Arthritis & Exercise - Pure Training and Development 2020 - PTD Hub
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Arthritis & Exercise
Part 1
Pure Training and Development © 2020
Tutor – Who am I? • Emma Haughton • Creator of workshops and seminars • 7 years experience in Exercise Referral Industry • Passionate about improving the health and wellbeing of your community

Learner Support ✓ Home study does not mean no support ✓ Supporting materials in ‘Resources’ section ✓ Contact us for different formats Call: 03302231302 Email: support@puretraininganddevelopment.co.uk Or Facebook Messenger

Learning • Explore the aetiology and pathophysiology of
osteoarthritis and rheumatoid arthritis
Objectives • Understand the recent prevalence statistics of
arthritis in the UK
• Identify the benefits of physical activity and
exercise in the management of the condition
• Identify an exercise prescription framework
• Recognise and apply health and safety
considerations
Let’s get ready to study…

Question…
Do you know the key differences between
OA and RA?
On a piece of paper, bullet point the key things you remember
about Osteoarthritis and Rheumatoid Arthritis.
You have 1 minute….
• An estimated 18.8 million people live with a
Introduction musculoskeletal condition in the UK (GBD 2017)
& Prevalence
• There are more than 100 different forms of
arthritis
• Most common two explored during this
seminar:
• Osteoarthritis and rheumatoid arthritis
• 8.75 million live with osteoarthritis
• 430,000 live with rheumatoid arthritis (Arthritis
Research UK, 2019)
• Each person is affected in a unique way
Introduction • Estimated to cost the economy £10.2 billion
in direct costs to the NHS and wider
& Costs healthcare system
• Cumulatively the healthcare cost will reach
£118.6 billion over the next decade.
• The cost of working days lost is £2.58
billion in 2017 rising to £3.43 billion by
2030.
Sourced: York Health Economics, “The Cost of Arthritis: Calculation conducted on behalf of
Arthritis Research UK,” Unpublished, 2017.
Aetiology & Pathophysiology of Osteoarthritis
Pathophysiology of Osteoarthritis • Common in older population • Osteoarthritis is a non-inflammatory condition • Functional limitations and reduced quality of life • No cure but condition can be managed • A condition which typically has a gradual onset
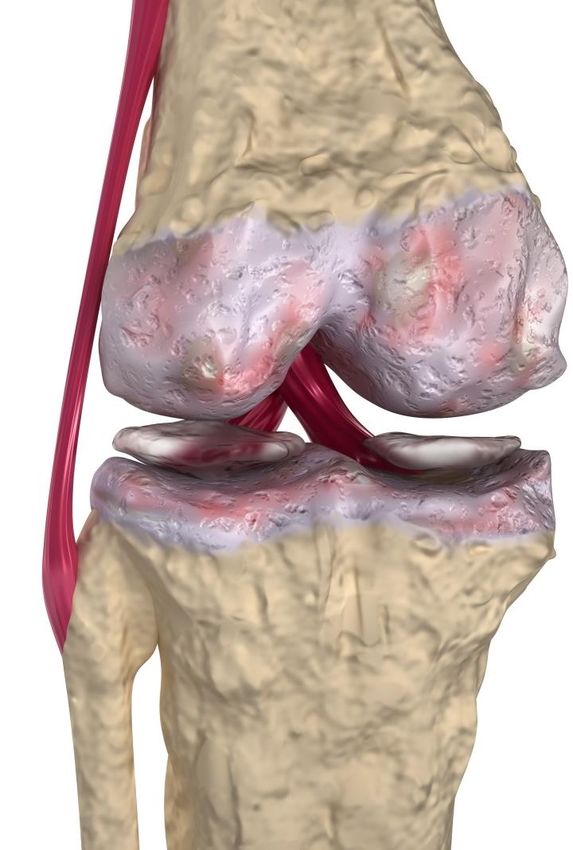
Pathophysiology of Osteoarthritis • Cartilage acts as a shock absorber • Enables smooth movement of bones • Starts with progressive loss of articular cartilage • Degenerative condition of the joints • Bone becomes exposed • Surfaces become rough and thin
Impact bearing properties are diminished
Body compensates by changing shape, thickening
(subchondral sclerosis ) and developing bone spurs
(osteophytes/osteophytosis)
Pathophysiology Movement becomes restricted and painful
of Osteoarthritis
All contributes to joint crepitus and pain
Inflammation of joint membrane in severe arthritisOsteoarthritis Image
Arthritis Research UK/Versus ArthritisOsteoarthritis Image
Arthritis Research UK/Versus ArthritisCondition can occur with and without
symptoms of pain and weakness
Can affect any joint in the body
Pathophysiology Commonly affects hips, knees, spine and
of Osteoarthritis hands
Changes occur to the entire joint, not just the
cartilage and bone
Observed physical changes occurPathophysiology of Osteoarthritis • Inflammation is a frequent symptom – (Sokolve et al, 2013) • Muscle wastage occurs • Connective tissues, tendons and ligaments become tight • Results in reduced range of movement
• Discomfort
Signs and Symptoms • Pain (exercise and rest)
• Stiffness
• Swelling
• Decreased range of motion
• Muscle weakness
• Joint deformity
• Joint instability
• Depression (Lepine & Briley, 2004)Causes/Risk Factors
• Age
• Gender
• Obesity
• Occupation
• Sedentary lifestyle
• Physical injury/trauma
• Genetic factors
Georgiev et al, 2019• Pain relievers such as paracetamol
Medications • NSAID/Corticosteroids – aim to reduce
swelling and pain
Side Effects • Gastrointestinal problems
• Potential asthma attacks for asthmatics
• Addiction
• Increased risk of osteoporosisAetiology & Pathophysiology of Rheumatoid Arthritis
Pathophysiology of Rheumatoid Arthritis • Approximately 430,000 people in UK (VersusArthritis, 2019) • Cause is not fully known • Auto immune disease • Chronic inflammatory disease • Systemic condition • A condition typically with a rapid onset • Indicated by flare up and remission phases
Pathophysiology of Rheumatoid Arthritis • Tends to affect smaller joints • Hands, fingers and toes • Antibodies attack synovium • Thick and swollen synovium • Synovium invades and destroys • Hot, red and swollen • Stretched capsule can cause instability/ deformation
Pathophysiology of Rheumatoid Arthritis
Arthritis Research UK/Versus ArthritisPathophysiology of Rheumatoid Arthritis
Arthritis Research UK/Versus ArthritisFlare ups and remissions
Pain
Inflammation
Symptoms Damage to joint tissues
of Fever
Rheumatoid Joint deformity
Arthritis Limited ROM
Symptoms during a flare up include:
• Fatigue
• Loss of appetite
• Muscle aches
• Red, swollen and painful joints• NSAID/Corticosteroids – aim to reduce
Medications swelling and pain
• DMARDS – reduce joint damage and
promote remission
• Goal is to supress the immune system
Side Effects
• Gastrointestinal problems
• Potential asthma attacks for asthmatics
• Risk of osteoporosis
• HypertensionCauses/Risk Factors • Age • Genetic factors • Gender • Smoking • Obesity • Diet
Associated Risks • Increases the risk of • CV disease and stroke • Lung disease • Osteoporosis • Higher risk of falls • depression
Many more arthritic conditions:
Gout (1.6 million)
Other
Forms of Ankylosing spondylitis (222,00 people)
Arthritis
Cervical spondylosis
Recommended to complete further reading on these
conditions.Break Time Take a 10-15 minute break
End of Part 1
Please continue with Part 2
Pure Training and Development © 2020Arthritis & Exercise
Part 2
Pure Training and Development © 2020Welcome back from break…
Exercise
In the management of these conditions
Pure Training and Development © 2020What are the benefits of physical activity and exercise?
Decrease Decrease joint pain and stiffness
Improve
or Improve or maintain joint motion
maintain
Physical Decrease the risk of cardiovascular
Activity Decrease disease (higher in those with rheumatoid
arthritis)
Benefits Improve ability to do activities of daily
Improve living (i.e. access in and out of car or
going up and down stairs)
Decrease Decrease disease activityBetter pain management
Increase muscular strength
Improved bone mineral density protect against osteoporosis
Physical Maintain control of weight
Activity Improved balance and co-ordination
Benefits Reduced stress and depression
Improved sleep patterns
Increased energy levels
Improved self-esteemReduces risk of:
Hip and knee osteoarthritis pain by 6% (Hurley et
al, 2018)
Regular Joint and back pain by 25% (Choi et al, 2010)
physical Depression by up to 30% (DOH, 2011)
activity
Hip fracture rates by up to 68% (Scottish Government,
2003)
Falls by 76% (Foster et al, 2017)
Source: https://www.versusarthritis.org/media/14594/state-of-musculoskeletal-health-2019.pdfHighlighted Statement
Advise people with osteoarthritis to exercise as a core
treatment, irrespective of age, comorbidity, pain severity
or disability.
Exercise should include:
• Local muscle strengthening
• General aerobic fitness
NICE (2008 - 2020)Osteoarthritis & A review suggested that ‘aerobic,
Exercise - Evidence strengthening, flexibility, aquatic, yoga and
Tai chi improve outcomes related to joint
symptoms, mobility, quality of life,
psychological health, musculoskeletal
properties, body composition, sleep and
fatigue. (Wellsandt et al 2018; Schiphof et al, 2018)
'the benefits of exercise
therapy extend beyond
pain and physical function ‘there is substantial evidence regarding the
with moderate effects on benefits of strengthening exercises to
depression in people with reduce pain in knee osteoarthritis patients.
hip and knee OA’ (Hurley et al, Based on the included studies analysis,
2018, Villafane, 2018) exercises should be performed three times
weekly for a duration of 8-11 or 12-15
weeks.’ (Imoto et al, 2019)There is strong evidence to
Rheumatoid Arthritis suggest that increasing
physical activity
& Exercise –Evidence and/or exercise can
simultaneously improve
symptoms and reduce the
impact of systemic
No studies have found increased disease manifestations in RA. (Metsios et
al, 2018)
activity as a result of physical training
‘Based on the evidence,
aerobic capacity training
‘Physical activity and exercise are effective
combined with muscle
methods to improve arthritis symptoms,
strength training is
enhance mental health and reduce the risk
recommended as routine
for CVD; however, the majority of patients
practice in patients with
with RA lead sedentary lifestyles.’ (Veldhuijzen van
Zanten et al, 2015) RA” (Hurkmans et al, 2009; Verhoeven et
al, 2016)Barriers • External influences/ previous advice • Pain • Fatigue • Speed joint breakdown/wears joint down • Psychological concerns • Excess weight • Experienced exacerbating symptoms and stopped/been put off • Understanding the benefits
Psychological Aspect • Fear largely contributes to lack of exercise • Misunderstanding about further damage • Motivation is key – use SMART goals • Find an enjoyable form of exercise • RA can be disabling and impact life and work • Depression, anxiety and lack of motivation
Break Time Take a 10-15 minute break
End of Part 2
Please continue with Part 3
Pure Training and Development © 2020Arthritis & Exercise
Part 3
Pure Training and Development © 2020Welcome back from break…
Exercise Prescription
• Manage pain and discomfort
Key
• Improve joint range of motion
Objectives
• Increase muscular strength
• Improve balance and co-ordination
• Decrease excess body fat (where applicable)
• Improve quality of life
• Change health behaviour with education
and adviceSlow and gradual
Pulse raising and mobility
Warm Up
Considerations
Seated if balance is affected
Dynamic StretchesTrain unaffected joints for cardiovascular
Main Choose smooth and rhythmic exercises
Workout
Considerations Consider the order of exercises
Ensure the focus is on functional strength
and endurance and cardiovascular fitnessSlow and extended period
Cool Down Seated or lying for some stretches
Considerations
Hold to the point of tension within painExercise Prescription
American College of Sports Medicine Exercise Guidelines for Osteoarthritis and Rheumatoid arthritis
Cardiovascular Musculoskeletal Flexibility
Frequency 3-5 days a week 2-3 days a week Daily
Moderate Intensity (40-59% Move through ROM feeling
60-80% 1RM. Initial intensity should be
HRR) tightness/stretch without pain. Progress
Intensity lower (50-60% 1RM) for those
RPE 11-16/20 ROM of each exercise only when there
unaccustomed to resistance training
Or vigorous (≥60% HRR) is very little or no joint pain
Use healthy adult values and adjust Up to 10 repetitions for dynamic
150 mins per week of moderate
Time accordingly (i.e. 8-12 repetitions for 2-4 movements, hold static stretches for
intensity or 75 mins of vigorous
sets); include all major muscle groups 10-30s
Activities with low joint stress Machine or free weights. Body weight
A combination of dynamic and static
Type such as walking, cycling, exercises might also be appropriate for
stretching focused on all major joints
swimming or aquatic exercise select individualsExercise Prescription
American College of Sports Medicine Exercise Guidelines for Osteoarthritis and Rheumatoid arthritis
Cardiovascular Musculoskeletal Flexibility
Frequency 3-5 days a week 2-3 days a week Daily
Moderate Intensity (40-59% Move through ROM feeling
60-80% 1RM. Initial intensity should be
HRR) tightness/stretch without pain. Progress
Intensity lower (50-60% 1RM) for those
RPE 11-16/20 ROM of each exercise only when there
unaccustomed to resistance training
Or vigorous (≥60% HRR) is very little or no joint pain
Hold a stretch for 5-10
secs and repeat 5-10
Use healthy adult values and adjust Up to 10 repetitions for dynamic
150 mins per week of moderate times
Time accordingly (i.e. 8-12 repetitions for 2-4 movements, hold static stretches for
intensity or 75 mins of vigorous
sets); include all major muscle groups (Versus Arthritis)
10-30s
Activities with low joint stress Machine or free weights. Body weight
A combination of dynamic and static
Type such as walking, cycling, exercises might also be appropriate for
stretching focused on all major joints
swimming or aquatic exercise select individualsExercise Prescription - Exercise Ideas Versus Arthritis UK suggest these exercises are regular examples to integrate: Knee Osteoarthritis: • Sit to stand • Quadriceps strengthening exercises • Step ups Hip Osteoarthritis: • Hip abduction • Hip extension
Exercise Prescription - Exercise Ideas Versus Arthritis UK suggest these exercises are regular examples to integrate: Rheumatoid Arthritis: • Whole body exercises • Low impact aerobic exercises i.e. swimming, walking
Exercise Prescription - Methods of Monitoring • Observation • Talk test • RPE • Be aware of medication affecting their pain sensation levels
Exercise Prescription -
Contraindications & Considerations
Do not exercise a joint during acute flare ups
Avoid/reduce high impact exercises (depending on the client)
Avoid excessive repetitions
Avoid over stretching the joints
Do not bounce when stretching
Avoid prolonged exercise in the same position
Avoid kneeling positions (as appropriate)Exercise Prescription - Contraindications & Considerations Perform an extended warm up and cool down Be aware of the side effects of medication Monitor pain levels Consider shorter durations and build over time Inform the client about post exercise associated muscle discomfort Check for suitable footwear
Exercise Advice • Resources from Arthritis Research UK/Versus Arthritis
Two key forms of arthritis: OA and RA
OA is the degeneration of the joint
RA is an auto immune condition causing synovial
membrane swelling
Summary 8.75 million with OA
Points 430,000 with RA
Programmes won’t necessarily be the same each
session
Every individual diagnosed with arthritis will be unique
and requires an individualised programme
Regular participation in exercise can improve function
and reduce painEvidence supports exercise as a form of management
for both OA and RA
Evidence supports that exercise does not cause
damage to the joints (as long as it’s safe and
appropriate)
Summary Aerobic exercise is recommended on 3-5 days per
Points
week
Gentle, low impact exercise for shorter durations
should be performed at the start
Include resistance and flexibility components into the
training programme using ACSM guidelines (2018)Regularly assess the client to identify safe methods of
progression
Do not exercise the area affected during a flare up
Summary Encourage good posture during exercise and in daily
Points
life
Exercise has psychological benefits for the condition
Build a rapport with your client and you will be able to
work more effectively with them1. Exercise and osteoarthritis: an update
2. Exercise as medicine to be prescribed
in osteoarthritis
Recommended
Reading
In Your ‘Resources
Section’Useful Websites & Documents
Information and links can be found within the
‘Resources Section’.
Exercises to manage pain - Versus Arthritis
NHS Website
Arthritis Foundation
The Arthritis Society Top 10 Exercises for Arthritis PDF
(type this in to a search engine to directly access PDF)Other CPD Seminars
References
• Baillet, A., Vailliant, M., Guinor, M., Juvin, R and Gaudin, P. (2012). Efficacy of resistance exercises in rheumatoid arthritis: meta analysis of randomized controlled trials. Rheumatology, 51(2), 519-527.
• Cooney, J.K., Law, RJ., Matschke, V., Lemmey, A.B., Moore, J.P., Yasmeen, A., Jones, J.G., Maddison, P and Thom, J.M. (2011). Benefits of Exercise in Rheumatoid arthritis. Journal of Aging Research, 2011.
• Wenham, C. Y. J. & Conagham, P.G. (2010). The Role of synovitis in osteoarthritis. Therapeutic Advances in Musculoskeletal Disease, 2(6), 349-359.
• Pelletier, J-P., Martel-Pelletier, J., & Abramson, S.B. (2001). Osteoarthritis, an Inflammatory Disease: Potential Implication for the Selection of New Therapeutic Targets. Arthritis & Rheumatism, 44(6), 1237-1247.
• Jorge, R.T.B., De Souza, M.C., Chiari, A., Jones, A., Fernandes, A.DR.C., Junior, I.L., Natour, J. (2014). Clinical Rehabilitation. [ahead of print].
• NICE (2008,2014). Osteoarthritis: The care and management of osteoarthritis in adults, quick reference guide. NICE. Updated version retrieved in August 2018, from
https://www.nice.org.uk/guidance/cg177/chapter/1-Recommendations#non-pharmacological-management-2
• National Collaborating Centre for Chronic Conditions. Osteoarthritis: national clinical guideline for care and management in adults. London: Royal College of Physicians, 2008.
• Right Care (2011), The NHS Atlas of Variation in Healthcare.
• 4 Department of Health (2011), England level data by programme budget: 2010-11.
• HL Select Committee (2013), Ready for Ageing?
• State of musculoskeletal health 2017. Arthritis & other musculoskeletal conditions in numbers. Arthritis Research UK.
• Hunter, D.J & Eckstein, F. (2009). Exercise and Osteoarthritis. Journal of Anatomy, 214 (2), 197-207.
• Veldhuijzen van Zanten et al. (2015). Perceived Barriers, Facilitators and Benefits for Regular Physical Activity and Exercise in Patients with Rheumatoid Arthritis: A Review of the Literature. Sports Med, 45(10), 1401-
1412.
• ACSM Guidelines for Exercise Testing and Prescription. 10 th Edition. Wolters Kluwer Health
• Osthoff, AK R., Juhl, CB., Knittle, K., Dagfinrud, H., Hurkmans, E., Braun, J., Schoones, J., & Niedermann, K. (2018). Effects of exercise and physical activity promotion: meta-analysis informing the 2018 EULAR recommendations for
physical activity in people with rheumatoid arthritis, spondyloarthritis and hip/knee osteoarthritis. BMJ, RMD Open 2018;4:e000713. doi: 10.1136/rmdopen-2018-000713
• Imoto AM, Pardo JP, Brosseau L, Taki J, Desjardins B, Thevenot O, Franco E, & Peccin S. (2019) Evidence synthesis of types and intensity of therapeutic land-based exercises to reduce pain in individuals with knee osteoarthritis.
Rheumatol Int. 2019 Jul;39(7):1159-1179
• Wellsandt E, & Golightly Y (2018) Exercise in the management of knee and hip osteoarthritis. Curr Opin Rheumatol. 2018 Mar;30(2):151-159
• Georgiev T, & Angelov AK (2019). Modifiable risk factors in knee osteoarthritis: treatment implications. Rheumatol Int. 2019 Jul;39(7):1145-1157.
• Veldhuijzen van Zanten JJ, Rouse PC, Hale ED, Ntoumanis N, Metsios GS, Duda JL, & Kitas GD (2015). Perceived Barriers, Facilitators and Benefits for Regular Physical Activity and Exercise in Patients with Rheumatoid Arthritis: A
Review of the Literature. Sports Med. 2015 Oct;45(10):1401-12
• M. Hurley, K. Dickson, R. Hallett, R. Grant, H. Hauari, N. Walsh, C. Stansfield and S. Oliver. (2018). Exercise interventions and patient beliefs for people with hip, knee or hip and knee osteoarthritis: a mixed methods review. Cochrane
Database of Systematic Reviews, no. 4.
• B. Choi, J. Verbeek, W. Tam and J. Jiang (2010). Exercises for prevention of recurrences of low-back pain. The Cochrane Database for Systematic Reviews, vol. 1
• Guidance from the Chief Medical Officers in the UK on the amount and type of physical activity people should be doing to improve their health. 2019. Access via: https://www.gov.uk/government/collections/physical-activity-guidelines
• Arthritis Research UK. The Musculoskeletal Calculator (prevalence data tool). 2019.
• Hurkmans E, van der Giesen FJ, Vliet Vlieland TP, Schoones J, & Van den Ende EC. (2009). Dynamic exercise programs (aerobic capacity and/or muscle strength training) in patients with rheumatoid arthritis Cochrane Database Syst
Rev. 2009 Oct 7;(4).
• Metsios, GS., &Kitas, GD. (2018). Physical activity, exercise and rheumatoid arthritis: Effectiveness, mechanisms and implementation. Volume 32, Issue 5, October 2018, Pages 669-682.
• Pedersen, B.K., & Saltin, B. (2015). Exercise as medicine- evidence for prescribing exercise as therapy in 26 different chronic disease. Scandinavian Journal of Medicine & Science in Sports. 3, 25: 1-72 Joint Bone Spine. 2016
May;83(3):265-70. doi: 10.1016/j.jbspin.2015.10.002. Epub 2015 Nov 28.
• Verhoeven F, Tordi N, Prati C, Demougeot C, Mougin F, & Wendling D. (2016). Physical activity in patients with rheumatoid arthritis. Joint Bone Spine. 2016 May;83(3):265-70
• Ravalli S, Castrogiovanni P, Musumeci G. Exercise as medicine to be prescribed in osteoarthritis. World J Orthop. 2019;10(7):262–267. Published 2019 Jul 18. doi:10.5312/wjo.v10.i7.262
• Goh SL, Persson MSM, Stocks J, et al. Efficacy and potential determinants of exercise therapy in knee and hip osteoarthritis: A systematic review and meta-analysis. Ann Phys Rehabil Med. 2019;62(5):356–365.
doi:10.1016/j.rehab.2019.04.006
• Public Health England: Muscle and bone strengthening and balance activities for general health benefits in adults and older adults (2018). Sourced from:
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/721874/MBSBA_evidence_review.pdf
• The state of musculoskeletal health 2019: Versus Arthritis. Sourced from: https://www.versusarthritis.org/media/14594/state-of-musculoskeletal-health-2019.pdfThank you
for participating in today’s training
Any Questions?
Tutor: Emma Haughton
t: 03302231302
e: support@puretraininganddevelopment.co.uk
w: www.puretraininganddevelopment.co.uk
/PureTrainingandDevelopment @PureTraining2You can also read

















































