An Evaluation of the Advanced Illness Management (AIM) Program: Increasing Hospice Utilization in the San Francisco Bay Area
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
JOURNAL OF PALLIATIVE MEDICINE
Volume 9, Number 6, 2006
© Mary Ann Liebert, Inc.
An Evaluation of the Advanced Illness Management
(AIM) Program: Increasing Hospice Utilization
in the San Francisco Bay Area
ELIZABETH L. CIEMINS, Ph.D., M.P.H.,1 BRAD STUART, M.D.,2
ROSEMARY GERBER, R.N.,2 JEFF NEWMAN, M.D., M.P.H.,1
and MARJORIE BAUMAN, R.N., M.S.2
ABSTRACT
Background: In the Medicare population, end-of-life care is fragmented and hospice is un-
derutilized. Evidence suggests that hospice care is associated with increased patient/family
satisfaction and reductions in overall health care costs. Advanced Illness Management (AIM)
is a home-based program established to ease the transition between curative and comfort care
for seriously ill patients who lack coordinated hospital, home health, and hospice care.
Objective: Measure the impact of the AIM program on the discharge disposition of partic-
ipating home health patients.
Design: Retrospective cohort study.
Setting/subjects: A total of 435 patients who received home health services through the Sut-
ter Visiting Nurse Association and Hospice (SVNA&H) and who were discharged between
2003 and September 2005 were included in this study. Participants were selected based on a
life expectancy of 6 months or less and additionally matched on prognosis of current episode
of illness and symptom status. Intervention patients were compared to those receiving usual
home health care at two SVNA&H branches.
Results: In the within-branch comparison, a 28% difference was observed in the number of
hospice referrals between patients who received the AIM intervention and Usual Care I (47%
AIM; 33% UCI, p 0.003). When patients receiving the AIM intervention were compared to
patients from another branch, Usual Care II, a 67% difference emerged (47% AIM; 16% UCII,
p 0.0001). Among African American patients, 60% and 73% more patients were referred to
hospice when AIM patients were compared to Usual Care I and Usual Care II patients, re-
spectively (p 0.01). These differences persisted after controlling for symptom status, patient
demographics and home health length of stay.
Conclusions: The AIM program was successful at increasing hospice utilization through a
targeted intervention focused on palliative and end-of-life care, increased patient education
and decision making, and a dynamic treatment approach. The finding of increased utiliza-
tion by African Americans, a population traditionally reluctant to use hospice, was particu-
larly noteworthy.
1Sutter Health Institute for Research and Education, San Francisco, California.
2Sutter Visiting Nurse Association & Hospice, Emeryville, California.
14011402 CIEMINS ET AL.
INTRODUCTION younger decedents with cancer. However, avoid-
ing the cost of hospital-based life-saving proce-
T HE POPULATION of the United States is aging
at a rapid rate. By 2010, the U.S. Census Bu-
reau estimates a 44% increase in the population
dures is not the only issue; more importantly, in-
vasive inpatient care often causes distress, pain
and discomfort to patients and their families.17
aged 85 and older.1 This increase in longevity is Simply stated, hospice is generally a low-cost,
associated with a higher prevalence of chronic high-benefit option.
conditions characterized by unpredictable dis- Despite these advantages, hospice remains
ease trajectories and episodic needs for higher widely underutilized. In 2004, hospice provided
levels of care.2 Yet the United States health care care for 1.06 million patients through 3650 agen-
system remains focused on the treatment and cies.18 While this is a marked increase from the
management of the pathophysiological aspects of 160,000 patients served in 1985, the potential of
acute illness.3,4 The symptoms and psychological hospice care is still unfulfilled. The National Hos-
needs of an aging population have been largely pice and Palliative Care Organization has annu-
neglected. ally estimated the number of decedents who were
Evidence suggests that current end-of-life care also hospice appropriate (S. Connor, Alexandria,
is often ineffective and expensive, with insuffi- VA 2006, personal communication). Only 31% of
cient attention paid to pain management, which all patients who died and were appropriate for
is agonizing to both patients and their families.5,6 hospice in 2004 died while receiving hospice ser-
Care preferences are seldom assessed and ad- vices.18,19 In addition, patients who do enroll in
vance directives are often ignored.7,8 One study hospice rarely utilize the full 6-month benefit. In
found that nearly one quarter of patients with se- 2004, approximately one third of hospice patients
vere heart failure stated that they would have died 7 days or less after enrollment. Fewer than
preferred comfort-focused treatment, rather than 5% of hospice patients are enrolled for longer
the life-prolonging treatment they actually re- than 6 months.18 Survivors of patients referred
ceived.9 In addition, given the choice, most adults late to hospice report higher levels of unmet need
say they would prefer to die at home rather than and lower satisfaction with care.20
in an acute care setting.10 Several barriers to hospice enrollment have
been identified in the literature including those re-
lated to the health care system in general, specific
Hospice: benefits and barriers
hospice requirements, physician attitudes, lack of
One way to address the wishes of patients who awareness and cultural mistrust, and the lack of
prefer to die at home is through the increased uti- transition between curative and comfort care.
lization of Medicare’s hospice benefit, because at Barriers presented by the health care system in-
least 75% of hospice patients die at their current clude Medicare-imposed limitations on eligibility
place of residence.11 The benefits of hospice, re- for care, lack of a hospice benefit by many third-
imbursed by Medicare since 1983, include high- party payers, and a Medicare reimbursement
quality end-of-life care at home, in nursing structure that separates curative and palliative
homes, and in acute care settings. Care is pro- care while providing financial incentives for ag-
vided by an interdisciplinary team that focuses gressive treatment.
on symptom management and relief of physical, Medicare’s Conditions of Participation for hos-
emotional, and spiritual suffering. Hospice pro- pice contain rigid requirements for its providers
vides comprehensive services that allow patients that act as barriers to admission, as well as to con-
to die at their place of residence in comfort, and tinuous enrollment. Prospective hospice enrollees
provides bereavement services for the family for must sign away their right to Medicare coverage
up to 1 year after the patient’s death. for life-prolonging medical treatment. Although
Evidence suggests that hospice care results in the hospice benefit can be revoked at any time,
improved outcomes and high levels of patient this mandatory provision deters many patients
and family satisfaction.12–15 Hospice use has also and families from electing hospice treatment. Hos-
been associated with reductions in hospital ex- pice eligibility is contingent on a prognosis of 6
penditures. Campbell and colleagues16 demon- months or less, and recertification for each bene-
strated a correlation between hospice enrollment fit period requires the demonstration that the en-
and reduced Medicare expenditures among rollee is in continuous clinical decline. Any patientADVANCED ILLNESS MANAGEMENT: INCREASING HOSPICE UTILIZATION 1403
whose clinical course stabilizes must be dis- hospitalization or home health to hospice. These
charged from hospice. programs provide a blended model of care com-
Physician barriers include incorrect knowl- bining palliative with curative practices. The fo-
edge, unfavorable attitudes toward hospice, and cus of such programs is symptom management
a knowledge deficit in palliative medicine in gen- with an emphasis on earlier pain control, in-
eral. A mail survey of area physicians in East creased patient awareness of disease process and
Lansing, Michigan, found that they were uncer- treatment choices, psychosocial and spiritual sup-
tain about most questions related to hospice poli- port and a gradual shift, when appropriate, from
cies and services.21 In addition, physicians report curative toward more palliative care. The care
a need for more specific education in pain man- plan changes with the progression of illness as
agement as well as a need for improved skills in patients and families adjust their goals from dis-
communication and treatment of emotional dis- ease-modifying toward supportive care.
tress in patients and families.22,23 There is currently limited evidence supporting
Barriers specific to hospice use by ethnic mi- such programs, particularly in the community
norities have created great disparities in utiliza- setting, outside of the staff-model health mainte-
tion. Historically, hospice has been dispropor- nance organization (HMO) environment. A
tionately utilized by Caucasian patients. home-based palliative care program at Kaiser
Christakis and colleaues24 found that 92.4% of Permanente in Southern California found that the
Medicare beneficiaries enrolled in hospice were early integration of palliative care into curative
white. Hospice use among African Americans has care practices resulted in improved patient and
been reported to be 40% lower than among family satisfaction and reduced costs.31 Patients
whites, independent of income and health care participating in this program were also more
access.25 Several explanations have been posited likely to die at home than in the hospital. Another
to explain these differences including cultural program targeting nursing home patients, which
mistrust26 and lack of awareness,27,28 potentially identified residents appropriate for hospice
due to hesitation by physicians to discuss end-of- through structured interviews, increased hospice
life care with African American patients.29 These referral rates and family satisfaction while de-
cultural-specific barriers may benefit from special creasing use of acute care services.32 While this
attention to increase hospice use among histori- program was not a traditional bridge program, it
cally underutilizing population groups. demonstrated the benefits of discussing end-of-
Finally, the lack of continuous transition be- life goals and preferences with patients and their
tween curative and comfort care, combined with families.
prognostic uncertainty, have proven to be major The Advanced Illness Management (AIM) Pro-
barriers in hospice utilization. The agenda of hos- gram, a home-based palliative care program, was
pital-based providers tends to be focused on dis- designed to provide concurrent disease-modify-
ease- modifying treatment until most or all op- ing and comfort care to home health patients with
tions for “cure” have run out, at which point advanced illness in an open community-based
hospital discharge, often without referral to hos- system of care. The purpose of the present study
pice, becomes the goal.30 Patients are effectively was to evaluate the impact of the AIM program
forced to choose between comfort care and life- on discharge disposition, specifically whether the
prolonging treatment. The route from acute hos- program accomplished its goal of increasing en-
pital to home-based hospice care remains a rollment into hospice.
bumpy one. The lack of a smooth passage be-
tween these two treatment extremes prevents pa-
tients from making what should be a seamless
METHODS
transition to a dignified death.
Palliative care intervention: The AIM Program
Bridging the divide between acute care
Established as a bridge between curative and
and hospice
comfort care, the AIM Program seeks to meet the
Attempts have been made to increase the uti- needs of chronically ill patients who currently
lization of hospice services through palliative “fall between the cracks” of hospital, home health
care transition programs that create a bridge from and hospice services. The program was estab-1404 CIEMINS ET AL.
lished at the Emeryville, California, branch of Sut- • Insurance coverage.
ter Health’s Visiting Nurse Association and Hos- • Homecare and hospice regulations.
pice (SVNA&H). Sutter Health is a network of • Interface of AIM with hospice.
not-for-profit hospitals and physician organiza- • Identification of AIM patients.
tions in California that share resources and ex- • Operations, including forms, orders, desired
pertise to advance health care quality. The goal outcomes.
of the AIM Program is to eliminate the “revolv- • Advance directives and advance care plan-
ing door” of care for men and women with ad- ning.
vanced illness, replacing it with a strategic plan • Facilitating difficult conversations.
of service delivery tailored to meet the specific • Death and dying, including clinical and ethical
needs of individual patients at various stages of issues.
the illness trajectory. The AIM Program seeks (1) • SVNA&H administrative policies addressing
to provide a greater number of seriously ill pa- pain control and dying.
tients with a broad array of home-based services; • Pain and symptom management.
(2) to ease their transition from home health to
hospice; and (3) to avoid unnecessary hospital- AIM training staff included hospice and home
izations. health social workers, hospice and home health
The home-based palliative care model was de- physicians, hospice and home health nurses, and
veloped in 2002 as a direct outgrowth of the SVNA&H medical director.
CHOICES (Comprehensive Home-based Options At the conclusion of the training, trainees were
for Informed Consent about End-stage Services), given an extensive examination. Two weeks after
a nurse practitioner–based palliative care team the training, a 1-hour review session was attended
model designed to deliver palliative care within by all trainees. Finally, all trained AIM staff par-
the managed Medicare environment.33 CHOICES ticipated in biweekly patient-centered conferences,
was 1 of 22 projects in the United States funded which provided ongoing training related to end-
by The Robert Wood Johnson Foundation’s Pro- of-life issues and symptom management.
moting Excellence in End-of-Life Care initiative. AIM patients were guided through decisions
With the decline of Medicare HMOs in 2000–2001, about care options when they were ready to pro-
however, the number of covered lives served by cess the information. Unlike hospice, the AIM
SVNA&H was reduced so drastically that a new program did not require that a patient forego life-
source of funding was needed. The AIM program prolonging treatment. Instead, the value of cur-
was thus developed to work within the regula- rent treatment was discussed, and when appro-
tory structure of Medicare-certified home health priate, alternatives were considered. In addition,
care, funded by home care’s Prospective Payment AIM nurses focused specifically on education of
system and other home care payers. patient and caregivers about disease process and
The AIM Program employs a combination of prognosis, advance care planning, avoidance of
home care and hospice staff to provide home- unnecessary emergent care and hospitalization,
based palliative care to patients and families not aggressive management of pain, dyspnea and
yet ready for hospice, but eligible for home care, other symptoms, and facilitation of hospice en-
regardless of Medicare eligibility or insurance rollment. These nurses became the primary
coverage. During 2002, all Emeryville branch providers of care for the AIM patients. AIM be-
home care nurse case managers were trained in gan operating in March 2003 in western Alameda
AIM philosophy and methodology, which in- County and is currently undergoing dissemina-
cluded a focus on disease process education, tion into three other San Francisco Bay Area coun-
symptom management, goal clarification, and ad- ties served by Sutter Health. The current study
vance care and contingency planning. examines the AIM program at the Emeryville
Each case manager attended two 4-hour train- home health branch.
ing classes, which covered the following specific Referrals to AIM were initiated by hospital dis-
areas: charge planners, community physicians, the
SVNA&H intake staff, and the home care staff
• Palliative care definition and philosophy. providing care to homebound patients. All pa-
• History, description and purpose of AIM Pro- tients referred to the AIM program were home
gram. care patients and were therefore discharged fromADVANCED ILLNESS MANAGEMENT: INCREASING HOSPICE UTILIZATION 1405
the program when they were no longer eligible for hort was created to address potential treatment
home health services. The criteria for referral to bias resulting from nurses caring for both AIM
AIM began with a “no” response to the following and non-AIM patients at the Usual Care I home
key question, “Would you be surprised if this pa- health branch. Patients in all three cohorts were
tient died in 6–12 months?” as determined by the limited to those with a life expectancy of 6 months
home health nurse. This was primarily an intuitive or less.
assessment in which the patient’s age, diagnosis, Patients in the Usual Care cohorts were
and functional or nutritional decline were taken matched to the AIM cohort on selected symp-
into consideration. If the answer to this question toms, i.e., pain, dyspnea, cognitive function, con-
was “no,” then patients were referred to AIM if fusion, depression, and anxiety.
they met any two of the following criteria: They were additionally matched on current
prognosis, or their likelihood to recover from
1. Diagnosis of advanced cancer, advanced con- their current episode of illness. The majority of
gestive heart failure (CHF), end-stage pul- the patients in both Usual Care cohorts would
monary disease, end-stage hepatic disease, have been eligible for AIM based on their current
end-stage neurologic disease, other end-stage prognoses, life expectancy, and symptom status.
medical diagnosis, or advanced debility and Patients in both Usual Care cohorts received stan-
decline. dard home health services, without the pro-
2. Failing or reduced effectiveness of nonpallia- grammatic focus on palliative care, goal clarifica-
tive treatment of primary disease process. For tion, or advance care and contingency planning.
example, ineffective chemotherapy or radia-
tion for cancer; refractory fluid overload for Data source
CHF; severe or frequent exacerbations of
Home health data were gathered using the
chronic obstructive pulmonary disease
Center for Medicare and Medicaid Services
(COPD).
(CMS)’s Outcome and Assessment Information
3. Decline in functional status and/or nutritional
Set (OASIS). These measures represent core items
status in past 30 days.
of a comprehensive assessment for adult home
care patients and form the basis for evaluating
Patients who were eligible for hospice, but who patient outcomes for quality improvement pur-
refused enrollment, were also eligible for AIM as poses. The OASIS dataset is completed by a nurse
long as they met home care eligibility criteria, al- at the time of admission to home care, every 60
though the majority of AIM patients were not yet days, when resuming homecare following a hos-
eligible or ready for hospice. Once the determi- pitalization and at discharge from home care. The
nation was made that a patient was eligible for OASIS data utilized in this study included infor-
AIM, the program was described to the patient mation from the initial or “start of care” visit
and/or family. Patients who refused hospice en- as well as the discharge or “end of care” visit.
rollment could agree to participate in AIM. The OASIS items include patient sociodemographic,
majority of patients agreed to participate in AIM environmental, support system, health status,
when it was described to them as intended by the and functional status characteristics. Some attri-
program developers. Approximately 71% of re- butes of health service utilization are also included.
ferrals were made internally, from within the The reliability of these measures has been
SVNA&H system. Another 15% and 14% were re- tested by the developers of the dataset.34,35 Ad-
ferred from hospitals and physicians’ offices, re- ditional testing in the research setting demon-
spectively. strated excellent interrater reliability ( 0.75)
for urinary incontinence, pressure ulcers, anxiety,
Usual care vision and hearing, and moderate reliability (
0.40–0.75) for depressed mood, cognition, pain,
Two Usual Care cohorts were created for this
bowel incontinence, and sleep.36
study. Usual Care I comprised patients from the
same home health branch as the AIM program.
Study participants
Usual Care II patients were drawn from another
demographically similar SVNA&H home health All study participants received home health
branch without an AIM Program. The second co- services through the SVNA&H Emeryville or San1406 CIEMINS ET AL.
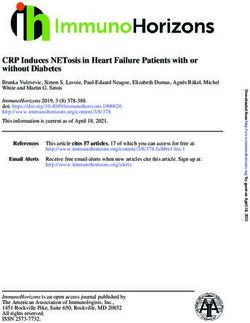
Leandro home health branches and were dis- through September 2005, 425 patients were en-
charged alive to either hospice or the community rolled in AIM at the Emeryville branch of
between January 2003 and September 2005. Dur- SVNA&H. Of these, 140 were available in the OA-
ing the study period, the Emeryville and San Le- SIS database, had a prognosis of 6 months or less
andro home health branches had an average daily at the time of discharge from home health, and
census of 490 and 216 patients, respectively. All were enrolled in the Intervention Group of the
study participants were selected based on a dis- study. During the same time period, 68 and 227
charge life expectancy of 6 months or less as patients with a similar life expectancy, current ep-
recorded in the OASIS dataset. isode of illness prognosis, and symptom status
This measure was based on the professional were enrolled into a Usual Care study group at
judgment of the clinician completing the assess- Emeryville and San Leandro home health
ment and other clinical input such as the patient’s branches, respectively. None of the participants
age, comorbidities, expected disease progression, died during the study period.
and the number of hospitalizations in past sev-
eral months. This study criterion created a subset
Statistical methods
of AIM patients, since one of the enrollment re-
quirements of AIM patients was a 6- to 12-month To measure the impact of the AIM Program on
life expectancy. The additional limitation was im- discharge disposition, i.e., hospice versus the
posed to create more similar comparison groups. community, univariate and multivariate analyses
Usual Care patients were additionally matched were conducted, utilizing a retrospective cohort
on selected symptoms and current episode of ill- design. AIM patients were compared to those re-
ness prognosis. ceiving usual care at the two home health
Figure 1 presents the study enrollment algo- branches described above on the outcome vari-
rithm. From the inception of AIM in March 2003 able of discharge disposition. Independent vari-
FIG. 1. Evaluation of advanced illness management: Enrollment of study participants.ADVANCED ILLNESS MANAGEMENT: INCREASING HOSPICE UTILIZATION 1407
ables examined in these analyses included symp- groups were comparable in terms of age with
tom status, demographic and administrative more than 80% of patients in all groups aged 65
characteristics, and home health length of stay. and older. More than half of the patients in all
The evaluation of this home health care model three cohorts were white. Approximately 60% of
was supported through funding from both the patients used Medicare fee-for-service as their
Metta Fund and Aetna. This study received ex- primary payer, followed by Medicare managed
empt certification from the Sutter Health Services care (19%), and private HMO insurance (13%).
Institutional Review Board. Table 2 describes the symptom status of the In-
tervention and Usual Care groups. The results of
univariate analysis found Usual Care patients to
RESULTS be significantly more likely to suffer from symp-
toms of confusion (p 0.01) and to have been
A sample of 140 AIM patients, 68 Usual Care given a poor prognosis for their current episode
I, and 227 Usual Care II patients was available for of illness (p 0.0001). While more than three
analysis. Table 1 provides a descriptive compar- quarters of patients in all groups experienced
ison of the three study groups. Study groups were symptoms of dyspnea and cognitive impairment,
demographically comparable on most character- the differences between groups were not signifi-
istics. Usual Care I had significantly more female cant. At the start of care, Usual Care patients in
patients than the Intervention group (p 0.04). both cohorts were significantly more likely to
Usual Care II had significantly fewer African have a life expectancy of 6 months or less (p
American and more Hispanic patients (p 0.02). 0.0001). All patients in all three cohorts had a life
Compared to the Intervention group, the pa- expectancy of 6 months or less at the time of dis-
tients in Usual Care II were more likely to be charge.
cared for by their children (p 0.02) and less Table 3 compares the discharge disposition for
likely to have paid help (p 0.04). Patients in the AIM and Usual Care patients. A 28% difference
Usual Care II group had a shorter length of stay was observed in the number of hospice referrals
than the Intervention group (p 0.01). Study between patients who received the AIM inter-
TABLE 1. DEMOGRAPHIC CHARACTERISTICS OF ADVANCED ILLNESS MANAGEMENT AND USUAL CARE PATIENTS
AIM Usual Care Ia Usual Care IIb
(n 140) (n 68) (n 227)
Age group (@SOC)
65 17.3% 16.2% 16.2%
65–75 20.5% 10.3% 17.8%
76–85 30.7% 30.9% 34.0%
85 31.5% 42.6% 32.0%
Gender
Female 58.3% 73.5%c 61.9%
Race/ethnicity
African American 26.8% 23.5% 16.2%c
Asian 5.5% 11.8% 6.5%
Hispanic 2.4% 2.9% 8.9%c
White 63.0% 57.4% 53.9%
Other 1.0% 1.5% 4.9%
Unknown 1.3% 2.9% 9.6%
Primary Caregiver
Spouse or significant other 31.5% 20.6% 29.6%
Daughter or son 26.0% 25.0% 38.5%c
Other family 6.3% 14.7% 12.6%
Paid help 18.1% 20.6% 10.5%c
Other 18.1% 19.1% 8.8%
aUsual Care I refers to the within-branch cohort at the Emeryville SVNA&H branch.
bUsual Care II refers to the external branch cohort at the San Leandro SVNA&H branch.
cDenotes p 0.05 as compared to intervention (AIM) cohort.
AIM, Advanced Illness Management; SOC, start of care; SVNA&H, Sutter Visiting Nurse Association & Hospice.1408 CIEMINS ET AL.
TABLE 2. SYMPTOM STATUS OF ADVANCED ILLNESS MANAGEMENT AND USUAL CARE PATIENTS
AIM Usual Care Ia Usual Care IIb
(n 140) (n 68) (n 227)
Shortness of breath 79.5% 76.5% 81.0%
Confusion 79.5% 86.8%c 89.5%c
Cognitive function 78.0% 86.8% 85.4%
Anxiety 51.2% 58.8% 52.6%
Poor prognosis 43.3% 95.6%c 96.8%c
Life expectancy 6 mo. SOC 59.0% 86.8%c 90.3%c
Life expectancy 6 mo. EOC 100.0% 100.0% 100.0%
Pain 60.6% 55.9% 70.0%
Depression 33.0% 33.8% 25.5%
aUsual Care I refers to the within-branch cohort at the Emeryville SVNA&H branch.
bUsual Care II refers to the external branch cohort at the San Leandro SVNA&H branch.
cDenotes p 0.05 as compared to intervention (AIM) cohort.
AIM, Advanced Illness Management; SOC, start of care; EOC, end of care; SVNA&H, Sutter Visiting Nurse Asso-
ciation & Hospice.
vention and Usual Care I (47% AIM; 33% UCI, Usual Care I revealed that the AIM intervention
p 0.003). When patients receiving the AIM in- predicted hospice discharge (p 0.003). Home
tervention were compared to Usual Care II pa- health LOS (p 0.008) and current illness prog-
tients, a 67% difference emerged (47% AIM; 16% nosis (p 0.03) were also independent predictors
UCII, p 0.0001). Among African American pa- of discharge to hospice. To further control for
tients, 60% and 73% more patients were referred home health length of stay, an additional analy-
to hospice when AIM patients were compared to sis was conducted eliminating patients with a
Usual Care I and Usual Care II patients, respec- home health length of stay falling into the lowest
tively (p 0.01). quartile in an attempt to increase the compara-
These observed differences in discharge dispo- bility of cohorts. While this step did reduce dif-
sition persisted after controlling for patient symp- ferences in home health length of stay, it did not
tom status, current episode of illness prognosis alter the study findings.
and home health length of stay. Compared to the
Usual Care II group, the AIM intervention
emerged as an independent predictor of dis- DISCUSSION
charge to hospice (p .0001) along with home
health LOS (p 0.008) and prognosis for current The AIM program was designed to address the
episode of illness (p 0.03). A comparison with needs of patients who are not yet eligible or not
TABLE 3. DISCHARGE DISPOSITION OF ADVANCED ILLNESS MANAGEMENT AND USUAL CARE PATIENTS
AIM Usual Care Ia Usual Care IIb
(n 140) (n 68) (n 227)
Discharge disposition
Hospice 47.2% 33.8%c 15.8%d
Community 53.0% 66.2% 84.2%
Race African American
Hospice 47.0% 18.8%e 12.5%f
Community 53.0% 81.2% 87.5%
aUsual Care I refers to the within-branch cohort at the Emeryville SVNA&H branch.
bUsual Care II refers to the external branch cohort at the San Leandro SVNA&H branch.
cp 0.003, controlling for race, LOS, symptom status, and prognosis.
dp 0.0001, controlling for race, LOS, symptom status, and prognosis.
ep 0.008, controlling for LOS, symptom status, and prognosis.
fp 0.0001, controlling for LOS, symptom status, and prognosis.
AIM, Advanced Illness Management; SVNA&H, Sutter Visiting Nurse Association & Hospice; LOS, length of stay.ADVANCED ILLNESS MANAGEMENT: INCREASING HOSPICE UTILIZATION 1409 ready to accept hospice. The components of the the current episode of illness, overall life ex- intervention were aimed at increasing patient un- pectancy and symptomatology. Additionally, the derstanding of his or her illness, including the validity of these and other measures found in changing array of treatment options through the OASIS has not been well tested and requires fur- trajectory of the individual’s disease. Efforts were ther study. The correlation between prognosis made to prepare patients for important end-of- and death in this database is unknown, but clin- life decision making. As a result, it was expected icians tend toward conservatism in determining that patients’ understanding of hospice, and prognoses. Evidence suggests a reluctance among therefore its utilization, would increase. The pro- physicians to bestow limited prognoses on pa- gram was successful in this respect. tients.38 Better predictors of mortality based on The addition of a second cohort was para- OASIS data are currently being explored. Finally, mount in controlling for potential contamina- data on the number of total and weekly visits tion resulting from the creation of a cohort at would also have potentially helped create better the same home health branch where the inter- matched comparison groups. vention was implemented. Indeed, the finding While the study groups appear comparable on of a greater effect among patients in the Usual many characteristics, there remain several unan- Care II cohort suggests that some degree of con- swered questions. Despite their more limited tamination did occur. This is consistent with the prognoses and more severe symptom status, pa- fact that AIM nurses cared for both AIM and tients in the Emeryville home health branch non-AIM patients at the Usual Care I home Usual Care I group were not referred to the AIM health branch. program. Without conducting clinician inter- The finding that AIM had an even greater ef- views, reasons for nonreferral cannot be deter- fect on African Americans is impressive and mined with certainty. warrants further investigation. The proportion In this observational study, we cannot reach of African American discharges from AIM to definitive conclusions regarding causality in the hospice was almost identical with that of Cau- association between the AIM program and hos- casian patients. Any program that can increase pice enrollment. Appropriateness for and inter- hospice utilization among a population histori- est in hospice may have predisposed to AIM re- cally ambivalent to participation is promising. ferral, rather than being a result of it. However, Several studies support the notion that lack of the fact that patients in both Usual Care cohorts awareness may be contributing to this observed had poorer prognoses, combined with the ab- underutilization. Rhodes and colleagues27 sence of an AIM program at the Usual Care II site, found that half of African American families helps reduce the likelihood of such a bias. A ran- surveyed were not informed about hospice, par- domized trial of the AIM intervention would pro- ticularly those with a diagnoses other than can- vide a stronger test of its effect on hospice en- cer. Another study comparing African Ameri- rollment. can with white decedents found the former to Next steps in the evaluation of the AIM pro- be 21/2 times as likely to have experienced prob- gram include an economic evaluation to deter- lems with being informed about end-of-life mine whether enrollment in AIM prevents un- care.28 This explanation is the most congruent necessary and costly hospitalizations, as would with a major component of the AIM program: be expected with increased hospice enrollment. increasing awareness and understanding of Additional service measures will be examined in- hospice. In addition, it is possible that the AIM cluding hospice length of stay as well as emer- program’s promotion of unrestricted choice in gency department care utilization. An expanded treatment modalities removed a barrier to hos- evaluation of AIM programs throughout Sutter pice enrollment that has been attributed to the VNA&H will be informative regarding the gen- perception among African Americans that re- eralizability of the results of this study, and will ferral to hospice may be associated with denial include a patient/family satisfaction component, of treatment.37 as well as an assessment of symptom manage- There are several limitations to this study. Be- ment. Additional studies of home-based pallia- cause primary diagnosis is not available for home tive care are needed to identify best practices and health patients in the OASIS database, the selec- provide guidance for the development of appro- tion of study cohorts was based on prognosis in priate reimbursement policy.
1410 CIEMINS ET AL.
REFERENCES 14. Miller SC, Weitzen S, Kinzbrunner B: Factors associ-
ated with the high prevalence of short hospice stays.
1. United States Census Bureau. 2005. www.census. J Palliat Med 2003;6:725–736.
gov/prod/www/statistical-abstract.html (Last ac- 15. Teno JM, Clarridge BR, Casey V, Welch LC, Wetle T,
cessed September 28, 2006). Shield R, Mor V: Family perspectives on end-of-life
2. Centers for Disease Control and Prevention. 2005. care at the last place of care. JAMA 2004;291:88–93.
www.cdc.gov (Last accessed September 28, 2006). 16. Campbell DE, Lynn J, Louis TA, Shugarman LR:
3. Galanos AN: Hospital-based palliative care units: an- Medicare program expenditures associated with hos-
swering a growing need. NC Med J 2004;65:217–220. pice use. Ann Intern Med 2004;140:269–277.
4. Starr JM: Toward a social phenomenology of aging: 17. Baker ME: Knowledge and attitudes of health care so-
studying the self process in biographical work. Int J cial workers regarding advance directives. Soc Work
Aging Hum Dev 1982;16:255–270. Health Care 2000;32:61–74.
5. A controlled trial to improve care for seriously ill hos- 18. NHPCO’s 2004 Facts and Figures: National Hospice
pitalized patients. The study to understand prognoses and Palliative Care Organization, 2005.
and preferences for outcomes and risks of treatments 19. Centers for Disease Control and Prevention: National
(SUPPORT). The SUPPORT Principal Investigators. Vital Statistics Reports, Births, Marriages, Divorces,
JAMA 1995;274:1591–2598. and Deaths: Provisional Data for 2004. Department of
6. Desbiens NA, Wu AW, Broste SK, Wenger NS, Con- Health and Human Services, National Center for
nors AF, Jr., Lynn J, Yasui Y, Phillips RS, Fulkerson Health Statistics, 2005.
W: Pain and satisfaction with pain control in seriously 20. Schockett ER, Teno JM, Miller SC, Stuart B: Late re-
ill hospitalized adults: findings from the SUPPORT ferral to hospice and bereaved family member per-
research investigations. For the SUPPORT investiga- ception of quality of end-of-life care. J Pain Symptom
tors. Study to Understand Prognoses and Preferences Manage 2005;30:400–407.
for Outcomes and Risks of Treatmentm. Crit Care 21. Ogle K, Mavis B, Wyatt G. Physicians and hospice
Med 1996;24:1953–1961. care: Attitudes, knowledge, and referrals. J Palliat
7. Haidet P, Hamel MB, Davis RB, Wenger N, Reding Med 2002;5:85–92.
D, Kussin PS, Connors AF Jr, Lynn J, Weeks JC, 22. Haines A, Booroff A: Terminal care at home: Per-
Phillips RS: Outcomes, preferences for resuscitation, spective from general practice. Br Med J (Clin Res Ed)
and physician-patient communication among pa- 1986;292:1051–1053.
tients with metastatic colorectal cancer. SUPPORT In- 23. Dworkind M, Shvartzman P, Adler PS, Franco ED:
vestigators. Study to Understand Prognoses and Pref- Urban family physicians and the care of cancer pa-
erences for Outcomes and Risks of Treatments. Am J tients. Can Fam Physician 1994;40:47–50.
Med 1998;105:222–229. 24. Christakis NA, Escarce JJ: Survival of Medicare pa-
8. Hofmann JC, Wenger NS, Davis RB, Teno J, Connors tients after enrollment in hospice programs. N Engl J
AF, Jr., Desbiens N, Lynn J, Phillips RS: Patient pref- Med 1996;335:172–178.
erences for communication with physicians about 25. Greiner KA, Perera S, Ahluwalia JS: Hospice usage by
end-of-life decisions. SUPPORT Investigators. Study minorities in the last year of life: Results from the Na-
to Understand Prognoses and Preference for Out- tional Mortality Followback Survey. J Am Geriatr Soc
comes and Risks of Treatment. Ann Intern Med 2003;51:970–978.
1997;127:1–12. 26. Cort MA: Cultural mistrust and use of hospice care:
9. Krumholz HM, Phillips RS, Hamel MB, Teno JM, Bel- Challenges and remedies. J Palliat Med 2004;7:63–71.
lamy P, Broste SK, Califf RM, Vidaillet H, Davis RB, 27. Rhodes RL, Teno JM, Welch LC: Access to hospice for
Muhlbaier LH, Connors AF Jr, Lynn J, Goldman L: African Americans: Are they informed about the op-
Resuscitation preferences among patients with severe tion of hospice? J Palliat Med 2006;9:268–272.
congestive heart failure: Results from the SUPPORT 28. Welch LC, Teno JM, Mor V: End-of-life care in black
project. Study to Understand Prognoses and Prefer- and white: Race matters for medical care of dying pa-
ences for Outcomes and Risks of Treatments. Circu- tients and their families. J Am Geriatr Soc 2005;53:
lation 1998;98:648–55. 1145–1153.
10. Fried TR, van Doorn C, O’Leary JR, Tinetti ME, Drick- 29. Borum M, Lynn J, Zhong Z: The effects of patient race
amer MA: Older persons’ preferences for site of ter- on outcomes in seriously ill patients in SUPPORT: An
minal care. Ann Intern Med 1999;131:109–112. overview of economic impact, medical intervention,
11. 2004 National Summary Statistics and Trends: Na- and end-of-life decisions. Study to Understand Prog-
tional Hospice and Palliative Care Organization, 2005. noses and Preferences for Outcomes and Risks of
December 28, 2005. Treatments. J Am Geriatr Soc 2000;48(5 Suppl):
12. Casarett DJ, Marenberg ME, Karlawish JH: Predictors S194–198.
of withdrawal from hospice. J Palliat Med 2001;4: 30. Kaufman SR: And a Time to Die : How American Hospi-
491–497. tals Shape the End of Life. New York, NY: Scribner, 2005.
13. Kane RL, Berstein L, Wales J, Rothenberg R: Hospice 31. Brumley RD, Enguidanos S, Cherin DA: Effectiveness
effectiveness in controlling pain. JAMA 1985;253: of a home-based palliative care program for end-of-
2683–2686. life. J Palliat Med 2003;6:715–724.ADVANCED ILLNESS MANAGEMENT: INCREASING HOSPICE UTILIZATION 1411
32. Casarett D, Karlawish J, Morales K, Crowley R, usual care for older adults receiving an acute episode
Mirsch T, Asch DA: Improving the use of hospice ser- of home care. JAMA 2002;287:2098–2105.
vices in nursing homes: A randomized controlled 37. Crawley LM, Marshall PA, Lo B, Koenig BA: Strate-
trial. JAMA 2005;294:211–217. gies for culturally effective end-of-life care. Ann In-
33. Stuart B, D’Onofrio C, Boatman S, Feigelman G: tern Med 2002;136:673–679.
CHOICES: Promoting early access to end-of-life care 38. Christakis NA, Lamont EB: Extent and determinants
through home-based transition management. J Palliat of error in doctors’ prognoses in terminally ill pa-
Med 2003;6:671–683. tients: Prospective cohort study. BMJ 2000;320:469–
34. Hittle DF, Shaughnessy PW, Crisler KS, Powell MC, 472.
Richard AA, Conway KS, Stearns PM, Engle K: A
study of reliability and burden of home health as- Address reprint requests to:
sessment using OASIS. Home Health Care Serv Q Elizabeth Ciemins, Ph.D.
2003;22:43–63.
Sutter Health Institute for Research and Education
35. Crisler KS, Baillie LL, Richard AA: Integrating OASIS
data collection into a comprehensive assessment.
345 California Street, Suite 2000
Home Healthc Nurse 2000;18:249–54. San Francisco, CA 94611
36. Tinetti ME, Baker D, Gallo WT, Nanda A, Charpen-
tier P, O’Leary J: Evaluation of restorative care vs E-mail: CieminE@sutterhealth.orgYou can also read