CalAIM: Equity Considerations - The 2021-22 Budget
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The 2021-22 Budget:
CalAIM: Equity Considerations
MARCH 2021
The California Advancing and Innovating withdrawn proposal, and analyzes overarching
Medi-Cal (CalAIM) proposal is a far-reaching set issues related to the proposal. The second post
of reforms to expand, transform, and streamline in this series analyzes CalAIM financing issues,
Medi-Cal service delivery and financing. This including both the Governor’s funding plan for
post—the third in a series assessing different CalAIM as well as CalAIM’s policy changes related
aspects of the Governor’s proposal—analyzes to Medi-Cal financing. The fourth post in this
equity considerations in the CalAIM proposal. The series will assess how CalAIM could affect the care
first post in this series provides an overview of provided to seniors and persons with disabilities
CalAIM, including the key changes from last year’s served by Medi-Cal.
Background
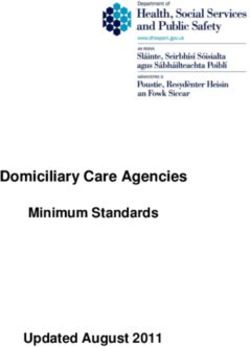
What Are Health Disparities and Health definition, while a widening of such disparities
Equity? Health disparities and health equity does the opposite. Coronavirus disease 2019
are concepts that have no universally accepted (COVID-19) has accentuated health disparities in
definition. As such, this post uses a broad California as seen in Figure 1 on the next page
definition of the terms. Health disparities, under which breaks down differences in life expectancy
this broad definition, exist when a particular and COVID-19 mortality by select racial or ethnic
population group experiences systematically group.
worse health or greater health risks than another Health Disparities Are Significantly Driven
population group. Population groups can by a Variety of Medical and Nonmedical
be categorized in different ways, such as by Determinants of Health. The determinants
demographic characteristics such as race and of health are the range of personal, social,
gender, geography, socioeconomic status, or other environmental, and medical factors that influence
factors such as access to housing. Population health status. The following bullets distinguish
groups that may experience worse health and give a sense of the relative magnitude of the
outcomes can include people of color, low-income different medical and nonmedical determinants
individuals, and homeless or housing-insecure of health as drivers of health status. Figure 8,
individuals. For instance, individuals experiencing later in this post, breaks out many of the health
homelessness are disproportionately likely to determinants we identified in our review of the
develop health conditions such as mental illness, research and indicates which determinants different
which is associated with comorbidities and higher CalAIM components are intended to address.
premature death rates. Most often, academic
research measures health disparities in terms of • Medical Determinants. We find that
differences in mortality, though other measures differences in access to health care explain
such self-reported health status, diagnosed chronic as much as 20 percent of health disparities.
conditions, and disability are sometimes used. Notably, these medical determinants of
The narrowing of health disparities corresponds health have been found to explain differences
to improvements in health equity, under this broad in health disparities even after accounting
2 0 21-2 2 L AO B u d g e t S e r i e s 1Figure 1 security), health behaviors
(such as diet and alcohol,
Racial and Ethnic Disparities Exist in Terms of tobacco, and drug use), and
Life Expectancy and COVID-19 Mortality
environmental factors (such as
California
air or water quality). Nonmedical
Life Expectancy COVID-19 Death Rate
(Age in Years)a
determinants of health are
(Deaths per 100,000 Residents)b
among the most systematic
Asian differences between certain
population groups, such as racial
Black
and ethnic groups, and therefore
explain much of the disparity in
Hispanic
health outcomes between those
White
groups. Accordingly, changes
to such groups’ nonmedical
70 75 80 85 90 30 60 90 120 150 circumstances could improve
a 2017 data. their health and, as a result,
b Data is up to date through February 2021. reduce health disparities.
Note: There are significant differences in mortality within each racial or ethnic group. For example,
the Asian category comprises many different ethnic groups and we understand there is
Medi-Cal Provides Health
variation among these ethnic groups in terms of life expectancy and COVID-19 death rates. Care Coverage to Populations
COVID-19 = coronavirus disease 2019. Who Suffer Disparate Health
Outcomes. Medi-Cal provides
health care coverage to more
than one-third of the state’s
for other nonmedical determinants of
population. In part by covering low-income
health (which we discuss below). These
individuals and families, Medi-Cal disproportionately
differences include factors such as health
serves state residents whose socioeconomic
insurance status and the quality of health
and health characteristics are associated with
care provided. Research indicates individuals
poor health outcomes. For example, Medi-Cal
from disadvantaged population groups
disproportionately covers state residents who
often receive lower-quality care than others
are out of work, disabled, and/or do not have a
from more advantaged population groups.
college degree. Additionally, people of color are
For example, some studies suggest the
disproportionately represented in Medi-Cal relative
existence of systemic disparities in the quality
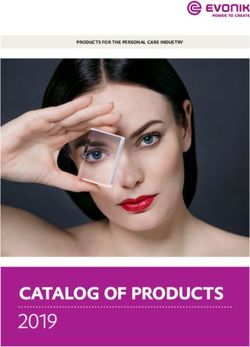
to the overall population. As Figure 2 on the
of preventive care different groups receive,
next page shows, Medi-Cal beneficiaries suffer
leading to more preventable emergency
worse health on a variety of dimensions compared
department visits. Other research indicates
to other state residents (which largely includes
that racial bias or deficiencies in cultural
those with other forms of coverage but also the
competency on the part of some clinicians
uninsured).
can adversely affect the quality of care they
Health Disparities Exist Within the Population
provide.
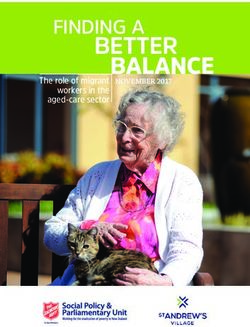
Served by Medi-Cal. Health disparities are
• Nonmedical Determinants. Following our
present among Medi-Cal beneficiaries of different
review of academic literature, we find that the
races or ethnicities. For example, as shown in
nonmedical determinants of health likely are
Figure 3 on page 4, compared to white Medi-Cal
responsible for 80 percent or more of health
recipients below age 65, non-senior Black Medi-Cal
disparities. Nonmedical determinants include
beneficiaries self-report poor or fair health (the two
social determinants (such as income, housing
worst ratings) at 30 percent higher rates. Hispanics
status, racism and discrimination, intentional
below age 65 on Medi-Cal, on the other hand,
and unintentional physical harm, and food
2 0 21-2 2 L AO B u d g e t S e r i e s 2Figure 2
can result in premature death.
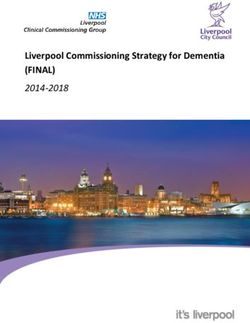
Figure 4 on page 5 compares
Medi-Cal Beneficiaries Suffer Worse Health the prevalence of major
Outcomes Than Non-Medi-Cal Beneficiaries chronic conditions among
the top 5 percent most costly
20% beneficiaries compared to
Poor or fair overall health
10% Medi-Cal enrollees overall. In
addition to having low incomes,
40% which is true for all Medi-Cal
Poor or fair dental health
20% enrollees, those who suffer from
the listed chronic conditions may
come disproportionately from
4%
Has no natural teeth Medi-Cal particular population groups—
1%
Not Medi-Cal such as individuals lacking stable
(Rest of State Population)
housing or persons of color. For
15%
Ever diagnosed with diabetes example, Black and Hispanic state
9%
residents have higher rates of
diabetes and Black state residents
Ever diagnosed with
34% experience homelessness at very
high blood pressure 29% disproportionate rates.
State Has Attempted to
20% Reduce Health Disparities
Recently experienced serious
psychological distress 13% Through Various Medi-Cal
Initiatives. As previously
discussed, the Medi-Cal
Source: California Health Interview Survey, 2018 or 2019 edition depending on the specific measure
(due to data constraints). program serves individuals who
disproportionately suffer from
a myriad of health conditions
and face other circumstances
report poor or fair health at 24 percent lower rates associated with poor health.
than non-senior white recipients. Accordingly, changes to the Medi-Cal program
Health disparities also can be seen by looking that result in improved access to care or quality
at how service needs vary among Medi-Cal of care have significant potential to reduce
beneficiaries. The top 5 percent most costly health disparities. In recent years, the state has
beneficiaries, on a per-enrollee basis, utilize over implemented several reforms to the Medi-Cal
30 times as many resources, in dollar terms, as program, which, in concept, have potential to
the least 50 percent costly. This illustrates that a reduce health disparities across the state. These
relatively small number of Medi-Cal beneficiaries reforms included (1) expanding Medi-Cal coverage
have extremely disproportionate needs compared to additional populations—such as to single adults
to more typical Medi-Cal beneficiaries. Moreover, under the Patient Protection and Affordable Care
the top 5 percent most costly beneficiaries Act (ACA) optional expansion and to undocumented
disproportionately suffer from certain chronic immigrants under age 26—and (2) establishing
conditions—including mental illness, diabetes, programs that focus resources and attention on
hypertension, asthma, and alcohol and drug the highest-risk, highest-needs beneficiaries,
dependency—compared to Medi-Cal enrollees often with the intent to prevent the worsening of
overall. Such chronic conditions often are severe health conditions. (The latter can serve to
accompanied by comorbidities, which significantly address disparities since certain population groups
impair the overall health of beneficiaries and disproportionately may be high-risk, high-need.)
2 0 21-2 2 L AO B u d g e t S e r i e s 3Figure 3 Twenty-four counties and one city
have opted in to the Whole Person
Self-Reported Health Differs Among Care program. As of September
Medi-Cal Beneficiaries by Race and Ethnicity 2020, about 86,000 people were
Medi-Cal Beneficiaries Ages 0-64 participating in Whole Person
Care.
Overall Self-Reported Health by Race or Ethnicity
• Health Homes. The Health
Poor or Fair Excellent or Very Good Homes Program, which was
Asian 18% 55% implemented in 2018, has similar
goals to the Whole Person
Black 25% 57% Care program and provides
extra services—including care
Hispanic 15% 58%
management—to Medi-Cal
White 19% 55% beneficiaries who suffer from
chronic health and/or mental
health conditions that result in
high use of health care services.
Relative Likelihood of Reporting Being in Poor or Fair Health
Compared to White Medi-Cal Beneficiaries Twelve counties—with managed
care plans arranging and
paying for services within these
Asian -5% counties—are participating in
the Health Homes Program. As
Black 30% of March 2020, Health Homes
served about 27,000 beneficiaries.
-24% Hispanic
This program also is set to expire
at the end of 2021.
• Mental Health Services
Source: California Health Interview Survey, 2019 edition.
Act (MHSA) Full-Service
Partnerships. Approved by voters
Three of these programs include: in 2004, MHSA places a 1 percent
tax on incomes over $1 million and dedicates
• Whole Person Care. The Whole Person Care the vast majority of associated revenues to
program, which began in 2016, is a set of counties to provide mental health services.
local pilot programs—typically run by county A substantial portion of the MHSA funding
health agencies—to coordinate physical counties receive is required to be used on
health, behavioral health, and social services Full-Service Partnerships, which provide
for beneficiaries with the highest levels of intensive mental health and wraparound
need and/or risk. Each local Whole Person services—such as housing, employment
Care pilot determines target populations— support, and case management—to
among a predetermined set which includes, individuals with the greatest mental health
for example, high utilizers of services and needs. Full-Service Partnerships are intended
homeless individuals—and develops strategies to provide services to populations—identified
to tailor service delivery to those groups. The by counties—who disproportionately do
program is funded with a mix of federal and not access mental health care. Counties
local funds and is set to expire at the end of use a variety of dimensions to identify
2021. Notably, additional state-only funding these populations, which include (1) racial
also has been provided to Whole Person or ethnic characteristics, (2) housing
Care pilots to support housing services. status, or (3) criminal justice involvement.
2 0 21-2 2 L AO B u d g e t S e r i e s 4Figure 4
Care and/or Health Home
programs.
Certain Chronic Conditions Are Much More Prevelant Governor Proposed CalAIM
Among the Most Costly Medi-Cal Beneficiaries
as Part of the January 2020-21
Comparison of the 5 Percent Most Cosly and 95 Percent Least Costly
Medi-Cal Beneficiaries With the Listed Chronic Condition
Budget Before Withdrawing
the Proposal in May. CalAIM
is a large package of reforms
aimed at (1) reducing health
45% disparities by focusing attention
Serious mental health
5% and resources on Medi-Cal’s
high-risk, high-need populations;
(2) rethinking behavioral
27%
Hypertension health service delivery and
4%
financing, (3) transforming and
streamlining managed care, and
21% (4) extending federal funding
Diabetes
3% opportunities currently available
under the state’s soon-to-expire
1115 waiver. Originally proposed
11%
Asthma Top 5 Percent Bottom 95 Percent
in January 2020 as part of the
5%
2020-21 budget, CalAIM was
withdrawn at the May Revision
10% due to the COVID-19 pandemic
Alcohol and drug
dependency 1% and its estimated effects on
the state’s fiscal situation. To
maintain continuity of certain
Medi-Cal programs such as
Source: Department of Health Care Services Analysis of 2011 expenditure data.
Whole Person Care and the
Dental Transformation Initiative—
whose federal authorization
While not an explicit Medi-Cal program,
under the state’s 1115 waiver would have expired
Full-Service Partnerships provide services
at the end of 2020—the state secured a one-year
to many individuals eligible for Medi-Cal
extension of the 1115 waiver. With this extension,
and, accordingly, are often partially
the state’s 1115 waiver is set to expire on
Medi-Cal-funded.
December 31, 2021.
Figure 5 on the next page shows the counties
that currently are participating in the Whole Person
2 0 21-2 2 L AO B u d g e t S e r i e s 5Figure 5
Whole Person Care and/or Health Homes Are Available in 26 Counties
All Counties Operate Full-Service Partnerships
Whole Person Care
Health Homes
Both
Whole Person Care operated by City of Sacramento.
Counties that offer Whole Person Care
and/or Health Homes include roughly
87 percent of Medi-Cal beneficiaries statewide.
2 0 21-2 2 L AO B u d g e t S e r i e s 6Governor’s Proposal
Overall Proposal Proposal Elements With Direct Health
Reintroduces CalAIM in Largely Similar Equity Implications
Form to Last Year’s Proposal. The Governor’s CalAIM reflects a large suite of proposed reforms
2021-22 budget reintroduces CalAIM. The vast that touch nearly every aspect of Medi-Cal. While
majority of proposed CalAIM reforms are essentially essentially all of CalAIM has potential to improve
unchanged from last year’s proposal except as health equity, certain CalAIM components are more
relates to their proposed implementation time line. directly intended to do so. This section describes
The Governor’s reintroduced proposal emphasizes the major components of CalAIM that are intended
health equity as an important rationale for pursuing to directly have such impacts.
CalAIM. For a general overview of CalAIM, see our Better Identification of High-Risk, High-Need
budget post, The 2021-22 Budget: CalAIM: The Beneficiaries Through Population Health
Overarching Issues. Management Programs. Population health
CalAIM Reflects One of the Governor’s management programs represent a bundle of
Proposals Aimed at Health Equity. The administrative activities—typically performed
Governor’s 2021-22 budget includes a number of by managed care plans—that aim to (1) identify
proposals that the Governor intends to improve beneficiaries’ medical and nonmedical risks
health equity. While many of the new proposals and needs and (2) facilitate care coordination
aim to improve reporting on health equity metrics, and referrals. CalAIM would require all Medi-Cal
others would expand benefits with the goal of more managed care plans to operate population
directly improving health equity. The major health health management programs. Managed care
and human services proposals either wholly or plans would be required to collect and analyze
partially intended by the administration to address information on their members’ health status,
health equity include: service utilization history, and social needs. While
existing data sources would form the basis of
• Development of a Health and Human Services
some of this information, a new standardized,
Agency-wide health equity dashboard.
statewide Individual Risk Assessment tool would
• An analysis of COVID-19’s health equity
be developed by the Department of Health Care
implications.
Services (DHCS) to ensure consistent information
• Health system-wide equity reporting by the collection across managed care plans. With this
proposed Office of Health Care Affordability. information, managed care plans would assign their
• Inclusion of health equity benchmarks among members into one of four risk categories: “low risk,”
new standards and requirements that would “medium and rising risk,” “high risk,” or “unknown
be set on all managed care plans operating risk.” While plans would remain responsible for
in the state, including those that provide connecting low-risk members to preventive and
coverage through Medi-Cal and the state’s wellness services, they would be responsible for
Health Benefit Exchange (Covered California). providing increasing levels of care coordination
• Expanded Medi-Cal coverage of continuous and service linkages to their higher-risk members.
glucose monitoring for beneficiaries with Type As discussed below, for many of their highest-risk
I diabetes. members, plans would be required to provide a
• Permanent expansion of certain telehealth higher level of case management services than
services under Medi-Cal (which is intended they currently provide. Currently, at least 17 of the
to improve access to health care among state’s 24 Medi-Cal managed care plans operate
Medi-Cal beneficiaries). public health management programs generally
2 0 21-2 2 L AO B u d g e t S e r i e s 7consistent with the population health management how the target population of ECM compares to the
requirements of CalAIM. target populations of the Health Homes Program
Better Coordination of Services Through and Whole Person Care. ECM would build upon
Enhanced Care Management (ECM). CalAIM case management strategies developed in these
proposes to create a new statewide managed other programs that also were designed to focus
care benefit, ECM, to provide intensive case resources and attention on the highest-risk and
management and care coordination for Medi-Cal’s highest-need beneficiaries.
most high-risk and high-need beneficiaries Provision of Broader Array of Nonmedical
(provided they are enrolled in managed care). Supportive Services Through “in Lieu of
The intent is for ECM to provide much more Services” (ILOS). CalAIM would authorize
high-touch, community-centered care coordination managed care plans to provide an array of
services than generally are available to the nonmedical services to their members. Under
targeted populations, which include, for example, federal rules, these ILOS generally are nonmedical
high utilizers of emergency departments and services that can be provided as alternatives to
members with unstable housing. The intent is for standard Medicaid benefits in the managed care
ECM to connect high-risk, high-need members delivery system. ILOS are intended to be provided
to the appropriate services necessary for the in place of a more expensive standard Medicaid
improvement of health outcomes. Figure 6 shows benefit. If states opt in to provide ILOS (and receive
Figure 6
Comparing Target Populations:
CalAIM (Enhanced Care Management) Versus Health Homes and Whole Person Care
CalAIM (Enhanced Care Management) Health Homes Program Whole Person Care
Beneficiaries must be from one of the Beneficiaries must have a chronic condition in Pilots were allowed to choose one or more of
following categories: at least one of the following categories: the following populations:
• Children or youth with complex physical, • At least two of the following: chronic • High utilizers of avoidable emergency
behavioral, developmental, and/or oral obstructive pulmonary disease, diabetes, department, hospitals, or nursing
health needs. traumatic brain injury, chronic or congestive facilities—high utilizers.
• Individuals experiencing homelessness, heart failure, coronary artery disease, • Individuals with two or more chronic
chronic homelessness, or who are at risk of chronic liver disease, chronic renal physical conditions.
becoming homeless. (kidney) disease, dementia, substance use • Individuals with severe mental illness and/
• High utilizers with frequent hospital disorders. or substance use disorders.
admissions, short-term skilled nursing • Hypertension and one of the following: • Individuals experiencing homelessness—
facility stays, or emergency room visits. chronic obstructive pulmonary disease, homeless.
• Individuals at risk for institutionalization diabetes, coronary artery disease, chronic • Individuals at risk of homelessness.
who are eligible for long-term care or congestive heart failure.
• Individuals recently released from
services. • One of the following: major depression institutions, including jail or prison—justice
• Nursing facility residents who want to disorders, bipolar disorder, psychotic involved.
transition to the community. disorders (including schizophrenia).
• Individuals at risk for institutionalization • Asthma.
with serious mental illness, or children Beneficiaries must also meet at least one of
with serious emotional disturbances or the following acuity/complexity criteria:
substance use disorders with co-occurring
• Has at least three or more of the
chronic health conditions.
HHP-eligible chronic conditions.
• Individuals transitioning from incarceration
• At least one inpatient hospital stay in the
who have significant complex physical
past year.
or behavioral health needs requiring
immediate transition of services to the • Three or more emergency department
community. visits in the last year.
• Chronic homelessness.
CalAIM = California Advancing and Innovating Medi-Cal and HHP = Health Homes Program.
2 0 21-2 2 L AO B u d g e t S e r i e s 8federal funds in respect of them), federal law care plan demonstrates why provision of the benefit
requires that ILOS be optional for managed care for an additional time would be cost-effective
plans to provide and beneficiaries to accept. Under Figure 7 summarizes the proposed list of ILOS
CalAIM, DHCS has proposed a menu of 14 ILOS benefits in the Governor’s CalAIM proposal.
benefits that managed care plans could choose to Improved Access to Behavioral Health
provide beginning in January 2022. (Managed care Services. As was shown earlier in Figure 4, a
plans that elect to offer ILOS benefits could select higher proportion of Medi-Cal’s highest-need
which specific benefits to provide.) Some of the beneficiaries suffer from severe behavioral health
proposed ILOS benefits have restrictions on how conditions. Severe behavioral health conditions
much they can be used or who is eligible for them, also are associated with worse physical health
including benefits that are only available for use outcomes, as individuals with severe behavioral
once in a beneficiary’s lifetime unless the managed health needs often have difficulty navigating their
Figure 7
Proposed “In Lieu of Services” Benefits
Benefit Description
Services to Address Homelessness and Housing
Housing depositsa Funding for one-time services necessary to establish a household, including security deposits to obtain
a lease, first month’s coverage of utilities, or first and last month’s rent required prior to occupancy.
Housing transition navigation Assistance with obtaining housing. This may include assistance with searching for housing or
servicesa completing housing applications, as well as developing an individual housing support plan.
Housing tenancy and sustaining Assistance with maintaining stable tenancy once housing is secured. This may include interventions for
servicesa behaviors that may jeopardize housing, such as late rental payment and services, to develop financial
literacy.
Services for Long-Term Well-Being in Home-Like Settings
Asthma remediationb Physical modifications to a beneficiary’s home to mitigate environmental asthma triggers.
Day habilitation programs Programs provided to assist beneficiaries with developing skills necessary to reside in home-like
settings, often provided by peer mentor-type caregivers. These programs can include training on use
of public transportation or preparing meals.
Environmental accessibility Physical adaptations to a home to ensure the health and safety of the beneficiary. These may include
adaptations ramps and grab bars.
Meals/medically tailored meals Meals delivered to the home that are tailored to meet beneficiaries’ unique dietary needs, including
following discharge from a hospital.
Nursing facility transition/diversion to Services provided to assist beneficiaries transitioning from nursing facility care to community settings,
assisted living facilitiesc or prevent beneficiaries from being admitted to nursing facilities.
Nursing facility transition to a home Services provided to assist beneficiaries transitioning from nursing facility care to home settings in
which they are responsible for living expenses.
Personal care and homemaker Services provided to assist beneficiaries with daily living activities, such as bathing, dressing,
servicesd housecleaning, and grocery shopping.
Recuperative Services
Recuperative care (medical respite) Short-term residential care for beneficiaries who no longer require hospitalization, but still need to
recover from injury or illness.
Respite Short-term relief provided to caregivers of beneficiaries who require intermittent temporary supervision.
Short-term post-hospitalization Setting in which beneficiaries can continue receiving care for medical, psychiatric, or substance use
housinga disorder needs immediately after exiting a hospital.
Sobering centers Alternative destinations for beneficiaries who are found to be intoxicated and would otherwise be
transported to an emergency department or jail.
a Restricted to use once in a lifetime, unless managed care plan can demonstrate cost-effectiveness of providing a second time.
b New benefit introduced this year. Restricted to lifetime maximum amount of $5000, unless beneficiary’s condition changes dramatically.
c Includes residential facilities for the elderly and adult residential facilities.
d Does not include services already provided in the In-Home Supportive Services program.
2 0 21-2 2 L AO B u d g e t S e r i e s 9physical health needs. In addition, data indicate generally are intended to (1) increase capacity to
that there are differences among Medi-Cal provide Medi-Cal behavioral health services—for
populations in utilizing behavioral health services, example, by leveraging additional federal funding
which may reflect disparities in access to care. for behavioral health services (including residential
For example, Hispanic and Asian and Pacific mental health services)—and (2) increase access
Islander beneficiaries utilize Medi-Cal mental health to Medi-Cal behavioral health care—for example,
services at lower rates than other beneficiary by revising medical necessity criteria to make it
groups. CalAIM includes a package of reforms to easier for beneficiaries to receive behavioral health
Medi-Cal behavioral health service delivery, which services.
Assessment
This section provides our assessment of the could help address housing insecurity, (2) home
potential of CalAIM to reduce health disparities modifications for beneficiaries with asthma could
and thereby improve health equity. Overall, we find help address harmful environmental exposure, and
that CalAIM has significant potential to improve (3) medically tailored meals could help address
health outcomes for the highest-risk, highest-need unmet diet and nutrition requirements. Managed
Medi-Cal beneficiaries. Improved health outcomes care plans also would take on a greater role in
could lead to improved health equity insofar as addressing nonmedical needs through the new
the improved outcomes are concentrated among ECM benefit, by coordinating some nonmedical
certain groups who today disproportionately community care and human services for high
experience worse health outcomes. We find this utilizers. Figure 8 on the next page provides
likely would be the case under CalAIM, for reasons examples of how various CalAIM proposals address
that we detail below. particular determinants of health, including both
While CalAIM has potential to improve health medical and nonmedical ones.
equity, we also find that it comes with significant By Better Connecting Individuals With a
risks, challenges, and limitations. These relate to Larger Set of Medical and Nonmedical Services,
implementation issues as well as oversight and Health Outcomes Could Improve. By providing
evaluation. a wider array of services and better connecting
individuals with those services, CalAIM could
WHILE CALAIM COULD IMPROVE improve health outcomes. Specifically, the new
statewide ECM benefit would require plans to
HEALTH EQUITY… connect those individuals with higher needs to a
more comprehensive set of health care and social
CalAIM Would Increase Medi-Cal’s support services. Improving access to services
Role in Addressing the Broader affecting determinants of health could improve
Determinants of Health individuals’ outcomes. In addition, the package of
the behavioral health reforms—generally intended
CalAIM Includes Initiatives Aimed at
to increase capacity for services provided and
Addressing an Array of Medical and Nonmedical
access to care—could improve overall health
Determinants of Health. CalAIM would
outcomes given that severe behavioral health
significantly expand Medi-Cal’s role in addressing
conditions are associated with a variety of physical
nonmedical determinants of health outcomes,
health comorbidities. Additionally, ILOS benefits
primarily by encouraging managed care plans to
have the potential to improve health outcomes for
offer beneficiaries a range of nonmedical ILOS
Medi-Cal beneficiaries by providing them access
benefits. For example, (1) housing navigation
to services that address some of the underlying
services and payments for housing deposits
nonmedical determinants of their health, like
2 0 21-2 2 L AO B u d g e t S e r i e s 10Figure 8
CalAIM Proposals and Determinants of Health They Would Address
Health Determinanta Health Determinant Components Related CalAIM Proposal (Beyond ECM) b
Medical Health insurance coverage Enrollment assistance for individuals transitioning from incarceration.
(10% to 20%) Physical health care Extension of public hospital financing programs.
Behavioral health care Behavioral health reforms.
Dental health care Dental benefit expansion and incentive payments.
Social circumstances Education None.
(15% to 40%) Income None.
Housing stability Housing and long-term services and supports ILOS.
Race State oversight of population health management.
Neighborhood safety None.
Behavior Diet and nutrition Medically tailored meals for beneficiaries with unique dietary needs.
(30% to 50%) Smoking None.
Substance use Sobering centers ILOS.
Extension of Drug-Medi-Cal Organized Delivery System.
Level of physical activity None.
Environment Exposure to pollution and contaminants Asthma remediation to mitigate environmental asthma triggers.
(5% to 20%)
a Percents in parentheses reflect the portion of health disparities explained by the listed determinant. They are listed as ranges due to the differences in academic research findings on the
impacts of each determinant.
b ECM has potential to address most determinants and their components through the coordination of Medi-Cal and non-Medi-Cal benefits.
CalAIM = California Advancing and Innovating Medi-Cal; ECM = enhanced care management; and ILOS = in lieu of services.
housing. The addition of asthma remediation to the groups that disproportionately suffer poor health
list of ILOS benefits is particularly promising, as it outcomes today. The following bullets describe
would remove triggers from the home environment several of the ways CalAIM could improve health
that lead to worse health outcomes for Medi-Cal equity by narrowing disparities between different
beneficiaries with asthma. groups.
Possible Improvements in Health Outcomes
• Narrowing Disparities Between Low- and
Likely Would Be Concentrated Among
High-Income Californians. Medi-Cal
Individuals Who Currently Suffer the Worst
exclusively serves low-income individuals.
Health Outcomes. Many major CalAIM initiatives—
As Figure 2, shows, Medi-Cal beneficiaries
including those targeting the nonmedical
generally suffer worse health outcomes than
determinants of health—are aimed at improving
non-Medi-Cal beneficiaries. Therefore, if
health outcomes for Medi-Cal’s highest-risk,
CalAIM is successful in improving the health
highest-need beneficiaries. Many of the intended
of even a subset of Medi-Cal beneficiaries,
beneficiaries are homeless, have mental illness, are
the health disparities between low- and
at risk of institutionalization in nursing homes, and/
high-income state residents could narrow.
or have one or more serious chronic physical health
• Narrowing Disparities Between Those
conditions.
With and Without Stable Housing. Key
CalAIM’s Targeting of Medi-Cal’s
components of CalAIM aim to improve the
Highest-Risk, Highest-Need Beneficiaries Could
health and other outcomes for individuals
Serve to Reduce Disparities and Improve Health
experiencing or at risk of homelessness.
Equity. Any improved health outcomes that result
(Medi-Cal likely is the main source of health
from CalAIM could improve health equity insofar as
care coverage for state residents who
the improved outcomes are concentrated among
are homeless.) These include, but are not
2 0 21-2 2 L AO B u d g e t S e r i e s 11limited to, targeted enrollment of homeless CalAIM Builds on the Potential
individuals into ECM, the addition of new Promise of Existing Programs
housing services through ILOS (including
paying housing deposits and utilities), and CalAIM Consolidates and Scales up Health
medical respite for individuals who no longer Homes and Whole Person Care. As previously
need hospital-level care but do not have discussed, CalAIM would build upon existing
a safe place to convalesce. Accordingly, if programs—Whole Person Care and Health
successful, CalAIM could improve health Homes—that would end once CalAIM is launched.
outcomes for those without stable housing CalAIM does this in a number of ways. First,
and thereby narrow the disparities between by requiring managed care plans to establish
those without stable housing and those who population health management programs and
are stably housed. provide ECM on a statewide basis, CalAIM would
expand certain service components of Whole
• Narrowing Disparities Between Certain
Person Care and Health Homes to all 58 counties.
Racial or Ethnic Groups. Certain population
Second, while ILOS offerings would vary regionally
groups within Medi-Cal generally have higher
depending on which ILOS plans elect to provide,
risks and/or needs. For example, Black
overall, such services offerings are likely to
Medi-Cal beneficiaries report worse overall
expand relative to today under existing programs.
health and suffer from chronic conditions such
Third, CalAIM would consolidate Whole Person
as diabetes at higher rates than other racial or
Care and Health Homes within a single suite of
ethnic groups. Moreover, Black state residents
programs operated or arranged by managed care
as a whole experience homelessness at
plans. Because Whole Person Care and Health
highly elevated rates. Accordingly, if CalAIM
Homes target overlapping, though not identical,
is successful in improving health outcomes
populations, challenges have been reported
among Medi-Cal’s highest-risk, highest-need
by program administrators around determining
beneficiaries, these improvements likely
which program should serve which populations.
would be concentrated among individuals
By consolidating the services offered by these
from certain racial or ethnic groups, which
programs under managed care, CalAIM eliminates
could reduce disparities between such
this potential fragmentation challenge. The nearby
groups. In addition, persons of color are
text box briefly discusses how CalAIM relates to
disproportionately represented among seniors
Full-Service Partnerships.
in the Medi-Cal program compared to seniors
living in the state as a whole. Many CalAIM Evaluations of Existing Programs Reveal
reforms could improve care for Medi-Cal’s Some Promising Results. Evaluations have been
senior population, which, in turn, could carried out of Whole Person Care, Health Homes,
disproportionately benefit the state’s seniors and Full-Service Partnerships. These evaluations
of color. show significant progress has been made under
these programs in establishing the infrastructure
Comparing CalAIM and Full-Service Partnerships
The approach of California Advancing and Innovating Medi-Cal (CalAIM) is similar to that
of Full-Service Partnerships in that both provide supportive services (including housing) and
care coordination to individuals with severe mental illness. While Full-Service Partnerships
would continue in conjunction with CalAIM, the similarity between the approaches provides the
Legislature an opportunity to (1) draw lessons from these longstanding Mental Health Services
Act programs in its deliberations over CalAIM and (2) explore where coordination between CalAIM
programs and Full-Service Partnerships might improve service delivery and outcomes.
2 0 21-2 2 L AO B u d g e t S e r i e s 12needed to identify and serve high-risk, high-need assessment, the evaluations do not conclusively
beneficiaries. Infrastructure improvements include show improved outcomes.
the formation of care coordination and outreach
• Challenges Developing Population Health
teams, the execution of multiagency data-sharing
and Service Delivery Infrastructure
agreements, and the establishment of incentive
in Programs. While clear progress was
payments to improve local service delivery. In the
made under Whole Person Care and
case of Whole Person Care, these infrastructure
Health Homes in establishing cross-agency
improvements facilitated the enrollment of over
collaboration, data sharing, and program
100,000 program beneficiaries by the third year
linkages, challenges also arose. For example,
of implementation (almost half of whom were
despite the execution of a new data sharing
experiencing homelessness, a population that can
agreement under Whole Person Care, half
be hard to reach and engage in services).
of all pilots reported continued difficulties
Additionally, the evaluations of these existing
in obtaining necessary data for successful
programs provide some evidence of improvements
program implementation. Additionally, pilots
in clinical care and health outcomes. For
commonly reported a lack of available housing
example, Whole Person Care enrollees reported
and behavioral health services capacity
improvements in their overall and mental health,
constraints as impediments to improving
Health Homes participants visited emergency
enrollee outcomes.
departments at a significantly lower rate after one
• Clinical Care and Health Outcome
year of enrollment, and Full-Service Partnership
Improvements for Whole Person Care
clients utilized primary health care at higher rates
Participants Were Not Systematically
than before they joined the program. (Full-Service
Different Than Similarly Situated
Partnership clients also demonstrated lower rates
Non-Participants. We previously highlighted
of criminal justice involvement than prior to program
several clinical care and health outcome
participation.) However, as we discuss below, these
improvements that were found in evaluations
evaluations fall short of conclusively demonstrating
of existing pilot programs that CalAIM builds
improved clinical care and health outcomes as a
upon or draws inspiration from. In our
result of these programs. Final evaluations of Whole
assessment, however, these evaluations fall
Person Care and Health Homes have yet to be
short of conclusively demonstrating improved
completed, which we expect will shed additional
outcomes as a direct result of the pilot
light on the impacts of these programs.
programs. As shown in Figure 9 on the next
page, while the interim evaluation of Whole
…THE PROPOSAL FACES SEVERAL Person Care shows certain improvements in
RISKS, CHALLENGES, AND care delivery among program participants,
LIMITATIONS these improvements do not appear to differ
systematically from a comparison group of
fairly similarly situated Medi-Cal beneficiaries
Implementation Issues
not participating in Whole Person Care.
CalAIM Builds on Programs Whose Impacts This similarity could indicate that the
Are Not Fully Understood. As previously noted, improved outcomes reported for program
evaluations of existing programs that major new beneficiaries may not be due to the impacts
CalAIM initiatives would build on or otherwise draw of the programs but instead due to other
inspiration from do not conclusively demonstrate factors, such as the tendency of individuals
the effectiveness of these programs in improving experiencing acute health crises to improve
care delivery and health outcomes. The following in health following acute episodes (provided
bullets highlight several of the challenges that adequate medical care is delivered). Moreover,
existing programs have faced and why, in our differences in acute care utilization between
Whole Person Care participants prior to their
2 0 21-2 2 L AO B u d g e t S e r i e s 13Figure 9
effectiveness of different
approaches in terms of
Whole Person Care Interim Evaluation Does Not Conclusively program structure, care
Demonstrate Improved Acute Care Outcomes coordination, and population
Acute Care Utilization Per 1,000 Member Months targeting and outreach
across different participating
Emergency Department Utilization Inpatient Hospitalizations
program administrators.
180 120
Program
We understand that
Program Participants
Participants
100 evaluations of Full-Service
160 Partnerships similarly
Comparison 80 have rarely focused on
Groupa
140 Comparison Group a comparative effectiveness of
60
different approaches across
120 40 partnership participants.
Pre-WPC Pre-WPC WPC WPC Pre-WPC Pre-WPC WPC WPC
Year 1 Year 2 Year 1 Year 2 Year 1 Year 2 Year 1 Year 2
While we understand that
different approaches across
the state in implementing a
a Comparison group reflects a large sample of Medi-Cal beneficiaries with similar health and other characteristics as
program may be warranted
Whole Person Care participants but who are not enrolled in Whole Person Care.
given differences in local
Note: Pre-WPC Years reflect the two years prior to when a Whole Person Care participant enrolled in the program and a
comparable time period for the comparison group. WPC Years 1 and 2 reflect the first two years after a program environments and needs,
participant joined the program and a comparable time period for the comparison group.
we believe different
WPC = Whole Person Care.
programmatic approaches
may produce different results.
enrollment in Whole Person Care and the Evaluation of how pilot
comparison group raise questions about results compare given differences in approach
whether the two groups are similar enough could help the Legislature better determine
to compare for the purpose of judging the which models of care to expand to additional
impacts of Whole Person Care. All that said, localities.
the evaluations only cover the expiring pilot
Based on the above findings related to the
program’s earliest years of implementation.
programs CalAIM would build upon, it is difficult to
Positive impacts directly related to program
definitively expect CalAIM to achieve its intended
implementation could take longer to arise.
outcomes related to improvements in health equity.
The forthcoming evaluations should cover the
While ECM Target Populations Generally Are
impacts of the latter years of implementation
Reasonable, They May Be Overly Broad for
and, therefore, fundamentally could change
Targeting Those With Greatest Needs. Although
our understanding of the impacts of these
the administration says it intends for ECM to be
programs.
targeted at the top 1 percent of Medi-Cal utilizers,
• Comparative Effectiveness of
the proposed criteria for ECM eligibility may apply
Different Approaches Among Program
to a much larger share of the overall Medi-Cal
Administrators Not Evaluated. The
population. Some managed care plans have
Whole Person Care and Health Homes
suggested that, as currently written, the proposed
interim evaluations primarily analyze the
eligibility criteria could apply to a significant share
impacts of the pilot programs from a total
of their enrollees. However, as the administration
statewide perspective, while also highlighting
releases further information on CalAIM, it may
differences in approach among the different
continue to clarify the proposed ECM eligibility
participating program administrators. Per the
criteria such that it applies to a narrower group of
state’s evaluation instructions, however, the
current Medi-Cal enrollees.
evaluations do not focus on the comparative
2 0 21-2 2 L AO B u d g e t S e r i e s 14Medi-Cal Beneficiaries Not Enrolled in benefits. For example, constraints in the local
Managed Care Would Not Be Able to Access housing supply in certain communities could make
Certain New CalAIM Benefits. CalAIM’s most assisting members in obtaining appropriate housing
significant benefit expansions—ECM and ILOS—are a challenge for managed care plans. Notably,
proposed to be available only through managed limited housing availability has been among the
care, through which more than 11 million Medi-Cal most common challenges cited by implementers
beneficiaries receive services. Medi-Cal’s more than of the Whole Person Care pilots in addressing the
1 million beneficiaries eligible for comprehensive nonmedical determinants of health.
coverage who receive care through Medi-Cal’s Plan Discretion Makes Access to ILOS
fee-for-service delivery system would not be eligible Benefits Uncertain. Federal law requires the
for these services. Many of these beneficiaries are state to allow Medi-Cal managed care plans to
members of populations with high needs, such as choose whether—and which—ILOS benefits to
elderly and disabled individuals and foster youth, offer. If managed care plans do not widely opt
who potentially could benefit from the expanded to provide ILOS benefits, the availability of these
services and care coordination under CalAIM. new services could be more limited in scope than
As part of CalAIM, DHCS intends to develop a the state ultimately desires. Furthermore, the
specialized model of care for current and former degree to which managed care plans would elect
foster children. At this time, however, how this to offer ILOS benefits would vary from county to
new specialized model of care would allow current county. As a result, which specific ILOS benefits
and former foster children to avail themselves of would be available to a Medi-Cal beneficiary
CalAIM’s new managed care benefits is unclear. would vary based on where they live in the state
CalAIM as a Package of Reforms Only Would and what managed care plan they are enrolled
Address Certain Drivers of Health Disparities. in. In addition, plans may vary in determining
Although CalAIM would address a wide range of which beneficiaries receive ILOS benefits. These
underlying determinants of health, there are some potential inconsistencies in access to ILOS
significant nonmedical drivers of health disparities benefits could reduce CalAIM’s effectiveness in
that it does not directly address. For example, promoting health equity statewide. Therefore, while
while some ILOS benefits would address particular the proposed ILOS benefits under CalAIM have
nonmedical determinants of health—in particular, significant potential to reduce health disparities
housing insecurity—they would not directly mitigate in the Medi-Cal program, these uncertainties in
the negative consequences of other nonmedical access to ILOS benefits makes the degree to
determinants, such as unemployment or education which this would occur unclear. However, although
level. Similarly, although a healthy diet and regular ILOS benefits are proposed to be optional for
exercise are two health behaviors that have a managed care plans to provide at this time, the
significant impact on health outcomes, the ILOS administration has indicated that including these
medically tailored meals benefit is the only one with new benefits in CalAIM reflects an opportunity to
any direct relationship to these behaviors. assess the feasibility of converting some services
Constraints in Supply Could Limit proposed under ILOS into statewide mandatory
Effectiveness of Reforms. Whether the CalAIM benefits in the future. To the extent that more
package would be able to effectively reduce health plans provide these services in the future—either
disparities within Medi-Cal depends, in part, on voluntarily or as a result of a statewide mandate—
the degree to which managed care plans would be disparities in access to these services, and thus
able to take advantage of and expand community health disparities in the Medi-Cal program, could be
resources to serve the broader, nonmedical further reduced.
needs of their members. Accordingly, limits in the Strategy for Ensuring Lack of Bias in
availability of community resources could limit the Population Health Management Program
effectiveness of the CalAIM initiative, as well as Implementation Deserves Scrutiny. Under the
the time frame for realizing potential health equity CalAIM’s population health management proposal,
2 0 21-2 2 L AO B u d g e t S e r i e s 15managed care plans would use algorithms determining whether CalAIM is proving successful
to assist in identifying their highest-need, in promoting health equity would be difficult.
highest-risk enrollees (in addition to using Moreover, CalAIM may provide the state with
traditional identification means such as referrals new opportunities to track Medi-Cal beneficiary
and self-assessments). Research has shown such outcomes, the improvement of which could help set
algorithms sometimes are biased, such that they the foundation for future progress on health equity.
systematically refer fewer members of certain racial As previously discussed, under CalAIM, managed
groups for additional medical care. These biases care plans would be required to build, improve, and
could inadvertently contribute to existing health maintain significant infrastructure for the purpose
disparities. As a result, the administration has of identifying high-risk, high-need beneficiaries and
proposed that managed care plans be required to tracking their connection to services. This, in turn,
identify any potential biases in their algorithms and presents the state with an opportunity to draw
correct for them. However, the administration has on this data to better track Medi-Cal beneficiary
not yet provided guidance on how managed care outcomes and needs, as well as CalAIM’s overall
plans should identify and correct for bias in their performance in improving health outcomes and
algorithms. equity. For example, the state potentially could
track (1) rates of housing instability among
Evaluation and Oversight Issues Medi-Cal beneficiaries; (2) changes in Medi-Cal
Unclear How Progress in Improving Equity beneficiaries’ risk scores; (3) progress in linking
Would Be Measured and Evaluated. By high-risk, high-need beneficiaries to services; and
improving health outcomes for many of the state’s (4) various other beneficiary outcomes and CalAIM
highest-risk, highest-need residents, CalAIM is impacts. As yet, however, the administration has
intended to promote health equity. However, to not clearly articulated how improved managed
date, the administration has not released a detailed care plan infrastructure related to population
plan for how CalAIM would be evaluated. Without health management would translate into improved
careful and robust monitoring and evaluation, statewide performance monitoring through public
reports and dashboards.
Key Takeaways and Issues For Legislative
Consideration
CalAIM Has Potential to Improve Health significant social and policy challenges the state
Equity... As mentioned above, health disparities faces—including many challenges that have
are driven in large part by nonmedical determinants traditionally been considered beyond the scope
of health. By encouraging managed care plans to of health care policy. Due to the scale of these
provide nonmedical services, CalAIM has potential challenges, whether CalAIM can make a meaningful
to address some of the underlying causes of health impact on them is unclear. Evaluations of similar
disparities, and thereby promote health equity. programs, such as the Health Homes Program and
Additionally, CalAIM would direct more health care Whole Person Care, have yet to find any conclusive
resources toward the highest-need, highest-risk evidence that the major interventions included
beneficiaries. Targeting enrollees who systematically in CalAIM—such as ECM and ILOS—lead to
face the worst health outcomes also has the significant reductions in health disparities.
potential to improve health equity in Medi-Cal. Legislature Could Consider Which
…But Success Is Far From Certain. In Nonmedical Determinants Medi-Cal Is Most
addressing the nonmedical determinants of health, Suited to Address. While CalAIM is intended
CalAIM is intended to mitigate some of the most to address several nonmedical determinants of
2 0 21-2 2 L AO B u d g e t S e r i e s 16health, there are other nonmedical determinants sacrifice the opportunity to draw down additional
of health that it is not positioned to address. For federal funding for these services.
example, as discussed earlier, overall economic Recommend Formulating Specific Equity
well-being and educational status also are key Metrics to Ensure CalAIM Is Meeting Equity
nonmedical determinants of health that drive Goals. While CalAIM holds promise in improving
disparities in health outcomes among population health equity, its success is not certain. This
groups. To address these other sources of makes monitoring the performance of CalAIM
health disparities, the Legislature might need to critical. To do so, we recommend that the
pursue distinct policy changes that are better Legislature formulate a set of metrics related to
equipped to improve outcomes in these areas. the health equity goals of CalAIM and require
In addition, for the nonmedical determinants the administration to report on these metrics
of health that CalAIM is intended to address, periodically. In addition to including metrics related
whether Medi-Cal is the program best equipped to to care delivery and utilization, we also would
improve outcomes is unclear. For example, there encourage inclusion of metrics that more directly
are other state departments that aim to address indicate beneficiary health outcomes to the fullest
housing issues (a key nonmedical determinant extent possible. Figure 10 on the next page lists
of health that CalAIM intends to address). Given examples of health equity metrics that, should
these considerations, the Legislature may wish to systems allow, we would recommend be included
consider which nonmedical determinants of health in periodic public reports or a dashboard related
Medi-Cal is most primed to address, and consider to CalAIM. (This list is not meant to be exhaustive.)
whether additional resources should be provided Creation of a CalAIM equity reporting mechanism
to other state programs to address nonmedical or dashboard could be considered in concert with
determinants of health statewide. Importantly, the Health and Human Services Agency’s effort
without Medi-Cal playing a role, the state would to create a dashboard tracking health disparities
beyond Medi-Cal.
2 0 21-2 2 L AO B u d g e t S e r i e s 17You can also read