Blood Cultures: Practice, Utilization, and Challenges
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
5/19/2020
Blood Cultures:
Practice, Utilization, and Challenges
Kyle G. Rodino, PhD, MLS(ASCP)
Clinical Microbiology Fellow
Mayo Clinic, Rochester, MN
©MFMER | 3793435-1
Disclosures
Relevant Financial Relationship(s):
Nothing to Disclose
Off Label Usage:
Nothing to Disclose
©MFMER | 3793435-2
15/19/2020
Objectives
• Define a blood culture set and the number of blood cultures
needed to diagnose a bloodstream infection
• Identify ways to decrease blood culture contamination
• Describe the impact of antibiotics on blood culture positivity
rates
©MFMER | 3793435-3
Bloodstream Infection (BSI)
• Bacteremia – Presence of bacteria in blood
• “-emia” – condition of the blood (Greek)
• Can range from contamination life threating sepsis or septic shock
- Singer M et al. JAMA 2016; 315:801
Adapted from slide by Dr. Audrey Schuetz - Martin et al. N Engl J Med 2003;348:1546
- Torio CM & Andrews RM. National Inpatient Hospital Costs: The Most Expensive Conditions by
Payer, 2011: Statistical Brief #160. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs
Rockville (MD): Agency for Health Care Policy and Research (US) 2006-2013. ©MFMER | 3793435-4
25/19/2020
Bloodstream Infection (BSI)
• Bacteremia – Presence of bacteria in blood
• “-emia” – condition of the blood (Greek)
• Can range from contamination life threating sepsis or septic shock
• Sepsis – Physiologic and biochemical abnormalities due to a
pathogen in the blood
• High morbidity and mortality; 1 in 4 patients die
• 660,000 cases annually
• Significant economic burden
• Costs attributable to sepsis: $20 billion, or 5.2% of total U.S. hospital
costs in 2011
• Costs are increasing on average annually by 11.9%
- Singer M et al. JAMA 2016; 315:801
Adapted from slide by Dr. Audrey Schuetz - Martin et al. N Engl J Med 2003;348:1546
- Torio CM & Andrews RM. National Inpatient Hospital Costs: The Most Expensive Conditions by
Payer, 2011: Statistical Brief #160. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs
Rockville (MD): Agency for Health Care Policy and Research (US) 2006-2013. ©MFMER | 3793435-5
Sepsis: Why So Elusive?
1. No clear definition of sepsis
• Defined by clinical symptoms which are nonspecific
2. No diagnostic criterion or validated standard diagnostic test
Slide courtesy of Dr. Audrey Schuetz - Surviving Sepsis Campaign.http://www.survivingsepsis.org/Pages/default.aspx.
- Rhodes A et al. Intensive Care Med 2017; 43:304.
- World Sepsis Day. https://www.world-sepsis-day.org/.
©MFMER | 3793435-6
35/19/2020
Sepsis: Why So Elusive?
1. No clear definition of sepsis
• Defined by clinical symptoms which are nonspecific
2. No diagnostic criterion or validated standard diagnostic test
Group of professional organizations
which aims to decrease mortality
from sepsis by:
- Building awareness
- Developing guidelines of care
- Educating healthcare providers
World Sepsis Day, - Facilitating data collection
September 13, 2020
Slide courtesy of Dr. Audrey Schuetz - Surviving Sepsis Campaign.http://www.survivingsepsis.org/Pages/default.aspx.
- Rhodes A et al. Intensive Care Med 2017; 43:304.
- World Sepsis Day. https://www.world-sepsis-day.org/.
©MFMER | 3793435-7
The Definitions of Sepsis Have Changed
1991
Sepsis SIRS criteria
Severe sepsis Sepsis + organ
dysfunction
Septic shock Sepsis-induced
hypotension
despite fluid
resuscitation
SIRS = System inflammatory response syndrome
Bone RC et al. Crit Care Med 1991; 20:864.
Slide courtesy of Dr. Audrey Schuetz
©MFMER | 3793435-8
45/19/2020
The Definitions of Sepsis Have Changed
1991 2016 (Sepsis-3)
Sepsis SIRS criteria* SEPSIS - Life-threatening organ
dysfunction caused by a dysregulated
Severe sepsis Sepsis + organ host response to infection
dysfunction
Septic shock Sepsis-induced SEPTIC SHOCK - Subset of sepsis in
hypotension which abnormalities are profound
despite fluid enough to substantially affect mortality
resuscitation
*SIRS criteria replaced with Sequential Organ Failure
Assessment (SOFA) score
-Singer M et al. The Third International Consensus Definitions for
Slide courtesy of Dr. Audrey Schuetz Sepsis and Septic Shock (Sepsis-3) JAMA 2016; 315:801.
©MFMER | 3793435-9
The Role of Blood Cultures in the Diagnosis of BSI
• In patients with BSI:
• Detect the organism causing the infection
• Allow for antimicrobial susceptibility testing
• Determine the involvement of a line or other device
Gupta S et al. Chest. 2016; 150(6): 1251
©MFMER | 3793435-10
55/19/2020
The Role of Blood Cultures in the Diagnosis of BSI
• In patients with BSI:
• Detect the organism causing the infection
• Allow for antimicrobial susceptibility testing
• Determine the involvement of a line or other device
• In patients without BSI:
• Establish that an infection is not present
• Aid in reduction of antimicrobial use
• Reduce total cost and hospital stay
Gupta S et al. Chest. 2016; 150(6): 1251
©MFMER | 3793435-11
The Basics of Blood Cultures
Image courtesy of Dr. Robin Patel
©MFMER | 3793435-12
65/19/2020
What’s in a Blood Culture Bottle?
• Designed to enhance growth of microorganisms
• Water
• Nutrients
• Soybean casein-digest, broth, vitamins, sugar, amino acids, etc.
• Anticoagulant: Sodium polyanethol sulfonate (SPS)
• Neutralizes lysozyme, inhibits phagocytosis and complement cascade
• Increases rate/speed of growth for many bacteria
• Resins
• Absorb antimicrobials… to some degree
• Provide increased surface area for growth
• Anaerobic bottles: Contain N2 and CO2, no O2
©MFMER | 3793435-13
What Type of Blood Bottle to Use?
Aerobic
• Most BSIs due to
aerobic/facultative
bacteria
• If limited volume,
inoculate aerobic
bottle first
*Bottles are examples and are available from multiple manufacturers
Images courtesy of Beth Marx
©MFMER | 3793435-14
75/19/2020
What Type of Blood Bottle to Use?
Aerobic Anaerobic
• Most BSIs due to • For adults,
aerobic/facultative recommend pairing
bacteria with aerobic bottle
• If limited volume, • Anaerobic BSIs
inoculate aerobic • Abscess
bottle first • GI
• Anaerobic BSI in
peds is rare
*Bottles are examples and are available from multiple manufacturers
Images courtesy of Beth Marx
©MFMER | 3793435-15
What Type of Blood Bottle to Use?
Aerobic Anaerobic Pediatric
• Most BSIs due to • For adults, • Lower blood:broth
aerobic/facultative recommend pairing ratio (1:5)
bacteria with aerobic bottle • Lower levels of
• If limited volume, • Anaerobic BSIs media components
inoculate aerobic • Abscess • Functions similar to
bottle first • GI adult aerobic bottle
• Anaerobic BSI in
peds is rare
*Bottles are examples and are available from multiple manufacturers
Images courtesy of Beth Marx
©MFMER | 3793435-16
85/19/2020
Specialized Blood Culture Bottles
• Fungi/Mycobacteria
• Designed for improved recovery
of Mycobacterium spp. and some
fungi
• Extended incubation; e.g. 42
days
*Bottles are examples and are available from multiple manufacturers
Images courtesy of Beth Marx
©MFMER | 3793435-17
Specialized Blood Culture Bottles
• Fungi/Mycobacteria • Lysis Centrifugation
• Designed for improved recovery • Media lyses cells, inactivates
of Mycobacterium spp. and some complement
fungi • After centrifugation, sediment is
• Extended incubation; e.g. 42 inoculated to solid/liquid media
days • Advantages
• Increased recovery of some fungi;
e.g. Histoplasma spp., M. furfur
• Also some fastidious bacteria
• Disadvantages
• Open system → opportunity for
*Bottles are examples and are available from multiple manufacturers
contamination
Images courtesy of Beth Marx
©MFMER | 3793435-18
95/19/2020
Blood Culture Contamination
Common contaminants include:
• Indicators of contamination • Bacillus spp.
• Corynebacterium spp.
• Organisms commonly found on skin • Micrococcus spp. and related Kocuria spp.
• Cutibacterium (Propionibacterium) spp.
• Present in 1 set of ≥2 sets • Coagulase-negative staphylococci
• Viridans group streptococci
• Delayed time to detection
• Contamination rates are tracked, as required by the College of
American Pathologists
• ≤3% is an acceptable blood culture contamination rate
• 2.5% median contamination rate
Schifman RB et al. Arch Pathol Lab Med 1998; 122:216.
©MFMER | 3793435-19
The Cost of False-Positive Blood Cultures
• Financial
• Study looking at ~5400 blood cultures from ED at a large university
• $8,720 additional charged with false-positive blood culture compared to
negative culture
Gander RM et al. J Clin Microbiol. 2009; 47:1021 .
©MFMER | 3793435-20
105/19/2020
The Cost of False-Positive Blood Cultures
• Financial
• Study looking at ~5400 blood cultures from ED at a large university
• $8,720 additional charged with false-positive blood culture compared to
negative culture
• Patient
• Many false-positive cultures are from Gram-positive organisms =
vancomycin
• Side effects of vancomycin
• Time and cost of drug level monitoring
• Increased length of stay for intravenous treatment
• Potential for C. difficile infection and other impacts of microbiota
• Need for catheter placement for IV therapy
Gander RM et al. J Clin Microbiol. 2009; 47:1021 .
©MFMER | 3793435-21
Preventing Blood Culture Contamination
Disinfection
• Over 180 bacterial species are found as normal
inhabitants of skin
• Skin preparation
• Clean with 70% isopropyl alcohol, dry for 30 sec
Photo courtesy of Bobbi Pritt, MD
• Apply antiseptic, dry for 60 sec
Photo courtesy of Bobbi Pritt, MD
Note: iodine-based antiseptic shown.
Various institutions use different antiseptics.
Slide modified from Dr. Audrey Schuetz
©MFMER | 3793435-22
115/19/2020
Preventing Blood Culture Contamination
Disinfection
• Over 180 bacterial species are found as normal
inhabitants of skin
• Skin preparation
• Clean with 70% isopropyl alcohol, dry for 30 sec
Photo courtesy of Bobbi Pritt, MD
• Apply antiseptic, dry for 60 sec
Culture of site Same site, after
prior to aseptic proper aseptic
scrub technique scrub
Photo courtesy of Bobbi Pritt, MD
Note: iodine-based antiseptic shown.
Photo courtesy of Bobbi Pritt, MD Various institutions use different antiseptics.
Slide modified from Dr. Audrey Schuetz
©MFMER | 3793435-23
Choice of Antiseptic
• Chlorhexidine gluconate (CHG) and tincture of iodine (iodine +
alcohol) are preferred to povidone-iodine
• CHG preferred because:
• Faster drying
• Less messy
• Fewer allergies
• CHG not recommended for children5/19/2020
Preventing Blood Culture Contamination
Diversion Devices
• Divert and sequester first 1.5-2 mL of blood
• Rationale
• Bacteria can be present in “skin plug”
• Port or line may have colonizing bacteria
Zimmerman et al. Clin Infect Dis 2019
Rupp et al. Clin Infect Dis 2017
Binkhamis et al. J Clin Micro 2014
Skoglund et al. J Clin Micro 2019
©MFMER | 3793435-25
Preventing Blood Culture Contamination
Diversion Devices
• Divert and sequester first 1.5-2 mL of blood
• Rationale
• Bacteria can be present in “skin plug”
• Port or line may have colonizing bacteria
• Diversion devices reduce blood culture contamination
• Degree of reduction multifactorial
• Current contamination rate
• Dedicated, highly trained phlebotomy staff
• Cost benefit of diversion devices impacted by many factors
Zimmerman et al. Clin Infect Dis 2019
Rupp et al. Clin Infect Dis 2017
Binkhamis et al. J Clin Micro 2014
Skoglund et al. J Clin Micro 2019
©MFMER | 3793435-26
135/19/2020
Preventing Blood Culture Contamination
Diversion Devices
Diversion Standard Procedure P value
Devices
Contamination rate 2/904 (0.22%)* 16/904 (1.8%)** 0.001
Sensitivity (true bacteremia rate) 7.2% 7.6% 0.41
% Cultures representing true positives 65/67 (97%) 69/85 (81%)
*1 coagulase-negative staphylococcus (CoNS), 1 Corynebacterium spp.
**Contaminating Organisms with Standard Discordant Cultures
Procedure, n=16 Device +/ Standard (-) Standard +/ Device (-)
CoNS
Klebsiella (4) E. coli (2)
Corynebacterium S. aureus (2) S. aureus (2)
Cutibacterium Enterococcus (2) S. pneumoniae (2)
S. pneumoniae (1) Morganella (2)
Viridans strep
E. coli (1) S. pyogenes (1)
Micrococcus Peptostreptococcus (1) Enterobacter (1)
H. influenzae (1)
C. albicans (1)
Rupp ME et al. Clin Infect Dis 2017; 65:201.
Slide courtesy of Dr. Audrey Schuetz
©MFMER | 3793435-27
Which Sites to Draw?
• Draw from veins, not arteries
• No increased yield with arterial blood
• At least one set should be from peripheral venipuncture
• Cultures from indwelling intravascular access devices show higher
contamination rates
• Need a set from the peripheral draw for comparison
©MFMER | 3793435-28
145/19/2020
How Many Bottles to Draw?
• Blood Culture Set
• All bottles collected from a single venipuncture
• Can be comprised of 2-3 bottles; at least 1 aerobic and 1 anaerobic
blood culture bottle
• Blood Culture Order
• 2 sets drawn simultaneously (within short time frame)*
• Avoid single set orders
• Inadequate volume for optimal sensitivity
• Complicates interpretation of potential contamination
*Exception: Interval draws for suspected endocarditis
©MFMER | 3793435-29
What is the Optimal Blood Draw Volume?
Studies reporting percent sensitivity based on blood culture volume
Volume
Washington 1975 Cockerill 2004 Lee 2007 Patel 2011
1 bottle = 10 mL
20 mL 80% 65.1% 73.1% 70.5%
40 mL 89% 80.4% 89.7% 82.1%
60 mL 99% 95.7% 98.2% 91.9%
• Optimal organism recovery with 60 mL blood draws
- Washington. Mayo Clin Proc. 1975, 50:91
- Cockerill. Clin Infect Dis. 2004, 38:1724-30
- Lee et al. J Clin Microbiol. 2007, 45:3546
- Patel et al. J Clin Microbiol. 2011, 49:4047
Table Adapted from Dr. Tom Grys - Cheruvanky. J Clin Microbiol. 2016, 54:64-67
©MFMER | 3793435-30
155/19/2020
What is the Optimal Blood Draw Volume?
Studies reporting percent sensitivity based on blood culture volume
Volume
Washington 1975 Cockerill 2004 Lee 2007 Patel 2011
1 bottle = 10 mL
20 mL 80% 65.1% 73.1% 70.5%
40 mL 89% 80.4% 89.7% 82.1%
60 mL 99% 95.7% 98.2% 91.9%
• Optimal organism recovery with 60 mL blood draws
• 60 mL draws have been shown to…
• Increase detection
• Decrease morbidity and mortality
• Have a positive financial impact on BSI related care
- Washington. Mayo Clin Proc. 1975, 50:91
- Cockerill. Clin Infect Dis. 2004, 38:1724-30
- Lee et al. J Clin Microbiol. 2007, 45:3546
- Patel et al. J Clin Microbiol. 2011, 49:4047
Table Adapted from Dr. Tom Grys - Cheruvanky. J Clin Microbiol. 2016, 54:64-67
©MFMER | 3793435-31
What Bottle Combination to Achieve 60 ml?
Number of patients, by volume of blood
3 sets of 2 bottles
10 ml 20 ml 30 ml 40 ml 50 ml 60 ml
• Total: 3 aerobic, 3 anaerobic 2 BACTEC Plus Aerobic/F and 1 BACTEC Lytic/10 Anaerobic/F bottle
Positive Cultures 545 683 738 805 859 893
2 sets of 3 bottles (2 aero, 1 ana) Pathogens detected 584 744 801 885 954 989
• Total: 4 aerobic, 2 anaerobic 1 BACTEC Plus Aerobic/F and 1 BACTEC Lytic/10 Anaerobic/F bottle
(simulated)
• Most BSI due to aerobic organisms Positive Cultures 545 683 761 824
• Eliminate additional venipuncture Pathogens detected 584 744 840 917
2 BACTEC Plus Aerobic/F resin bottles (simulated)
Positive Cultures 545 622 708 754
Pathogens detected 584 666 770 819
Patel R et al. J Clin Microbiol 2011;49:4047
©MFMER | 3793435-32
165/19/2020 Fill Volume Impacts Blood Culture Sensitivity • Organism burden in blood is low •
5/19/2020
Example of Blood Culture Inoculation Guide for
Adults
Order of Inoculation (Left to Right)
Volume Gray Purple Gray
(Aerobic) (Anaerobic) Aerobic
21-30 ml Divide equally: 7-10 ml 7-10 ml 7-10 ml
10-20 ml Divide equally: 5-10 ml 5-10ml
40 30.0 10.0 10.0 10.0
• 0.5-1 mL minimum volume Appropriate volumes and bottles to inoculate according to
weight
Table Courtesy of Dr. Audrey Schuetz
©MFMER | 3793435-36
185/19/2020
The Impact of Antibiotics on Blood Cultures
• Blood cultures should be drawn before the initiation of antibiotics
• Blood culture positivity decreases by ≥50% within two hours of IV antibiotic
treatment
Probability of Mortality
• Blood cultures should be drawn 40
35 32.3 33.1
promptly to avoid treatment delay 30 27 27.9 28.8
24.6 25.9
• 6
Hours
Graph adapted from Ferrer R et al. Crit Care Med 2014; 42:1749
©MFMER | 3793435-37
Blood Culture Quality Metrics
• Tracking contamination rates
• College of American Pathologists (CAP) checklist item requires
monitoring of the contamination rate
• ≤3% contamination rate is the national benchmark
©MFMER | 3793435-38
195/19/2020
Blood Culture Quality Metrics
• Tracking contamination rates
• College of American Pathologists (CAP) checklist item requires
monitoring of the contamination rate
• ≤3% contamination rate is the national benchmark
• Bottle fill volume monitoring
• Verify the fill volume of bottles received in the lab
• Must be able to provide evidence of monitoring and feedback
©MFMER | 3793435-39
Blood Culture Quality Metrics
• Tracking contamination rates
• College of American Pathologists (CAP) checklist item requires
monitoring of the contamination rate
• ≤3% contamination rate is the national benchmark
• Bottle fill volume monitoring
• Verify the fill volume of bottles received in the lab
• Must be able to provide evidence of monitoring and feedback
• Single blood culture in 24 hours
• Discourage collection of solitary blood cultures
• Provider feedback related to consensus recommendation for ≥2 sets per
draw
©MFMER | 3793435-40
205/19/2020
After Collection, Where Do They Go?
©MFMER | 3793435-41
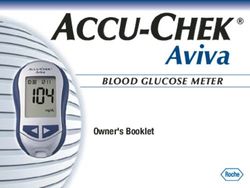
What Happens After the Draw?
• Send bottles promptly to the laboratory
• 2 hours maximum transport time
• Room temperature
Images courtesy of Dr. Robin Patel
©MFMER | 3793435-42
215/19/2020
What Happens After the Draw?
• Send bottles promptly to the laboratory
• 2 hours maximum transport time
• Room temperature
• In clinical microbiology processing area
• Verify labels and orders
• Track bottles into laboratory information system
• Check for damaged bottles
• Verify the fill volume
• Bottles loaded onto the blood culture instrument
Images courtesy of Dr. Robin Patel
©MFMER | 3793435-43
How Does an Automated Blood Culture Instrument
Work?
• Incubates bottles for 5 days
• >90% of positives will signal within 48 hours
©MFMER | 3793435-44
225/19/2020
How Does an Automated Blood Culture Instrument
Work?
• Incubates bottles for 5 days
• >90% of positives will signal within 48 hours
• Periodically monitors bottles, plotting results over 5 day period
• Reading ~10 mins
• Looks for changes in growth indicator
©MFMER | 3793435-45
How Does an Automated Blood Culture Instrument
Work?
• Incubates bottles for 5 days
• >90% of positives will signal within 48 hours
• Periodically monitors bottles, plotting results over 5 day period
• Reading ~10 mins
• Looks for changes in growth indicator
• Sensing growth
• CO2 production from actively metabolizing organisms
• Colorimetric or Fluorometric
• O2 consumption resulting in pressure changes
• Headspace pressure transducer
©MFMER | 3793435-46
235/19/2020
Automated Alert to Positive Culture
Images courtesy of Dr. Robin Patel
©MFMER | 3793435-47
What Happens When a Bottle Signals Positive?
• Gram stain performed from the bottle
• Read microscopically to determine the Gram
characteristics of the organism
Images courtesy of Dr. Robin Patel
©MFMER | 3793435-48
245/19/2020
What Happens When a Bottle Signals Positive?
• Gram stain performed from the bottle
• Read microscopically to determine the Gram
characteristics of the organism
• Preliminary identification of organism
• e.g., “Gram-positive coccus resembling
Streptococcus”
• Technologist phones physician to notify of
positive blood culture - provides Gram stain
result
Images courtesy of Dr. Robin Patel
©MFMER | 3793435-49
What Happens When a Bottle Signals Positive?
• Subculture the positive blood culture bottle
• Media determined by the organism seen on Gram stain
• Streak for isolation
• Allow plates to incubate and examine
Images courtesy of Dr. Robin Patel
©MFMER | 3793435-50
255/19/2020
What Happens When a Bottle Signals Positive?
• Subculture the positive blood culture bottle
• Media determined by the organism seen on Gram stain
• Streak for isolation
• Allow plates to incubate and examine
• Pure or mixed culture?
• Identify the organism
• Matrix-assisted laser desorption ionization time-of-flight
mass spectrometry – MALDI-TOF MS
• Biochemicals – automated, tubed
• Molecular methods – e.g. DNA sequencing
Images courtesy of Dr. Robin Patel
©MFMER | 3793435-51
What Happens When a Bottle Signals Positive?
• Subculture the positive blood culture bottle
• Media determined by the organism seen on Gram stain
• Streak for isolation
• Allow plates to incubate and examine
• Pure or mixed culture?
• Identify the organism
• Matrix-assisted laser desorption ionization time-of-flight
mass spectrometry – MALDI-TOF MS
• Biochemicals – automated, tubed
• Molecular methods – e.g. DNA sequencing
• Perform antimicrobial susceptibility testing
Images courtesy of Dr. Robin Patel
©MFMER | 3793435-52
265/19/2020
Improving Turnaround Time with Rapid Diagnostics
Traditional 12-18 h ~24 h ~48 h Total: 4 days
Workflow
Modified from slide by Dr. Audrey Schuetz
©MFMER | 3793435-53
Improving Turnaround Time with Rapid Diagnostics
Traditional 12-18 h ~24 h ~48 h Total: 4 days
Workflow
~2 h • Rapid Organism ID
Rapid ID +/- • Molecular Resistance Determinants
Antimicrobial 12-18 h
Resistance • Rapid Organism ID
~8 h • Rapid Phenotypic AST
Modified from slide by Dr. Audrey Schuetz
©MFMER | 3793435-54
275/19/2020
Impact of Rapid Blood Culture Diagnostics
• Full benefit realization depends on the diagnostic platform,
reporting comments, and stewardship intervention
• Rapid results reduced treatment of contaminants and use of
broad-spectrum antibiotics
• Reporting comments included with the result
• Stewardship intervention resulted in de-escalation of antibiotics
• Rapid ID with rapid phenotypic AST
• Resulted in faster antibiotic changes for Gram-negative bacteria BSI
Banerjee, R, et al. CID. 2015
Banerjee, R, et al. CID 2020
©MFMER | 3793435-55
Stewardship Guidelines for Rapid Blood Culture Testing
Infectious Diseases Society of America and Society for Healthcare Epidemiology of America
• IDSA/SHEA expert panel reviewed studies involving
rapid molecular assays and MALDI
• Both identification and antimicrobial susceptibility
testing
Barlam TF et al. Clin Infect Dis 2016; 62:e51.
©MFMER | 3793435-56
285/19/2020
Stewardship Guidelines for Rapid Blood Culture Testing
Infectious Diseases Society of America and Society for Healthcare Epidemiology of America
• IDSA/SHEA expert panel reviewed studies involving
rapid molecular assays and MALDI
• Both identification and antimicrobial susceptibility
testing
• Significant associations between rapid testing and
patient outcomes were seen with:
• Combination of rapid testing with antimicrobial
stewardship support
• Performance of rapid testing “continuously (i.e.,
24/7) or at least in frequent batches”
Barlam TF et al. Clin Infect Dis 2016; 62:e51.
©MFMER | 3793435-57
Improving Turnaround Time with Rapid Diagnostics
Traditional 12-18 h ~24 h ~48 h Total: 4 days
Workflow
~2 h • Rapid Organism ID
Rapid ID +/- • Molecular Resistance Determinants
Antimicrobial 12-18 h
Resistance • Rapid Organism ID
~8 h • Rapid Phenotypic AST
Modified from slide by Dr. Audrey Schuetz
©MFMER | 3793435-58
295/19/2020
Improving Turnaround Time with Rapid Diagnostics
Traditional 12-18 h ~24 h ~48 h Total: 4 days
Workflow
~2 h • Rapid Organism ID
Rapid ID +/- • Molecular Resistance Determinants
Antimicrobial 12-18 h
Resistance • Rapid Organism ID
~8 h • Rapid Phenotypic AST
Sample to ~5 h • Rapid Organism ID
Answer • Molecular Resistance Determinants
• Predictive AST
Modified from slide by Dr. Audrey Schuetz
©MFMER | 3793435-59
Summary
• Blood cultures play a key role in combating sepsis
• Adequately clean the skin to avoid contamination
• Draw blood cultures before antibiotic administration
• Blood volume is important
• Fill bottles appropriately
• Obtain at least two sets; 60 mL total volume is optimal
• Advanced technologies are improving blood culture TAT
• Reporting comments can aid clinicians
• Stewardship is key to success
©MFMER | 3793435-60
305/19/2020
QUESTIONS & DISCUSSION
©MFMER | 3793435-61
Next Upcoming Webinar
Capillary Puncture vs. Venipuncture
Brad Karon, M.D., Ph.D.
August 19, 2020
11am-12pm CT
© MFMER | slide-62
31You can also read