Adult Growth Hormone Deficiency: How to Incorporate Guidelines into Clinical Practice - Continuing Education
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

1/25/20
UCSF CME
Pituitary Disorders: Advances in Diagnosis and Management
San Francisco, CA
Saturday January 25, 2020
Adult Growth Hormone Deficiency: How to Incorporate
Guidelines into Clinical Practice
Kevin C.J. Yuen, MD, FRCP(UK), FACE
Professor of Medicine and Medical Director
Barrow Neurological Institute Pituitary Center
St. Joseph’s Hospital and Medical Center
University of Arizona College of Medicine and Creighton School of Medicine
Phoenix, AZ
1
Disclosures
• Received research grants to Barrow Neurological Institute from Ionis,
Crinetics, Millendo, Corcept and Novartis
• Served on Advisory Boards for Pfizer, Novo Nordisk, Ipsen, and Corcept
2
1
1/25/20
What are Clinical Practice Guidelines (CPG)?
“Systematically developed statements to assist practitioner and patient
decisions about appropriate health care for specific clinical
circumstances.” (Institute of Medicine, 1990)
• Most of the content are derived from extensive literature reviews
• Reflects the state of the field at time of publication, and because changes in this
area are expected, periodic updates may be implemented
• Some recommendations may not be appropriate in certain situations
Bottomline: use CPG in conjunction with best clinical judgment
3
GRS Workshop in Australia
April 14-17, 1997
4
2
1/25/20
2007 Consensus Guidelines for
the Diagnosis and Treatment
of adults with GHD:
GRS, ESPE, Lawson Wilkins
Society, European Society of
Endocrinology, Japan
Endocrine Society and
Endocrine Society of Australia
5
2009 Medical
Guidelines for Clinical
Practice for GH Use in
GH-Deficient Adults and
Transition Patients:
AACE
6
3
1/25/20
2011 Evaluation and
Treatment of Adult GH
Deficiency Clinical
Practice Guideline:
Endocrine Society
7
2016 Hormone Replacement
in Hypopituitarism in Adults
Clinical Practice Guideline:
Endocrine Society
8
4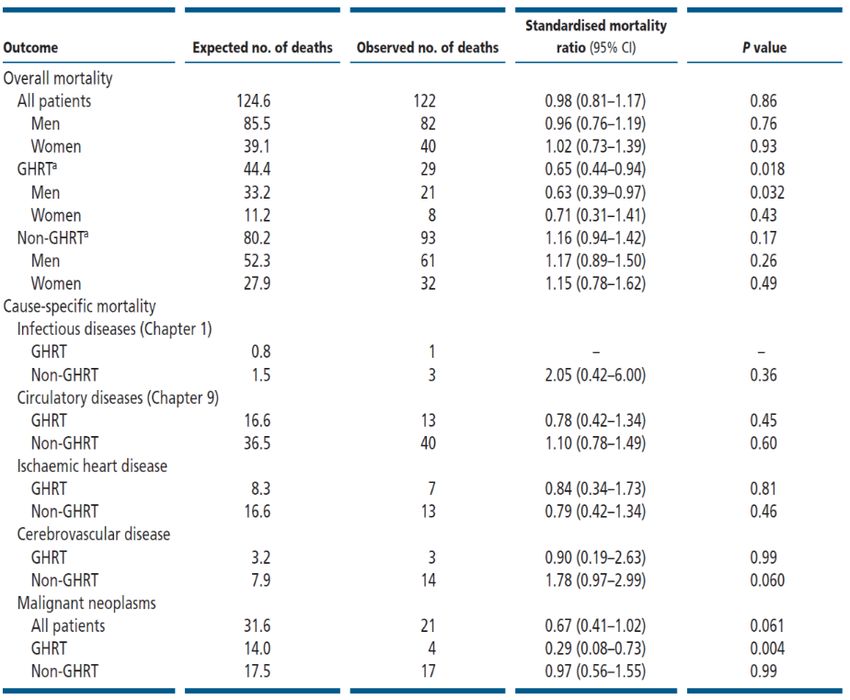
1/25/20
2019 Guidelines for
Management of GH
Deficiency in Adults and
Patients Transitioning from
Pediatric to Adult Care:
AACE
9
Why another CPG in 2019?
• Summarize current knowledge of GH stimulation tests
• Summarize the increasing evidence of beneficial effects and long-term safety of GH replacement
• Address skepticism about GH use:
- high cost of therapy and its true benefits
- difficulty conducting GH stimulation tests in the office
- concerns about safety of long-term therapy
- still a misconception of true adult GHD vs physiological decline in GH
• Highlight several sub-populations of patients described to be “at risk” for adult GHD
- how to test?
- when and how to treat?
• Review the literature of GH use for conception and pregnancy
• Dispel the myth of using GH for sports and aging
• New developments
10
5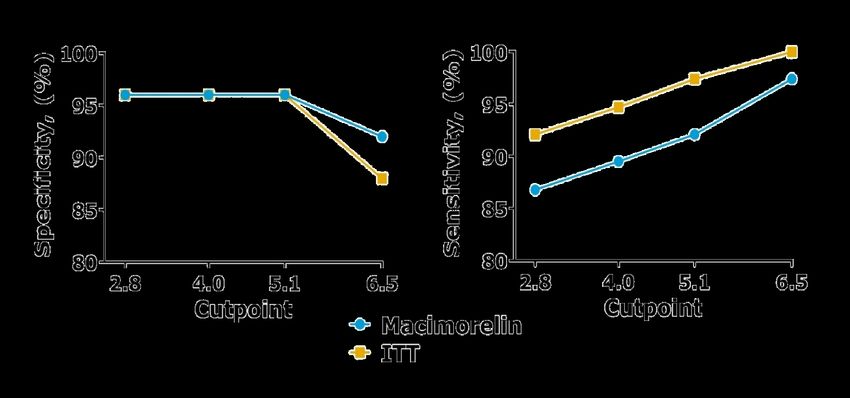
1/25/20
Outline summary of the new AACE 2019 CPG
• 58 numbered recommendations:
- 12 Grade A (21%), 19 Grade B (33%), 21 Grade C (36%), and 6 Grade D (10%)
• 13 question-based sub-sections
• 357 references:
- 51 (14%) EL 1 (strong)
- 168 (47%) EL 2 (intermediate)
- 61 (17%) EL 3 (weak)
- 77 (22%) EL 4 (no clinical evidence)
11
Case 1: 57 y/o male with NFPA
• TSS 3 years ago and SRS 2 years ago
• Now has TSH and ACTH deficiencies (on stable doses of
Levothyroxine and Hydrocortisone)
• IGF-I SDS -1.5
• Healthy, except for possible childhood febrile seizures
• Presents with a 10 lb (4.5 kg) weight gain over 6 months,
and persistent fatigue
• Family history of osteoporosis, hyperlipidemia and cancer
Read on the internet and would like to be considered for GH
12
6
1/25/20
Case 1 discussion points
• Why treat adult GHD?
• Who to test for adult GHD?
• Use of appropriate GH stimulation tests and cut-points
• Interactions between GH and concurrent GCs and thyroid hormone
• Safety concerns associated with long-term GH replacement
• Use of GH for anti-aging
13
Why treat adult GHD?
Body composition
• lean body mass
• ¯ fat mass
Bone
• total body bone mass
• BMD
• Effects require >18–24 months treatment
Aerobic exercise capacity
• VO2 max (most studies)
Quality of life (QoL)
• in some aspects of QoL (proportional to degree of baseline impairment)
Improved surrogate CV risk markers
?Decreased mortality risk
BMD, bone mineral density; QoL, quality of life.
Simpson H et al. Growth Horm IGF Res 2002;12:1–33.
14
7
1/25/20
Potential impact of untreated GHD vs benefits of GH
replacement on CV risk
UNTREATED ADULT GHD REPLACEMENT
CV RISK FACTORS
CONVENTIONAL SURROGATE CV RISK MARKERS
Lipids (total cholesterol, LDL, TG) ¯ CRP ¯
Glucose intolerance/hyperglycemia Pro-inflammatory cytokines (IL-6, TNF-a) ¯
β-cell function ¯ Adipokines (adiponectin , leptin /«) «¯
Insulin resistance ¯ Pregnancy-associated plasma protein A ¯
Metabolic syndrome ¯ Coagulation system (pro-coagulation ) ¯
Endothelial dysfunction ¯
INCREASED INDIVIDUAL CV RISK IMPROVED
CRP, C-reactive protein; CV, cardiovascular; GH, growth hormone; GHD, growth hormone disorder; LDL, low-density lipoprotein; TG, triglyceride; TNF, tumor necrosis factor.
15
Life expectancy in adults with NFPA receiving
GH replacement therapy
CI, confidence interval; GH, growth hormone; GHRT, growth hormone replacement therapy; NFPA, non-functioning pituitary adenoma
Olsson DS et al. Eur J Endocrinol 2017;176:67–75.
16
8
1/25/20
17
Who to test for adult GHD?
Acquired Congenital
Skull-based lesions Genetic
Pituitary adenoma, craniopharyngioma, Rathke’s cleft cyst, Transcription factor defects (PIT-1, PROP-1, LHX3/4, HESX-1,
meningioma, glioma/astrocytoma, hamartoma, chordoma, PITX-2)
lymphoma, metastases GHRH receptor gene defects
Brain injury GH gene defects
TBI, sports-related head trauma, blast injury, perinatal insults GH receptor/post-receptor defects
Infiltrative/granulomatous disease Associated with brain structural defects
Single central incisor
Langerhans cell histiocytosis, autoimmune hypophysitis,
sarcoidosis, TB, amyloidosis Cleft lip/palate
Surgery to sella, suprasellar and parasellar region
Cranial irradiation
CNS infections
Bacterial, viral, fungal, parasital
Infarction/hemorrhage
Apoplexy, Sheehan’s syndrome, SAH, stroke, snake bite
Empty sella
Hydrocephalus
Idiopathic
Yuen KCJ, et al. Endocr Pract. 2019;25(11):1191-1232.
18
9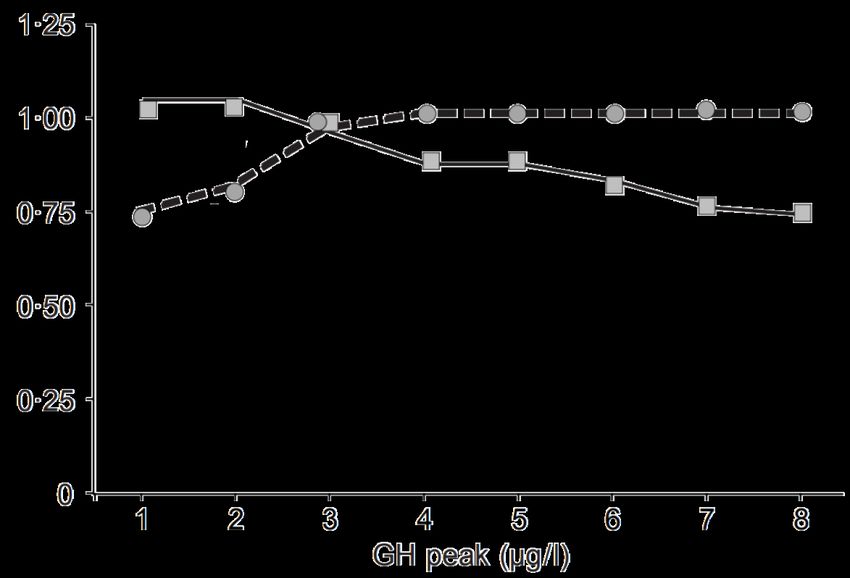
1/25/20
Pulsatile pattern of 24-hr GH secretion in a
30 y/o vs 60 y/o healthy adult vs an adult with GHD
25 Sleep
20 30 yo healthy adult
60 yo healthy adult
15
GH (µg/L)
Random points of Adult with GHD
overlap with GH levels
10 in healthy adults
05
0
09:00 21:00 09:00
Clock time
GH, growth hormone; GHD, growth hormone disorder.
19
Serum IGF-I levels throughout life
640
Men (n = 81)
320 Women (n = 71)
160
IGF-I (µg/L)
80 Normal range
40
IGF-I more reliable for
20 screening for diagnosis
in young adults
10
10 20 30 40 50 60 70 80 90 100
Age (years)
IGF, insulin-like growth factor.
Hilding A et al. J Clin Endocrinol Metab 1999; 84:2013–9
20
101/25/20
AACE 2019 CPG algorithm for testing adult patients with
clinical suspicion of GHD
Adult patient with clinical suspicion of GHD
Organic GHD Organic GHD
≥3 hormone deficiencies 0, 1 or 2 hormone deficiencies History of hypothalamic-pituitary tumors, surgery, cranial
irradiation, empty sella, pituitary apoplexy, traumatic brain
Low IGF-I (1/25/20
Previous GST studies suggesting the effects of central adiposity
and glucose intolerance in decreasing peak GH levels
Yuen et al. Pituitary 2013 Jun;16:220–30
Dichtel et al. J Clin Endocrinol Metab 2014 Dec;19:4712–9
Retrospective
Diri et al. Pituitary 2015 Dec;18:884–92
Wilson et al. Growth Horm IGF Res 2016 Feb;26:24–31
Hamrahian et al. Pituitary 2016 Jun;19:332–41 Prospective
GH, growth hormone; GST, glucagon stimulation test.
23
Mechanism of action of macimorelin
Macimorelin acetate
+ –
GHRH SRIF
Hypothalamus
+ +
Ghrelin
Pituitary
– gland
GH
–
Stomach
Liver
IGF
GH, growth hormone; GHRH, growth hormone-releasing hormone; IGF, insulin-like growth factor.
Camina JP et al. Endocrine 2003 Oct;22(1):5-12.
24
121/25/20
Features of the macimorelin test
Oral administration
Non-
parenteral
administration
Only 1.5 hours
4 blood draws
No hospitalization Less time Fewer blood
consuming draws
Well- No
contra-
tolerated indications
Garcia JM et al. J Clin Endocrinol Metab 2013;98:2422–9.
25
Macimorelin dosage and administration
1 Weigh your patient 2 Dissolve in water 3 Stir gently (for 2-3 minutes) 4 Calculate volume
X kg = X mL solution
(Patient (Macrilen
Quick Guide to (a small Quick Guide
weight) to
solution)
Administration amount of Administration
Example: A patient weighing
undissolved 70 kg will need 70 ml of
particles reconstituted Macrilen
≤120 kg=1 pouch 1 pouch=120 ml water will remain) solution.
>120 kg=2 pouches 2 pouches=240 ml water
5 Measure exact volume 6 Transfer exact volume 7 Administer solution 8 Draw blood samples
Use a syringe Transfer the Have patient
(without a exact drink the
needle) with Guide to required entire
Quick Guide to
Quick 30 45 60 90
graduations volume of volume of min min min min
in mLAdministration
to Macrilen Administration
Macrilen
measure the solution into solution in
exact volume drinking drinking glass Draw venous blood samples for
of solution. glass. within 30 GH determination at 30, 45, 60,
seconds. and 90 minutes.
EMA Macimorelin Aeterna Zentaris SmPC. Available at: https://www.ema.europa.eu/en/documents/product-information/macimorelin-aeterna-zentaris-epar-product-information_en.pdf,
Accessed 11 June 2019; FDA Macrilen Highlights of Prescribing Information. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/205598Orig1s000LBL.pdf Accessed 11 June 2019
26
131/25/20
Oral macimorelin GH test
Diagnostic accuracy and correlation analysis compared to the GHRH-arginine test
100
Sensitivity (true positive rate)
80 4.5 ng/ml: 90% sens;
79% spec; 15% misclass
60 2.7 ng/ml: 82% sens;
92% spec; 13% misclass
40
20
ROC AUC=0.923
0
0 20 40 60 80 100
100-specificity (false positive rate)
AUC, area under the curve; GH, growth hormone; GHRH, growth hormone-releasing hormone; ROC, receiver operator characteristics.
Garcia JM et al. J Clin Endocrinol Metab 2013;98:2422–9.
27
Peak GH concentrations in macimorelin and ITT stratified
by likelihood of having adult GHD
Validation Phase 3 study comparing with the ITT
MAC not evaluable at first
ITT evaluable ITT not try, evaluable on repeat
Intermediate 1%
High risk Low risk Controls on request evaluable twice
risk 9% 3%
ITT not
GH level (ng/ml)
repeated
6%
ITT evaluable MAC evaluable
at first try at first try
82% 99%
ITT (N=157) Macimorelin (N=154)
Now approved by the FDA and EMA*
• Greater pituitary GH secretion than the ITT
• Sensitivity (87%) and specificity (96%) with cut-point of 2.8 ng/ml vs ITT cutpoint of 5.1 ng/ml
• Highly reproducible and good safety profile
*Not commercialized yet in the EU.
ITT, insulin tolerance test.
Garcia JM et al. J Clin Endocrinol Metab 2018;103:3083–99.
28
141/25/20
Estimated specificities and sensitivities of macimorelin and ITT
A cut-off point of 5.1 ng/ml instead of 2.8 ng/ml, increases
sensitivity without decreasing specificity
ITT, insulin tolerance test.
Garcia JR, et al. Presented at ENDO 2019, New Orleans, March 24, 2019
29
Accepted GH cut-points (µg/L) for GH stimulation tests used in the
US by different consensus guidelines to diagnose adult GHD
GRS 2007 AACE 2009 Endocrine Society 2011 Endocrine Society 2016 AACE 2019
(Molitch et al.) (Fleseriu et al.)
ITT < 3.0 ≤ 5.0 < 3.0 to 5.0 ≤ 3.0 to 5.0 ≤ 5.0
GHRH-arginine
- BMI < 25 kg/m2 < 11.0 ≤ 11.0 < 11.0 < 11.0 No recommendation
- BMI 25-30 kg/m2 < 8.0 ≤ 8.0 < 8.0 < 8.0 (not commercially
- BMI ≥ 30 kg/m2 < 4.0 ≤ 4.0 < 4.0 < 4.0 available since 2008)
Glucagon
- BMI < 25 kg/m2 All patients < 3.0 All patients < 3.0 All patients < 3.0 All patients < 3.0 ≤ 3.0
- BMI 25-30 kg/m2 regardless of BMI regardless of BMI regardless of BMI regardless of BMI ≤ 3.0 or ≤ 1.0
- BMI ≥ 30 kg/m2 ≤ 1.0
Macimorelin Not commercially Not commercially Not commercially Not commercially ≤ 2.8*
available available available available
Arginine Not recommendations ≤ 0.4 No recommendations No recommendations No longer recommended
to be used
*5.1 µg/L may be considered in patients with high pre-test probability
30
151/25/20
Recommendations for starting GH doses in adults with GHD
AACE 2009 and 2019
GRS 2007:
Age 30 - 60 years - young men and women, start at 0.2-0.3 mg/day
Age < 30 years
- older individuals, start at 0.1 mg/day
0.2–0.3 mg/day - target IGF-I SDS < +2
0.4–0.5 mg/day
(higher for transition
and younger patients) Age > 60 years Endo Society 2011:
- age 30 – 60 years, start at 0.2-0.3 mg/day
0.1–0.2 mg/day - target IGF-I SDS between 0 and +2
• Use lower GH doses (0.1–0.2 mg/day) in Endo Society 2016:
patients with DM, obesity, and previous - age < 60 years, start at 0.2-0.4 mg/day
GDM - age > 60 years, start at 0.1-0.2 mg/day
• Target IGF-I SDS between -2 and +2 - target IGF-I SDS to the mid-range
31
Interactions between GH therapy and concurrent GCs
and thyroid hormone
GRS 2007, AACE 2009, Endo Society 2011, Endo Society 2016 and AACE 2019
GH therapy may unmask clinical central hypothyroidism and hypoadrenalism
levothyroxine and hydrocortisone doses
32
161/25/20
Safety concerns associated with long-term GH replacement
• DM and glucose intolerance – use low GH doses
• History of active malignancy and proliferative diabetic retinopathy -
contraindicated
• Strong family history of cancer – careful consideration
• Previous history of cancer – careful consideration, discuss with oncologist,
initiate > 5 years after cancer remission, and use low GH doses
• History of CVD – GH replacement exerts positive effects on some CV risk
markers
• Recurrence of pituitary adenoma – no increase in relative risk
• Cancer risk – no increased risk (possibly even reduced risk)
• Mortality risk – no increased risk (possibly even reduced risk)
Yuen KCJ, et al. Endocr Pract. 2019;25(11):1191-1232.
33
Use of GH for anti-aging
• No studies have assessed long-term (> 6 months) efficacy or safety of GH
for anti-aging purposes
• Meta-analysis of 31 studies in healthy elderly subjects reported small
changes in body composition but increased AEs (Liu et al. Ann Intern Med
2007;146:104-115), while animal studies have shown reduced life spans and
premature onset of age-related cognitive changes (Bartke A. World J Mens
Health. 2019;37:19-30)
Use of GH for marketing, distributing, or administration for any reason other than the
well-defined approved uses of the drug is illegal and strongly discouraged
Yuen KCJ, et al. Endocr Pract. 2019;25(11):1191-1232.
34
171/25/20
Case 2: 21 y/o male with panhypopituitarism due to
suprasellar germinoma
• S/p chemotherapy and cranial DXT
• On DDAVP, Hydrocortisone, and Levothyroxine
• IGF-I SDS -0.1
• Underwent Macimorelin test: serum GH levels
0.06, 3.22, 3.27, 2.84 and 1.29 µg/L
• Amenable to resume GH therapy
• Childhood GH dose was 2.0 mg/day
35
Case 2 discussion points
• When to retest and which test to use?
• To treat or not to treat? If treat, what dose to resume GH therapy?
• Safety concerns regarding long-term GH replacement
• Fertility and pregnancy
• Use of GH for sports
• Long-term adherence
36
181/25/20
AACE 2019 CPG algorithm for testing transition patients with
clinical suspicion of GHD
Adult patient with clinical suspicion of GHD
Organic GHD
Congenital defects 0, 1 or 2 hormone deficiencies
Genetic defects Idiopathic isolated childhood GHD or suspected
Low IGF-I (1/25/20
Safety concerns regarding long-term GH replacement
• Risk of secondary neoplasms in childhood cancer survivors
- increased risk more likely related to previous exposure to cranial irradiation
2018 Endo Society CPG (Sklar CA, et al. JCEM 2018) and 2019 AACE CPG recommend
carefully considering GH to childhood cancer survivors with confirmed GHD
39
AACE 2019 CPG recommendations on GH use during conception
and pregnancy
• Not approved by the FDA
• Several studies support use of GH while seeking fertility, and continuing
GH during pregnancy does not appear to impact mother or fetus
- Giampietro A, et al. Fertil Steril. 2009
- Vila G, et al. Fertil Steril. 2015
- Bassiouny YA, et al. Fertil Steril. 2016
- Correa FA, et al. J Endocr Soc. 2017
More data still needed on safety of GH use in women with GHD to assist conception
and during pregnancy before it can be routinely recommended
Yuen KCJ, et al. Endocr Pract. 2019;25(11):1191-1232.
40
201/25/20
Use of GH for sports
• GH improves body composition but may not improve strength, worsen
exercise capacity and increase AEs (Hermansen K, et al. Growth Horm IGF
Res. 2017;34:38-44)
• Detecting GH abuse is challenging
- short t1/2 of exogenous GH
- urine sampling of GH not viable
- what biomarkers to test for?
Use of GH for marketing, distributing, or administration for any reason other than the
well-defined approved uses of the drug is illegal and strongly discouraged
Yuen KCJ, et al. Endocr Pract. 2019;25(11):1191-1232.
41
Improving long-term adherence
• See some patients more frequently (“individualized care”)
• Provide electronic resources (cater to “the millennials”)
• Have an open and non-judgmental conversation with patient (ask “open-
ended” questions about adherence barriers)
• Review the risks of untreated GHD with the patient
• Review the benefits and safety of long-term GH replacement therapy
• RN to spend time reviewing the patient’s injection technique
• Medication reminder systems and longer duration of GH prescriptions
• Regular educational and motivational support
Bozzola M, et al. Horm Res Paediatr. 2014; 81(5):331-335.
Mohseni S, et al. J Pedistr Endocrinol Metab. 2018;3:13-20.
42
211/25/20
Why consider LAGH preparations?
Problems with daily GH injections
• Inconvenient, painful and distressing
• Non-adherence increases over time
• Life circumstances can interfere with adherence
By decreasing injection frequency, long-acting GH preparations may improve
adherence and thereby potentially improve clinical outcomes
43
Overview of LAGH preparations currently under development
Technology used Product (Company) Modification to the GH molecule Frequency of Current status
administration
Depot LB03002 (LG Life Sciences, Ltd)Microparticles containing GH incorporated into 7 days Approved and marketed in S Korea
sodium hyaluronate and dispersed in an oil base of for childhood GHD. Approved but
medium-chain TG not marketed in Europe.
Depot CP016 (Critical Supercritical carbon dioxide, formed when carbon 14 days (planned) Pre-clinical studies
Pharmaceuticals) dioxide exceeds its thermodynamic critical point,
used to create the depot
PEGylated BBT-031 (Bolder Biotechnology) Site-specific PEGylated GH analog 7 days (planned) Pre-clinical studies
PEGylated Jintrolong (GeneScience 40-kDa PEG linked to GH 7 days Approved in China for childhood
Pharmaceuticals, Ltd) GHD
Prodrug TransCon ACP-001 (Ascendis) GH transiently linked to carrier molecule via a self- 7 days Phase 3 in children completed and
cleaving linker, and releases GH unmodified presented, phase 3 in adults in
planning stages
GH molecule Somapacitan NNC0195-0092 Single point mutation in GH, with non-covalent 7 days Phase 3 in children, phase 3 and
bound to albumin (Novo Nordisk) albumin binding moiety attached extension study in adults
GH molecule AG-B1512 (Ahngook Recombinant human GH genetically fused to a 14-28 days (planned) Pre-clinical studies
bound to Fab Ab Pharmaceutical Co., Ltd.) polypeptide linker and an anti-HSA Fab antibody
GH fusion protein ProFuse GH (Asterion) GH-binding protein 1 month (planned) Pre-clinical studies
GH fusion protein GX-H9 (Genexine, Inc. and Hybridization of non-cytolytic immunoglobulin Fc 7-14 days Phase 2 in children and adults,
Handok, Inc.) portion of IgD and IgG4 pending phase 3 trial in adults
GH fusion protein LAPSrhGH/HM10560A (Hanmi Homodimeric aglycosylated IgG4 Fc fragment 7-14 days Phase 2 in children and adults
Pharmaceutical Co., Ltd.)
GH fusion protein MOD-4023 (Pfizer, Inc.) Carboxyl-terminal peptide of hCG β-subunit 7 days Phase 3 in children, phase 3 in adults
failed primary end-point and further
studies planned for pen devices
Yuen KC, et al. Expert Rev Endocrinol Metab. 2019 Nov 13:1-18.
44
221/25/20
Questions regarding LAGH preparations
• Where is the place of LAGH in relation to naïve GH-deficient patients and patients
already on daily GH?
• Are all the LAGH preparations the same?
• Will the effects of LAGH preparations be durable with long-term use?
• Any prolonged metabolic consequences and side effects?
• Can LAGH preparations with large molecular sizes penetrate all tissues equally?
• When to measure IGF-I levels and is it the same for all LAGH preparations?
• Are LAGH cost-effective?
• Will LAGH receive regulatory approval if convenience not accepted as an added
value?
• Will LAGH truly improve adherence and outcomes?
• Will the safety profile of LAGH be different to daily GH?
45
Summary of changes of AACE 2019 CPG compared to previous CPG
• Recently described non-tumoral causes of adult GHD
• More emphasis on clinical suspicion when ordering and interpreting GH stimulation
tests
• More emphasis on re-testing, how to re-test, and recommendations on re-initiation
and benefits of continuing GH therapy in transition patients
• Recommendations of BMI-specific cut-points for the GST and deleted the prior
recommendation of using arginine test for assessing adult GHD
• Recommendation regarding the place of macimorelin when testing for adult GHD,
and interpretation of its results
46
231/25/20
Summary of changes of AACE 2019 CPG compared to previous CPG
• Emphasizing the importance of standardized GH and IGF-I assays for diagnosis and
guiding GH dosing
• More detailed recommendations on initiation and monitoring of GH replacement
• Insufficient data to recommend routine GH use for conception and pregnancy
• Increasing data supporting the safety of long-term GH use
• Strong emphasis of NOT using GH for sports and aging
• Discussion of current status of LAGH preparations
47
Outstanding knowledge and treatment gaps
• Are the currently available GH stimulation tests reliable and accurate when
used in different types of GHD?
• Is there a better biomarker than IGF-I?
• What is the optimal IGF-I target to titrate GH doses to?
• How long to treat with GH?
• Safety data of GH > 20 yr follow-up
• Safety data of GH for fertility (male and female) and pregnancy
• Safety data of GH in the elderly (> 80 yrs)
• Optimal interval between completion of cancer treatment and initiation of
GH therapy
• Reliable diagnostic methodology in assessing GH misuse for unapproved
conditions
48
241/25/20
THANK YOU FOR YOUR ATTENTION!
49
25You can also read