AN EVALUATION OF COMMUNITY ENGAGEMENT STRATEGIES TO IMPROVE TRUST AND VACCINE CONFIDENCE - DIVA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
An evaluation of community engagement
strategies to improve trust and vaccine
confidence
A review of the Primary Healthcare for Travellers Projects in
Ireland
Michael Buggle
Word count: 13,784 (includes in-text citations; excludes cover page, contents, and
references)
Communication for Development
Two-year master
15 Credits
HT 2020
Supervisor: Josepha WesselsTable of Contents
Abstract ................................................................................................................................. 4
Introduction ........................................................................................................................... 5
Vaccine hesitancy ................................................................................................................ 5
Irish Travellers .................................................................................................................... 6
COVID-19 ............................................................................................................................ 6
Research objectives and key questions.................................................................................. 7
Background ............................................................................................................................ 8
Who are Irish Travellers? ..................................................................................................... 8
Health inequalities among the Traveller population ............................................................... 8
Primary Healthcare for Travellers Project .............................................................................. 9
Relevance to C4D .............................................................................................................. 10
Literature review .................................................................................................................. 11
Community engagement .................................................................................................... 11
Best practices ................................................................................................................ 12
Types of community-led interventions............................................................................. 12
Gaps in CE research ........................................................................................................ 15
Vaccine hesitancy .............................................................................................................. 16
Vaccine hesitancy terminology and discourse ................................................................... 16
Vaccine hesitancy determinants and models .................................................................... 18
Vaccine hesitancy and Irish Travellers .............................................................................. 20
Solutions to vaccine hesitancy ........................................................................................ 20
Theme of trust .................................................................................................................. 21
Vaccine hesitancy and trust ............................................................................................ 21
Community engagement and trust .................................................................................. 22
Conclusion ........................................................................................................................ 23
Theoretical framework .......................................................................................................... 25
Trust as a theoretical framework ........................................................................................ 25
Methodology ........................................................................................................................ 30
Methodological approach .................................................................................................. 30
Research methods ............................................................................................................. 30
Semi-structured interviews ............................................................................................. 31
Data analysis..................................................................................................................... 33
Validity ............................................................................................................................. 34
Page 2 of 58Ethical or philosophical considerations ............................................................................ 34
Challenges..................................................................................................................... 34
Results and discussion ........................................................................................................... 35
Inherent trust ................................................................................................................... 36
Earned trust ...................................................................................................................... 37
Tailoring to needs of community ..................................................................................... 39
How trust is built ........................................................................................................... 40
Signs of trust ................................................................................................................. 41
Access to vaccines ............................................................................................................. 41
Limitations and future research .......................................................................................... 42
Conclusion ........................................................................................................................... 42
References ........................................................................................................................... 45
Appendices .......................................................................................................................... 49
Page 3 of 58Abstract
Public trust in vaccines has shifted over time and at different rates based on vaccine and
contextual factors. Despite the known benefit for public health, recent studies across many
countries have indicated a perceived ‘hesitancy’ toward vaccines, namely those for the
prevention of COVID-19. The decision to vaccinate can be complex, involving psychological
and socio-cultural factors that can cause vaccination barriers. Trust or confidence, both in a
vaccine and the people behind the vaccine, has been identified as a core element impacting
people’s willingness to vaccinate, particularly if a vaccine is new.
Community engagement (CE) methodologies have been recommended in previous reports
as strategies to improve trust among populations in health services such as vaccinations.
The following study evaluates the applicability of CE strategies, such as the community
health worker model, in addressing factors of vaccine hesitancy (VH) by leveraging trusted
relationships. The study looks at the approach of a model used to address health
inequalities among the Traveller Population in Ireland as a case study of community
engagement methodologies within an ethnic minority population.
Using the Primary Healthcare for Travellers Projects (PHCTP) as a case, this study evaluates
how trust as a by-product of CE can play a role in improving vaccine confidence. The study
examines elements of CE strategies that can be applied to the Irish Traveller context to
address any potential COVID-19 vaccine confidence issues. Interviews with several
stakeholders uncover perspectives on the PHTCP model and CE strategies generally and
their impact on vaccine decision-making. These stakeholders include primary health
workers of the PHCTP teams in Dublin, and ‘expert’ stakeholders consisting of public health
specialists with experience in the field of VH. The study shows that the PHCTPs have built
up significant trust levels with the Traveller community and may be effective in improving
vaccine confidence in a COVID-19 vaccine in the future.
Page 4 of 58Introduction
Vaccine hesitancy
Vaccine hesitancy (VH) challenges the efficacy of immunisation programmes all over the
world; however, some solutions are available. VH is defined by the SAGE working group
(WG) on VH as ‘a delay in acceptance or refusal of vaccines despite availability of
vaccination services’ (MacDonald, 2015, p.4162). Despite widespread coverage, pockets of
hesitant people remain across Europe, impacting vaccines’ ability to guarantee immunity
within populations (Butler et al., 2015). Lack of trust has been reported as a factor of
hesitancy among minority ethnic populations in the UK, where racism and discrimination
have ‘eroded’ trust in the healthcare system (Razai et al., 2021, p.1). In overcoming the
challenge, communication for development methodologies such as community engagement
(CE) and social mobilisation have been described as having a role in encouraging uptake and
ensuring necessary trust in vaccines and those providing vaccines (Goldstein et al., 2015). In
an article on the effectiveness of health communication in immunisation strategies,
Goldstein et al. (2015) outline the importance of ‘who’ the messenger is and ‘where’ the
message comes from in situations where trust is a key driver of vaccine hesitancy (p.4213).
Unfortunately for health service providers, a one-size-fits-all approach to VH is argued to be
ineffective. Many public health academics and practitioners argue for the importance of
adapting communication and interventions to the given community’s local nuances (ibid.).
In the absence of a panacea, and to provide a tool that could help with the process of
adapting interventions to the needs of local communities, WHO Europe developed a VH
diagnostic tool and intervention framework called Tailoring Immunisation Programmes (TIP)
(Butler et al., 2015; World Health Organisation [WHO], 2019). The TIP framework seeks to
identify subgroups of populations within regions with low vaccine uptake. The approach
focuses on the community’s barriers and motivators to vaccines and recommends
combining a multi-disciplinary approach to tailor interventions that leverage these
motivators and minimise the barriers to achieve the greatest uptake (WHO, 2019, p.4). This
model has been adopted in several countries in Europe to date, addressing hesitancy in a
range of different populations unified by varying characteristics. Some of the groups
included those categorised by religion, ethnic background, immigration status, or even
Page 5 of 58pregnancy. For example, among an Orthodox Jewish community in the UK, the TIP model
was applied to improve vaccine coverage rates in the North London community (Letley et
al., 2018).
Irish Travellers
One such subgroup with anticipated sub-optimal immunisation rates is the Irish Traveller
(Traveller) community based in Ireland (All Ireland Traveller Health Survey [AITHS], 2010).
Despite feeling that health services are generally accessible; Travellers typically engage less
with preventive health services, including immunisation, compared with the settled
community in Ireland (ibid.). This lower immunisation coverage was underscored by a
previous measles outbreak among the traveller community in 2009 (Gee et al., 2010). The
reasons for avoiding preventive health services are evident from the All-Ireland Traveller
Health Study (2010), a collaborative piece of research developed in partnership with many
Traveller peer researchers and organisations across Ireland. In this study, it was shown that
over half of travellers feel discriminated against in a health service setting, and less than half
(41%) trust their general practitioners, a significant contrast to the majority population
(83%) (AITHS, 2010, p.79).
The Primary Health Care for Travellers Projects (PCHTP) was set up in 1995 to improve the
health inequalities faced by travellers, and to improve health service utilisation by
Travellers. The PHCTP developed a community health worker model of health promotion
among the community to help engage Travellers in essential health services such as
childhood immunisation (Keyes & McCabe, 2005). This primary healthcare model is
discussed further in the background section and is referenced throughout as a CE case
study.
COVID-19
The issue of VH is currently pertinent for many public health experts, policymakers, and
members of the public around the world due to the ongoing COVID-19 pandemic. As many
governments and health systems continue to roll out a COVID-19 vaccine in 2021, they will
also be cognisant of addressing hesitancy towards uptake to ensure the efficacy of the
Page 6 of 58inoculation. Herd immunity for COVID-19 has been estimated at 67% coverage, meaning
that two-thirds of people will need to receive the vaccine for it to be effective within the
population (Kwok, 2020). Compliance from the population to get vaccinated ‘relies on a
personal risk-benefit perception’ that is vulnerable to ‘misinformation’ regarding safety or
efficacy (Dror, 2020, p.775). This vulnerability poses a potential threat to the effectiveness
of inoculation programmes. It should be noted that the primary concern with the COVID-19
vaccine reported in some surveys, which is consistent with other new vaccines, is the safety
and the fear of potential side-effects (Dodd et al., 2021). Conversely, the primary reason for
those who are motivated to vaccinate is ‘to protect themselves and others’ (ibid., p.162).
Research objectives and key questions
This study will evaluate elements of CE strategies, including the community-led model of
PHCTP, to see if they may be useful in ensuring trust in future COVID-19 vaccines. These
learnings may also be useful for other minority groups within Ireland and abroad that may
have comparably lower trust levels in vaccination, as is the case in the UK (mentioned
above). The study will seek to answer the following research questions:
Primary research question:
1. What elements of community engagement strategies are important in determining
trust for vaccines within the Irish Traveller community?
Secondary research questions:
1. Which community engagement strategies are best-suited to improve confidence in a
COVID-19 vaccine among Irish Travellers?
2. How might the existing Primary Health Care for Travellers Project (PHCTP) be useful
in influencing acceptance of a COVID-19 vaccine for the Irish Traveller community?
3. How might these learnings be useful to COVID-19 vaccine immunisations strategies
for Travellers and other minority groups in Ireland?
To provide additional context, the PHCTP model will be explained further and how its
community-led development model is relevant to the field of Communication for
Development. Following that, relevant literature will be presented on the topics of VH and
Page 7 of 58CE. This grounding in relevant literature on the core topics will provide the basis for the
theoretical framework, which is presented as cross-cutting theory within the core fields (CE
and VH). Theories of trust both interpersonally and the trustworthiness of communication
are presented as models to underpin the analysis and discussion section. The research
methodology is discussed including participant selection criteria, study sample, validity, and
potential strengths and weaknesses of the method. Results from six semi-structured
interviews will be presented and interpreted in a discussion using the findings from the
literature review and theoretical framework to situate the results within the broader field of
study. Finally, the conclusion will offer a reflection on the research objective and pose a
possible resolution or need for further research.
Background
Who are Irish Travellers?
Irish Travellers are an indigenous population that has been present in Irish culture for
centuries. There are an estimated 36,224 Travellers currently in Ireland, spread across much
of the country, with the majority living in urban areas near cities (Central Statistics Office
(CSO), 2016; AITHS, 2010). Historically nomadic people moving from place to place,
Travellers differentiate themselves from the so-called majority ‘settled’ population in
Ireland (Relenthford & Crawford, 2013). In recent years, however, the majority (83%) of the
Traveller population have moved to fixed residences, although despite this, they remain
somewhat socially isolated from wider society in their tight-knit communities (CSO, 2016;
Relenthford & Crawford, 2013).
Health inequalities among the Traveller population
Travellers across Ireland face stark health inequalities when compared with the majority
settled population. Most notably, Travellers have a significantly lower life expectancy than
the settled community, 70 vs 82 in women and 62 vs 77 in men, respectively (AITHS, 2010,
p.96). Low life expectancy in males is partly due to high external causes of death, including a
Page 8 of 58high suicide rate when compared with the settled community. The disproportionate impact
of morbidity and mortality among the Traveller population is explained in the AITHS as
being, in part, due to lifestyle risk factors such as smoking and poor diet explained as a
coping strategy of hardship and disadvantage endured, as well as other psychosocial factors
including distrust in others and general poor mental health (p.160).
Although Travellers self-report as attending health services e.g., general practitioners (GPs),
roughly as much as the general population, their confidence or trust in healthcare
professionals is significantly lower (AITHS, 2010). Only 41% of Travellers have complete faith
in their GP, compared with 83% of the general population (p.79). One explanation for this
distrust in health services is the high level of discrimination faced by Travellers within health
service settings and throughout society (p.150). Many advocates in the Traveller community
see this discrimination from the broader society as the primary contributor to ill-health
within the community (p.165). This lack of trust in healthcare professionals poses a potential
communication challenge for the health promotion efforts within the community (AITHS,
2010).
Primary Healthcare for Travellers Project
The Primary Healthcare for Travellers Projects (PHCTP) began initially to serve the Traveller
community’s unmet needs in terms of healthcare services and health literacy. In their report
on Primary Health Care as a model of good practice, Keyes and McCabe (2005) outline a
rationale for ‘special consideration’ for Traveller health solutions, namely because Travellers
are a distinct ‘cultural group’ and share different perceptions of health to the general
population. They also recognised the different health issues and health behaviours present
among the community, and thus the need for different and innovative approaches to solve
them (Keyes & McCabe, 2005, p.15).
Along with capacity building and some advocacy efforts, one of the primary objectives of the
PHCTPs has always been to ‘liaise and assist in the dialogue between Travellers and Health
service providers’. This emphasis on bridging the gap between the health service and the
Page 9 of 58community has focused on aligning important communications to the community
preferences and capabilities. This includes acknowledging barriers such as low literacy levels
and creating health promotion materials that are optimised for Travellers, often
incorporating symbols and shapes in printed materials to make them more accessible. Due
to this, much of the work that PHCTPs do is based around interpersonal communication
between Travellers and the Traveller Community Health Workers (Keyes & McCabe, 2005).
What do the projects do?
The PHCTPs coordinate and implement several health services within the community and
take part in continuous health education training. They spend a portion of their time doing
‘fieldwork’, meeting with community members at their homes, collecting information on the
status of the community’s health to tailor their future efforts (Keyes & McCabe, 2005). The
PHCTPs are a valuable platform for data collection for external studies on community health
and were leveraged during the AITHS in 2010. Since 2015, the PHCTPs have also prioritised
improving uptake of childhood vaccinations with young mothers in the community. The
PHCTPs ensure mothers have the latest information about immunisation schedules and
emphasise the importance of vaccinating for the baby’s sake, but also the good of the
community. The PHCTPs also work with the older Travellers in the community to promote
the benefits of the influenza vaccine each flu season (Pavee Point, 2017).
Relevance to C4D
At its core, the PHCTP model is a community development project aimed at fostering social
change among Travellers toward more positive health behaviours e.g., vaccinating new-born
babies against measles, mumps, and rubella or attending a breast check. The PHCTP model
is grounded in communication for development (C4D) style theories and principles. As
outlined by Manyozo (2012), CE as a concept was adopted in development fields to ‘provide
the relevant political economy in which grassroots participation’ can occur (p.154).
Grassroots participation is evident within the PHCTP model and the wider Traveller health
structure more broadly. Several local, regional and national representative committees
organise projects based on the community’s needs (AITHS, 2010). While CE does not directly
Page 10 of 58equal communication for development, it is a core tenet at the centre of many C4D
strategies.
Literature review
Relevant literature on VH and CE have been reviewed to help situate the study within
previous research. A series of systematic reviews with a focus on CE strategies in health
interventions are assessed. Similarly, relevant findings of community health worker
approaches are discussed to present a well-rounded view of the methodology in relation to
health services such as immunisation. Some gaps in the current research have been found
and are also discussed.
Community engagement
The literature analysis focused on several syntheses of CE intervention studies that sought
to improve a range of health-related outcomes to differing degrees. Given the breadth of CE
research, systematic reviews were useful to provide a synopsised understanding of the
methodologies in improving health behaviours. Individual public health and social science
studies were also reviewed to help provide contextual examples of interventions using CE
strategies concerning health service utilisation, vaccine acceptance and/or Traveller
populations.
Overall, the literature showed that CE strategies can be effective in improving the success of
health interventions, but there is a lack of evidence to show which strategies are most
effective and how they achieve effectiveness (Cyril et al., 2015; Haldane et al., 2019; Milton
et al., 2011; O'Mara-Eves et al., 2015).
In their analysis of CE studies in disadvantaged populations, Cyril et al. (2015) showed that
CE models can be effective in improving health and health behaviours. Effectiveness was
shown in interventions that were designed in collaboration with communities and
implemented ‘through effective community consultation and participation’, while
incorporating the ‘voice and agency’ of the community within the planning, design, and
implementation phases of the intervention (p.2; p.7).
Page 11 of 58In a multi-method and multi-phase study on CE and health service utilisation, McFadden et
al (2018) examined the importance of trust between communities and health services. They
analysed the impact of trust in the service provider and service user relationship and put
forth a conceptual framework that suggested a strong correlation between trust in services
and efficacy of interventions or usage. The study explained the importance of trust in
ensuring service utilisation and as a result, improved health (McFadden et al., 2018).
In a meta-analysis of public health interventions adopting CE strategies among minority
populations, O’Mara-Eves et al. (2015) examined studies using a ‘theories of change’
framework to look at specific CE models as potential ‘moderators of effectiveness’ (p.2). The
study shows that CE interventions have a positive impact on a range of health outcomes and
behaviours. They found insufficient evidence to point to one strategy over another but
identified several themes and provided recommendations based on these, which are
discussed further below (O’Mara-Eves et al., 2015).
Best practices
Despite challenges regarding the conclusiveness of evidence favouring one CE method over
another, several elements emerged from the literature that may be applied to improving
vaccinations among an Irish Traveller population. One primary approach or strategy is the
inclusion of community members in the delivery of an intervention. It should be noted that
the design and planning phases also benefit from community involvement and collaboration
particularly in assessing and understanding the needs of the community (Cyril et al., 2015).
Carr et al. (2014) advocate for, in their systematic review of outreach programmes to
improve Traveller health, for the further prioritisation of outreach work for socially excluded
populations such as Traveller communities (p.7). They noted that ‘outreach’ can be an
effective strategy in reaching communities and defined outreach as ‘alleviating physical and
ideological gaps between service and users’ (MacKenzie et al., 2005, p.2, as cited in Carr et
al., 2014). Emphasis in this study is therefore placed on literature exploring the delivery of
services to improve trust and engagement in health behaviours.
Types of community-led interventions
Community member-led or lay-delivered interventions have shown success in improving
health behaviour outcomes by offering additional reliability and empathy to service users. In
Page 12 of 58their review of CE strategies in reducing health inequalities for disadvantaged populations,
O’Mara-Eves et al.’s meta-analysis of health behaviour, health consequences, self-efficacy,
and social support outcomes looked at a variety of CE approaches and their impact on the
outcomes of the study. In the study, there was no conclusion as to what type of CE had
greatest effect as a moderator of efficacy, however it should be noted that the delivery of
services or intervention through lay community members showed the greatest added
improvement with some caveats. The reason for this increased improvement, O’Mara-Eves
et al. note may be due to ‘credibility, expertise, or empathy that community members can
bring’ (p.10). Further to this, they also noted that the studies included in the meta-analyses
that were lay member focused had smaller sample sizes which may have resulted in
increased 1:1 time, which has been shown to be more effective at increasing engagement
(ibid.).
Lay health educator
Research has shown that lay health worker models have been effective in promoting both
child and adult immunisation (Lewin et al., 2010). Focusing on ‘outreach programmes for
health improvement’ specifically, in Carr et al.’s (2014) multi-method systematic review into
the efficacy of community outreach in improving the health of Travellers, a realist synthesis
is developed to examine ‘explanations of how, for whom and in what circumstances
outreach works best’ (p.10). The ‘by whom’ and ‘how’ categories of analysis are particularly
relevant for this study on trust as they look at the characteristics of the person delivering
the intervention, as well as the nature of how the information or intervention is
disseminated. The impact of these characteristics on trust are discussed in the discussion
section.
While lay health educator models have demonstrated to be effective due to added empathy
shown, this approach has also indicated to be effective in ensuring cultural suitability of
behaviour messages. Cyril et al.’s (2015) systematic review aims to understand which CE
methodological approaches showed most effectiveness and which ‘components are
acceptable, feasible and effective with disadvantaged groups’ (p.1). In this study, it is shown
that community health worker models can be effective in ‘fostering improved health
behaviours’ by ‘enhancing the relevance of messages’, and in improving the efficacy and
Page 13 of 58feasibility of interventions as community members can overcome possible ‘cultural and
access barriers’ (p.6-7).
It should be noted that through the available evidence in the study, Cyril et al.
recommended accompanying lay health advisors with other strategies to ensure success
(2015). The systematic review also highlighted the effectiveness of including community
members at the research phase of the intervention, and that this has added benefit in terms
of focus group recruitment and research protocol design. Many of the studies included in
the analysis adopted a community-based participatory research (CBPR) approach which
seeks to connect research and practice through engaging the community in the research
design and implementation. Combining community health worker models with CBPR was
useful in several studies, with needs assessments being considered as adding positive
outcomes (Cyril et al., 2015).
Community outreach and trust
The literature has shown that interventions adopting outreach strategies have success in
improving immunisation behaviours among Traveller populations specifically for a variety of
reasons (p.37; Lewin et al, 2005). As mentioned, the characteristics of the messenger are
important in understanding the level of trust an outreach worker has in a given community.
It is pointed out that those of similar ethnicity experience greater levels of trust due to close
social ties within the community, however being a Traveller does not automatically earn the
trust of the community (ibid.). Carr et al. put forth a suggested trust score typology (see
below) based on the studies within their analysis. They suggest that outreach workers
‘already acquainted with families’ as well as professionals with ‘long standing relationships’
have high trust scores, whereas a professional with no previous relationship with
community members may have a low trust score (p.45). This shows that although ethnicity
and being a member of the community is important, the quality of the interpersonal
relationships are more important in determining the effectiveness of the health outreach
intervention.
1. Outreach worker is a highly connected member of the Community, already
acquainted with the extended family group – high trust
Page 14 of 582. Outreach worker is a Traveller with no immediate connection to the network –
neutral trust
3. Outreach worker is a professional or semi-professional with a long-standing
relationship with the Traveller Communities targeted – high trust
4. Outreach worker is a professional without a prior relationship with the Traveller
Communities targeted – low trust
5. Outreach worker is a settled lay person with no prior relationship to the
Community – low trust.
Typology of trust in outreach workers working with Traveller populations (Carr et al., 2014,
p.45)
In addition to the above, McFadden et al. further explore the relationship of trust between
Traveller populations and health service utilisation, they find that trust can enhance CE
strategy effectiveness in immunisation promotion (2018). It has been reported in the
literature that Traveller communities can have levels of mistrust toward healthcare
professionals due to previous bad experiences. This is both common in the UK and in
Ireland, where, as mentioned, trust in GPs can be as low as 41% due to a several reasons
including feeling of discrimination or no previous relationship (AITHS, P.76; McFadden et al.,
2018). Mcfadden et al. (2018) aimed to examine how to increase trust between Travellers
and health services and found that many solutions were on the service supply side e.g.,
ensuring Traveller patients have repeated exposure to the same GP to build a trusting
relationship. However, they also found that working with community organisations, and in
the PHCTP context, lay health worker projects, this could also help ensure engagement with
services. Although the study is limited in detailing how CE can enhance trust specifically, it
does advise that any intervention avoid being tokenistic, and ensure commitment to
following through with results (McFadden et al., 2018).
Gaps in CE research
Although some efficacy for CE strategies in improving health interventions, such as
vaccinations, has been shown, many of the systematic reviews raised concerns about the
robustness of evidence across CE studies. In many instances, studies were unable to show
Page 15 of 58the impact of the CE model or approach on the intervention itself, but merely that in some
cases the interventions with CE elements were more successful (Cyril et al., 2015; Haldane
et al., 2019; Milton et al., 2011; O’Mara-Eves et al., 2015; Swainston & Summerbell, 2008). A
lack of longitudinal evidence is cited as a reason for lack of robustness in the studies, with
many focusing on evaluation at a single point in time (Milton et al.; O’Mara-Eves et al.;
Haldane et al.). Swainston & Summerbell’s meta-analysis points out that many studies in its
review did not have control data which limits the ‘inferences that can be drawn about
effectiveness’ (2008, p.5). Similarly, the research aims of CE health intervention studies did
not focus on the specific impact of the CE element of the intervention, and therefore could
not show with certainty how CE strategies improved the effectiveness (O’Mara-Eves et al.;
Swainston & Summerbell).
In addition to data being non-robust, literature shows a challenge with the evaluation of CE
interventions due their complex nature, as well as limitations of methods or tools for
assessing the impacts of CE components specifically (Cyril et al., 2015; Haldane et al., 2019;
Milton et al., 2011; O’Mara-Eves et al., 2015; Swainston & Summerbell, 2008). Health
interventions with CE aspect often ‘operate on non-linear pathways’ meaning that the
evaluation is less straightforward compared to ‘simple dose-response relationships’
(O’Mara-Eves, 2015, p.17). It is also said that CE and health processes are ‘influenced by an
array of contextual factors’ and therefore it can be difficult to manage these variables
(Haldane, 2019, p.21). Due to the complexity and multi-faceted nature, many authors call
for more robust measurement ‘innovations’ to assess the efficacy of these interventions
(Cyril et al; Swainston & Summerbell).
Vaccine hesitancy
Vaccine hesitancy terminology and discourse
VH research is a relatively new (10-15 years) multi-disciplinary field and discourse that seeks
to understand and solve challenges to do with sub-standard vaccination coverage
(Habersaat & Jackson, 2020). The evidence gathered in the field comes from a range of
disciplines including ‘psychology, sociology, medical anthropology, social and political
Page 16 of 58science, and communication’ (ibid., p.36). Given the breadth of the field, there are
contested topics among interdisciplinary colleagues, including the use of the word
‘hesitancy’, as well as some of the core factors impacting VH. There are also elements that
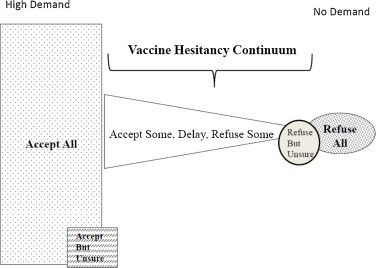
are largely accepted, such as the spectrum of vaccine acceptance and refusal (see fig.1), and
the idea that VH is determined by both contextual and vaccine-related factors.
VH is a debated term primarily due to the semantics of the word ‘hesitancy’, as well as some
of the core categories of contributing factors that were put forth by the SAGE WG. In a
review of the SAGE WG on VH, MacDonald (2015) acknowledge the potential ‘negative’
connotations of the term in addressing a health challenge. When trying to define the term,
vaccine ‘confidence’ is a term that was considered by the group and is used by many in the
field to capture trust relationships between user and service provider, as well as perceived
safety and efficacy of the vaccine (Larson, 2011). However, while ‘confidence’ is useful to
explain some elements of lack of acceptance of vaccines, the Sage WG argued that it does
not fully cover other factors such as individuals’ perceived risk of disease or issues relating
to vaccine access (MacDonald, 2015). In their report the SAGE WG define VH factors as
‘complacency, convenience and confidence’ (see fig.2) (MacDonald, 2015, p.4163).
.
There is a consensus in the literature that VH is vaccine and ‘context specific’ meaning that
different vaccines can impact hesitancy to different degrees and similarly, that different
populations or communities can have different perspectives for different contextual reasons
(Jackson & Habersaat, 2020; Karafillakis et al., 2018; MacDonald, 2015; Larson et al., 2014;
Dubé et al., 2013;). This is a significant point for those developing interventions to minimise
VH in that, it is necessary to understand the context as well as the specific vaccine
perceptions of a particular population. This is evident in the case of the HPV vaccine in
countries across Europe, where hesitancy manifests among parents and young adults due to
a variety of reasons. In their systematic review, Karafillakis et al. show that these
determinants of VH can be different depending on the location, e.g., in the UK ‘perceived
insufficient and inadequate information’ was regarded as the most common contributor for
hesitant populations. This differs in France, where fear of vaccine side-effects was the most
common determinant. In Spanish studies, doubt in the effectiveness drove hesitancy
(Karafillakis et al., 2018, p.4).
Page 17 of 58Fig. 1 “Continuum of vaccine hesitancy between full acceptance and refusal” (MacDonald,
2015)
Vaccine hesitancy determinants and models
As discussed, VH is complex and therefore has a range of determinants that are influenced
by vaccines and contexts. As part of their report, the SAGE WG endeavoured to categorise
these determinants to aid future research and interventions around VH. The three Cs model
(confidence, complacency, and convenience; see fig. 2) was conceptualised to provide a
simple yet broad framework to better understand the determinants of VH. Confidence in
the model is defined as trust in a) the effectiveness and safety of the vaccine, b) the system
that delivers the vaccine, including in healthcare professionals and c) the government or
policy makers who make decisions about vaccines. Complacency relates to the perception of
benefit versus risk in deciding to vaccinate, with many additional sub-factors impacting that
weighing up exercise. Paradoxically, the success of a vaccine can cause greater complacency
among individuals, who feel that the threat of the disease has lowered and therefore may
be less likely to decide to vaccinate (p.4162). Finally, convenience refers to physical access
and ability to vaccinate, as well as less physical elements such as health literacy and vaccine
offerings, including information being culturally sensitive or tailored to a group (MacDonald,
2015, p.4162).
Page 18 of 58Another approach to categorise determinants, or ‘root causes’ as they are referred, of under
vaccination, is the five A’s taxonomy developed by Thomson et al (2016). In response to
varying existing models, Thomson et al. developed the approach to provide a more
‘practical’ framework that practitioners can use to identify and address causes of sub-
optimal uptake. In their narrative review, they identify previous VH interventions as being
ineffective, and acknowledge that the social and behavioural factors that influence VH can
be complex. Their review argues that in many instances where VH is identified as the
primary cause of sub-standard uptake, other reasons may be of greater importance,
including vaccine delivery. To move away from ‘conceptual’ models to a taxonomy that can
be better translated into ‘practice’, the five A’s provides a ‘pragmatic methodology to
identify primary root causes of vaccination coverage gaps, and then to support development
of strategies in closing these gaps’ (p.1018).
The above models offer useful parameters for the development of strategies to address sub-
optimal vaccination coverage, or VH. In the context of this study, which seeks to look at how
CE strategies can have a positive effect on trust of vaccination, it is pertinent to identify
areas within these taxonomies that CE can have the greatest added impact for the Irish
Traveller population. This will be explored further under the theme of trust in this literature
review.
Page 19 of 58Fig. 2 “Three Cs” model of vaccine hesitancy. (MacDonald & SAGE WG, 2015)
Vaccine hesitancy and Irish Travellers
Although there are no studies focusing on VH or sub-optimal uptake of vaccines among Irish
Travellers in Ireland, some UK studies look at barriers and motivators of vaccine uptake, as
well as health service utilisation generally (which includes immunisation). Although there is
some evidence to say that immunisation rates can be low among Traveller populations
(Dixon et al., 2017), an in-depth qualitative study with members of four Traveller
communities in the UK shows that many of the barriers and facilitators towards vaccines are
comparable with the general public (Jackson et al., 2017). This study (Jackson et al.) noted as
being the first of its kind, looked at vaccination uptake factors and Travellers. It highlighted
that acceptance of vaccines and access to health services are primary motivators and
barriers respectively (2017). The study showed that much of the negative or cautionary
beliefs around vaccines such as whooping cough or influenza are ‘historical’ and are not
present in the younger parents of the community (p.13). The primary challenge identified by
respondents in the study was around registering with a GP without a fixed address and
booking appointments with offices. The study also underlined the importance of ‘trust in
health professionals, particularly GPs’ and other healthcare workers including health visitors
(like community health worker model except not lay people). These relationships were
viewed to be important influencing factors among Traveller communities but are also
important in the wider population. It should be noted that these relationships may be
particularly pertinent for the Traveller community as they have a history of not accessing
preventive care and of experiencing discrimination in health settings (AITHS, 2010). This is
also underscored by the close-knit communities that Travellers live in. The communities are
characterised by trust and have a long-standing oral tradition, leaving the community
potentially vulnerable to spreading of false or misleading information (Jackson et al., 2016,
p.103).
Solutions to vaccine hesitancy
The literature on strategies or interventions to address VH is disparate but does show some
core principles that should be considered for future interventions. While no one
Page 20 of 58intervention is recommended over another, several best practices have emerged in the
literature. Outlined by Habersaat & Jackson (2020), the use of community health workers
has been shown to be effective to provide ‘clear and balanced information about
vaccination risks and benefits’ (p.36). In their review of vaccine demand and acceptance,
Habersaat & Jackson also note the importance of the ‘face-to-face interaction’ between
health workers and individuals on the decision-making process, and how that can be useful
in building trust and providing reassurance (2020, p.37). In a ‘review of published reviews’
Dubé et al. (2015) present evidence on strategies to address VH and to improve vaccine
acceptance. They note that there is no strong evidence to suggest which strategy is most
effective, due to wide-ranging data and disparate studies. Despite this, they highlight the
significance of the healthcare provider relationship as ‘the cornerstone of maintaining
confidence in vaccination’ (Dubé et al., p.4201). This is echoed in the SAGE WG report
(MacDonald, 2015) and in the article by Leask et al. (2014) that identifies ‘provider
interactions’ as being a primary influencing factor on VH, along with social norms (p.2601).
They suggest ‘confident recommendations combined with respectful engagement,
narrative, and personalised approaches’ to help reassure parents or individuals when
making vaccine decisions (ibid., p.2601). In the context of Irish Travellers, where trust in
health care professionals may be lower due to discrimination faced or from previous poor
experiences, bridging or improving that relationship is key, and therefore building or
rebuilding trust in that dyad.
Theme of trust
Vaccine hesitancy and trust
As discussed, VH encompasses a broad range of factors that can contribute to indecision
around, or refusal of, vaccines. Outlined as part of the three Cs model (MacDonald, 2015),
confidence is one of the primary factors identified as impacting VH. As indicated in this
literature review, the confidence subset of the model is characterised by trust. This can refer
to individuals’ trust in the safety of the vaccine itself, their trust in the provider of the
vaccine, their trust in the messenger of vaccine information (which can include a health care
professional or community health worker), as well as trust in the policy makers involved in
Page 21 of 58delivering the vaccine programme. Low trust in these areas can negatively impact on
vaccine confidence. It should be noted that all factors within the three Cs model are
important to consider with respect to VH. However, within the parameters of this study,
confidence is particularly applicable given that CE methodologies have been considered as
strategies to garner public trust in addressing potential factors of VH (MacDonald, 2015).
Equally, within the Irish Traveller population, considering the goals of the PHCTP in bringing
health services to the community, trust is an important vehicle for service delivery, including
immunisation.
As mentioned, public trust in vaccines plays a significant role in ensuring the success of
vaccine interventions. Several key determinants play a role in ensuring that trust is built or
maintained. In an appeal to the vaccine community, Larson et al (2011) discuss the
‘confidence gap’ that has enlarged in years gone by due to waning trust in vaccinations.
Although primarily concerning childhood immunisations, Larson and colleagues illustrate
several possible explanations for this downturn in trust, including fear over vaccine safety,
new media and the democratisation of media, and the range of vaccines (p.527). In
identifying determinants of public trust, Larson et al (2011) apply the learnings from a study
of environmental-risk communication by Peters et al (1997), which provides an overview of
factors that influence the ‘extent to which an individual or institution’ is trusted (Larson at
al., 2011, p529.). To analyse perceptions of trust in risk communication for environmental
issues, Peters et al (1997) showed strong evidential support for their hypothesis that trust,
and credibility are influenced by: ‘perceptions of knowledge and expertise; perceptions of
openness and honesty; and perceptions of concern and care’ (p.43). Addressing public trust
deficits can be complex, however several studies have pointed to CE strategies for their
potential in ‘garnering’ trust. It is also highlighted, as is consistent with all components of VH
strategy, that they ‘need be locally tailored’ to the needs and concerns of the local
population (MacDonald, 2015; Larson et al., 2011, p.533).
Community engagement and trust
As mentioned in several studies above, CE can be a useful strategy to ensure public trust in
health services including in vaccinations, and in those distributing or recommending them
(Kallafinakis et al., 2018; McFadden et al., 2018; MacDonald, 2015). Trust has been
Page 22 of 58associated with higher utilisation rates of health services, as well as ‘improved health
behaviours’ (Ozawa & Sripad, 2013, as cited in McFadden et al., 2016, p.2). CE strategies
have shown promise in enhancing this trust between service and user, particularly in
marginalised populations such as Irish Travellers, where CE methods can ensure services are
delivered in a culturally appropriate way (O’Mara-Eves, 2014; McFadden, 2016). In their
multi-phase analysis of trust in health services among the Traveller population, McFadden et
al. (2018) identify trust in healthcare professionals as a ‘facilitator’ of trust, and the
importance of this relationship in building confidence in the system.
It is also useful to explore CE and trust within the dyadic relationship as a potential solution
to factors of VH. As outlined in the literature review, community health outreach strategies
have also shown to be effective in garnering trust in health services including immunisation
among Traveller populations (Carr et al., 2014). Trust within interpersonal relationships may
have a positive impact in addressing factors of VH such as low confidence. This has been
shown in the case of the healthcare professional and service user relationships, as well as
with health workers generally (Dubé et al., 2015). Interventions adopting outreach
strategies had success particularly when the deliverer of the outreach was a person with a
high trust score, as indicated in the typology by Carr et al (2014). This could be an ‘outreach
worker [who] is a highly connected member of the Community’ or a professional with a
‘long-standing relationship with the community’ (p.45). In the context of the Irish Traveller
population, the GP relationship can lack trust due to previously mentioned factors, including
bad experiences and services being culturally insensitive (AITHS, 2010). In this regard,
outreach workers or lay members of the community provide a trust bridge between the
community members and important health services such as immunisation.
Conclusion
The literature has shown that CE strategies focused on community outreach have been
reported to improve public trust in vaccinations by leveraging trusted sources and focusing
on tailoring health promotion to needs of the communities. Several suited strategies have
been identified as being particularly applicable to the case of improving trust in vaccines
among Irish Travellers. Included in these strategies are those leveraging the interpersonal
relationships of community health workers, including peer health educators and outreach
Page 23 of 58workers. Overall, the literature shows that CE strategies demonstrate effectiveness in
improving the success of health interventions, but there is a lack of robust evidence to
concretely show which strategies/approaches are most effective and how they achieve
effectiveness (Cyril et al., 2015; Haldane et al., 2019; Milton et al., 2011; O'Mara-Eves et al.,
2015).
The VH literature covers a range of disciplines including ‘psychology, sociology, medical
anthropology, social and political science, and communication’ (Habersaat & Jackson, 2020,
p.36). There are a variety of determinants of VH that are said to be unique to the context
and the vaccine itself. The term ‘hesitancy’ is a debated term and is described by some as
laden as it encompasses several broad topics including core determining factors as outlined
by the SAGE WG on VH, confidence, convenience, and complacency. Alternative models
have been suggested that aim to provide more practical assessments of the contributing
factors sub-optimal vaccination, including Thomson’s five A’s taxonomy (Thomson, 2012).
Models also exist to try address VH, including the previously mentioned TIP model which
uses the COM-B model to assess individual and contextual factors of VH (Habersaat &
Jackson, 2020).
Several cross-cutting themes are present in the literature presented on CE and VH. Most
pertinent of these for this study on vaccine confidence among the Traveller community is
the theme of trust. Combining how the two concepts intersect with trust can help explore
how the PHCTP model can impact potential VH among the Traveller community toward a
COVID-19 vaccine. From the above discussion, it is shown that trust can play an important
role in ensuring vaccine confidence, and in particular the impact of key dyadic relationships
on that trust, e.g., with lay healthcare workers or doctors. It is also understood that a
primary concern of the COVID-19 vaccine specifically is around its safety and the fear of
side-effects, therefore a potential lack of confidence in it. Couple this with the possible low
trust levels of travellers in their GPs, as outlined in the AITHS (2010). For the reasons and
evidence outlined, the subsequent theoretical framework for this study focuses on the
Confidence element of the core theories underpinning it e.g., trust. The subsequent section
provides a grounding theory in trust, borrowing from a widely cited model in the field of
Page 24 of 58organisational management (Mayer et al., 1995), as well as similar interpretations of trust in
the context of environmental risk communication (Peters et al., 1997).
Theoretical framework
To analyse the relationship between the two core concepts of this study, CE and VH, trust
will be explored to provide a framework to guide the analysis of results in the discussion
section. In this study, CE methodologies have been explored with an emphasis on peer- or
lay person-led approaches. The concept and study of VH has also been discussed along with
determinants of and strategies to address it. It has been illustrated that a lack of trust can
contribute to VH in the form of low confidence as indicated by the three Cs model
(MacDonald, 2015). Conversely, leveraging trustful relationships or trusted sources can help
address hesitancy and reassure hesitant people of concerns they may have (Larson et al.,
2011). This section explores a theoretical model of trust, and subsequent studies on the
topic and the most pertinent elements within trust for the specific context.
Trust as a theoretical framework
There are several trust frameworks that are useful to underpin the analysis of the empirical
data in this thesis. Borrowing from the field of organisational management (Hurley, 2006;
Mayer et al., 1995) and environmental risk communication (Peters, 1997) respectively, this
section will outline useful frameworks with which to better understand the potential benefit
of the PHCTP in ensuring trust in a COVID-19 vaccine.
Mayer et al.’s Integrative model of organizational trust (1995) will be outlined first. Although
the study was intended for use in an organisational setting, the model has been applied in
many varying fields, including communication, sociology, and healthcare (Schoorman et al.,
2007). It is a well-cited and robust presentation of trust and trustworthiness, which the
other two mentioned studies (Peters, 1997; Hurley, 2006) are drawn from. The purpose of
Mayer et al.’s study was to present a ‘model of trust of one individual for another’, the
authors clarify in a subsequent article, that the model is also intended for trust in groups or
organisations (Schoorman et al., 2007). The integrative model of organisational trust differs
Page 25 of 58You can also read