Angela Coladonato, MSN, RN, NEA-BC Tina Maher, BSN, RN, NE-BC Kathy Zopf-Herling, MSN, RN-BC
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Leveraging IT to Support a Re-engineered Discharge Process
Angela Coladonato, MSN, RN, NEA-BC
Tina Maher, BSN, RN, NE-BC
Kathy Zopf-Herling, MSN, RN-BC
All speakers have completed commercial bias disclosure forms
and do not have any conflicts of interest.
January 2013
Disclosures
• It is the policy of Corexcel and IMNE to ensure fair balance,
independence, objectivity, and scientific rigor in all
programming.
• In compliance with the American Nurses Credentialing Center
(ANCC) and the Accreditation Council for Pharmacy Education
(ACPE), it is the policy of Corexcel and IMNE that faculty
disclose all financial relationships with commercial interests
over the past 12 months.
• Corexcel’s provider status through the ANCC and IMNE’s
provider status through the ACPE, are limited to educational
activities. Corexcel, IMNE, ANCC and ANCC do not endorse
commercial products.
1
Objectives
• Understand the current discharge process and its impact on
readmissions
• Discuss three components of a re-engineered discharge process
• Articulate ways in which IT can support the discharge process
• Review the discharge process and how it is used in daily
practice
• Describe the impacts of a re-engineered discharge process
2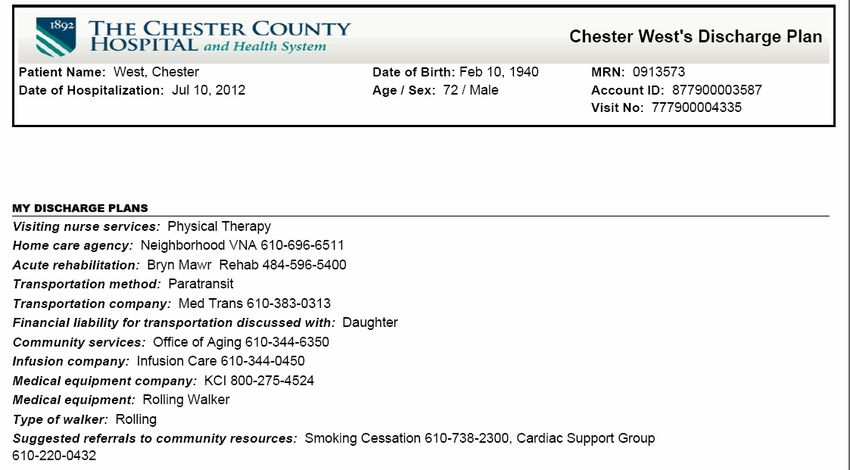
Agenda
• Current state of discharge nation-wide.
• Project RED – History and purpose at TCCH
• Soarian Re-Engineered Discharge Project
– Goals
– Multi-disciplinary inputs to the new Discharge Plan
– Outputs- “My Discharge Plan” (Patient and facility Version)
– Identification and management of high risk patients
– Outcomes so far
• Questions/Discussion
3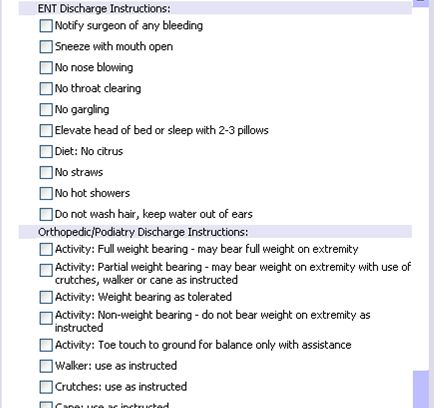
Discharge: the “Perfect Storm" for
Patient Safety
The hospital discharge is non-standardized and
frequently marked with poor quality.
• Loose Ends
• Communication
• Poor Quality Info
• Poor Preparation
• Fragmentation
• 20% of Medicare patients readmitted within 30 days
• Only half had a visit in the 30 days after discharge
N Engl J Med 2009 2;360(14):1418-28.
4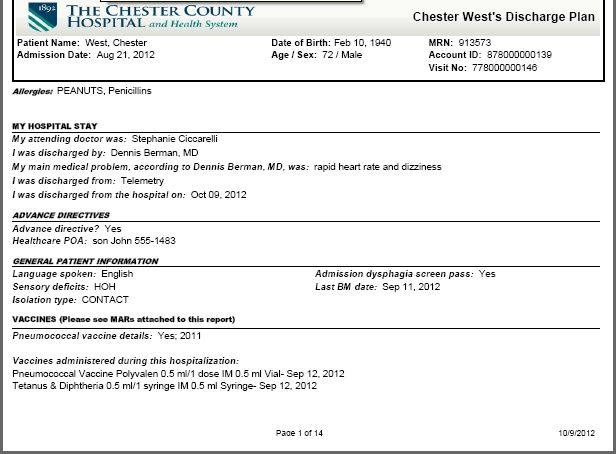
Other references:
• “…the last place patients want to end up after a hospital stay is right
back in the hospital…millions of patients are readmitted to hospitals
each year, and many of those admissions could have been
prevented…on average, 8 minutes of conversation occurs about how to
care for oneself at home, so it is no surprise that patients end up in
trouble..” (AHRQ 2011)
• More than 1/3 of required appointments for follow up not completed
(Moore et al. Archives of Internal Medicine. 2007;167:1305-11)
• 41% of inpatients discharged with a pending test result
• 37% actionable and 13% urgent
• 2/3 of physicians unaware of results (Roy, et. al. Annals of Internal
Medicine. 2005; 143(2):121-8.)
• Patients are not prepared at discharge: 37% able to state
the purpose of their medications; 42% able to state their
diagnosis (Mayo Clinic Proceedings. August 2005; 80(8):991-994.
5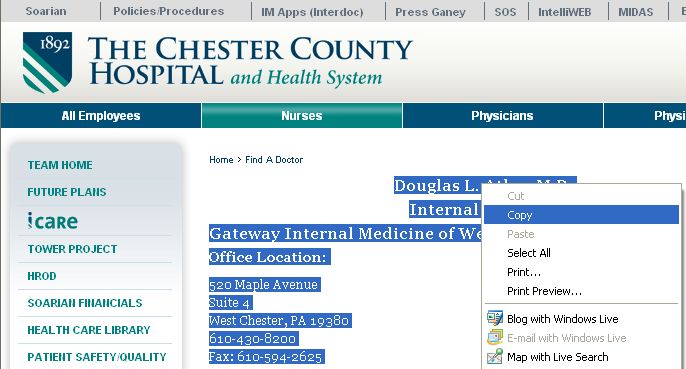
Our Story: 2011-2012
• Dr. B. Jack/AHRQ- the national RED Roll-Out Pilot
Project
• TCCH asked to be one of 11 hospitals to participate nationally
• Answer the following questions:
• Does the Project RED 11 Element Checklist work in the real world?
• Can the Project RED 11 Element Checklist be used more efficiently?
• June 2011 site visit; Dr. Jack, Boston Implementation team, AHRQ
• CHF patients discharged to home from Telemetry = pilot population
• Pilot year: summer 2011-2012
6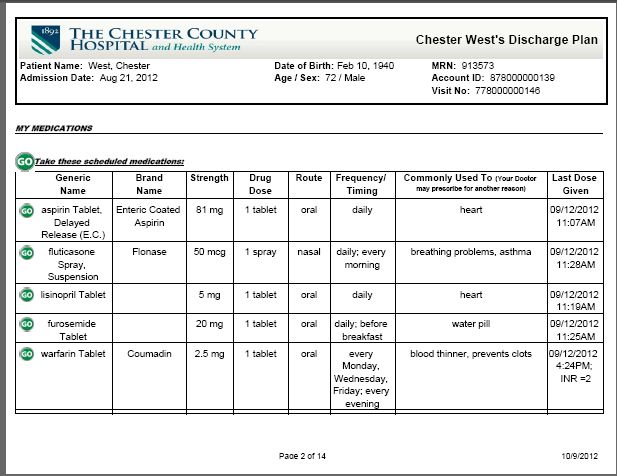
Readmission Rate Data during pilot - FY11 vs. FY12
• All Telemetry Patients
with a Primary
Diagnosis of CHF at
Discharge
• 30 Day Readmissions
7
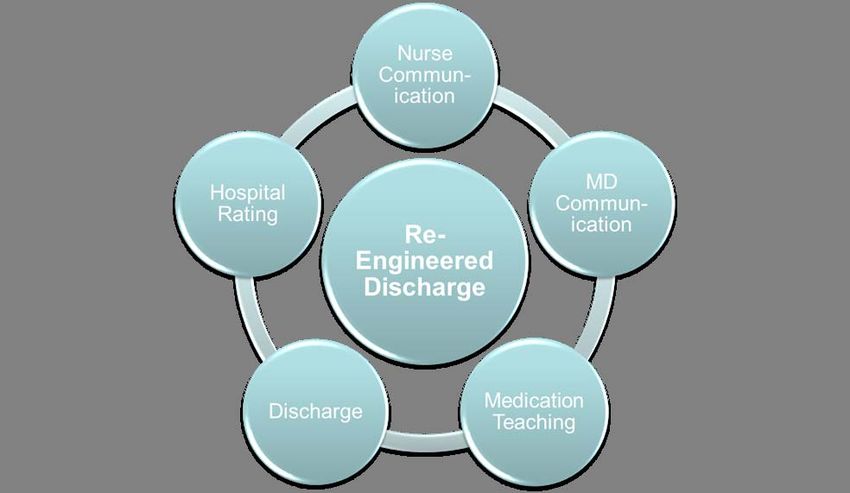
RED & HCAHPS : Enhancing Communication 8 8
Adopted by National
RED Checklist Quality Forum as Safe
Practice-15
1. Make appointments for follow-up medical appointments and post
discharge tests/labs.
2. Plan for the follow-up of results from lab tests or studies that are
pending at discharge.
3. Organize post-discharge outpatient services and medical
equipment.
4. Identify the correct medicines and a plan for the patient to obtain
and take them.
5. Reconcile discharge plan with national guidelines.
6. Teach a written discharge plan (AHCP) the patient can understand.
7. Educate the patient about his/her diagnosis.
8. Assess the degree of the patient’s understanding of this plan.
9. Review with the patient what to do if a problem arises.
10. Expedite transmission of the discharge summary to clinicians
accepting care of the patient.
11. Provide telephone reinforcement of the Discharge Plan.Our Story: Personalized Plan
10List of Medicines: Why & How
11TCCH Clinical Pharmacists: Medication Teaching
Brand Why am I What do I need
Name taking this med? to look for?
too much can cause liver damage (read OTC labels),
Tylenol pain, fever higher doses for long periods can increase warfarin
effects
Ventolin,
ProAir, breathing problems, asthma "rescue" inhaler, fast heart beat, chest pain/pressure
Proventil
Dizziness ,HA, avoid grapefruit juice, alcohol,
Uroxatral enlarged prostate, kidney stones
changes in sex ability
Zyloprim gout/high uric acid upset stomach, rash/skin irritation
Xanax anxiety, "nerves" drowsiness, dry mouth
Cordarone,
abnormal heart rhythm constipation, sensitivity to sunlight (wear sunscreen)
Pacerone
Elavil mood, migraine, nerve pain sedation, dry mouth, avoid grapefruit juice
12Our Story : Appointment Calendar
13Re-Engineered Discharge: TCCH Expansion 2012-2013
• Pilot project was a success.
• Biggest challenge= biggest opportunity!
– Replication of the AHCP in Soarian; collaboration once more!
• RED 11 element Checklist worked; what is TCCH model?
• Re-Engineer the discharge experience for all; additional
interventions for some
• TCCH Re-Engineered Discharge: 5 Core RED Principles
– Discharge planning begins Day 1 ………………all TCCH patients
– “My Discharge Plan” …………………………all TCCH patients
– Teach-back methodology …………………………all TCCH patients
– Follow-up apts. ……………………………………High Risk patients
– Follow-up phone calls …………………………High Risk patients
14Re-Engineered Discharge: TCCH Expansion 2012-2013
• Staff education on discharge and teach back methodology
• High Risk patients: F/Up Apts.
– Unit Coordinators own the process
– Patient/family interaction & the MD offices—huge value!
• High Risk patients: F/Up phone calls
– Modified script from the Project RED pilot year; 48-72 hours after D/C
– Access the medical record ; document the call
– CV Nurse Navigator, Paramedics and Clinical Pharmacists
– Content to date: medication clarification, transition support & compliments
• Volunteers & transport staff: discharge at curb-side
– Reinforce importance of “My Discharge Plan” as TCCH says “good-bye”
15 15Goal of Soarian Re-engineered Discharge
• Leverage our already existing electronic
interdisciplinary documentation and processes to
create patient friendly discharge instructions:
–Make the small RED pilot scalable to benefit all of our
patients.
–No niche system
–No double documentation and re-work for staff/physicians
• Leverage Soarian work flow engine to identify high
risk patients and help ensure that key activities occur,
such as making appts and post discharge phone
calls.
16Goal 1: Patient friendly discharge instructions
The discharge plan that the patient receives is created from electronic
interdisciplinary documentation that is captured in the natural course
of providing care:
• Uses ADT information- Demographics
• Uses CPOE orders
• Uses Case Management -facility plans, VNA, DME, etc.
• Uses Discharge Medication Reconciliation
• Uses Nursing Documentation- MAK, Discharge Instructions, Shift
Assessments, ADLs, Vital Signs
• Unit Coordinators pull in follow-up contact information; make appts
• Discharge Instructions Library
• Nutritionists, Diabetes Nurse Educators, NPs, PAs, RT, PT/OT can add
discharge instructions too!
• Facility/VNA “version” has additional clinical data
17Input: Case Management
18Input: Clinicians via discharge instruction order sets
19Specialty addendums can easily be added
20Unit Coordinator Role
• Unit Coordinators add follow-up appointment information-
addresses, phone numbers, time frame, and, for high risk
patients, make these appointments in consultation with the
patient and family.
– This made possible due to successful CPOE and MAK
implementation that reduced amount of time spent in order
transcription.
• We were able to insert links into the assessment form so
that physician office locations and contact information
could be readily found and inserted into the form (and
eventually the report)
21Patient Ed form- last chapter for discharge: nurse and
others enter specific instructions/appts
22Populating follow up physician contact information
23Find the clinician, cut and paste!
24Nurses and other disciplines add instructions- free text
or templated information.
25Text block library for templated “last licks” instructions
26Nurses Role
•Nurses are responsible for patient education throughout the
patient’s hospitalization. They use teach back methodology and a
variety of tools, such as Lexicomp, ExitCare, total joint booklet,
etc.
•At discharge, they add final discharge instructions individualized
for the patient- either free text or from a document library. These
become part of the discharge plan given to the patient.
•Nurses coordinate discharge, so help to ensure that the
discharge plan given to the patient is complete and accurate.
•Nurses also review the final discharge plan with the patient
before discharge.
27Physicians, Nurses, Pharmacists: Medication Section
•Clinicians complete discharge medication reconciliation in
Soarian, which will inform the patient what medications they
should continue at home.
•Nurses administer medications in MAK, which populate the last
dose taken
•Pharmacists pre-built “Commonly Used to” for top 400
discharged medications.
28Discharge Medication Reconciliation and MAK
29Nurses contribute some Clinical Data from Shift Assessments
30Creating the Report Specs for the Discharge Plan
31Report Specs: Identifying the look back period
3233
Discharge Plan Features
• Labels are in Patient Friendly language. For example,
Physician enters “discharge diagnosis” in Soarian,
but the label on the report is “My main medical
problem, according to Dr. Smith was:”
• Visually designed to be easy on the eye and
welcoming.
• Change from historically, where we gave patients very
important information in a manner that was
overwhelming.
• Large Font and Landscape orientation
• Lots of Page Breaks so that (for example) the
medication chart starts on a new page
34First page- vaccines and general info about hospital
35Clinician Orders inserted into the document
36Medication instructions- DMR with MAK last dose time and
common use of medications
37Yield and Stop signs for PRN and stopped meds.
38Instructional material inserted into document or typed in free text.
39Case Management “section”
40Appointments section
41Calendar included if appts made.
42Final product
For SNF/VNA – all the patient stuff plus more!
43First page- some added sections on Advance Directives, general
patient information.
44Added sections for the “Nursing Home/VNA” version
45Last set (within 24 hours) of vitals signs, O2
46Part 2: Management of High Risk Patients
• Automated work flow processes to identify patients at risk
(modified Boost criteria). List updates with changes:
• Poly pharmacy
• Recent 30 day Readmission, all cause
• Certain diagnoses: Stroke, AMI, HF, COPD, TIA, Psych
• Lives alone
• On Warfarin or Aspirin/Clopidogrel
• SNF patients excluded
• Creates high risk for readmission “order” visible in chart
47Part 2: Management of High Risk Patients
•Populates a report showing all high risk patients on the
unit/hospital and reason for inclusion
•Populates a report for after discharge phone calls:
48Lessons Learned
Need robust DC instructions in the text block “library”.
Engage physicians and staff early and include broader
stakeholders (we started with heart failure because they
were the pilot)
Get a top notch report writer! Make sure report runs
consistently and quickly.
Plan to spend a lot of time on report specifications and
testing.
Tell nurses to preview the report to ensure completeness
and accuracy.
Nurses will sometimes have to sign DMR as complete if
clinician forgot. Need to review report for accuracy
Allow that nurses will spend more time with patient at
discharge reviewing this discharge document.
49Summary
•From an organizational perspective, this project has been a
huge success, and has been well received by our patients:
– Minimized duplication and manual entry
– Refocused Unit Coordinator role on a value added patient activity.
– More robust, automated identification of patients at high risk for
readmission.
– Legible, and complete discharge plan that is well received by patients,
primary care physicians and receiving facilities.
–“My Discharge Plan—it’s like getting an award for discharge”
(patient quote)
•Huge paradigm shift for most clinical staff - instead of the
focus being on what they could enter into the electronic
medical record, they saw their normal documentation
actually used to produce something that would benefit the
patients.
50TCCH : HCAHPS Discharge Domain 51 51
RED & HCAHPS: Enhancing Communication
• New 2013 HCAHPS Care Transition Questions
• 4 point scale; from “Strongly Disagree” to “Strongly Agree”
– “During this hospital stay, staff took my preferences & those of my
family/caregiver into account in deciding what my health care needs
would be when I left”
– “When I left the hospital, I had a good understanding of the things I
was responsible for in managing my health”
– “When I left the hospital, I clearly understood the purpose for taking
each of my medications”
52TCCH : HCAHPS Care Transitions 53 53
Lots of positive feedback from community agencies:
I just wanted to let you know, how pleased we are with the ease of
discharge from your hospital to our community . Mrs. E was followed by
your SW, Linda. She communicated well with our SW. And the
information that was sent upon discharge was terrific and will follow the
resident home. We have commented among ourselves what a great
discharge program you have in your IT dept, and how helpful all this info
was.
It was a pleasure working with you, hope we can do again sometime in
the future.
Thanks,
Maggie
54Future Plans
Roll out to Maternal Child Health next week!
Continue to improve the discharge instructions library
Continue to improve the report (My discharge plan)
Add past med/surg history at request of SNFs
Move sections for maximum emphasis/readability
Add eprescribe transactions including quantity and refill
Try to find a way not to have to print and copy report
(patient portal/HIE/electronic patient signature and
electronic annotations.
Query review to make report run faster (completed)
Review newly available metrics reports and see where that
leads us
55Questions?
Download the Free Chapter
The Chester County Hospital and Health System:
Using Technology to Re-Engineer Discharge
Processes and Enhance Transitional Care
Part of the new series, Technology
in the New World of Healthcare,
from Siemens Healthcare.
www.usa.siemens.com/
techseries2013
57Contact Hour Credits
In order to receive contact hours for today’s session:
If you are eligible and would like to receive credit, please follow the instructions for completing the
evaluation. The instructions will appear on your screen momentarily. Or you can click on the evaluation
link located on the bottom of your viewing console.
Once you have completed the evaluation, you will have the ability to print out your certificate for
Continuing Nursing Education Credits of 1.0 contact hour offered by Corexcel.
For those of you in a group setting:
If you are viewing this webcast in a group setting and would like credits, you may do the following:
If you are not already registered, please be sure to register to view the playback of this event.
You can access the playback through the www.usa.siemens.com/clinicalgateway or through the
follow-up email that will be sent to all registrants. The playback will be available within a few days
after the conclusion of the live event.
Once you complete the evaluation and are eligible for credits, you may print your certificate.
These instructions will also be included in the follow-up email to all attendees.
Copyright © 2013 Siemens Medical Solutions USA, Inc. All rights reserved.Upcoming Siemens Webcast Topics
Contact Information:
Gail E. Latimer, MSN, RN, FACHE, FAAN, Vice President,
Chief Nursing Officer, Siemens Healthcare
gail.latimer@siemens.com
Upcoming Thought-Leadership Webcasts will be Announced Shortly.
- Check Siemens Clinical Gateway for more information
Missed a webcasts?
To view previous webcasts or to learn more on how healthcare IT can help tackle the challenges
clinicians face today visit Siemens Clinical Gateway at: www.usa.siemens.com/clinicalgateway
Copyright © 2013 Siemens Medical Solutions USA, Inc. All rights reserved.You can also read

















































