Ann Bruno, MFM Fellow Pregnancy ECHO February 28, 2020
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Ann Bruno, MFM Fellow
Pregnancy ECHO
February 28, 2020
©UNIVERSITY OF UTAH HEALTH
I have not financial disclosures.

Objectives • Review the background of aspirin and its proposed use in pregnancy • Review literature on aspirin use for preeclampsia risk reduction • Review safety of aspirin • Review current guidelines for aspirin use
Aspirin & Preeclampsia: Why?
• Pathophysiology of preeclampsia remains poorly understood.
• Related to “poor placentation”
• Chronic uteroplacental ischemia
• Immune maladaptation
• Inflammatory response of trophoblast
• VLDL toxicity
• Imbalance of angiogenic factors
• Evidence that an imbalance in prostacyclin and thromboxane A2.
• Prostacyclin: vasodilator, inhibitor of platelet aggregation
• Thromboxane A2 (TXA2): vasoconstrictor, promoter of platelet aggregation
ACOG 2019.
Redman et al. Science, 2005.
Low-Dose Aspirin (LDA)
• Aka acetylsalicylic acid
• Nonsteroidal anti-inflammatory
drug (NSAID) family
• MOA (at low dose):
• Inhibits cyclooxygenase isoenzyme
(COX-1) via irreversible acetylation
• Decreased thromboxane A2
(vasoconstrictor)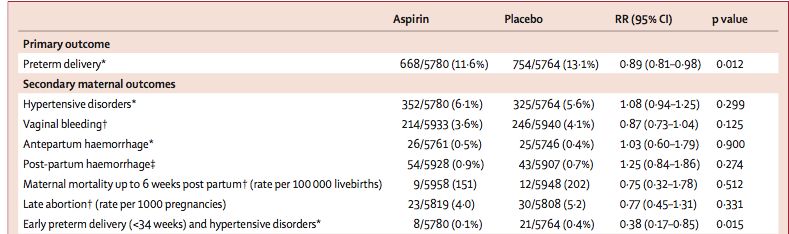
Early Aspirin Studies
• Based on proposed relationship of
prostacyclin/TXA2 and
preeclampsia, early small studies of
aspirin in women at risk for
preeclampsia carried out.
• Small trials suggested LDA may be
beneficial for women at high risk.
• Example:
• Double-blind, placebo-controlled RCT
• 65 women enrolled in 3rd trimester
• LDA v Placebo
Schiff et al. NEJM, 1989.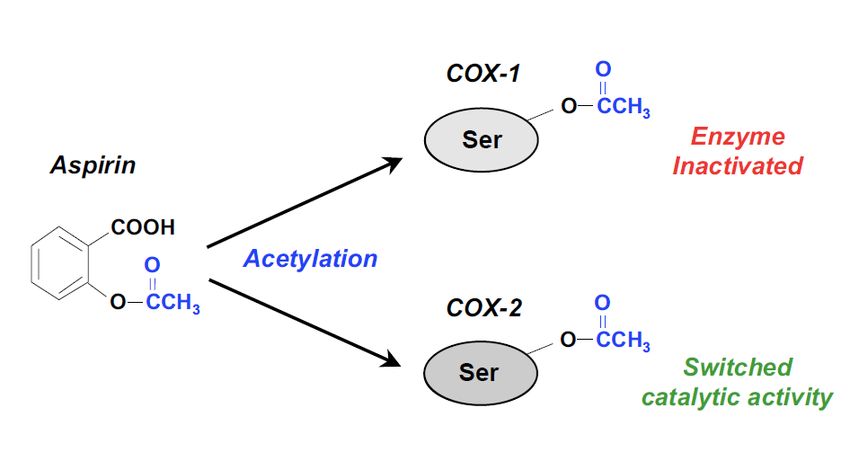
Two largest RCTs to Follow
• CLASP (Lancet 1994) • MFMU Trial (NEJM 1998)
• Multicenter • Multicenter
• 9364 women • 2539 women
• 16 countries; international • Included between 13-26w
• Included between 12-32w • DM, multifetal gestations, chronic
• Considered “at risk” by clinician HTN, prior preeclampsia
• 60mg aspirin v. placebo • 60mg aspirin v. placebo
• 12% reduction in preeclampsia • 10% reduction in preeclampsia
(RR 0.9, 95% CI 0.6-1.2)
MFMU, NEJM 1998.
CLASP, Lancet 1994.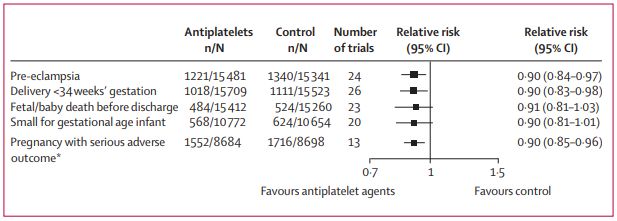
Next step: Meta
• Initial findings were
not immediately
confirmed in larger
RCTs; multiple RCTs
with varying results.
• PARIS Meta-analysis
(2007): individual
patient data (32,217
women)
• From 31 RCTs on use
of anti-platelet
agents for prevention
of preeclampsia
• LDA v Placebo: RR for
preeclampsia 0.9
(95% CI 0.84-0.97)
Askie et al, JAMA 2007.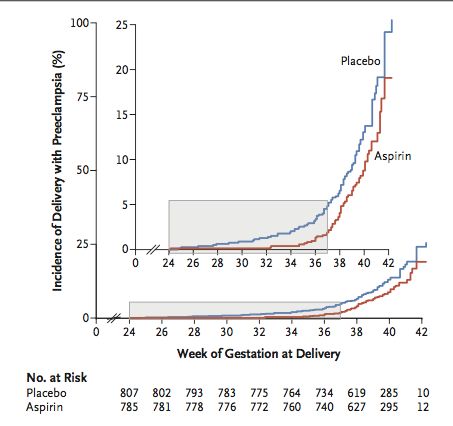
Cochrane meta-analysis (2019): LDA v Placebo: RR for preeclampsia 0.82 (95% CI 0.77-0.88)
Cochrane 2019.U.S. Preventive Services Task Force (USPSTF)
• Systematic review (2014)
• Pooled data from 15 RCTs – all placebo-controlled
• Baseline incidence of preeclampsia: 8-30%
• No trials with aspirin initiation prior to 12 weeks
• Results:
• 24% reduction in risk for preeclampsia (RR 0.76, CI 0.62-0.95)
• 14% reduction in risk for preterm birth (RR 0.86, 95% CI 0.76-0.98)
• 20% reduction in risk for growth restriction (RR 0.8, CI 0.65-0.99)
• Number needed to treat (NNT): 42
MFMU, NEJM 1998.
CLASP, Lancet 1994.
LeFevre et al, An Int Med, 2014.Prior Guidelines: • 2011: World Health Organization (WHO) • 2013: Hypertension in Pregnancy Task Force Report • 2013: National Institute of Health and Care Excellence • 2014: U.S. Preventative Services Task Force (USPSTF) Recommend aspirin for risk reduction of pre- eclampsia, but with varying criteria for “risk”, dosing regimens, and initiation timing.
“Low-dose aspirin (81 mg/day) prophylaxis is recommended in women at high risk of
preeclampsia and should be initiated between 12 weeks and 28 weeks of gestation
(optimally before 16 weeks) and continued daily until delivery.“
ACOG 2018.
USPSTF Guidelines. LeFevre et al, Annals Int Med, 2014.ACOG 2018. USPSTF Guidelines. LeFevre et al, Annals Int Med, 2014.
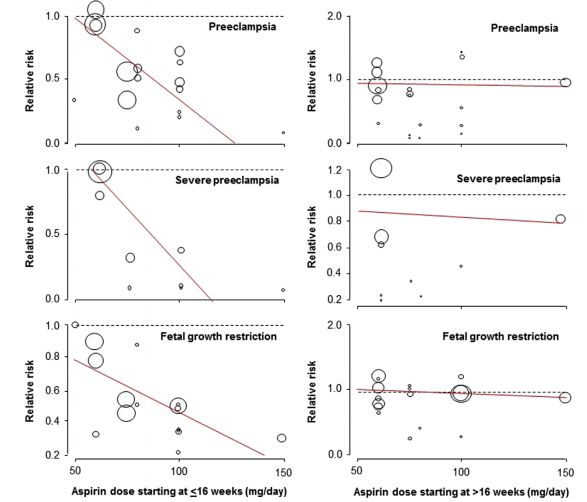
LDA Timing • Ideal timing is to initiate at
Aspirin Dose • Most trials have utilized range of 60- 150mg • CLASP – 60mg • MFMU – 75mg • Meta-analyses utilizing LDA are at doses
Aspirin & Preeclampsia • 2017 RCT • 1776 women • Screened/included in 1st trimester • LDA (150mg) v Placebo • Preeclampsia with delivery
Safety – Maternal
• No (or minimal) increased risk:
• Postpartum hemorrhage
• Placental abruption • USPSTF:
• Blood loss • PPH – RR 1.02, CI 0.96-1.09
• Abruption – RR 1.17, CI 0.93-1.48
• Cochrane:
ACOG 2018.
LeFevre et al, Annals Int Med, 2014.Safety – Fetal
• No increased risk:
• Congenital anomalies (cohort 15,000 women with LDA exposure in 1st trimester)
• Neonatal hemorrhagic complications
• Ductus arteriosus closure; persistent pulmonary hypertension
• USPSTF: RR for ICH in neonates 0.84 (CI 0.61-1.16)
• CLASP trial: no difference in neurologic development @ 18 months
• Gastroschisis
• Meta-analysis of case-control data showing increased risk
• Dose of aspirin not indicated
• Other variables not controlled (i.e., illicit drug use)
CLASP, 1994. Kozer et al. AJOG, 2002. ACOG 2018.
LeFevre et al, Annals Int Med, 2014.Absolute Contraindications to Aspirin
• Aspirin allergy
• Hypersensitivity to NSAIDs
• Nasal polyps
• Asthma with known history of
aspirin-induced bronchospasm
Relative: history of GI bleed,
peptic ulcer disease (active),
severe hepatic dysfunction,
obstetric bleedingAspirin for other indications
• In women receiving LDA for
preeclampsia prevention:
• 10-20% reduction in growth restriction
• Insufficient evidence to support • 8-14% reduction in preterm birth
LDA for prevention of:
• Stillbirth • But these findings are in context of
• Fetal growth restriction larger trials and meta-analyses
• Preterm birth
considering women at risk of
preeclampsia.
• No strong data (?) to independently
recommend.
LeFevre et al, An Int Med, 2014.Conclusions: • Low-dose aspirin (81mg/day) is
recommended as prophylaxis in
women at high risk of preeclampsia.
• Aspirin should be initiated between 12-
28 weeks gestation (ideallyReferences: • ACOG. Committee Opinion 743: Low-Dose Aspirin Use During Pregnancy. Obstetrics & Gynecology, 2018; 132(1): e44-e52. • Rolnik DL, Wright D, Poon LC, O’Gorman N, Syngelaki A, de Paco Matallana C, et al. Aspirin versus placebo in pregnancies at high risk for preterm preeclampsia. N Engl J Med 2017;377:613–22. • Duley L, Henderson-Smart DJ, Meher S, King JF. Antiplatelet agents for preventing pre-eclampsia and its complications. Cochrane Database of Systematic Reviews 2007, Issue 2. Art. No.: CD004659. • Askie LM, Duley L, Henderson-Smart DJ, Stewart LA. Antiplatelet agents for prevention of pre-eclampsia: a meta-analysis of individual patient data. PARIS Collaborative Group. Lancet 2007;369:1791–8. • CLASP: a randomised trial of low-dose aspirin for the prevention and treatment of pre-eclampsia among 9364 pregnant women. CLASP (Collaborative Low-dose Aspirin Study in Pregnancy) Collaborative Group. Lancet 1994; 343:619–29. • Caritis S, Sibai B, Hauth J, Lindheimer MD, Klebanoff M, Thom E, et al. Low-dose aspirin to prevent preeclampsia in women at high risk. National Institute of Child Health and Human Development Network of Maternal–Fetal Medicine Units. N Engl J Med 1998;338:701–5. • LeFevre ML. Low-dose aspirin use for the prevention of morbidity and mortality from preeclampsia: U.S. Preven- tive Services Task Force recommendation statement. U.S. Preventive Services Task Force. Ann Intern Med 2014;161: 819–26. • Redman CS, Sargent IL. Latest advanced in understanding preeclampsia. Science 2005; 308: 1592-4. • ACOG. Practice Bulletin: 202: Gestational Hypertension and Preeclampsia. Obstetrics & Gynecology, 2018; 133(1): e1-e25. • Roberge S, Nicolaides K, Demers S, et al. The role of aspirin dose on the prevention of preeclampsia and fetal growth restriction: systematic review and meta-analysis. Am J Obstet Gynecol 2017; 216: 110-20.e6. • Hoffman MK, Goudar SS, Kodkany BS, Metgud, M. Low-dose aspirin for the prevention of preterm delivery in nulliparous women with a singleton pregnancy (ASPIRIN): a randomised, double-blind, placebo-controlled trial. Lancet 2020; 395: 285- 293 • Mallampati D, Grobman W, Rouse DJ, Werner EF. Strategies for prescribing aspirin to prevent preeclampsia: a cost- effectiveness analysis. Obstet Gynecol, 2019; 134(3): 537-544.
• RCT • 6 countries (Congo, Guatemala, Kenya, Pakistan, Zambia, India) • Primary outcome: PTB
• Decision analysis
• 4 strategies for aspirin:
1) No aspirin
Cost-Effectiveness 2)
3)
Biomarker/US predicted use
Use per USPSTF guidelines
*Universal aspirin use dominated 4) Universal use
• Outcomes:
• Preeclampsia-related costs
• # cases preeclampsia/100,000
Malampati et al. Obstet Gyn 2019. pregnant womenYou can also read