The One Stop Cervical Assessment Clinic: Clinical Guideline - V1.0 March 2021 - RCHT
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The One Stop Cervical Assessment
Clinic:
Clinical Guideline
V1.0
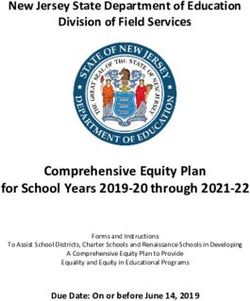
March 2021Summary: The “One-Stop” Cervical Assessment Clinic
Referral for Cervical Assessment
from:
Community / Internal Referral
on
2WW or 18 week pathway
Booking Office
Book directly onto “One-Stop” Cervical Assessment Clinic
Standard letter and Patient Information Leaflet sent to patient
“One-Stop” Cervical Assessment Clinic
Clinic Database pre-populated by clinic nurse
History taken by clinician
Further assessment as indicated
Clinical Examination Colposcopy Ultrasound Scan Hysteroscopy
Clinic Database
Details of assessment to be completed by clinician
Clinic letter generated for patient and GP
Letter uploaded into MAXIMS by admin staff
Clinic Outcome
Immediate Discharge Investigations Onward Referral
Reassurance Clinician to contact patient
Advice with results and plan
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 2 of 141. Aim/Purpose of this Guideline
1.1. This guideline applies to all patients referred to for assessment of their
uterine cervix, and the staff involved in their healthcare. The provision of a
dedicated clinic for patients with possible abnormalities of the cervix (some
of which may represent serious pathology such as cervical cancer) ensures
that all patients are seen within two weeks of referral, achieving equality of
access for all, regardless of the route of referral. Ensuring that patients are
seen by clinicians with an appropriate skill set means that consultations are
responsive to patients’ concerns and needs. The one-stop model reduces
fragmentation of care and delay, whilst promoting efficiency and protecting
scare healthcare resource.
Data Protection Act 2018 (General Data Protection Regulation – GDPR)
Legislation
The Trust has a duty under the DPA18 to ensure that there is a valid legal basis to
process personal and sensitive data. The legal basis for processing must be identified
and documented before the processing begins. In many cases we may need consent;
this must be explicit, informed and documented. We cannot rely on opt out, it must be
opt in.
DPA18 is applicable to all staff; this includes those working as contractors and providers
of services.
For more information about your obligations under the DPA18 please see the
Information Use Framework Policy or contact the Information Governance Team
rch-tr.infogov@nhs.net
2. The Guidance
2.1. Nationally, it is recommended that in individuals presenting with symptoms
of cervical cancer (for example post-coital bleeding or persistent vaginal
discharge that cannot be explained by infection or other causes), once “the
common causes of these symptoms have been excluded … the individual
must be referred for examination by a gynaecologist experienced in the
management of cervical disease”.
2.2. Patients may be referred for an assessment of their uterine cervix for a
variety of reasons. Referrals may be made on the two-week wait cancer
pathway, or on routine 18 week pathway. Referrals may or may not be in
line with existing local referral guidance, however it is recommended that all
referrals are accepted and processed swiftly in order to facilitate early
diagnosis of significant pathology such as cervical cancer. The patient’s
cervix may or may not have been clearly visualized by the referring
practitioner, and may or may not have been noted to be macroscopically
abnormal at the time.
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 3 of 142.3. The cervical assessment service at RCHT follows a “one-stop” model, with
the expectation that patients will not be followed-up in the cervical
assessment clinic, although they may require referral to another clinic after
initial investigation. Sufficient clinic provision allows all patients to be seen
within 2 weeks of referral.
2.4. The clinic is intended for two-week wait referrals for patients with suspected
cervical cancer and all “non-urgent” referrals to colposcopy clinic. The clinic
is not intended for patients referred from the cervical screening programme.
These referrals do not require vetting by a consultant or nurse colposcopist,
they should be booked directly by the booking office, and sent the standard
introductory letter and patient information leaflet (Appendix 3). This applies
to both referrals from the community and internal referrals via MAXIMS.
2.5. Each “One-Stop Cervical Assessment Clinic” has 2 “two-week wait” slots
and 6 “non-urgent/18 week pathway slots”. Two-week wait patients can be
booked into “non-urgent” slots as required to meet the two-week target.
Ideally, patients on a “non-urgent/18 week pathway” should be booked
within two weeks of referral, but it is acceptable to book their first
appointment up to 6 weeks from referral if required. Issues with clinic
capacity should be directed to the Lead Colposcopist / Lead Colposcopy
Nurse in the first instance. It is accepted that clinics may not always be “fully
booked” as this allows time for multi-modal “one-stop” assessment when
required.
2.6. The clinic database (currently Viewpoint) will be pre-populated by the clinic
nurse with the patient’s demographic information and the reason for the
referral by the clinic nurse prior to the clinic starting.
2.7. Reasons for referral may include:
Post-Coital Bleeding (PCB). The local RMS guidance suggests that
patients with “PCB only” should be referred for a cervical assessment,
and an up to date Chlamydia swab be taken as part of their initial
investigations. It is accepted that evidence for the positive predictive
value of PCB as a symptom of cervical cancer is poor. Local
guidelines suggest that patients with a “mixed picture of abnormal
bleeding” such as PCB with intermenstrual bleeding (IMB) should be
seen in the Menstrual Disorders Clinic (MDC). Often patients in the
latter group are referred for cervical assessment, rather than to the
MDC.
“Abnormal Cervix” on examination. The speculum examination may
have been undertaken for a variety of reasons e.g. routine cervical
screening, insertion/removal of IUCD or for symptoms such as
unscheduled/unexpected vaginal bleeding. The majority of the time,
the findings on cervical assessment will not be of concern, or
physiological in nature. The patient’s original health concern may
therefore still need to be addressed after their cervix has been fully
assessed.
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 4 of 142.8. Causes of PCB and “Abnormal Cervix”
Vulval, vaginal, cervical, endometrial cancer; rarely ovarian and non
gynaecological malignancies
Infective causes e.g. Chlamydia
Physiological e.g. cervical ectropion, Nabothian cysts
Iatrogenic e.g. scarring following previous LLETZ treatment
Local cervical cause e.g. benign cervical polyp
Menstrual disorders
Contraceptive problems
2.9. It may be helpful to conduct a quick “briefing session” before the clinic
starts. Staff may consider reviewing the referral letters to see what each
patient is likely to need in terms to outpatient procedures in order to ensure
that the clinic runs as smoothly as possible.
2.10.At the cervical assessment clinic the clinician will take a history to include
details of presenting symptoms, a menstrual history, obstetric history,
contraceptive history to include the patient’s desire for future fertility and a
cervical screening history.
2.11.The chlamydia swab result will be checked, and if it is not available,
consideration should be given to repeating the test.
2.12.A urinary pregnancy test should be considered if indicated from the history.
2.13.The clinician will undertake a physical examination to include inspection of
the vulva, vagina and cervix and proceed as clinically indicated. Bimanual
examination can be helpful in assessing patients with symptoms of
bleeding, pain or pressure.
2.14.Colposcopy is not routinely indicated if the cervix is obviously
macroscopically normal, or there are obvious benign lesions such as an
obvious ectropion, Nabothian cysts, or a benign cervical polyp.
2.15.Formal colposcopy with application of acetic acid may be required for
confirmation of some lesions e.g. large ectropions. A biopsy should only be
performed if there is a strong clinical suspicion of pathology, and not to
confirm a clinically benign entity (e.g. an ectropion).
2.16.Benign cervical polyps can usually be treated by avulsion, or excised with
loop diathermy if they have an especially large/broad base.
2.17.A cervical ectropion usually does not usually require treatment. An
explanation backed up with written patient information and reassurance is
sufficient in the majority of cases. In selected patients it may be appropriate
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 5 of 14to offer ablative treatment with silver nitrate, cold cautery, diathermy or
shallow LLETZ, provided patients have an up to date cervical screening
history and no evidence of CIN at colposcopy.
2.18.It may be necessary for cervical screening tests to be taken in the clinic.
These should be designated on the request form as having originated from
an “NHS Hospital” in order to allow for CSP “failsafe mechanisms” to
operate correctly. The appropriate referral will be made to the colposcopy
clinic by the laboratory if indicated. As with all investigations, it remains the
responsibility of the clinician to ensure that test results have been checked
and actioned as appropriate.
2.19.Patients who have biopsies taken in the clinic which show CIN should be
referred on to the colposcopy clinic for their ongoing management.
2.20.If a cervical malignancy is identified:
Multiple cervical punch or wedge biopsies of non-necrotic tissue
should be sent for 48 hour histology
The patient should be informed of the likely diagnosis
The patient should have the opportunity to meet the gynaeoncology
CNS team during the clinic if possible. If this is not possible on the
day, then verbal consent should be sought from the patient for CNS
contact, and they will make contact by telephone on the next working
day. The patient should be sent home with the contact details for the
gynaeoncology team
An MRI Pelvis and whole body PET-CT scan should be requested as
a two-week wait
The MDT coordinator, lead consultant for the MDT and the CNS team
should be informed of the patient details and the plan by email
The patient should be advised that follow-up will be arranged after the
MDT meeting
2.21.If the referral has been made in the context of a menstrual disorder, and
there are no concerns about cervical pathology after assessment, then the
patient can be offered immediate outpatient hysteroscopy, biopsy/treatment
of focal lesions as appropriate, and/or insertion of Mirena IUS if that is their
preference. Patients may prefer other medical treatments, in which case
they should advised about the different options. Patients are asked to see
their GP for follow-up if the treatment is subsequently ineffective. It is usual
practice at RCHT for patients with menstrual disorders to be offered a
transvaginal ultrasound scan. This can be undertaken at the time of the
consultation, or arranged in the radiology department and the patient
contacted with the results. If the scan demonstrates pathology requiring
follow-up, then the patient should be referred to the most appropriate team
for ongoing management.
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 6 of 142.22.If after assessment the symptoms appear to be secondary to a
contraceptive problem, then appropriate advice backed up with the relevant
patient information leaflet should be offered. The patient should be
encouraged to seek follow-up with their primary care team. Patients wishing
to have an IUCD fitted may have this done during their clinic attendance,
with follow-up in primary care to be arranged by the patient.
2.23.Post-menopausal patients with PCB, by definition also have post-
menopausal bleeding (PMB). These patients should be assessed in the
clinic and examined to look for a lower genital tract cause for their
symptoms, as per the referrer’s request. They also require a transvaginal
scan for endometrial thickness. This can be performed in the clinic, or
requested under the auspices of the “PMB Service” as a two-week wait.
Vaginal pessaries should be removed in the clinic (in patients who are
unable to remove their own) to facilitate the scan. An internal referral to the
PMB Service should be made on MAXIMS. The patient should be offered
RCHT leaflet 1797 “Post-menopausal Bleeding”. The patient will be
reviewed on the Virtual PMB clinic on the Friday morning in the week that
they have their scan, and advised of the outcome of the review by post.
2.24.Clinic correspondence to the patient and GP will be usually be generated
from the clinic database (currently viewpoint). It may be more appropriate on
some occasions to dictate a more detailed letter, at the discretion of the
clinician.
2.25.Clinic letters will be uploaded in MAXIMS by administration staff.
2.26.Checking investigation results and informing patients/referrers about results
and ongoing management plans is the responsibility of individual clinicians.
The results will not be checked by the administration team.
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 7 of 143. Monitoring compliance and effectiveness
Element to be Numbers of referrals will be monitored monthly to ensure that clinic
monitored provision meets demand to allow patients to be assessed within 2 weeks
of referral.
Clinic processes in terms of investigations undertaken and likely
diagnosis will be monitored through the clinic database (currently
viewpoint)
Cervical cancer diagnoses will continue to be monitored through the
existing “Cervical Cancer Audit”
Lead Miss S Julian
Lead Colposcopist
Consultant Gynecological Oncologist
&
Ms L Russ
Lead Nurse Colposcopist
Tool Process and outcome data will be recorded for every patient on the clinic
database (currently viewpoint). Data summaries are provided quarterly as
part of the NHS-CSP KC65 return to PHE.
Frequency As above
Reporting As above
arrangements
Acting on Miss S Julian
recommendations Lead Colposcopist
and Lead(s) Consultant Gynecological Oncologist
&
Ms L Russ
Lead Nurse Colposcopist
Change in Required changes to practice will be identified and actioned within 3
practice and months, immediately if required. A lead member of the team will be
lessons to be identified to take each change forward where appropriate. Lessons will be
shared shared with all the relevant staff/stakeholders.
4. Equality and Diversity
4.1. This document complies with the Royal Cornwall Hospitals NHS Trust
service Equality and Diversity statement which can be found in the 'Equality,
Inclusion & Human Rights Policy' or the Equality and Diversity website.
4.1. Equality Impact Assessment
The Initial Equality Impact Assessment Screening Form is at Appendix 2.
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 8 of 14Appendix 1. Governance Information
The One Stop Cervical Assessment Clinic: Clinical
Document Title
Guideline V1.0
This document replaces
(exact title of previous New Document
version):
Date Issued/Approved: March 2021
Date Valid From: March 2021
Date Valid To: March 2024
Miss S Julian, Consultant Gynaecological Oncologist
Directorate / Department
& Lead Colposcopist, Gynaecology Dept., Women’s
responsible (author/owner):
& Children’s.
Contact details: Secretary Nadia Francis (01872)252729
This guideline applies to all patients referred to for
assessment of their uterine cervix, and the staff
involved in their healthcare. The provision of a
dedicated clinic for patients with possible
abnormalities of the cervix (some of which may
represent serious pathology such as cervical cancer)
ensures that all patients are seen within two weeks
of referral, achieving equality of access for all,
Brief summary of contents
regardless of the route of referral. Ensuring that
patients are seen by clinicians with an appropriate
skill set means that consultations are responsive to
patients’ concerns and needs. The one-stop model
reduces fragmentation of care and delay, whilst
promoting efficiency and protecting scare healthcare
resource.
Abnormal Cervix
Post-coital Bleeding
One-Stop Cervical Assessment
Suggested Keywords:
Colposcopy
Rapid Access Clinic
Two-week Wait Clinic
RCHT CFT KCCG
Target Audience
Executive Director Medical Director
responsible for Policy:
Approval route for Obs and Gynae Specialty Meeting
consultation and ratification:
General Manager confirming
Mary Baulch
approval processes
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 9 of 14Name of Governance Lead
confirming approval by
Caroline Amukusana
specialty and care group
management meetings
Links to key external https://www.gov.uk/government/publications/cervical-
standards screening-programme-and-colposcopy-management
Related Documents: None
Training Need Identified? No
Publication Location (refer to
Policy on Policies – Internet & Intranet Intranet Only
Approvals and Ratification):
Document Library Folder/Sub
Clinical/Gynaecology
Folder
Version Control Table
Version Changes Made by
Date Summary of Changes
No (Name and Job Title)
06/02/2021 V1.0 Initial version Sophia Julian
All or part of this document can be released under the Freedom of Information
Act 2000
This document is to be retained for 10 years from the date of expiry.
This document is only valid on the day of printing
Controlled Document
This document has been created following the Royal Cornwall Hospitals NHS Trust
Policy for the Development and Management of Knowledge, Procedural and Web
Documents (The Policy on Policies). It should not be altered in any way without the
express permission of the author or their Line Manager.
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 10 of 14Appendix 2. Initial Equality Impact Assessment Form
Name of the strategy / policy /proposal / service function to be assessed
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Directorate and service area: New or existing document:
WCSH, Gynaecology New
Name of individual completing assessment: Telephone:
Sophia Julian Ext 2729
1. Policy Aim
Who is the
All patients referred to for assessment of their uterine cervix, and the
strategy / policy /
staff involved in their healthcare.
proposal / service
function aimed at?
2. Policy Objectives The provision of a dedicated clinic for patients with possible
abnormalities of the cervix (some of which may represent serious
pathology such as cervical cancer) ensures that all patients are
seen within two weeks of referral, achieving equality of access for
all, regardless of the route of referral. Ensuring that patients are
seen by clinicians with an appropriate skill set means that
consultations are responsive to patients’ concerns and needs. The
one-stop model reduces fragmentation of care and delay, whilst
promoting efficiency and protecting scare healthcare resource.
3. Policy
Intended To meet the mandated NHS “28 days faster diagnosis” target which came
Outcomes into force in April 2020.
4. How will
you measure See section 3 - Monitoring compliance and effectiveness
the outcome?
5. Who is intended
to benefit from the Patients referred to for assessment of their uterine cervix
policy?
6a Who did you Local External
Workforce Patients Other
consult with groups organisations
x
b). Please identify the
groups who have The RCHT Colposcopy Team
been consulted about
this procedure.
What was the Guideline approved
outcome of the
consultation?
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 11 of 147. The Impact
Please complete the following table. If you are unsure/don’t know if there is a negative impact
you need to repeat the consultation step.
Are there concerns that the policy could have a positive/negative impact on:
Protected
Yes No Unsure Rationale for Assessment / Existing Evidence
Characteristic
Age
X The policy applies to all adult patients with a cervix
Sex (male, female
non-binary, asexual X The policy applies to all adult patients with a cervix
etc.)
Gender
reassignment X The policy applies to all adult patients with a cervix
Race/ethnic
Any information provided will be in an accessible format for
communities X the patient’s needs – i.e. available in different languages if
/groups required/access to an interpreter if required
Disability
(learning disability,
physical disability, Those patients with any identified additional needs will be
referred for additional support as appropriate - i.e. to the
sensory impairment,
X liaison team or for specialist equipment.
mental health Information will be provided in a format to meet the patient’s
problems and some needs e.g. easy read, audio etc.
long term health
conditions)
Religion/ The policy applies to all adult patients with a cervix
other beliefs X
Marriage and civil The policy applies to all adult patients with a cervix
partnership X
Pregnancy and The policy applies to all adult patients with a cervix
maternity X
Sexual orientation The policy applies to all adult patients with a cervix
(bisexual, gay, X
heterosexual, lesbian)
If all characteristics are ticked ‘no’, and this is not a major working or service
change, you can end the assessment here as long as you have a robust rationale
in place.
I am confident that section 2 of this EIA does not need completing as there are no highlighted
risks of negative impact occurring because of this policy.
Name of person confirming result of initial Miss S Julian, Consultant Gynaecological
impact assessment: Oncologist & Lead Colposcopist
If you have ticked ‘yes’ to any characteristic above OR this is a major working or
service change, you will need to complete section 2 of the EIA form available here:
Section 2. Full Equality Analysis
For guidance please refer to the Equality Impact Assessments Policy (available
from the document library) or contact the Human Rights, Equality and Inclusion
Lead debby.lewis@nhs.net
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 12 of 14Appendix 3: Introductory Clinic Letter
To be sent to the patient with the clinic appointment
Dear Patient,
You have been referred to us for a check-up of your cervix (the neck of the womb). Usually this is
because you have had some vaginal bleeding, or something has been noticed on your cervix when
you were examined.
The vast majority of the time, it turns out that there is nothing serious wrong and patients can be
reassured that all is well. In a very small number of cases, cervical cancer is the cause of the
symptoms/cervical appearance. Because of this we offer all patients an appointment on an urgent
basis. The quicker you are seen, the quicker we can reassure you.
Please find enclosed a booklet about what to expect during your appointment. If you have any
questions, please contact the Colposcopy Team on (08172) 252360.
Yours sincerely,
Miss S Julian
Consultant Gynaecological Oncologist / Lead Colposcopist
Enc: Patient Information Booklet “The One-Stop Cervical Assessment Clinic”
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 13 of 14Appendix 4: List of Abbreviations
CIN Cervical intra-Epithelial Neoplasia
CNS Clinical Nurse Specialist
CSP Cervical Screening Programme
IMB Intermenstrual Bleeding
IUCD Intrauterine Contraceptive Device
LLETZ Large Loop Excision of the Transformation Zone
MDC Menstrual Disorders Clinic
MDT Multidisciplinary Team Meeting
MRI Magnetic Resonance Imaging
PCB Post-coital Bleeding
PET-CT Positron Emission Tomography and Computed Tomography
PMB Post-menopausal Bleeding
2WW Two-week Wait
The One Stop Cervical Assessment Clinic: Clinical Guideline V1.0
Page 14 of 14You can also read