CRP Induces NETosis in Heart Failure Patients with or without Diabetes
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CRP Induces NETosis in Heart Failure Patients with or
without Diabetes
Branka Vulesevic, Simon S. Lavoie, Paul-Eduard Neagoe, Elizabeth Dumas, Agnès Räkel, Michel
White and Martin G. Sirois
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
ImmunoHorizons 2019, 3 (8) 378-388
doi: https://doi.org/10.4049/immunohorizons.1900026
http://www.immunohorizons.org/content/3/8/378
This information is current as of April 18, 2021.
References This article cites 57 articles, 17 of which you can access for free at:
http://www.immunohorizons.org/content/3/8/378.full#ref-list-1
Email Alerts Receive free email-alerts when new articles cite this article. Sign up at:
http://www.immunohorizons.org/alerts
ImmunoHorizons is an open access journal published by
The American Association of Immunologists, Inc.,
1451 Rockville Pike, Suite 650, Rockville, MD 20852
All rights reserved.
ISSN 2573-7732.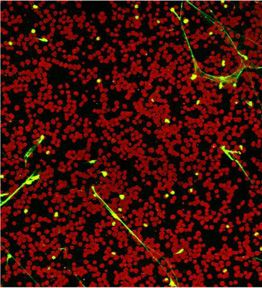
RESEARCH ARTICLE
Innate Immunity
CRP Induces NETosis in Heart Failure Patients with or
without Diabetes
Branka Vulesevic,*,† Simon S. Lavoie,*,† Paul-Eduard Neagoe,* Elizabeth Dumas,*,† Agnès Räkel,‡,§ Michel White,*,‡
and Martin G. Sirois*,†
*Centre de Recherche, Institut de Cardiologie de Montréal, Faculté de Médecine, Université de Montréal, Montreal, Quebec H1T 1C8, Canada;
†
Département de Pharmacologie et Physiologie, Faculté de Médecine, Université de Montréal, Montreal, Quebec H3C 3J7, Canada; ‡Département
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
de Médecine, Faculté de Médecine, Université de Montréal, Montreal, Quebec 3T 1J4, Canada; and §Centre de Recherche du Centre Hospitalier
Universitaire de Montréal, Faculté de Médecine, Université de Montréal, Montreal, Quebec H2X 0A9, Canada
ABSTRACT
C-reactive protein (CRP) is recognized as a biomarker of chronic, low-grade inflammation associated with vascular disorders. Lately,
the role of neutrophils and neutrophil extracellular traps (NETs) has been investigated as a potential source of chronic inflammation
and cardiovascular complications. This study investigated NETs as a marker of inflammation in patients with symptomatic heart
failure (HF) with or without type 2 diabetes (T2DM) and examined the correlation between NETs and CRP. We performed a
noninterventional study including patients with HF with or without T2DM, T2DM, and a healthy control (HC) group. NETs and other
inflammatory markers in serum were measured by ELISA. The release of NETs (NETosis) in vitro under various stimuli was measured
by confocal microscopy. The levels of NETs in the serum of HF patients were significantly higher compared with HC (112%). Serum
CRP concentrations were significantly increased in HF and HF plus T2DM patients compared with HC, and a positive correlation was
observed between serum CRP and NETs levels. Neutrophils from HF and HF plus T2DM patients underwent in vitro NETs release
faster than T2DM and HC without any stimuli. In vitro, serum collected from the HF and the HF plus T2DM group induced NETosis in
healthy neutrophils significantly more when compared with HC and T2DM, which was prevented by depletion from CRP. We
confirmed in vitro that CRP induces a concentration-dependent NETs synthesis. This study proposes a mechanism by which CRP
increases the risk of future cardiovascular events and supports mounting evidences on the role of neutrophils in chronic low-grade
inflammation associated with HF. ImmunoHorizons, 2019, 3: 378–388.
INTRODUCTION as during exercise. In healthy men and women, the left
ventricular ejection fraction (LVEF) ranges from 52 to 74%.
Heart failure (HF) is defined as a chronic and progressive Phenotypically, HF can be present with a reduced LVEF
condition in which the heart is unable to meet the requirements (HFrEF) #40%, whereas patients with symptoms and signs of
of metabolizing tissues in a situation of increased demand, such HF with LVEF $50% are classified as HF with a preserved LVEF
Received for publication March 27, 2019. Accepted for publication July 23, 2019.
Address correspondence and reprint requests to: Prof. Martin G. Sirois, Montreal Heart Institute, 5000 Belanger Street, Montreal, QC H1T 1C8, Canada. E-mail
address: martin.sirois@icm-mhi.org
ORCIDs: 0000-0002-3660-5410 (B.V.); 0000-0001-5594-121X (S.S.L.); 0000-0002-7945-1343 (M.W.).
This work was supported by grants from the Canadian Institutes of Health Research (MOP-97943 to M.G.S.), Fonds de Recherche du Québec - Santé (FRQS) - Research
Network on Cardiometabolic Health, Diabetes and Obesity (to M.W., A.R., and M.G.S.), and Fondation de l’Institut de Cardiologie de Montréal (FICM) (to M.G.S.). B.V. and
E.D. were recipients of a fellowship and doctoral studentship, respectively, from FRQS, and S.S.L. was a recipient of an FICM studentship. M.W. is the recipient of the
Carolyn and Richard Renaud Endowed Research Chair in Heart Failure of the Montreal Heart Institute.
Abbreviations used in this article: CRP, C-reactive protein; HC, healthy control; HF, heart failure; HFpEF, HF with a preserved LVEF; HFrEF, HF with a reduced LVEF;
hsCRP, high-sensitivity CRP; LDL, low-density lipoprotein; LVEF, left ventricular ejection fraction; MHI, Montreal Heart Institute; MPO, myeloperoxidase; NET, neutrophil
extracellular trap; NYHA, New York Heart Association; pEF, preserved ejection fraction; rEF, reduced ejection fraction; rhCRP, recombinant human CRP; T2DM, type 2
diabetes.
This article is distributed under the terms of the CC BY-NC-ND 4.0 Unported license.
Copyright © 2019 The Authors
378 https://doi.org/10.4049/immunohorizons.1900026
ImmunoHorizons is published by The American Association of Immunologists, Inc.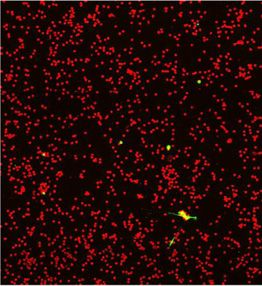
ImmunoHorizons CRP INDUCES NETosis IN HEART FAILURE PATIENTS 379
(HFpEF). More recently, the European Society of Cardiology has MATERIALS AND METHODS
proposed new guidelines for the inclusion of a third type of HF
with LVEF between 41 and 49%, named HF with midrange Population
ejection fraction (1, 2). Chronic, low-grade inflammation is one This was a prospective nonrandomized, noninterventional study
of the major factors impacting the development and progres- that included HF patients with reduced ejection fraction (rEF) or
sion of HF (3). It also contributes to an increase in a broad range preserved ejection fraction (pEF) with or without T2DM and
of inflammatory cytokines and biomarkers in both HFrEF and patients diagnosed with T2DM but without any heart pathologic
HFpEF (4). Moreover, coexistence of HF with other proin- condition. Nineteen patients with HF and 26 patients with HF plus
flammatory conditions, such as type 2 diabetes (T2DM) has been T2DM were recruited at the Montreal Heart Institute (MHI).
associated with an increase of adverse outcomes and mortality Twenty-one T2DM patients with no symptoms or signs of HF
(5), both in acute and chronic HFrEF and HFpEF (6). Despite were recruited from the Clinique d’Endocrinologie de Montréal.
numerous differences in the pathophysiology and the clinical The blood collection from all patients (66) and healthy controls
features of these two forms of HF, with or without T2DM, (HC; n = 25) was performed at the MHI. This study was approved
significant relationships between selected inflammatory markers by the Scientific Research Committee and the Ethics Committee of
and adverse cardiovascular outcomes have been reported (7). the MHI (ethics No. ICM #01-406 and No. ICM #12-1374) and
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
One of these inflammatory markers and predictors of future conform to the principles outlined in the Declaration of Helsinki.
cardiovascular events, C-reactive protein (CRP), produced in liver, Donors were informed about the procedures and signed a written-
has been used as a common indicator of both acute infection and informed consent before participating in the study.
subclinical inflammation (3). CRP is increased in patients with
chronic stable HF (8), but the mechanisms connecting CRP and Selection criteria of healthy volunteers and patients
the severity of HF remain unknown. Lately, multiple studies are HC volunteers recruited in this study were enrolled assuming they
reporting a correlation between CRP and neutrophil counts (9) were not having any significant medical conditions and were not
and an association between increased neutrophil counts and on any anti-inflammatory medication for at least 14 d before blood
higher prevalence of coronary disease (10), suggesting possible collection. All patients with T2DM alone had an HbA1c ,10% and
connections between CRP, neutrophils, and progression of undiagnosed for HF conditions. These T2DM patients were
cardiovascular disorders. Furthermore, mounting evidence is controlled by any available hypoglycemic medications and, as per
reporting novel mechanisms by which neutrophils can promote guidelines, were treated with preventive hypertension medication.
proinflammatory activities through the generation and release The characterization and recruitment of HF patients was in
of neutrophil extracellular traps (NETs), termed NETosis (11). concordance with the guidelines set in the Treatment of Preserved
NETosis occurs primarily through a cell death process, fol- Cardiac Function Heart Failure with an Aldosterone Antagonist
lowing a nuclear envelope disassembly and nuclear chromatin clinical trial (24), which was prior to the setting of the new
decondensation into the cytoplasm of intact cells, mixing with European Society for Cardiology guidelines (1). Therefore, HF
cytoplasmic and granule components (12). Under physiological patients recruited from the MHI Heart Failure Clinic were
conditions, this process takes 3–8 hours after neutrophil classified as HFrEF if their LVEF was #40% or HFpEF if their
activation (12). However, it has been reported that neutrophils LVEF was $45% (24–26), as documented by contrast ventricu-
from patients suffering from acute or low-inflammatory lography, magnetic resonance imaging, radionuclide ventriculog-
pathologic conditions are primed to release NETs; thus, a rapid raphy, or quantitative echocardiography within the previous 12 mo
release of NETs can be observed within minutes under various if no cardiac event occurred since the measurement of their LVEF
conditions (13–18). NETs are composed of dsDNA decorated (24). In addition to the previous inclusion criteria for the HF
with cytosolic and granule-derived proinflammatory cytokines patients, the HF plus T2DM patients had also an HbA1c ,10% and
and enzymes (19); their composition depends on the state of were controlled by any available hypoglycemic medications and,
neutrophil activation and possible conditions that affect them as per guidelines, were treated with preventive hypertension
(e.g., systemic lupus erythematosus, rheumatoid arthritis, cystic medication. HF patients had a New York Heart Association
fibrosis, and conditions associated with metabolic disorders) (NYHA) functional class II or III and, unless contraindicated,
(17). One of the unchangeable and obligatory protein compo- were treated with an angiotensin-converting enzyme inhibitor
nents of NETs is myeloperoxidase (MPO) (20). In vasculature, or with angiotensin II receptor blockers and stable doses of
besides their original role as a bacterial traps, NETs can contribute b-blockers for at least 30 d. Patients with severe chronic
to thrombi formation and vulnerable plaque destabilization (21). pulmonary disease, chronic active inflammatory disease, severe
Previous studies reported a correlation between CRP and NETs renal failure (creatinine .250 mmol/l), liver dysfunction (trans-
production under hemodialysis (22), rheumatoid arthritis, or sepsis aminases $3-fold upper normal values), and ongoing cancer
conditions (17, 23). However, there are as yet no studies reporting malignancy were not eligible for the study. HF patients with or
the relationship between CRP and NETs release in HF patients. without T2DM, T2DM patients, and HC having ongoing and/or
Thus, our objectives were to characterize the changes in NETs in recent infection (within 2 wk prior to the study, as this would
patients with HF with or without T2DM and to assess whether affect neutrophil counts) or had CRP values higher than 15 mg/l
there is a link between CRP level and NETs in these patients. (suggesting potential acute unrelated inflammatory state) were
https://doi.org/10.4049/immunohorizons.1900026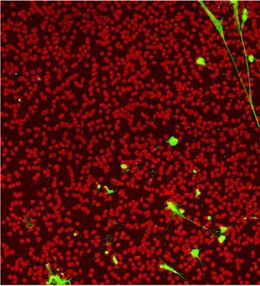
380 CRP INDUCES NETosis IN HEART FAILURE PATIENTS ImmunoHorizons
excluded from this study. Other exclusion factors were as follows: NETs and biomarkers quantification
recent myocardial infarction, recent stroke, HF functional NYHA As NETs are defined as chromatin bound to MPO, for their
class IV, unstable clinical condition, and recent open-heart surgery. detection in serum, an ELISA method that detects exclusively
MPO-bound DNA complexes in serum samples was used, and
Study protocol: serum and neutrophil collection results were analyzed by comparison of OD values between
Venous blood samples (20 ml) were obtained from HC, T2DM groups, as previously described (28). The biomarkers IL-6
patients, and HF patients with or without T2DM in Vacutainer and MPO were quantified by ELISA kits (Bio-Techne, Minneapolis,
serum separation tubes. Upon centrifugation (1000 3 g for 15 min) MN). High-sensitivity CRP (hsCRP) in serum samples was
at least 3 ml of serum was collected, aliquoted, and frozen at quantified by nephelometry at the biochemistry laboratory
280°C. Another 25 ml sample of venous blood was mixed with at the MHI.
Anticoagulant Citrate Dextrose Solution USP Formula A (MP
Biomedicals, Solon, OH). Neutrophils were isolated and resus- NETs quantification by confocal microscopy
pended in RPMI medium supplemented with 25 mM HEPES and Neutrophils (1 3 106 cells per ml) in RPMI medium were
1% penicillin/streptomycin, as described previously (27). Contam- incubated at 37°C, 5% CO2 for 15 or 60 min with different agonists:
ination with PBMCs was ,0.1% as determined by morphological PBS and Tris (control buffer solutions), homopentamer re-
analysis and flow cytometry (data not shown), and viability
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
combinant human CRP (rhCRP; 1, 5, and 10 mg/l) (R&D Systems,
was .98% (trypan blue dye exclusion) (27). Pure neutrophil Minneapolis, MN), IL-8 (25 nM, positive control) (PeproTech,
population was used for all in vitro studies. Rocky Hill, NJ), blood serum collected from volunteers (HC,
TABLE I. Baseline patient characteristics
Control Group (n = 25) T2DM Group (n = 21) HF Group (n = 19) HF with T2DM Group (n = 26) p Value
Age (y) 58.4 6 1.6 62.0 6 1.0 66.4 6 1.1 67.8 6 1.2 p # 0.03
Males n (%) 18 (72) 19 (90.5) 12 (63.2) 19 (73.1) NS
NYHA classification n (%)
Class II - - 15 (78.9) 19 (73.1)
Class III - - 4 (21.1) 7 (26.9)
LVEF n (%) - - 30.4 6 3 36.8 6 2.5
rEF n (%) - - 15 (78.9) 19 (73.1)
pEF n (%) - - 4 (21.1) 7 (26.9)
Ischemic HF n (%) - - 9 (47.4) 15 (57.7)
Nonischemic HF n (%) 10 (52.6) 11 (42.3)
Cardiomyopathy n (%) - - 3 (15.8) 1 (3.9)
Valvular n (%) - - 3 (15.8) 3 (11.6)
Others n (%) - - 4 (21.1) 7 (26.9)
Medical conditions n (%)
Hypertension - 8 (38.1) 15 (78.9) 10 (38.5) p = 0.006
Dyslipidemia - 9 (43.0) 15 (78.9) 19 (73.1)
Stroke - 0 (0) 5 (26.4) 9 (34.6)
Chronic kidney disease - 3 (14.3) 5 (26.4) 10 (38.5)
Treatment n (%)
ACEi - 8 (38.1) 3 (15.8) 9 (34.6)
ARBs - 5 (23.8) 12 (63.2) 13 (50)
b-blockers - 4 (19.1) 18 (94.7) 26 (100)
Diuretic agent - 2 (9.5) 16 (84.2) 26 (100)
Statin 6 (24) 17 (81) 16 (84.2) 21 (80.8)
Anticoagulant 1 (4) 0 (0) 8 (42.1) 15 (57.7)
Sulfonylureas - 5 (23.8) - 7 (26.9)
DPP-4 inhibitor - 9 (42.9) 8 (42.1) 12 (46.2)
a-Glucosidase inhibitors - 1 (4.8) 4 (21.1) 8 (30.8)
Agonists GLP-1 - 3 (14.3) - -
SGLT2 inhibitor - 5 (23.8) - -
Metformin - 18 (85.7) - 5 (19.2)
Insulin - 7 (33.3) - 4 (15.4)
Creatinine (mmol/l) 78.5 79.4 126.4 125.8 p , 0.001
Glucose (mmol/l) 5.25 8.60 6.64 9.40 p , 0.001
Cholesterol (mmol/l) 4.97 3.52 3.63 3.10 NS
Triglyceride (mmol/l) 1.79 1.57 1.56 1.93 NS
LDL (mmol/l) 3.10 1.75 201 1.54 NS
Values are mean 6 SE or percentage.
ACEi, angiotensin-converting enzyme; ARBs, angiotensin receptor blocker; DPP-4 inhibitor, dipeptidyl peptidase-4 inhibitor; GLP-1, glucagon-like peptide 1; SGLT2,
sodium/glucose cotransporter 2.
https://doi.org/10.4049/immunohorizons.1900026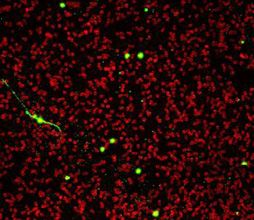
ImmunoHorizons CRP INDUCES NETosis IN HEART FAILURE PATIENTS 381
CRP-depleted serum and NETs induction
Serum CRP depletion was performed by using agarose-coated
beads with immobilized phosphorylcholine with specific affinity
for CRP (Life Technologies) (29). As negative control, serum
aliquots were treated with noncoated agarose beads. As per
protocol, after 30 min of incubation, the beads were centrifuged and
hsCRP content in the depleted serum was analyzed by nephelom-
etry at the biochemistry laboratory at the MHI. Incubation with
phosphorylcholine-coated beads produced serum depleted of
CRP (values ,0.16 mg/l), whereas agarose beads had no effect on
CRP values.
Statistical analysis
Any differences in variables between HC, T2DM patients, and
the HF with or without T2DM population were evaluated using a
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
one-way ANOVA followed by a Dunnett post hoc test. The rela-
tions between variables were assessed by using Pearson regression
analyses. Differences between groups for in vitro studies were
compared using a one-way ANOVA or a paired Student t test (for
neutrophil response to CRP and CRP-depleted serum). Statistical
significance was set at p , 0.05. All analyses were performed using
SPSS for Windows.
RESULTS
Patient characteristics
Ninety-one volunteers were enrolled in this study. A total of
45 patients with HF NYHA functional class II to III were studied;
34 (75.6%) of them were having rEF with or without T2DM. Baseline
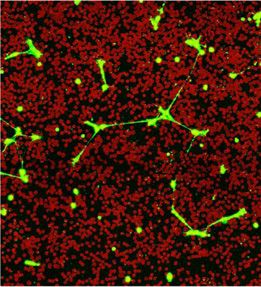
FIGURE 1. NETs release by neutrophils. demographics and clinical characteristics are summarized in
Neutrophils from patients with T2DM and HF with T2DM are precondi- Table I. The group of patients with HF with or without T2DM
tioned to produce NETs as compared with neutrophils from HC. Rep- was significantly older than the HC group. However, we
resentative pictures of NETs release at 60 min from the following groups: performed a Pearson correlation analysis that showed no
(a) HC, (b) T2DM, (c) HF and (d) HF with T2DM neutrophils. Neutrophils correlation between NETs concentration in serum and aging
are labeled with wheat germ agglutinin (conjugated with Alexa 647; red) (p = 0.196) in this population.
and NETs are labeled with SYTOX Green (green). Neutrophils collected
from all three patient groups showed increased tendency for NETs re-
lease at 15 and 60 min. Data shown as mean 6 SEM (n = 6–7 for each
In vitro release of NETs from unstimulated neutrophils
group, including HC). *p # 0.04 (e).
We performed a time-dependent study to assess the optimal time
needed for the release of NETs from patients with T2DM, HF, and
HF with T2DM as compared with HC. In that study, we were able
T2DM patients, HF patients, and HF patients with T2DM) and to test whether low-grade inflammation present in patients with
CRP-depleted serums from HF patients and HF patients with T2DM and/or HF prompts neutrophils to undergo NETosis. In
T2DM. Green-fluorescent nuclear and chromosome counter- our study, we observed by confocal microscopy that neutrophils
stain that is nonpermeable to live cells (SYTOX Green, 1 mM; from patients with T2DM, HF, and HF with T2DM were already
Life Technologies, Burlington, ON, Canada) was then added to capable of promoting a significant release of NETs as compared
detect dsDNA NETs released by neutrophils. Images were with HC within 15–60 min postisolation (representative images
obtained by confocal microscopy (LSM 710; Carl Zeiss, Toronto, in Fig. 1a–d). Neutrophils isolated from all three patient groups
ON, Canada) and set to acquire a mosaic of pictures (5 3 5 (T2DM, HF, and HF with T2DM) under basal condition increased
images) (Zen 2; Carl Zeiss) (magnification, 2003). To calculate NETs synthesis within 15 min by 5.5-, 6.2-, and 7.4-fold, respectively,
the percentage of total area of image covered by NETs, an as compared with HC (Fig. 1e for HF and HF with T2DM, p # 0.04).
algorithm in Image-Pro Plus 7 (Media Cybernetics, Rockville, After 60 min, NETosis was increased by 2.2-, 3.6-, and 4.1-fold in
MD) was used, and a threshold to exclude low-fluorescence patients with T2DM, HF, and HF with T2DM, respectively (Fig. 1e
background was applied (27). for HF and HF with T2DM, p # 0.02).
https://doi.org/10.4049/immunohorizons.1900026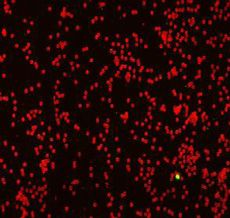
382 CRP INDUCES NETosis IN HEART FAILURE PATIENTS ImmunoHorizons
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
FIGURE 2. Measures of inflammatory markers in the serum.
Serum from all three patient groups was analyzed by ELISA for the presence of NETs, MPO, and IL-6 and by nephelometry for hsCRP. (a) NETs from HF
patients were increased compared with HC, *p = 0.015. (b) The concentration of MPO in the HF and HF with T2DM serum was increased compared with
HC, *p # 0.012, whereas (c) IL-6 and (d) CRP concentrations in all three groups were increased when compared with HC, *p # 0.025; (n = 25 for HC,
n = 21 for T2DM, n = 19 for HF, and n = 26 for HF with T2DM for NETs and CRP; n = 14–18 in each group for MPO and n = 8–11 in each group for IL-6).
NETs and biomarkers of inflammation in serum prompted us to differently regroup the collected data on NETs in
The levels of NETs in serum from HF patients were significantly serum. By grouping the patients and HC based on their serum CRP
higher than in HC (2.12-fold, p = 0.011), whereas patients with levels into three different categories (e.g., ,1, 1–3, and .3 mg/l),
T2DM and HF with T2DM had 1.61- and 1.58-fold increase we found a new perspective of the CRP–NETs correlation. The
compared with HC (Fig. 2a, p = 0.16). Our data showed a significant group with CRP levels between 1 and 3 mg/l had a significant
increase of MPO levels (both chromatin bound and free) in both increase in NETs content (Fig. 4, Table II, p = 0.011). The increase
HF patients and patients with HF with T2DM groups (Fig. 2b, in IL-6 was significant (p = 0.034), whereas the ST2 increase was
p # 0.011) but not in T2DM patients, compared with HC (p = 0.14). noticeable but NS (Table II, p = 0.39), and there was no significant
All three patient groups had a significant increase of IL-6, whereas rise in total MPO (Table II). The group with a CRP concentration
IL-6 (except for one healthy volunteer) was below the minimum .3 mg/l, besides having an increase in NETs serum level (Fig. 4,
detectable concentration in the HC group (Fig. 2c, p # 0.026). CRP p = 0.015), had an increase in all analyzed inflammatory markers
levels of all three patient groups were also significantly increased (Table II, IL-6 and MPO, p , 0.001 and p = 0.034, respectively)
(Fig. 2d, p # 0.039 compared with HC). more comorbidities (e.g., previous occurrence of stroke, renal
disease, pulmonary hypertension, and previous history of gout),
Correlations between NETs and inflammatory biomarkers higher fasting glucose and low-density lipoprotein (LDL),
The presence of NETs in serum positively correlated with CRP and higher levels of ST2, a protein biomarker of cardiac stress
(Fig. 3a, p = 0.033) and MPO levels (Fig. 3b, p = 0.003). IL-6 (Fig. 3c, (Table II).
p = 0.234) and NETs had no correlation, but IL-6 was positively
correlated with CRP (Fig. 3d, p = 0.039). Serum-mediated NETs release
Neutrophils from HC were exposed to PBS (basal control) and four
Elevated CRP concentration increases NETs content in serum types of serum (HC, T2DM, HF and HF with T2DM) for 60 min
Examining the results of NETs content in the serum and the and observed by confocal microscopy (representative images Fig.
correlation between CRP and NETs in all three patient groups 5a–e). Serum from HF and HF with T2DM patients significantly
https://doi.org/10.4049/immunohorizons.1900026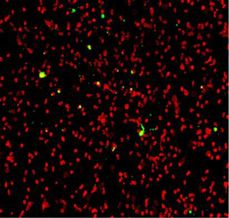
ImmunoHorizons CRP INDUCES NETosis IN HEART FAILURE PATIENTS 383
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
FIGURE 3. Correlation between proinflammatory cytokines and NETs in serum.
A significant positive correlation (Pearson regression) was found between NETs and CRP (a), NETs and MPO (b), CRP and IL-6 (d), and no correlation
was found between NETs and IL-6 (c).
augmented NETosis by 3.68- and 4.58-fold, respectively (Fig. 5f, NETosis was increased by 2.5-fold, and a treatment with 10 mg/l
p # 0.03). The serums of HC and T2DM patients increased (but significantly increased NETosis up to 3.5-fold (Fig. 6b, p # 0.025).
nonsignificantly) the release of NETs by 1.95- (p = 0.33) and 2.88- In addition, we observed that rhCRP (10 mg/l) was as potent as
fold (p = 0.06), respectively (Fig. 5f ). IL-8 (25 nM), a known inducer of NETosis (30) (Fig. 6b). Together,
our results are summarized in an illustration showing how HF and
CRP in serum stimulates NETs release diabetes are leading to NETs formation (Fig. 7).
Using the serum from HF and HF with T2DM patients with CRP
values of 4 6 1 mg/l, we tested if the CRP found in the serum is a
possible inducer of NETosis. The same serum sample but CRP DISCUSSION
depleted (,0.16 mg/l minimal detectable value) was used at the
same time and on the same HC neutrophils to induce NETosis In the current study we observed that patients with HF and/or
(Fig. 6a). Serum containing more than 4 mg/l of CRP significantly T2DM who have higher CRP levels in their serum also have higher
increased NETosis, (Fig. 6a, p # 0.04), whereas CRP-depleted NETs concentration, and their neutrophils are primed to
serum had no effect. synthesize NETs in vitro even in absence of stimulation. We also
observed that a treatment with the serums from these patients is
CRP stimulates NETs release capable of promoting NETosis in HC neutrophils, and this latter
To demonstrate that CRP has a direct capacity to induce NETs effect was lost when the serums were depleted from CRP. Finally,
release, neutrophils from HC were treated for 60 min with rhCRP we also experimentally confirmed the in vitro capacity of rhCRP to
(1, 5, and 10 mg/l), which is comparable to the range of CRP promote NETosis. Our study provides, to our knowledge, the first
concentrations observed in donors’ blood (HC and patients). evidence that CRP is a direct inducer of NETosis and that elevated
rhCRP induced NETosis in a concentration-dependent manner. At serum concentration of CRP participates in NETs formation.
the lowest rhCRP concentration (1 mg/l), as observed in healthy It has been demonstrated that neutrophils are not just
individuals, NETosis was increased by 1.5-fold, whereas at 5 mg/l, first responders to acute infections but also active contributors
https://doi.org/10.4049/immunohorizons.1900026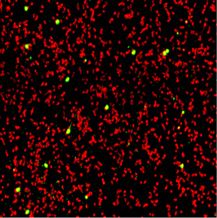
384 CRP INDUCES NETosis IN HEART FAILURE PATIENTS ImmunoHorizons
T2DM cohort in two distinct groups (,3 antidiabetes drugs or
$3 antidiabetes drugs), they did observe a significant increase of
circulating NETs in the serum of patients taking $3 antidiabetes
drugs. In another study, it has also been reported that circulating
NETs concentration is significantly increased in newly diagnosed/
uncontrolled diabetic patients that returned to nonsignificant
increase within 12 mo posttreatment on metformin (39). In our
study, we observed a trend but nonsignificant increase of circulat-
ing NETs in a cohort of well-controlled T2DM patients. Together,
these data suggest that, depending on the glycemic status, medica-
tion, and treatment duration since T2DM diagnosis (37–39), the
increase of circulating NETs can fluctuate from significant to
nonsignificant.
To our knowledge, our study is the first one to report a
significant increase of NETs levels in the serum of HF patients. As
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
FIGURE 4. Relationship between the levels of NETs and CRP in serum. T2DM is a common comorbidity factor in HF patients with a
The concentration of NETs in serum is increased in patients with CRP significant negative impact of prognosis (40), as well as higher
levels .1 mg/l as compared with low CRP levels (,1 mg/l) (n = 25 in mortality rates among patients with HF with T2DM compared
the CRP ,1 mg/l, n = 35 in the CRP = 1–3 mg/l, and n = 31 in the with HF alone (41), we assessed the comorbidity effect of T2DM on
CRP .3 mg/l groups, respectively). *p # 0.015. the release of NETs in HF patients. Although, we did not observe
an increase of NETs levels in the serum of HF with T2DM patients
to low-grade chronic inflammation (31), which can be explained, as compared with HF alone, we did observe an increasing trend on
in part, by their capacity to release NETs (32). Despite growing the release of NETs from the isolated neutrophils of HF with
evidences that various pathological conditions prime neutro- T2DM patients as compared with HF alone. CRP is one of the early
phils for NETosis (17), the prognostic value of NETs release in markers of inflammation, and it is used to predict the likelihood
serum is still debatable (33, 34). However, NETs can be considered of developing cardiovascular events (42) and coronary disease
as a risk factor of future cardiovascular events because of their progression (43). Patients at risk for future vascular events present
role in atherosclerosis, inflammation, and thrombosis in small stable elevations of CRP over time, probably because of sustained
blood vessels (17, 22, 35, 36). vascular inflammation (44). Based on the study from Pearson et al.
Previous findings reported a circulating increase of NETs in (45), it has been recommended by the Centers of Disease Control
T2DM patients (37) and that local stimuli affect spontaneous and Prevention/American Heart Association, to categorize pa-
NETosis in isolated neutrophils from diabetic patients (18). In tients as low- (,1 mg/l CRP), mid- (1–3 mg/l CRP), or high-risk
contrast, Miyoshi et al. (38) reported a nonsignificant increase in (.3 mg/l CRP) for cardiovascular events, and an inflammatory
circulating NETs from well-controlled T2DM patients when status was set for CRP values $3 mg/l (45, 46). In our study, in each
compared with HC. In their study, when the authors separated the of the three patient groups (T2DM, HF, and HF with T2DM),
TABLE II. Characteristics of populations based on the CRP level
CRP , 1 mg/l (n = 25) CRP = 1–3 mg/l (n = 35) CRP . 3 mg/l (n = 31) p Value
NETs (OD) 0.079 6 0.010 0.160 6 0.022 0.158 6 0.026 p# 0.015
CRP (mg/l) 0.65 6 0.06 1.94 6 0.10 7.18 6 0.61 p# 0.016
MPO (ng/ml) 292.1 6 33.0 311.0 6 32 411.8 6 48.3 p= 0.034
IL-6 (pg/ml) 0 1.74 6 0.51 4.77 6 0.57 p= 0.0001
ST2 (ng/ml) 22.0 6 1.8 31.1 6 4.8 58.0 6 15.6 p= 0.045
Creatinine (mmol/l) 90.0 6 3 100.4 6 6.6 126.1 6 10 p= 0.002
Fasting glucose (mmol/l) 6.34 6 0.53 7.12 6 0.43 7.77 6 0.47 p= 0.036
Total cholesterol (mmol/l) 4.49 6 0.28 3.85 6 0.17 3.26 6 0.19 p= 0.001
LDL (mmol/l) 2.66 6 0.27 2.11 6 0.16 1.65 6 0.14 p= 0.001
Triglycerides (mmol/l) 1.80 6 0.15 1.81 6 0.17 1.58 6 0.15
Statins (%) 11 (44) 16 (45.7) 21 (67.7)
Comorbidity n (%) 4 (16) 16 (45.7) 16 (51.6) p = 0.005
Age (y) 60.2 6 1.6 65.6 6 2 65.6 6 2
Sex: male n (%) 21 (84) 24 (68.6) 23 (74.2)
HC n (%) 15 (60) 9 (25.7) 1 (3.2)
T2DM n (%) 3 (12) 12 (34.3) 6 (19.4)
HF n (%) 3 (12) 8 (22.9) 8 (25.8)
HF with T2DM n (%) 4 (16) 6 (17.1) 16 (51.6)
Values are mean 6 SE or percentage.
ST2, cardiac damage biomarker.
https://doi.org/10.4049/immunohorizons.1900026
ImmunoHorizons CRP INDUCES NETosis IN HEART FAILURE PATIENTS 385
of other clinical variables, but MPO has been shown as an
influential factor in the progression of cardiovascular disease
among these patients (48). We selected T2DM patients with stable
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
FIGURE 5. NETs release by neutrophils in presence of serum.
Neutrophils were incubated for 60 min with serum from all three pa-
tient groups (T2DM, HF, HF with T2DM) and from HC (a–e). A significant
increase of NETs release was observed with the serum from HF and HF
with T2DM (f). Data shown as mean 6 SEM (n = 7). *p # 0.03 as
compared with PBS.
50% of them had CRP serum levels higher than 3 mg/l, even in
absence of any acute inflammatory condition. In all four groups
(T2DM, HF, HF with T2DM, and HC), we observed a correlation
between the levels of NETs and CRP concentration. Therefore, we
used CRP risk classification (low, mid and high) to assess its effect
on NETs synthesis. The two groups with CRP levels in the mid- FIGURE 6. CRP is an essential serum element for NETosis induction.
and high-risk range had a significant increase of NETs in serum. Neutrophils were treated for 60 min with controls (PBS, PBS plus CRP-
Surprisingly, the group with CRP .3 mg/l had lower cholesterol, depletion beads, and PBS plus agarose beads) with serums from patients (CRP
LDL, and triglyceride levels compared with the other two groups. 4 mg/l), matched CRP-depleted serums (CRP ,0.16 mg/l), and matched
This can be explained by lipid-lowering treatment routinely serums (CRP 4 mg/l) with control agarose beads (a). The serums from
prescribed to T2DM and cardiovascular disease patients. Despite patients (CRP 4 mg/l) and matched serums (CRP 4 mg/l) with control
these treatments, there was an increase in MPO and IL-6 serum beads significantly increased NETosis, *p # 0.04 compared with PBS, whereas
concentrations in the group with CRP .3 mg/l as well as NETs. matched CRP-depleted serums (CRP ,0.16 mg/l) were unable to increase
The correlation between MPO and NETs concentrations was NETs release (a). In another set of experiments, neutrophils were incubated
expected, as both increase upon neutrophil activation (17). MPO with control vehicles (PBS and Tris buffer) for 60 min, IL-8 (25 nM; positive
serum levels are characterized by pro-oxidative and proinflam- control), and rhCRP (1, 5, 10 mg/l). At the highest concentration, rhCRP in-
matory properties and correlate with CRP levels and WBC count duced a significant increase in NETs release (b), *p # 0.025 compared with
(47). T2DM is associated with a mild increase of MPO independent PBS. Data shown as mean 6 SEM (n = 6–7 for each group, including HC).
https://doi.org/10.4049/immunohorizons.1900026
386 CRP INDUCES NETosis IN HEART FAILURE PATIENTS ImmunoHorizons
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
FIGURE 7. Proposed schematic illustration on the role of CRP in the induction of NETosis and its implication in HF and diabetes.
HF and/or T2DM are marked by low-grade inflammation that increases concentration of inflammatory proteins in serum including IL-6 and CRP.
IL-6 will increase hepatic CRP release in the bloodstream, which, in turn, activates neutrophils to induce NETosis, leading to further aggravated
vasculature injury and associated cardiovascular events.
and controlled glycaemia and without diagnosed heart condi- directly involved in NETosis, which is itself more accepted as a
tions, which reflected in a nonsignificant MPO and NETs cause of cardiovascular complications. Recently, Martinod et al.
increase in the serum. Similarly, the basal activation of healthy (52) proposed a role for NETs in age-related cardiac fibrosis in
neutrophils tested in vitro was not exacerbated by the serum of mice, but such a study has not yet been conducted in humans.
T2DM patients. Furthermore, “netting” neutrophils may play important roles in
All three groups of patients in our study had significant the promotion of atherosclerosis, vasculitis of different aetiologies,
increases in IL-6 levels. Besides being the primary cytokine and other vascular disorders (17, 22).
promoting hepatic CRP production, IL-6 can lead to cardiomyo- To further validate whether the CRP contained in the serum
cytes hypertrophy, myocardial dysfunction, and muscle wasting plays a role in NETs release, we treated neutrophils with CRP-
(49). Increased IL-6 concentrations have been previously shown depleted serums, showing that they lost their capacity to induce
in the circulation of HF and T2DM patients (50). Although, in our NETosis. We also showed that rhCRP induces NETosis in a
study, it did not correlate directly with NETs content in serum, the concentration-dependent manner. In addition, to our knowledge,
indirect relationship can be assumed through induction of CRP our novel finding that CRP can promote NETosis, other studies
produced in the liver. have reported the capacity of CRP to induce neutrophil phagocy-
As it was previously described, elevated levels of ST2 tosis, motility, and binding to endothelium (53, 54). Together these
(biomarker of cardiac stress) at baseline and follow-up were data reinforce the notion that CRP is not simply a predictive
shown to be associated with an increased risk of adverse clinical biomarker of inflammation but also a proinflammatory agonist
events (39, 40). In our study, a random selection of serum collected acting likely through its binding capacity onto FcgR expressed
from each group of volunteers was tested for ST2, and the average on neutrophils (54–57). Forthcoming studies will be needed to
value in the group with CRP concentration .3 mg/l was above the better delineate the cellular mechanisms involved in CRP-mediated
diagnostic cut-off value for chronic HF (.35 ng/ml) (39). NETosis.
In addition to its predictive role in determining cardiovascular In summary, our study proposes, to our knowledge, a novel
risk, there is evidence that CRP might serve as an active participant mechanism by which CRP may increase the risk of cardiovascu-
in atherogenesis, as it is detected in human atherosclerotic plaques lar events in these high-risk patients through NETs induction.
(51). Our study proposes an additional mechanism by which CRP is In this study, we report that neutrophils can respond to chronic
https://doi.org/10.4049/immunohorizons.1900026ImmunoHorizons CRP INDUCES NETosis IN HEART FAILURE PATIENTS 387
inflammatory cytokines and can have a damaging effect on the 8. Danesh, J., J. G. Wheeler, G. M. Hirschfield, S. Eda, G. Eiriksdottir,
overall inflammatory state (Fig. 7). Further studies that will A. Rumley, G. D. Lowe, M. B. Pepys, and V. Gudnason. 2004.
C-reactive protein and other circulating markers of inflammation in the
examine the relationship of anti-inflammatory therapies aiming
prediction of coronary heart disease. N. Engl. J. Med. 350: 1387–1397.
to reduce CRP levels and changes in NETosis are needed. 9. Shah, A. D., S. Denaxas, O. Nicholas, A. D. Hingorani, and H. Hemingway.
2017. Neutrophil counts and initial presentation of 12 cardiovascular
Study limitations diseases: a CALIBER cohort study. [Published erratum appears in 2017
This is a small observational study with the primary goal to assess J. Am. Coll. Cardiol. 69: 3125–3126.] J. Am. Coll. Cardiol. 69: 1160–1169.
the effects of chronic inflammation in patients with HF and/or 10. Tracchi, I., G. Ghigliotti, M. Mura, S. Garibaldi, P. Spallarossa,
C. Barisione, V. Boasi, M. Brunelli, L. Corsiglia, A. Barsotti, and
T2DM on neutrophil activation. No discrimination was made
C. Brunelli. 2009. Increased neutrophil lifespan in patients with
between HFrEF and HFpEF. Despite their different phenotypes, congestive heart failure. Eur. J. Heart Fail. 11: 378–385.
the increase of inflammatory biomarkers has been reported in both 11. Kaplan, M. J., and M. Radic. 2012. Neutrophil extracellular traps:
conditions. Nevertheless, additional studies are needed to define double-edged swords of innate immunity. J. Immunol. 189: 2689–
the role of CRP and NETs in both forms of HF (4). As detailed 2695.
earlier, although there is significant difference between the age 12. Fuchs, T. A., U. Abed, C. Goosmann, R. Hurwitz, I. Schulze, V. Wahn,
Y. Weinrauch, V. Brinkmann, and A. Zychlinsky. 2007. Novel cell
of HC and patients with HF with T2DM, this did not affect the
death program leads to neutrophil extracellular traps. J. Cell Biol. 176:
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
correlation between NETs and CRP or other inflammatory 231–241.
markers. 13. Yipp, B. G., B. Petri, D. Salina, C. N. Jenne, B. N. Scott, L. D. Zbytnuik,
K. Pittman, M. Asaduzzaman, K. Wu, H. C. Meijndert, et al. 2012.
Infection-induced NETosis is a dynamic process involving neutrophil
DISCLOSURES multitasking in vivo. Nat. Med. 18: 1386–1393.
14. Yu, X., J. Tan, and S. L. Diamond. 2018. Hemodynamic force triggers
The authors have no financial conflicts of interest. rapid NETosis within sterile thrombotic occlusions. J. Thromb.
Haemost. 16: 316–329.
15. Carestia, A., T. Kaufman, L. Rivadeneyra, V. I. Landoni, R. G. Pozner,
ACKNOWLEDGMENTS S. Negrotto, L. P. D’Atri, R. M. Gómez, and M. Schattner. 2016. Me-
diators and molecular pathways involved in the regulation of neu-
We are thankful to the volunteers for kindly providing blood samples and trophil extracellular trap formation mediated by activated platelets.
to Louis Villeneuve for confocal microscopy technical support. J. Leukoc. Biol. 99: 153–162.
16. Maugeri, N., L. Campana, M. Gavina, C. Covino, M. De Metrio,
C. Panciroli, L. Maiuri, A. Maseri, A. D’Angelo, M. E. Bianchi, et al.
REFERENCES 2014. Activated platelets present high mobility group box 1 to neu-
trophils, inducing autophagy and promoting the extrusion of neu-
trophil extracellular traps. J. Thromb. Haemost. 12: 2074–2088.
1. Ponikowski, P., A. A. Voors, S. D. Anker, H. Bueno, J. G. F. Cleland,
17. Mitsios, A., A. Arampatzioglou, S. Arelaki, I. Mitroulis, and K. Ritis.
A. J. S. Coats, V. Falk, J. R. González-Juanatey, V. P. Harjola,
2017. NETopathies? unraveling the dark side of old diseases through
E. A. Jankowska, et al; ESC Scientific Document Group. 2016. 2016
neutrophils. Front. Immunol. 7: 678.
ESC guidelines for the diagnosis and treatment of acute and chronic
heart failure: the task force for the diagnosis and treatment of acute 18. Wong, S. L., M. Demers, K. Martinod, M. Gallant, Y. Wang,
and chronic heart failure of the European Society of Cardiology (ESC) A. B. Goldfine, C. R. Kahn, and D. D. Wagner. 2015. Diabetes primes
developed with the special contribution of the Heart Failure Associ- neutrophils to undergo NETosis, which impairs wound healing. Nat.
ation (HFA) of the ESC. [Published erratum appears in 2018 Eur. Med. 21: 815–819.
Heart J. 39: 860.] Eur. Heart J. 37: 2129–2200. 19. Brinkmann, V., U. Reichard, C. Goosmann, B. Fauler, Y. Uhlemann,
2. Dunlay, S. M., V. L. Roger, and M. M. Redfield. 2017. Epidemiology of D. S. Weiss, Y. Weinrauch, and A. Zychlinsky. 2004. Neutrophil ex-
heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 14: tracellular traps kill bacteria. Science 303: 1532–1535.
591–602. 20. Metzler, K. D., T. A. Fuchs, W. M. Nauseef, D. Reumaux, J. Roesler,
3. Danesh, J., P. Whincup, M. Walker, L. Lennon, A. Thomson, I. Schulze, V. Wahn, V. Papayannopoulos, and A. Zychlinsky. 2011.
P. Appleby, J. R. Gallimore, and M. B. Pepys. 2000. Low grade Myeloperoxidase is required for neutrophil extracellular trap for-
inflammation and coronary heart disease: prospective study and mation: implications for innate immunity. Blood 117: 953–959.
updated meta-analyses. BMJ 321: 199–204. 21. Rao, A. N., N. M. Kazzaz, and J. S. Knight. 2015. Do neutrophil ex-
4. Bozkurt, B., D. L. Mann, and A. Deswal. 2010. Biomarkers of in- tracellular traps contribute to the heightened risk of thrombosis in
flammation in heart failure. Heart Fail. Rev. 15: 331–341. inflammatory diseases? World J. Cardiol. 7: 829–842.
5. Benjamin, E. J., S. S. Virani, C. W. Callaway, A. M. Chamberlain, 22. Döring, Y., O. Soehnlein, and C. Weber. 2017. Neutrophil extracellular
A. R. Chang, S. Cheng, S. E. Chiuve, M. Cushman, F. N. Delling, traps in atherosclerosis and atherothrombosis. Circ. Res. 120: 736–743.
R. Deo, et al; American Heart Association Council on Epidemiology and 23. Xu, P. C., S. Lin, X. W. Yang, D. M. Gu, T. K. Yan, L. Wei, and
Prevention Statistics Committee and Stroke Statistics Subcommittee. B. L. Wang. 2015. C-reactive protein enhances activation of coagula-
2018. Heart disease and stroke statistics-2018 update: a report from the tion system and inflammatory response through dissociating into
American heart association. [Published erratum appears in 2018 Circu- monomeric form in antineutrophil cytoplasmic antibody-associated
lation 137: e493.] Circulation 137: e67–e492. vasculitis. BMC Immunol. 16: 10.
6. Bahtiyar, G., D. Gutterman, and H. Lebovitz. 2016. Heart failure: a major 24. Pitt, B., M. A. Pfeffer, S. F. Assmann, R. Boineau, I. S. Anand,
cardiovascular complication of diabetes mellitus. Curr. Diab. Rep. 16: 116. B. Claggett, N. Clausell, A. S. Desai, R. Diaz, J. L. Fleg, et al; TOPCAT
7. Dick, S. A., and S. Epelman. 2016. Chronic heart failure and inflam- Investigators. 2014. Spironolactone for heart failure with preserved
mation: what do we really know? Circ. Res. 119: 159–176. ejection fraction. N. Engl. J. Med. 370: 1383–1392.
https://doi.org/10.4049/immunohorizons.1900026388 CRP INDUCES NETosis IN HEART FAILURE PATIENTS ImmunoHorizons
25. Grodin, J. L., S. Philips, W. Mullens, P. Nijst, P. Martens, J. C. Fang, and diabetes: JACC state-of-the-art review. J. Am. Coll. Cardiol. 73:
M. H. Drazner, W. H. W. Tang, and A. Pandey. 2019. Prognostic im- 602–611.
plications of plasma volume status estimates in heart failure with 41. Bajpai, A., and D. G. Tilley. 2018. The role of leukocytes in diabetic
preserved ejection fraction: insights from TOPCAT. Eur. J. Heart Fail. cardiomyopathy. Front. Physiol. 9: 1547.
21: 634–642. 42. Pfützner, A., and T. Forst. 2006. High-sensitivity C-reactive protein as
26. Selvaraj, S., B. Claggett, S. J. Shah, I. Anand, J. L. Rouleau, E. O’Meara, cardiovascular risk marker in patients with diabetes mellitus. Diabetes
A. S. Desai, E. F. Lewis, B. Pitt, N. K. Sweitzer, et al. 2018. Prognostic Technol. Ther. 8: 28–36.
value of albuminuria and influence of spironolactone in heart failure 43. Fonseca, F. A., and M. C. Izar. 2016. High-sensitivity C-reactive
with preserved ejection fraction. Circ. Heart Fail. 11: e005288. protein and cardiovascular disease across countries and ethnicities.
27. Lavoie, S. S., E. Dumas, B. Vulesevic, P.-E. Neagoe, M. White, and Clinics (São Paulo) 71: 235–242.
M. G. Sirois. 2018. Synthesis of human neutrophil extracellular traps 44. Ridker, P. M. 2009. C-reactive protein: eighty years from discovery to
contributes to angiopoietin-mediated in vitro proinflammatory and emergence as a major risk marker for cardiovascular disease. Clin.
proangiogenic activities. J. Immunol. 200: 3801–3813. Chem. 55: 209–215.
28. Kessenbrock, K., M. Krumbholz, U. Schönermarck, W. Back, 45. Pearson, T. A., G. A. Mensah, R. W. Alexander, J. L. Anderson,
W. L. Gross, Z. Werb, H. J. Gröne, V. Brinkmann, and D. E. Jenne. R. O. Cannon III, M. Criqui, Y. Y. Fadl, S. P. Fortmann, Y. Hong,
2009. Netting neutrophils in autoimmune small-vessel vasculitis. Nat. G. L. Myers, et al; American Heart Association. 2003. Markers of
Med. 15: 623–625. inflammation and cardiovascular disease: application to clinical and
29. Kapur, R., K. M. Heitink-Pollé, L. Porcelijn, A. E. Bentlage, public health practice: a statement for healthcare professionals from
Downloaded from http://www.immunohorizons.org/ by guest on April 18, 2021
M. C. Bruin, R. Visser, D. Roos, R. B. Schasfoort, M. de Haas, C. E. van the Centers for Disease Control and Prevention and the American
der Schoot, and G. Vidarsson. 2015. C-reactive protein enhances IgG- Heart Association. Circulation 107: 499–511.
mediated phagocyte responses and thrombocytopenia. Blood 125: 46. Sabatine, M. S., D. A. Morrow, K. A. Jablonski, M. M. Rice,
1793–1802. J. W. Warnica, M. J. Domanski, J. Hsia, B. J. Gersh, N. Rifai,
30. Hazeldine, J., P. Harris, I. L. Chapple, M. Grant, H. Greenwood, P. M. Ridker, et al; PEACE Investigators. 2007. Prognostic signifi-
A. Livesey, E. Sapey, and J. M. Lord. 2014. Impaired neutrophil ex- cance of the Centers for Disease Control/American Heart Association
tracellular trap formation: a novel defect in the innate immune system high-sensitivity C-reactive protein cut points for cardiovascular and
of aged individuals. Aging Cell 13: 690–698. other outcomes in patients with stable coronary artery disease. Cir-
31. Caielli, S., J. Banchereau, and V. Pascual. 2012. Neutrophils come of culation 115: 1528–1536.
age in chronic inflammation. Curr. Opin. Immunol. 24: 671–677. 47. Loria, V., I. Dato, F. Graziani, and L. M. Biasucci. 2008. Myeloper-
oxidase: a new biomarker of inflammation in ischemic heart disease
32. Pérez-Sánchez, C., P. Ruiz-Limón, M. A. Aguirre, Y. Jiménez-Gómez,
and acute coronary syndromes. Mediators Inflamm. 2008: 135625.
I. Arias-de la Rosa, M. C. Ábalos-Aguilera, A. Rodriguez-Ariza,
48. Wiersma, J. J., M. C. Meuwese, J. N. van Miert, A. Kastelein,
M. C. Castro-Villegas, R. Ortega-Castro, P. Segui, et al. 2017. Di-
J. G. Tijssen, J. J. Piek, and M. D. Trip. 2008. Diabetes mellitus type 2
agnostic potential of NETosis-derived products for disease activity,
is associated with higher levels of myeloperoxidase. Med. Sci. Monit.
atherosclerosis and therapeutic effectiveness in Rheumatoid arthritis
14: CR406–CR410.
patients. J. Autoimmun. 82: 31–40.
49. Kamimura, D., K. Ishihara, and T. Hirano. 2003. IL-6 signal trans-
33. Wang, H., L. L. Sha, T. T. Ma, L. X. Zhang, M. Chen, and M. H. Zhao.
duction and its physiological roles: the signal orchestration model.
2016. Circulating level of neutrophil extracellular traps is not a useful
Rev. Physiol. Biochem. Pharmacol. 149: 1–38.
biomarker for assessing disease activity in antineutrophil cytoplasmic
50. Esteve, E., A. Castro, A. López-Bermejo, J. Vendrell, W. Ricart, and
antibody-associated vasculitis. PLoS One 11: e0148197.
J. M. Fernández-Real. 2007. Serum interleukin-6 correlates with
34. Arai, Y., K. Yamashita, K. Mizugishi, T. Watanabe, S. Sakamoto, endothelial dysfunction in healthy men independently of insulin
T. Kitano, T. Kondo, H. Kawabata, N. Kadowaki, and A. Takaori-Kondo. sensitivity. Diabetes Care 30: 939–945.
2013. Serum neutrophil extracellular trap levels predict thrombotic 51. Paffen, E., and M. P. DeMaat. 2006. C-reactive protein in athero-
microangiopathy after allogeneic stem cell transplantation. Biol. Blood
sclerosis: a causal factor? Cardiovasc. Res. 71: 30–39.
Marrow Transplant. 19: 1683–1689. 52. Martinod, K., T. Witsch, L. Erpenbeck, A. Savchenko, H. Hayashi,
35. Mozzini, C., U. Garbin, A. M. Fratta Pasini, and L. Cominacini. 2017. D. Cherpokova, M. Gallant, M. Mauler, S. M. Cifuni, and D. D. Wagner.
An exploratory look at NETosis in atherosclerosis. Intern. Emerg. 2017. Peptidylarginine deiminase 4 promotes age-related organ fibrosis.
Med. 12: 13–22. J. Exp. Med. 214: 439–458.
36. Jorch, S. K., and P. Kubes. 2017. An emerging role for neutrophil 53. Schlayer, H. J., U. Karck, U. Ganter, R. Hermann, and K. Decker. 1987.
extracellular traps in noninfectious disease. Nat. Med. 23: 279–287. Enhancement of neutrophil adherence to isolated rat liver sinusoidal
37. Menegazzo, L., S. Ciciliot, N. Poncina, M. Mazzucato, M. Persano, endothelial cells by supernatants of lipopolysaccharide-activated
B. Bonora, M. Albiero, S. Vigili de Kreutzenberg, A. Avogaro, and monocytes. Role of tumor necrosis factor. J. Hepatol. 5: 311–321.
G. P. Fadini. 2015. NETosis is induced by high glucose and associated 54. Ling, M. R., I. L. Chapple, A. J. Creese, and J. B. Matthews. 2014.
with type 2 diabetes. Acta Diabetol. 52: 497–503. Effects of C-reactive protein on the neutrophil respiratory burst in
38. Miyoshi, A., M. Yamada, H. Shida, D. Nakazawa, Y. Kusunoki, vitro. Innate Immun. 20: 339–349.
A. Nakamura, H. Miyoshi, U. Tomaru, T. Atsumi, and A. Ishizu. 2016. 55. Bodman-Smith, K. B., A. J. Melendez, I. Campbell, P. T. Harrison,
Circulating neutrophil extracellular trap levels in well-controlled type J. M. Allen, and J. G. Raynes. 2002. C-reactive protein-mediated
2 diabetes and pathway involved in their formation induced by high- phagocytosis and phospholipase D signalling through the high-affinity
dose glucose. Pathobiology 83: 243–251. receptor for immunoglobulin G (FcgammaRI). Immunology 107:
39. Carestia, A., G. Frechtel, G. Cerrone, M. A. Linari, C. D. Gonzalez, 252–260.
P. Casais, and M. Schattner. 2016. NETosis before and after hyper- 56. Stein, M. P., J. C. Edberg, R. P. Kimberly, E. K. Mangan, D. Bharadwaj,
glycemic control in type 2 diabetes mellitus patients. PLoS One 11: C. Mold, and T. W. Du Clos. 2000. C-reactive protein binding to
e0168647. FcgammaRIIa on human monocytes and neutrophils is allele-specific.
40. McHugh, K., A. D. DeVore, J. Wu, R. A. Matsouaka, G. C. Fonarow, J. Clin. Invest. 105: 369–376.
P. A. Heidenreich, C. W. Yancy, J. B. Green, N. Altman, and 57. Sproston, N. R., and J. J. Ashworth. 2018. Role of C-reactive protein at
A. F. Hernandez. 2019. Heart failure with preserved ejection fraction sites of inflammation and infection. Front. Immunol. 9: 754.
https://doi.org/10.4049/immunohorizons.1900026You can also read

















































