Biosurveillance in Maryland October 2014
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Biosurveillance in Maryland
October 2014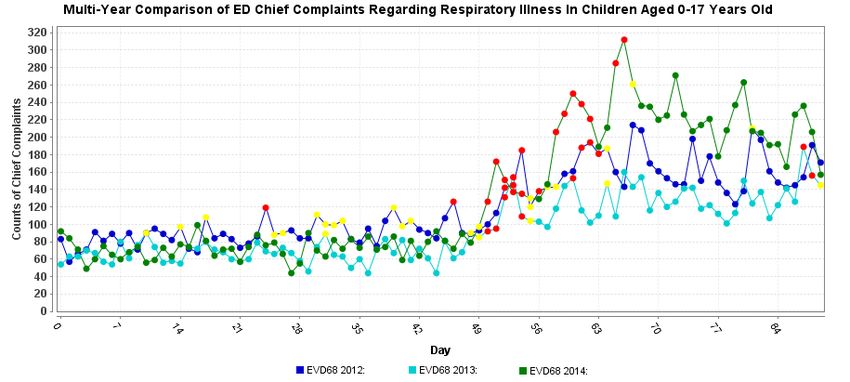
Public Health Goals of Biosurveillance
• Goal:
– Mitigate and/or reduce morbidity and mortality associated with disease
outbreak(s) and/or other public health events
• Objectives:
– Early identification of intentional or natural emerging infectious disease
outbreak(s)
– Expedient public health threat and risk assessment
• Situational awareness
– Prompt application of public health interventions
• Medical counter measure (MCM) distribution
• Social distancing
• Public information messaging
Overview of Maryland ESSENCE
• ESSENCE: Electronic Surveillance System for the Early
Notification of Community-based Epidemics
• ESSENCE is a syndromic surveillance system
– Automated system
– Uses non-traditional data sources
– Based on syndromes rather than diagnoses
– May provide earlier indication of disease outbreaks and
suspicious patterns of illness
– All data sources have statewide coverageESSENCE Capabilities
• Accepts, analyzes, and visualizes multiple data sources:
– Emergency department (ED) visits
• 100% of acute care hospitals in Maryland (n=45) and 2 freestanding
emergency medical facilities report data
– School absenteeism
• 100% of public schools in Maryland report all-cause absenteeism data
– Over-the-counter drug sales
– Poison control center calls
– Reportable disease dataESSENCE Capabilities Continued • Can query by syndrome, sub-syndrome or free text query • Can run queries for multiple syndromes or search criteria simultaneously • Can view aggregate or individual line list data • Can increase data reporting frequency if necessary • Generates alerts based on algorithms for all data sources • Generates alerts based on user defined thresholds or other criteria for all data sources • Has automated process to detect disease clusters • Can restrict user access • Meaningful use ready
ESSENCE EVD-68 Surveillance • Numerous queries are analyzed on a daily basis for patients age 0-17 years old, including: – Respiratory syndrome – Neurological syndrome – Cough sub-syndrome – Difficulty Breathing sub-syndrome – Shortness of Breath sub-syndrome – Wheezing sub-syndrome • School absenteeism is also being monitored
• The above graphs show the counts of chief complaints for the previously mentioned
sub-syndromes related to respiratory illness. The counts began to increase in late
August near the time that EVD-68 became prevalent in the US. The counts leveled
off approximately one month later. However, it is important to compare this year with
previous years to assess if anything is different.• The above graph shows the counts of chief complaints for the respiratory illness sub-
syndromes for 2012, 2013, and 2014. As you can see, each year follows the same
pattern with an increase in mid-August and a plateau approximately one month later.
This year is following a similar pattern, at a higher baseline than the last two years,
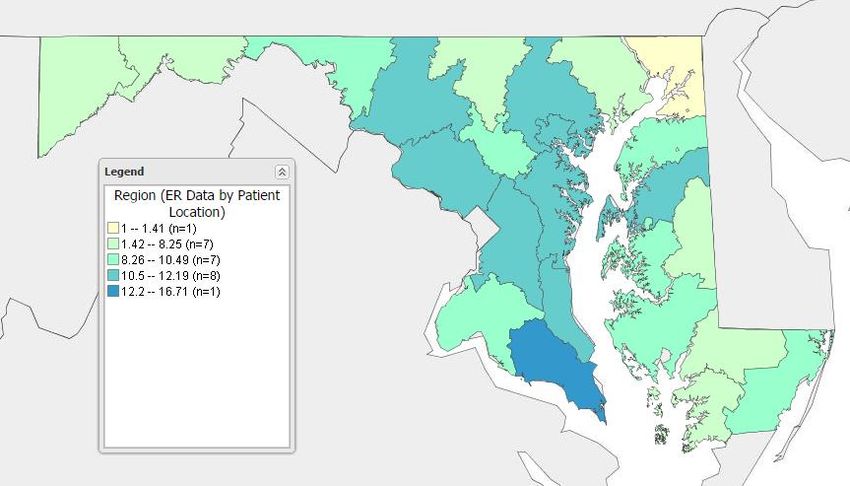
which were relatively mild. The pattern of alerts is similar to previous years as well.The above map shows the chief complaints for all 4 respiratory sub-syndromes combined expressed as a percentage of all chief complaints for each county. For example, in St. Mary's County (represented in dark blue), ED visits for these 4 respiratory sub-syndromes make up 12.2 – 16.71% of all ED visits. Viewing the data in this manner allows epidemiologists to assess which areas of Maryland are impacted the most.
The above graph is a comparison of school absenteeism data in all Maryland public schools for the past two school years. The dates shown are from the beginning of the school year (mid-August) to the present. The percent absenteeism during this school year is slightly higher than last year, but both trends are very similar. There has not been an appreciable increase in absenteeism this year due to respiratory illness or other condition.
Aggregated National Capital Region
ESSENCE (ANCR)
• Aggregated National Capital Region
– DC hospitals
– Northern VA hospitals
– Prince George’s and Montgomery County hospitals
– Over-the-Counter drug sales
– Poison control center calls
• Collaborate with DC and VA epidemiologists
• Monitor during large scale events and mass gatheringsMD ESSENCE Vs. ANCR ESSENCE
Maryland ESSENCE ANCR ESSENCE
All acute care hospitals in MD DC, MD, VA hospitals in the NCR
Only patients visiting MD hospitals Patients visiting any NCR hospital
captured captured
MD residents visiting DC or VA hospitals Captures all MD residents visiting DC or
not captured VA hospitals in the NCR
MD OTC sales NCR OTC sales
Poison control centers Poison control centerESSENCE Ebola Surveillance
• Coordinated with VA and DC to generate a
standardized ED query for all three regions
• Data is reviewed daily and all chief complaints of
interest receive follow-up
• Query focuses on ebola virus disease symptoms and
key words, including:
– Fever, vomiting, diarrhea, bleeding, hemorrhage, ebola, EVD,
Liberia, Guinea, Sierra Leone, etc.• The above graph shows the number of chief complaints generated by the ESSENCE ebola query
on a daily basis since the first US case arrived in Texas on 9/2014.Tri-Jurisdictional Collaboration
• Epidemiologists from MD, VA, and DC work
together to conduct syndromic surveillance
– Shared queries and procedures
– Notification of suspicious ED complaints
– Notification of suspected and confirmed cases of
disease
– Coordinated follow-upYou can also read

















































