcomes. Preoperative nutritional screening by the use of a validated tool and by measuring
serum albumin is also recommended. In patients with malnutrition or at risk for malnutrition, nutritional
and protein (>1.2 g/kg/day) supplementation (oral>enteral>parenteral) for at least five days and up to 14
days in cases of severe malnutrition is recommended routinely. In these surgical candidates, a combination
of at least two antiemetic drugs (ondansetron, dexamethasone, droperidol) should be indicated routinely to
prevent postoperative nausea and vomiting. Prophylactic antibiotics within one hour before incision for
CRS±HIPEC without the need for routine repeated administration should be indicated routinely to prevent
surgical site infection. Total intravenous anesthesia as an alternative to inhalation anesthesia could be
indicated to prevent postoperative nausea and vomiting. Preoperative mechanical bowel preparation alone
for patients undergoing CRS±HIPEC including probable colectomy should not be indicated to reduce the
incidence of surgical site infection and an anastomotic leak. Preoperative mechanical bowel preparation is
indicated with probable rectal resection. Epidural analgesia (T5-T11, low dose of local anesthetic and
opioids) for 72 h after CRS/HIPEC should be indicated routinely to obtain pain relief, spare opioids, and
hasten the resumption of bowel function. Limiting postoperative fluid-related weight gain (target: < 3.5 kg
on postoperative day 3) is advised.
Future perspectives
Most ongoing trials are being conducted on women having primary ovarian cancer. Cisplatin is the most
commonly used HIPEC drug in these trials followed by paclitaxel. In the HIPECOV trial, women with both
primary and recurrent ovarian cancer are being recruited and the efficacy of HIPEC with lobaplatin following
CRS will be evaluated. HORSE and CHIPOR are two large trials that are being conducted, recruiting women
with recurrent ovarian cancer. In these two trials, women would undergo platinum-based NACT followed by
interval debulking surgery followed by HIPEC in the treatment arm [37-38]. Until now there is no standard
guidelines with respect to the exact patient population and the histology of ovarian tumor in which HIPEC
would prove to be most beneficial. There is, at present, no standardized chemotherapy drug regimen or
guidelines on treatment duration and temperature decided for performing HIPEC. These ongoing trials
could probably provide answers to these questions, and their results are eagerly awaited.
Other controversial issues are whether HIPEC is effective as an addition to upfront surgery and after surgery
for recurrent disease, whether it has better efficacy as compared to adjuvant intraperitoneal chemotherapy,
what are the side/adverse effects of hyperthermia on the body, what is the optimal health care setting
required to perform HIPEC, and the use of biomarkers for selecting a suitable subset of patients likely to
benefit from HIPEC.
Pressurized intraperitoneal aerosol chemotherapy (PIPAC) is a novel technique in which the chemotherapy
drug is delivered in an aerosol form inside the abdominal cavity and maintained at high pressure inside the
abdominal cavity. The aerosol form leads to even distribution of the drug on the peritoneal surface while the
pressure ensures deeper penetration of the drug. During laparoscopy, the chemotherapy drug is delivered
from a high-pressure injector (1500 kPa) through a micropump into the abdominal cavity, and after 30
minutes, the drug-aerosol is suctioned out through a suction system [44]. PIPAC and its role is being
explored in women with recurrent ovarian cancer with peritoneal metastasis. Women with peritoneal
metastasis are candidates for systemic palliative chemotherapy. However, systemic chemotherapy is less
effective in peritoneal metastasis due to poor tumor absorption. In such women, intraperitoneal
chemotherapy with PIPAC without cytoreductive surgery has been found to be safe and well-tolerated [45]. It
allows for improved tumor penetration and intra-abdominal dissemination. In a systematic review
conducted by Tempfer et al., the objective tumor response rate was 69%, and the mean overall survival
duration was 13.7 months. It was concluded that PIPAC maintained the quality of life and was found feasible
safe and effective in women with ovarian cancer and peritoneal carcinomatosis [46]. In a single-arm, phase
1, nonrandomized study, PIPAC with dose-escalating cisplatin and doxorubicin could safely be applied in
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 11 of 14women with recurrent ovarian cancer [47]. All studies conducted are single-armed studies and large
randomized control trials are needed to provide further evidence in favor of this novel technique.
Table 7 summarizes all ongoing trials studying the role of HIPEC in ovarian cancers.
Trial HIPEC Duration
NCT number Trial title n Indication Treatment arm Control arm Country Outcome
acronym drug of trial
Surgery plus hyperthermic intra-peritoneal
chemotherapy (HIPEC) versus surgery alone in Recurrent Cisplatin
CRS with CRS without September
NCT01539785 HORSE patients with platinum-sensitive first recurrence 158 ovarian at 75 Rome, Italy PFI
HIPEC HIPEC 2012
of ovarian cancer: a prospective randomized cancer mg/m²
multicenter trial
Recurrent Platinum-based Platinum-based
platinum- NACT × 6 NACT × 6 Cisplatin
Hyperthermic intraperitoneal chemotherapy 4/2011–
NCT01376752 CHIPOR 444 sensitive cycles, followed cycles, followed at 75 Belgium/France OS
(HIPEC) in relapsed ovarian cancer treatment 4/2025
ovarian by CRS with by CRS without mg/m²
cancer HIPEC HIPEC
Cisplatin
Hyperthermic intraperitoneal chemotherapy Primary CRS or IDS with CRS or IDS 100 4/2019–
NCT03842982 CHIPPI 432 France DFS
(HIPEC) in ovarian cancer EOC HIPEC without HIPEC mg/m2 × 6/2024
90 min
Paclitaxel
HIPEC- Hyperthermic intraperitoneal chemotherapy Primary CRS with CRS without 175 1/2012–
NCT02681432 60 Spain OS
OVA with paclitaxel in advanced ovarian cancer EOC HIPEC HIPEC mg/m2 × 12/2019
60 min
Cytoreductive surgery (CRS) plus hyperthermic
Primary and Lobaplatin
intraperitoneal chemotherapy (HIPEC) with CRS with CRS without 9/2017–
NCT03371693 HIPECOV 112 recurrent 30 mg/m2 China OS
lobaplatin in advanced and recurrent epithelial HIPEC HIPEC 12/2020
EOC at 60’C
ovarian cancer
TABLE 7: Ongoing trials on HIPEC
[38-39], [48-50]
HIPEC: hyperthermic intraperitoneal chemotherapy; CRS: cytoreductive surgery; PFI: progression-free interval; OS: overall survival;
NACT: neoadjuvant chemotherapy; DFS: disease-free survival; IDS: interval debulking surgery; EOC: epithelial ovarian cancer
Conclusions
HIPEC is an alternative to cytoreductive surgery alone and palliative chemotherapy in women with advanced
ovarian cancer with extensive peritoneal metastasis. There exists controversy around HIPEC for both
primary and recurrent ovarian cancer, and there is a strong need for more randomized controlled trials on
this issue to reach some necessary conclusions. There are difficulties in including HIPEC as a standard of
care due to the variation and non-standardization of different studies, in design and protocol. Larger, well-
designed trials are, therefore, needed to provide further answers in terms of exact protocol and drug regimen
that would be suitable to perform HIPEC. The suitability of candidates for HIPEC is still an enigma, and the
results of ongoing trials would hopefully provide further knowledge in this direction. The five-year survival
of advanced ovarian cancer is around 50% and HIPEC could be a game-changer in the optimal management
of women with ovarian cancer and peritoneal metastasis, provided further, well-designed studies prove so.
Additional Information
Disclosures
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the
following: Payment/services info: All authors have declared that no financial support was received from
any organization for the submitted work. Financial relationships: All authors have declared that they have
no financial relationships at present or within the previous three years with any organizations that might
have an interest in the submitted work. Other relationships: All authors have declared that there are no
other relationships or activities that could appear to have influenced the submitted work.
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 12 of 14References
1. Tewari D, Java JJ, Salani R, et al.: Long-term survival advantage and prognostic factors associated with
intraperitoneal chemotherapy treatment in advanced ovarian cancer: a Gynecologic Oncology Group study. J
Clin Oncol. 2015, 33:1460-6. 10.1200/JCO.2014.55.9898
2. Kusumoto T, Holden SA, Ara G, Teicher BA: Hyperthermia and platinum complexes: time between
treatments and synergy in vitro and in vivo. Int J Hyperthermia. 1995, 11:575-86.
10.3109/02656739509022491
3. van de Vaart PJ, van der Vange N, Zoetmulder FA, et al.: Intraperitoneal cisplatin with regional
hyperthermia in advanced ovarian cancer: pharmacokinetics and cisplatin-DNA adduct formation in
patients and ovarian cancer cell lines. Eur J Cancer. 1998, 34:148-54. 10.1016/s0959-8049(97)00370-5
4. Panteix G, Beaujard A, Garbit F, et al.: Population pharmacokinetics of cisplatin in patients with advanced
ovarian cancer during intraperitoneal hyperthermia chemotherapy. Anticancer Res. 2002, 22:1329-36.
5. Ohno S, Siddik ZH, Kido Y, et al.: Thermal enhancement of drug uptake and DNA adducts as a possible
mechanism for the effect of sequencing hyperthermia on cisplatin-induced cytotoxicity in L1210 cells.
Cancer Chemother Pharmacol. 1994, 34:302-6. 10.1007/BF00686037
6. Hettinga JV, Konings AW, Kampinga HH: Reduction of cellular cisplatin resistance by hyperthermia—a
review. Int J Hyperthermia. 1997, 13:439-57. 10.3109/02656739709023545
7. Skitzki JJ, Repasky EA, Evans SS: Hyperthermia as an immunotherapy strategy for cancer . Curr Opin Investig
Drugs. 2009, 10:550-8.
8. Braude AI, Beck J, Zalesky M: Febrile response to bacterial pyrogens in leukemia . Blood. 1960, 16:1279-84.
10.1182/blood.V16.3.1279.1279
9. Berliner entomologische Zeitschrift / herausgegeben von dem Entomologischen Vereine in Berlin [Article in
German]. Entomologische Verein in Berlin. 1866, 1866:488.
10. Coley WB: The treatment of malignant tumors by repeated inoculations of erysipelas. With a report of ten
original cases. 1893. Clin Orthop Relat Res. 1991, 3-1.
11. Westermark F: Uber die Behandlung des ulcerirenden Cervix carcinoma mittels Knonstanter Warme [Article
in German]. Zbl Gynak. 1898, 22:1335-7.
12. Regional Chemotherapy. Hyperthermia in cancer treatment . (2016). Accessed: July 11, 2020:
https://regionalchemotherapy.com/treatments/hyperthermia-cancer-treatment/.
13. Luk KH, Hulse RM: Hyperthermia in cancer therapy . West J Med. 1980, 132:179-85.
14. Spratt JS, Adcock RA, Muskovin M, et al.: Clinical delivery system for intraperitoneal hyperthermic
chemotherapy. Cancer Res. 19801, 40:256-60.
15. Koga S, Hamazoe R, Maeta M, et al.: Treatment of implanted peritoneal cancer in rats by continuous
hyperthermic peritoneal perfusion in combination with an anticancer drug. Cancer Res. 1984, 44:1840-2.
16. Fujimura T, Yonemura Y, Muraoka K, et al.: Continuous hyperthermic peritoneal perfusion for the
prevention of peritoneal recurrence of gastric cancer: randomized controlled study. World J Surg. 1994,
18:150-5. 10.1007/BF00348209
17. Fagotti A, Costantini B, Petrillo M, et al.: Cytoreductive surgery plus HIPEC in platinum-sensitive recurrent
ovarian cancer patients: a case-control study on survival in patients with two year follow-up. Gynecol
Oncol. 2012, 127:502-5. 10.1016/j.ygyno.2012.09.020
18. Bakrin N, Cotte E, Golfier F, et al.: Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy
(HIPEC) for persistent and recurrent advanced ovarian carcinoma: a multicenter, prospective study of 246
patients. Ann Surg Oncol. 2012, 19:4052-8. 10.1245/s10434-012-2510-4
19. Fong Y, Gamblin TC, Han ES, Lee B, Zager JS: Cancer Regional Therapy. HAI, HIPEC, HILP, ILI, PIPAC and
Beyond. Springer Nature, Switzerland;
20. Lim MC, Chang S-J, Yoo HJ, et al.: Randomized trial of hyperthermic intraperitoneal chemotherapy (HIPEC)
in women with primary advanced peritoneal, ovarian, and tubal cancer. J Clin Oncol. 2017, 35: 5520.
10.1200/JCO.2017.35.15_suppl.5520
21. van Driel WJ, Koole SN, Sikorska K, et al.: Hyperthermic intraperitoneal chemotherapy in ovarian cancer . N
Engl J Med. 2018, 378:230-4. 10.1056/NEJMoa1708618
22. Ansaloni L, Agnoletti V, Amadori A, et al.: Evaluation of extensive cytoreductive surgery and hyperthermic
intraperitoneal chemotherapy (HIPEC) in patients with advanced epithelial ovarian cancer. Int J Gynecol
Cancer. 2012, 22:778-85. 10.1097/IGC.0b013e31824d836c
23. Spiliotis J, Halkia E, Lianos E, Kalantzi N, Grivas A, Efstathiou E, Giassas S: Cytoreductive surgery and HIPEC
in recurrent epithelial ovarian cancer: a prospective randomized phase III study. Ann Surg Oncol. 2015,
22:1570-5. 10.1245/s10434-014-4157-9
24. Shimizu T, Maeta M, Koga S: Influence of local hyperthermia on the healing of small intestinal anastomoses
in the rat. Br J Surg. 1991, 78:57-9. 10.1002/bjs.1800780119
25. Jacquet P, Stephens AD, Averbach AM, et al.: Analysis of morbidity and mortality in 60 patients with
peritoneal carcinomatosis treated by cytoreductive surgery and heated intraoperative intraperitoneal
chemotherapy. Cancer. 1996, 77:2622-9. 10.1002/(SICI)1097-0142(19960615)77:123.0.CO;2-T
26. Paris I, Cianci S, Vizzielli G, et al.: Upfront HIPEC and bevacizumab-containing adjuvant chemotherapy in
advanced epithelial ovarian cancer. Int J Hyperthermia. 2018, 35:370-4. 10.1080/02656736.2018.1503346
27. Lei Z, Wang Y, Wang J, et al.: Evaluation of cytoreductive surgery with or without hyperthermic
intraperitoneal chemotherapy for stage III epithelial ovarian cancer. JAMA Netw Open. 2020, 3:e2013940.
10.1001/jamanetworkopen.2020.13940
28. The Netherlands Cancer Institute. Phase III Randomized clinical trial for stage III epithelial ovarian cancer
randomizing between primary cytoreductive surgery with or without hyperthermic intraperitoneal
chemotherapy. (2021). Accessed: January 14, 2021: https://clinicaltrials.gov/ct2/show/NCT03772028.
29. Le Brun JF, Campion L, Berton-Rigaud D, et al.: Survival benefit of hyperthermic intraperitoneal
chemotherapy for recurrent ovarian cancer: a multi-institutional case control study. Ann Surg Oncol. 2014,
21:3621-7. 10.1245/s10434-014-3693-7
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 13 of 1430. Safra T, Grisaru D, Inbar M, et al.: Cytoreduction surgery with hyperthermic intraperitoneal chemotherapy
in recurrent ovarian cancer improves progression-free survival, especially in BRCA-positive patients—a
case-control study. J Surg Oncol. 2014, 110:661-5. 10.1002/jso.23688
31. Classe J-M, Glehen O, Decullier E, et al.: Cytoreductive surgery and hyperthermic intraperitoneal
chemotherapy for first relapse of ovarian cancer. Anticancer Res. 2015, 35:4997-5005.
32. Petrillo M, De Iaco P, Cianci S, et al.: Long-term survival for platinum-sensitive recurrent ovarian cancer
patients treated with secondary cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy
(HIPEC). Ann Surg Oncol. 2016, 23:1660-5. 10.1245/s10434-015-5050-x
33. Baiocchi G, Ferreira FO, Mantoan H, et al.: Hyperthermic intraperitoneal chemotherapy after secondary
cytoreduction in epithelial ovarian cancer: a single-center comparative analysis. Ann Surg Oncol. 2016,
23:1294-301. 10.1245/s10434-015-4991-4
34. Coleman RL, Brady MF, Herzog TJ, et al.: Bevacizumab and paclitaxel-carboplatin chemotherapy and
secondary cytoreduction in recurrent, platinum-sensitive ovarian cancer (NRG Oncology/Gynecologic
Oncology Group study GOG-0213): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2017,
18:779-91. 10.1016/S1470-2045(17)30279-6
35. Harter P, du Bois A, Hahmann M, et al.: Surgery in recurrent ovarian cancer: the Arbeitsgemeinschaft
Gynaekologische Onkologie (AGO) DESKTOP OVAR trial. Ann Surg Oncol. 2006, 13:1702-10.
10.1245/s10434-006-9058-0
36. Harter P, Sehouli J, Reuss A, et al.: Prospective validation study of a predictive score for operability of
recurrent ovarian cancer: the Multicenter Intergroup Study DESKTOP II. A project of the AGO Kommission
OVAR, AGO Study Group, NOGGO, AGO-Austria, and MITO. Int J Gynecol Cancer. 2011, 21:289-95.
10.1097/IGC.0b013e31820aaafd
37. Du Bois A, Sehouli J, Vergote I, et al.: Randomized phase III study to evaluate the impact of secondary
cytoreductive surgery in recurrent ovarian cancer: final analysis of AGO DESKTOP III/ENGOT-ov20. J Clin
Oncol. 2020, 38:6000. 10.1200/JCO.2020.38.15_suppl.6000
38. Surgery plus hyperthermic intra-peritoneal chemotherapy (HIPEC) versus surgery alone in patients with
platinum-sensitive first recurrence of ovarian cancer: a prospective randomized multicenter trial. (2014).
https://clinicaltrials.gov/ct2/show/NCT01539785.
39. A phase III randomized study evaluating hyperthermic intra-peritoneal chemotherapy (HIPEC) in the
treatment of relapse ovarian cancer. (2020). Accessed: May 20, 2021:
https://clinicaltrials.gov/ct2/show/NCT01376752.
40. Colombo N, Sessa C, du Bois A, et al.: ESMO-ESGO consensus conference recommendations on ovarian
cancer: pathology and molecular biology, early and advanced stages, borderline tumours and recurrent
disease. Ann Oncol. 2019, 30:672-705.
41. Vergote I, Harter P, Chiva L: Is there a role for intraperitoneal chemotherapy, including HIPEC, in the
management of ovarian cancer?. J Clin Oncol. 2019, 37:2420-3. 10.1200/JCO.19.00091
42. Armstrong DK, Alvarez RD, Bakkum-Gamez JN, et al.: NCCN Guidelines insights: ovarian cancer, version
1.2019. J Natl Compr Canc Netw. 2019, 17:896-909.
43. Hübner M, Kusamura S, Villeneuve L, et al.: Guidelines for perioperative care in cytoreductive surgery (CRS)
with or without hyperthermic IntraPEritoneal chemotherapy (HIPEC): Enhanced recovery after surgery
(ERAS®) society recommendations - part I: preoperative and intraoperative management. Eur J Surg Oncol.
2020, 46:2292-310. 10.1016/j.ejso.2020.07.041
44. Nadiradze G, Horvath P, Sautkin Y, Archid R, Weinreich FJ, Königsrainer A, Reymond MA: Overcoming drug
resistance by taking advantage of physical principles: Pressurized Intraperitoneal Aerosol Chemotherapy
(PIPAC). Cancers (Basel). 2019, 12:34. 10.3390/cancers12010034
45. Tempfer CB, Winnekendonk G, Solass W, et al.: Pressurized intraperitoneal aerosol chemotherapy in women
with recurrent ovarian cancer: a phase 2 study. Gynecol Oncol. 2015, 137:223-8.
10.1016/j.ygyno.2015.02.009
46. Tempfer C, Giger-Pabst U, Hilal Z, Dogan A, Rezniczek GA: Pressurized intraperitoneal aerosol
chemotherapy (PIPAC) for peritoneal carcinomatosis: systematic review of clinical and experimental
evidence with special emphasis on ovarian cancer. Arch Gynecol Obstet. 2018, 298:243-57. 10.1007/s00404-
018-4784-7
47. A phase I, single-arm, open-label, three step dose escalation study with intraperitoneal pressurized cisplatin
and doxorubicin in recurrent ovarian cancer and peritoneal carcinomatosis. (2018). Accessed: June 3, 2020:
https://clinicaltrials.gov/ct2/show/NCT02475772.
48. Phase III randomized clinical trial evaluating hyperthermic intraperitoneal chemotherapy (HIPEC) in
ovarian cancer considering two different settings: primary debulking surgery (PDS) and interval debulking
surgery (IDS). (2019). Accessed: June 3, 2020: https://clinicaltrials.gov/ct2/show/NCT03842982.
49. Hyperthermic intraperitoneal chemotherapy with paclitaxel for the treatment of patients with recurrent or
primary advanced ovarian cancer: a randomised phase 3 study. (2016). Accessed: June 3, 2020:
https://clinicaltrials.gov/ct2/show/NCT02681432.
50. A phase III clinical trial of cytoreductive surgery (CRS) plus hyperthermic intraperitoneal chemotherapy
(HIPEC) with lobaplatin in advanced and recurrent epithelial ovarian cancer . (2017). Accessed: June 3,
2020: https://clinicaltrials.gov/ct2/show/NCT03371693.
2021 Mishra et al. Cureus 13(6): e15563. DOI 10.7759/cureus.15563 14 of 14You can also read

















































