IGCS 2020 Abstracts: Oral Plenary Sessions
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
IGCS 2020 Abstracts: Oral Plenary Sessions Abstracts: Plenary I Thursday, September 10, 2020 14:30 – 15:00 UTC Channel 1 Abstracts: Plenary II Thursday, September 10, 2020 15:00 – 16:00 UTC Channel 1 Abstracts: Plenary III Friday, September 11, 2020 11:00 – 12:00 UTC Channel 1 Abstracts: Plenary V Sunday, September 13, 2020 5:00 – 6:00 UTC Channel 1
1 IGCS20_1256 Oral Plenary Plenary I Avelumab in combination with and/or following chemotherapy vs chemotherapy in treatment-naive patients with ovarian cancer: biomarker analyses from the phase 3 JAVELIN Ovarian 100 trial J. Ledermann1, N. Colombo2, A. Oza3, K. Fujiwara4, M.J. Birrer5, L. Randall6, E. Poddubskaya7, G. Scambia8, Y.V. Shparyk9, M.C. Lim10, S.M Bhoola11, J. Sohn12, K. Yonemori13, R.A. Stewart14, X. Zhang15, J. Perkins Smith15, C. Linn16, B.J. Monk17 1 UCL Cancer Institute and UCL Hospitals NHS Foundation Trust, United Kingdom; 2University of Milan-Bicocca and Istituto Europeo di Oncologia, IRCCS, Italy; 3Princess Margaret Cancer Centre, Canada; 4Saitama Medical University International Medical Center, Japan; 5O’Neal Comprehensive Cancer Center, The University of Alabama at Birmingham, United States; 6 Virginia Commonwealth University, Massey Cancer Center, United States; 7I.M. Sechenov First Moscow State Medical University and Clinical Center Vitamed, Russia; 8Gynecologic Oncology Unit, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Italy; 9Lviv State Oncological Regional Treatment and Diagnostic Center, Ukraine; 10Research Institute and Hospital, National Cancer Center, South Korea; 11Arizona Oncology Associates, PC - HAL, United States; 12 Severance Hospital, Yonsei University Health System, South Korea; 13Department of Breast and Medical Oncology, National Cancer Center Hospital, Japan; 14Pfizer Oncology, Pfizer Inc, United States; 15Pfizer Oncology, Pfizer Inc, United States; 16Global Product Development, Pfizer Inc, Taiwan; 17Arizona Oncology (US Oncology Network), University of Arizona and Creighton University, United States Introduction: In the JAVELIN Ovarian 100 trial (NCT02718417), avelumab (anti–PD-L1) in combination with chemotherapy or as maintenance did not improve progression-free survival (PFS) vs chemotherapy followed by observation in treatment-naive patients with epithelial ovarian cancer (EOC; hazard ratios [95% CI] were 1.14 [0.832, 1.565] and 1.43 [1.051, 1.946], respectively). The trial was terminated when prespecified futility boundaries were crossed at the interim analysis, and study treatment was subsequently discontinued. Here we report biomarker analyses. Methods: Women with stage III-IV EOC (post debulking/cytoreductive surgery or candidates for neoadjuvant chemotherapy) were randomized 1:1:1 to receive carboplatin/paclitaxel chemotherapy (6 cycles) followed by avelumab every 2 weeks as maintenance (CTx→Ave), chemotherapy + avelumab (10 mg/kg every 3 weeks) followed by avelumab every 2 weeks as maintenance (CTx+Ave→Ave), or chemotherapy followed by observation (CTx→O; control arm). The primary endpoint was PFS by blinded independent central review per RECIST version 1.1. Pretreatment tumor tissue was analyzed by immunohistochemistry (CD8 and PD- L1) and next-generation DNA and RNA sequencing.
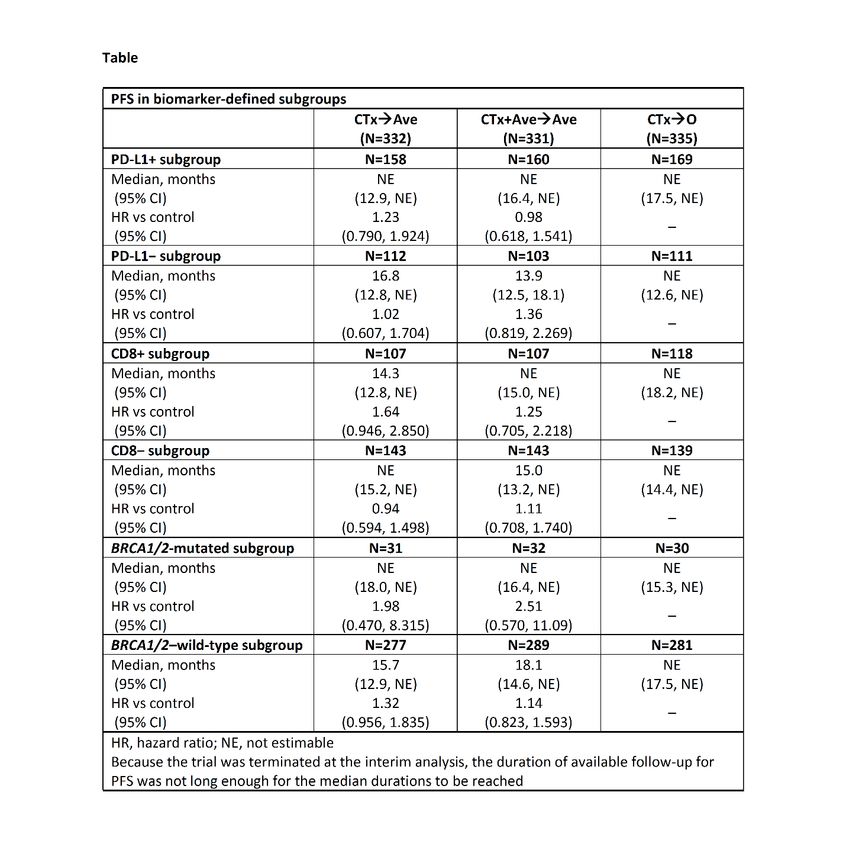
Results: 998 patients were randomized. Subgroup analyses based on PD-L1, CD8, and germline BRCA1/2 status did not identify subsets with clear PFS benefit in either avelumab arm vs control (Table). Whole-exome and RNA sequencing analyses will be presented. Conclusions: In the JAVELIN Ovarian 100 trial, PD-L1, CD8, and germline BRCA1/2 status did not predict differential clinical benefit with the addition of avelumab to chemotherapy in treatment-naive patients with EOC.
2 IGCS20_1255 Oral Plenary Plenary I Efficacy and Safety of Lenvatinib Plus Pembrolizumab in Patients with Previously Treated Ovarian Cancer in the Multicohort Phase 2 LEAP-005 Study A. González-Martín1, H. Chung2, E. Saada-Bouzid3, E. Yanez4, H. Senellart5, P.A. Cassier6, B. Basu7, R. Ghori8, P. Kubiak9, A. Smith10, K. Norwood8, Z. Lwin11 1 Clínica Universidad de Navarra, Spain; 2Yonsei Cancer Center, Yonsei University College of Medicine, South Korea; 3Department of Medical Oncology, Centre de Lutte Contre le Cancer Antoine Lacassagne, France; 4Oncology-Hematology Unit, Department of Internal Medicine, School of Medicine, Universidad de la Frontera, Chile; 5Institut de Cancérologie de l’Ouest, Centre René Gauducheau ICO, France; 6Department of Medical Oncology, Centre Léon Bérard, France; 7Department of Oncology, University of Cambridge, United Kingdom; 8Merck & Co., Inc., United States; 9Eisai Inc., United States; 10Eisai Ltd., United Kingdom; 11Royal Brisbane and Women's Hospital, Australia Introduction: Lenvatinib, an antiangiogenic multiple receptor tyrosine kinase inhibitor, plus pembrolizumab, a programmed death-1 immune checkpoint inhibitor, demonstrated promising clinical benefit in a previous phase Ib/II trial across several cancer types (ClinicalTrials.gov, NCT02501096). We assessed clinical outcomes with lenvatinib plus pembrolizumab in patients with ovarian cancer in the ongoing, open-label, multicohort, phase 2 LEAP-005 study (ClinicalTrials.gov, NCT03797326). Methods: Female patients aged ≥18 years with histologically/cytologically confirmed, metastatic/unresectable ovarian cancer, measurable disease per RECIST v1.1, ECOG performance status 0/1, and 3 prior lines of therapy were enrolled. Patients received lenvatinib 20 mg daily plus pembrolizumab 200 mg every 3 weeks for 35 cycles, or until confirmed disease progression or unacceptable toxicity. Primary endpoints were objective response rate (ORR; response assessed every 9 weeks for 54 weeks, then every 12 weeks, by blinded independent central review per RECIST v1.1) and safety. Secondary endpoints included disease control rate, duration of response, and progression-free survival. Results: 31 patients with ovarian cancer received ≥1 dose of lenvatinib plus pembrolizumab in LEAP-005 (median age 62 years [range 40–76]); median study follow-up was 7.8 months (range, 4.6–12.4) as of April 10, 2020. ORR was 32% (95% CI, 17–51); other efficacy endpoints were also favorable (Table). Treatment-related adverse events occurred in 29 (94%) patients (Table). Conclusion: Lenvatinib plus pembrolizumab demonstrated encouraging efficacy and manageable safety in patients with heavily pretreated ovarian cancer, including those with prior platinum failure and those with previous bevacizumab exposure.
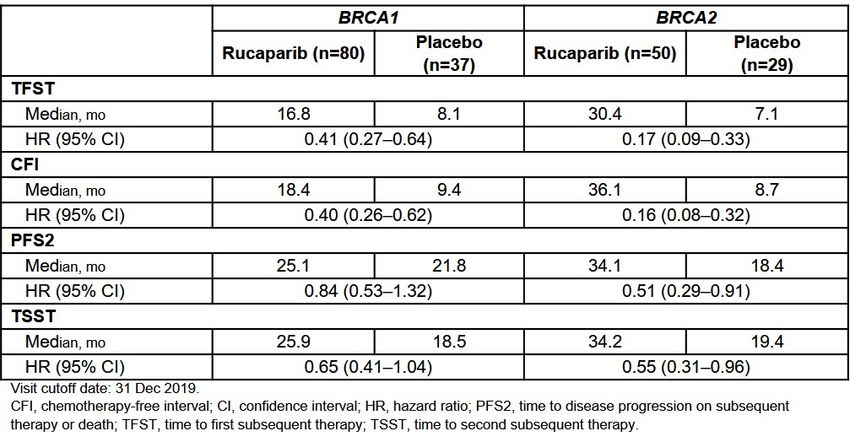
3 IGCS20_1268 Oral Plenary Plenary I Postprogression Efficacy Outcomes From the Phase 3 ARIEL3 Study of Rucaparib in Patients With Platinum-Sensitive Recurrent Ovarian Carcinoma Associated With Either BRCA1 or BRCA2 Mutations J. Weberpals1, A. Oza2, D. Lorusso3, G. Scambia3, C. Aghajanian4, A. Oaknin5, A. Dean6, N. Colombo7, A.R. Clamp8, A. Leary9, R.W. Holloway10, M. Amenedo Gancedo11, P.C. Fong12, J.C. Goh13, D.M. O’Malley14, D.K. Armstrong15, S. Banerjee16, J. García-Donas17, E.M. Swisher18, T. Cameron19, L. Maloney20, S. Goble20, R.L. Coleman21, J.A. Ledermann22 1 Ottawa Hospital Research Institute, Canada; 2Princess Margaret Cancer Centre, University Health Network, Canada; 3Fondazione Policlinico Universitario A. Gemelli IRCCS, Italy; 4 Memorial Sloan Kettering Cancer Center, United States; 5Vall d’Hebron University Hospital, Vall d’Hebron Institute of Oncology (VHIO), Spain; 6St John of God Subiaco Hospital, Australia; 7 European Institute of Oncology IRCCS and University of Milan-Bicocca, Italy; 8The Christie NHS Foundation Trust and University of Manchester, United Kingdom; 9Gustave Roussy Cancer Center, INSERM U981, and Groupe d'Investigateurs Nationaux pour l'Etude des Cancers Ovariens (GINECO), France; 10AdventHealth Cancer Institute Orlando, United States; 11 Oncology Center of Galicia, Spain; 12Auckland City Hospital and University of Auckland, New Zealand; 13Royal Brisbane and Women’s Hospital, Herston and University of Queensland, Australia; 14The Ohio State University, James Cancer Center, United States; 15Johns Hopkins University School of Medicine, United States; 16The Royal Marsden NHS Foundation Trust and Institute of Cancer Research, United Kingdom; 17HM Hospitales—Centro Integral Oncológico Hospital de Madrid Clara Campal, Spain; 18University of Washington, United States; 19Clovis Oncology UK Ltd., United Kingdom; 20Clovis Oncology, Inc., United States; 21US Oncology Research, United States; 22UCL Cancer Institute, University College London and UCL Hospitals, United Kingdom Introduction: In ARIEL3 (NCT01968213), rucaparib maintenance for recurrent ovarian cancer (rOC) significantly improved investigator-assessed PFS and postprogression efficacy outcomes versus placebo regardless of biomarker status. PFS was also improved in patients with rOC associated with either BRCA1 or BRCA2 mutations (HR, 0.32 [95% CI, 0.19–0.53] and 0.12 [0.06–0.26], respectively). This exploratory analysis further examined the subgroup of patients with rOC associated with BRCA1 or BRCA2 mutations to assess the durability of the clinical benefit of rucaparib maintenance following disease progression. Methods: Patients were randomised 2:1 to oral rucaparib (600 mg twice daily) or placebo. Postprogression efficacy endpoints were assessed in patients with germline or somatic BRCA1 or BRCA2 mutations. Results: Investigator-assessed postprogression efficacy endpoints for patients with either BRCA1 or BRCA2 mutations are presented in the Table.
There was a trend for better outcomes across all endpoints in patients with BRCA1 and BRCA2 mutations, with larger differences between the median values among patients with a BRCA2 mutation. The treatment-by-mutation group interaction test reached statistical significance for TFST and CFI. Among rucaparib-treated patients, the most common treatment-emergent adverse events (any grade) in the BRCA1 and BRCA2 subgroups were nausea (81.0% and 78.0%) and asthenia/fatigue (74.7% and 80.0%). Conclusions/Implications: All postprogression efficacy endpoints were longer with rucaparib maintenance than with placebo in both BRCA-mutant subgroups. Safety data for the two subgroups were similar and were consistent with the overall safety population.
4 IGCS20_1447 Oral Plenary Plenary II Refining Pathologic Interpretation of Endometrial Carcinomas: Lessons Learned from a Nationwide Study in a new Era of Molecular Classification E. Thompson1, J. Huvila1, S. Leung2, J. Irving3, N. van der Westhuizen3, M. Kinloch4, A. Lytwyn5, M. Sur5, C. Parra-Herran6, A. Yasmeen7, F. Gougeon8, C. Morin9, K. Grondin9, S. Offman10, T. Salisbury11, E. He12, J. Lawson12, J. Vanden Broek13, C. Bell14, K. Ennour-Idrissi9, C. Wohlmuth15, D. Vicus18, D. Vicus18, W. Gotlieb19, L. Helpman20, A. Lum1, J. Senz1, D. Huntsman1, B. Gilks11, J.N. McAlpine21 1 Molecular Oncology, University of British Columbia, Canada; 2Genetic Pathology Evaluation Centre, University of British Columbia, Canada; 3Pathology and Laboratory Medicine, Royal Jubilee Hospital and the University of British Columbia, Canada; 4Pathology and Laboratory Medicine, University of Saskatchewan,, Canada; 5Pathology and Molecular Medicine, McMaster University , Canada; 6Laboratory Medicine and Pathobiology, University of Toronto and Sunnybrook Health Sciences Centre, Canada; 7Gynecologic Oncology, Segal Cancer Center, Jewish General Hospital, McGill University, Canada; 8Department of Pathology, University of Montreal, Canada; 9Pathology Department, Centre Hospitalier Universitaire de Québec, L'Hôtel- Dieu de Québec, Laval University, Canada; 10Anatomical Pathology, Queen Elizabeth II Health Sciences Centre and Dalhousie University, Canada; 11Pathology and Laboratory Medicine, Vancouver General Hospital and University of British Columbia, Canada; 12MD Undergraduate Program, University of British Columbia, Canada; 13Faculty of Science, University of British Columbia, Canada; 14College of Medicine, University of Saskatchewan, Canada; 15Gynecologic Oncology, Department of Surgical Oncology, University Health Network, Canada ; 18 Gynecologic Oncology, Centre Hospitalier Universitaire de Québec, L'Hôtel-Dieu de Québec , Canada; 19Gynecologic Oncology, Jewish General Hospital, McGill University, Canada; 20 Gynecologic Oncology, Juravinski Cancer Center and McMaster University, Canada; 21 Gynecologic Oncology, Vancouver General Hospital and the University of British Columbia, Canada Objectives: Molecular classification of endometrial carcinoma (EC) enables consistent classification of tumours and provides valuable prognostic and predictive information. Herein we describe molecular subtype distribution and histomorphologic correlates in recently diagnosed (2016) ECs from across Canada. Methods: Molecular classification was performed on representative tumour specimens from participating centres. Clinicopathologic, management and outcome data were collected (REDCap). Results: 1453 ECs from 30 centres have been identified. Complete molecular (ProMisE) and outcome data is reportable for 862 patients. Histologic and clinicopathologic parameters associated with molecular subtype and are summarised in Table 1. Amongst participating centres, routine testing of MMR and p53 immunohistochemistry (IHC) was performed in only
23.5% (range 3.5-80.0% per centre) and 15% (2.2-45.7%) of cases respectively. We found p53 abn ECs across a range of histotypes, including low grade endometrioid EC. Subclonal p53 staining was observed in 3.9% of cases and significantly associated with the presence of pathogenic POLE mutations (p=
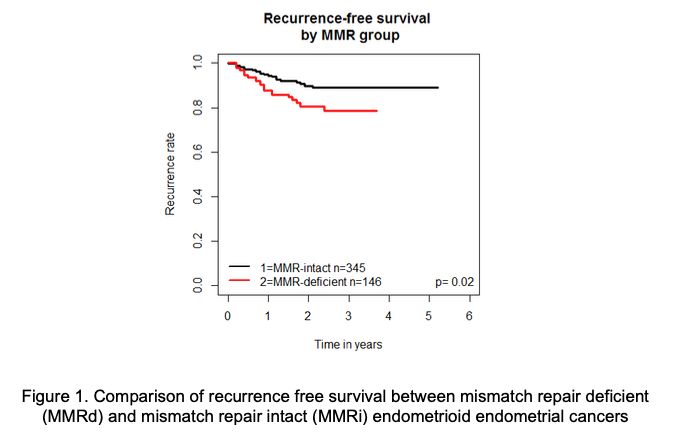
5 IGCS20_1251 Oral Plenary Plenary II Understanding the clinical implication of mismatch repair deficiency in endometrioid endometrial cancer through a prospective study S. Kim1, A. Tone2, A. Pollett3, R. Kim4, M. Cesari3, B. Clarke3, L. Eiriksson5, T. Hart6, S. Holter7, A. Lytwyn8, M. Maganti9, L. Oldfield10, T. Pugh10, S. Gallinger12, M. Bernardini1, A. Oza13, V. Dube3, J. Lerner-Ellis3, E. Van de Laar2, D. Vicus2, S. Ferguson1 1 Department of Obstetrics and Gynaecology, University of Toronto, Canada; 2Division of Gynecologic Oncology, Princess Margaret Cancer Centre/University Health Network/Sinai Health Systems, Canada; 3Department of Laboratory Medicine and Pathobiology, University of Toronto, Canada; 4Fred A Litwin Family Centre for Genetic Medicine, University Health Network, Canada; 5Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, Juravinski Cancer Centre, McMaster University, Canada; 6Department of Psychology, Ryerson University, Canada; 7Zane Cohen Centre for Digestive Diseases, Familial Gastrointestinal Cancer Registry, Mount Sinai Hospital, Canada; 8Division of Anatomical Pathology, Department of Pathology and Molecular Medicine, McMaster University, Canada; 9Department of Biostatistics, Princess Margaret Cancer Centre/University Health Network, University of Toronto, Canada; 10Department of Medical Biophysics, University of Toronto, Canada ; 12 Division of General Surgery, Princess Margaret Cancer Centre/University Health Network/Sinai Health Systems, Canada; 13Division of Medical Oncology and Hematology, Princess Margaret Cancer Centre/University Health Network/Sinai Health Systems, Canada Objectives: Findings on impact of mismatch repair deficiency (MMRd) on patient outcomes in endometrial cancer (EC) have been inconsistent to date. The objective of this study was to compare oncologic outcomes between MMRd and MMR-intact (MMRi) endometrioid EC (EEC). Methods: Between 2015-2018, we prospectively recruited 668 EC cases from three cancer centers in Ontario, Canada. Tumors were reflexively assessed for MMR protein expression by immunohistochemistry (IHC). Clinicopathological, treatment and survival data were compared between MMRd and MMRi cases. Results: Out of 668, there were 496 EEC (74%), with 347 MMRi (70%) and 149 MMRd (30%) cases treated with surgery and with complete follow-up information. Median follow-up was 16.8 months (6-96 months). MMRd tumors tended to be grade 2 or 3 (56% vs. 29%, p
deficient tumors had the lowest 3-year RFS compared to intact and other MMRd tumors (76% vs. 89% vs 87%, p=0.02). After adjusting for age, stage, grade, use of adjuvant treatment, and LVSI status, MLH1/PMS2 deficiency was still associated with the lowest RFS (p=0.05). Conclusions: MLH1/PMS2 deficient EECs exhibit more aggressive features compared to other MMRd and MMRi cases, with worse RFS. This may indicate an inherent difference in tumor biology, suggesting the importance of individualized management based on tumor’s molecular phenotype.
6 IGCS20_1049 Oral Plenary Plenary II Variation in practice in endometrial cancer (EC); can molecular classification direct care and reduce costs associated with management? E. Thompson1, A. Lum1, J. Huvila1, S. Scott3, V. Lui1, E. He1, T. Salisbury1, S. Keane4, S. Keane4, V. Samouelian5, J. Irving1, S. Salvador6, L. Helpman7, C. Wohlmuth8, M. Kinloch9, S. Offman3, D. Vicus8, K. Grondin10, W. Gotlieb6, M. Plante10, D. Huntsman1, A. Talhouk1, C.B. Gilks1, G. Hanley1, J. McAlpine1 1 University of British Columbia and BC Cancer, Canada ; 3Genetic Pathology Evaluation Center, Canada; 4Dalhousie University Medical School, Canada; 5Centre hospitalier de l'Université de Montréal, Canada; 6McGill University, Canada; 7McMaster University and the Juravinski Cancer Center, Canada; 8Sunnybrook Health Sciences Center, Canada; 9University of Saskatoon, Canada; 10Université Laval , Canada Objectives: We wished to assess the potential impact of directing EC management based on molecular classification, and the projected cost implications of molecular subtype-directed care. Methods: Surgical staging, treatment, surveillance, and hereditary cancer program(HCP) referrals were assessed for all ECs managed in a single calendar year (2016) across 24 Canadian centers. Variation of practice was recorded, as well as where a change in management would be projected and associated cost implications of that change based on molecular subtype assignment. Results: Data from 862 patients revealed wide variation in surgical staging, with lymph node dissection(LND) performed in 61% of ECs (range 25- 100%), including 38% LND in Gr1ECs (0- 100%). Adjuvant therapy (type, when/if given) and cancer surveillance (frequency, site e.g., community vs. cancer center) was inconsistent within and across centers for both early-and late-stage disease. Molecular classification identified 29% MMRd ECs (n=247) but only 8% of these women had been referred to HCP. 30 women who did consult HCP were MMRproficient. 38% of MMRd ECs had no LND and 43% did not receive radiation. 16% and 18% of p53abn ECs had no LND or omentectomy respectively, and only 58% received chemotherapy. De- escalation of treatment in early-stage POLEmut and NSMP ECs (n=63 treated, where molecular classification would direct observation or brachytherapy-only) would have reduced costs by $348,896-407,830CAD or $5538-6466CAD per patient. Conclusions: There is currently profound variation in practice for all aspects of EC management with implications to patients and health systems. Molecular classification can provide consistency in care and direct biologically-informed management.
7 IGCS20_1231 Oral Plenary Plenary II Sentinel lymph node biopsy versus lymphadenectomy for intermediate and high grade endometrial cancer staging (SENTOR trial): A prospective multicenter cohort study M. Cusimano1, D. Vicus2, K. Pulman3, M. Q. Bernardini4, G. Bouchard-Fortier4, S. Laframboise4, T. May4, L. Hogen4, A. Covens2, L.T. Gien2, R. Kupets2, M. Rouzbahman4, B.A. Clarke4, J. Mirkovic2, M. Cesari3, G. Turashvili5, M. Maganti4, A. Zia4, G.E.V. Ene4, S. Ferguson4 1 University of Toronto, Canada; 2Sunnybrook Health Sciences Centre, Canada; 3Trilium Health Partners, Canada; 4University Health Network, Canada; 5Sinai Health Systems, Canada Background: It is unclear whether sentinel lymph node biopsy (SLNB) can replace lymphadenectomy in women with high grade endometrial cancer (EC). We performed a prospective multicenter cohort study (the SENTOR trial) to evaluate the diagnostic accuracy of SLNB using indocyanine green in intermediate and high grade EC (NCT01886066). Methods: Patients with clinical stage I grade 2 endometrioid or high grade EC scheduled for minimally invasive hysterectomy at three academic centers in Toronto, Canada, were prospectively enrolled for SLNB followed by pelvic (PLND) and para-aortic lymphadenectomy (PALND) as the reference standard. The study was powered to determine sensitivity of the SLNB algorithm as the primary endpoint. Results: We enrolled 156 patients (126 high grade); all underwent SLNB and PLND, and 106 (84%) with high grade EC underwent PALND. Sentinel lymph node detection rates were 97% per patient (95% CI 94-99), 88% per hemipelvis (95% CI 83-91), and 78% bilaterally (95% CI 70-84). Of 27 patients (17%) with nodal metastases, 26 were correctly identified by the SLNB algorithm, yielding a sensitivity of 96% (95% CI 81-100), false negative rate of 4% (95% CI 0- 19), and negative predictive value of 99% (95% CI 96-100). Only one patient (0.6%) was misclassified by the SLNB algorithm. Two of 27 node-positive patients (7.5%) were identified outside traditional PLND boundaries, and five of 27 (18.5%) required immunohistochemistry for diagnosis. Conclusion: SLNB has comparable, if not superior, diagnostic accuracy relative to lymphadenectomy in high grade EC patients. SLNB is a viable option for the surgical staging of EC.
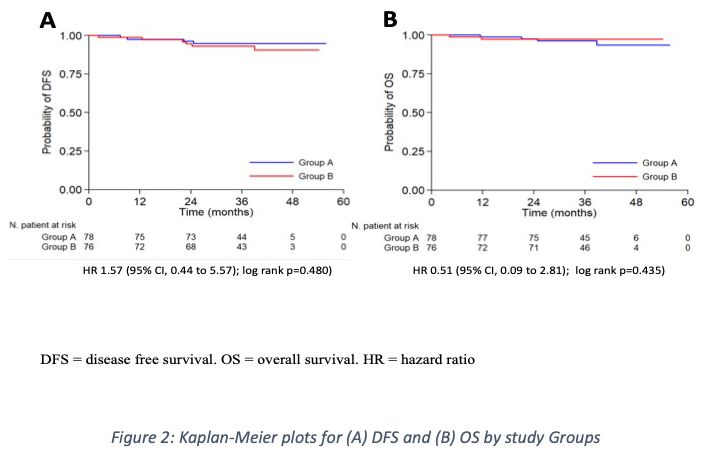
8 IGCS20_1246 Oral Plenary Plenary II A multicentric randomized trial to evaluate the ROle of uterine MANipulator on laparoscopic/robotic HYsterectomy for the treatment of low-risk endometrial cancer: the ROMANHY Trial (NCT:02762214) S. Gueli Alletti1, E. Perrone1, C. Fedele1, G. Vizzielli1, A. Fagotti1, V. Gallotta1, C. Rossitto1, B. Costantini1, S. Restaino1, G. Monterossi1, F. Fanfani1, G. Scambia1, S. Cianci2, V. Chiantera3, S. Uccella4, A. Ercoli5 1 Division of Gynecologic Oncology, Fondazione Policlinico Universitario A. Gemelli IRCCS, Italy; 2 Department of Woman, Child and General and Specialized Surgery, University of Campania “Luigi Vanvitelli”, Italy; 3Department of Gynecologic Oncology, ARNAS Civico Di Cristina Benfratelli, Università di Palermo, Italy; 4Department of Obstetrics and Gynecology, AOUI Verona, Università di Verona, Italy; 5Division of Obstetrics and Gynecology, Università degli studi di Messina, Policlinico G. Martino, Italy Background The role of the intrauterine manipulator in minimally invasive hysterectomy for endometrial cancer has been widely debated in terms of impact on the oncological outcomes. To date, definitive conclusions on the possible advantages and oncological safety of its use in endometrial cancer staging are still awaited. Objectives This randomized trial aimed to assess the role of the uterine manipulator in terms of oncological and perioperative outcomes in patients undergoing minimally invasive (laparoscopic/robotic) staging for presumed low-risk endometrial cancer. Study Design Enrolled patients were randomly allocated in two groups according to the use (Group A) or no use (Group B) of the uterine manipulator. The variables collected included baseline demographic characteristics, perioperative data, final pathology report, adjuvant treatment, and follow-up. Results 154 patients were randomly allocated in Group A (n=78) and Group B (n=76). A statistically significant difference was found in OT for the laparoscopic staging (p=0.005), while no differences were reported for the robotic procedures. The EBL was significantly lower in Group B (p=0.030). Only one conversion to laparotomy (1.3%) occurred in Group A. Comparable results were recorded in terms of peritoneal cytology, LVSI (p=0.584), and pattern of lymphovascular spread (p=0.790).
With a median follow-up of 38.7 months, no differences were detected in terms of OS and DFS, and in the number of recurrences. The uterine manipulator had no impact on DFS both at univariate and multivariable analysis. Conclusions The intrauterine manipulator does not affect the perioperative and oncological outcomes of presumed low-risk endometrial cancer patients undergoing laparoscopic/robotic staging.
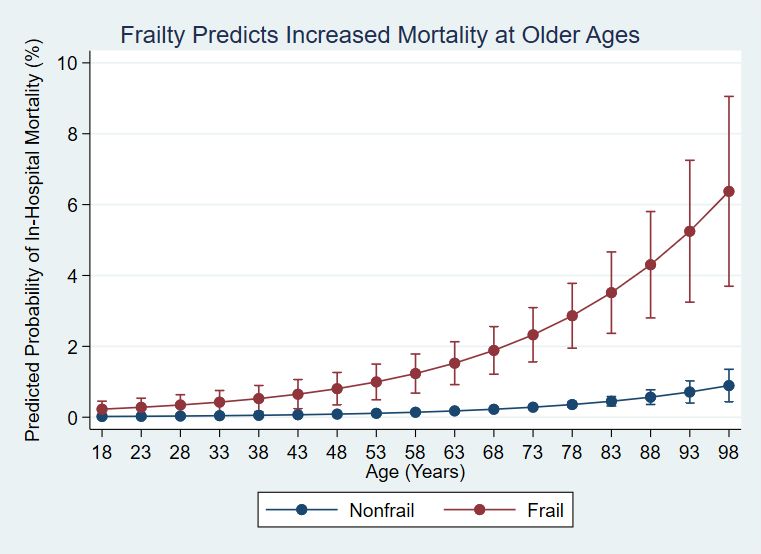
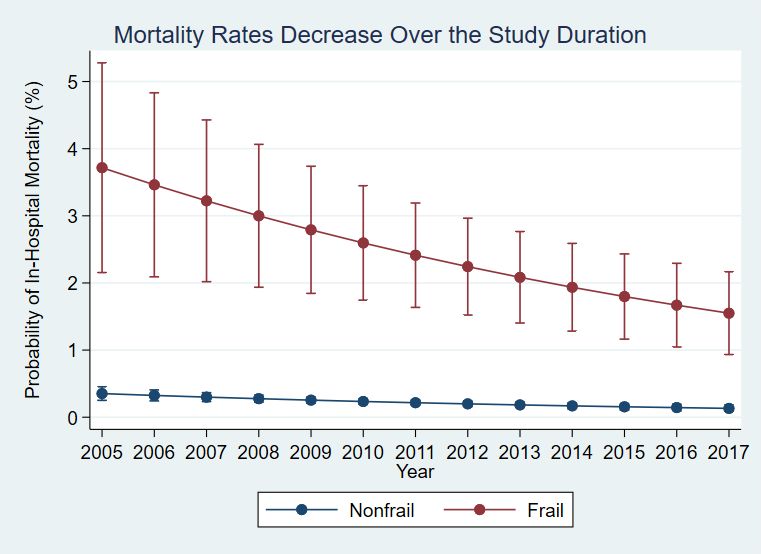
9 IGCS20_1423 Oral Plenary Plenary II Frailty is Independently Associated with Worse Outcomes and Increased Resource Use Following Procedures to Treat Endometrial Cancer M. Nakhla1, A. Mandelbaum2, R. Salani3, J. Cohen3, P. Benharash2 1 David Geffen School of Medicine at the University of California at Los Angeles, United States; 2 Cardiovascular Outcomes Research Laboratories (CORELAB), University of California Los Angeles, United States; 3Department of Obstetrics & Gynecology, David Geffen School of Medicine at UCLA, United States Introduction– Frailty has been associated with poorer surgical outcomes and is a critical factor in procedural risk assessment. The objective of this study is to validate surgical outcomes in patients undergoing surgery for endometrial cancer (EC). Methods– Patients undergoing inpatient gynecologic surgery for EC were identified using the 2005-2017 National Inpatient Sample database. The Johns Hopkins Adjusted Clinical Groups (ACG) frailty-defining diagnosis indicator was used to designate frailty. Multivariate regression models were used to assess the association of frailty with post-operative outcomes and resource use. Results–Of an estimated 339,846 patients, 2.9% (9,868) were considered frail. After adjusting for patient and hospital characteristics, frailty was associated with a four-fold increase in inpatient mortality (adjusted odds ratio [AOR]:4.1; p
10 IGCS20_1420 Oral Plenary Plenary III The learning curve of robot-assisted laparoscopy has impact on the oncological outcomes of early stage cervical cancer patients I. Baeten1, J. Hoogendam1, H. Schreuder1, I. Jürgenliemk-Schulz1, R. Verheijen1, R. Zweemer1, K. Gerestein1 1 University Medical Centre Utrecht, Netherlands Introduction: Previous learning curve studies are focused on short term surgical outcomes of robot-assisted surgery. We are the first to study the influence of learning curve on recurrence rate and quantify its impact on survival in patients with early stage cervical cancer using a validated analysis. Methods: We included all patients with early stage cervical cancer treated consecutively by one tertiary surgical team with robot-assisted laparoscopy (2007 - 2017). To establish the number of procedures needed to ascertain oncological proficiency, we performed a risk-adjusted cumulative sum (RA-CUSUM) analysis. The impact of the learning curve on oncological outcomes was quantified with Kaplan-Meier survival analysis. Results: In total, 165 patients received radical robot-assisted laparoscopy and had a median follow-up of 57 months (range 3-132 months). Multivariate RA-CUSUM analysis demonstrated a learning phase of 61 procedures. The recurrence rate decreased significantly with increasing experience in robot-assisted laparoscopy. No significant differences in baseline characteristics were observed between patients treated during the learning phase (n=61) and experienced phase (n=104). The 5-year disease-free, disease-specific and overall survival significantly increased in patients treated after the learning phase; 80.2% to 91.1% (P=0.040), 84.7% to 97.7% (P=0.002) and 84.7% to 94.8% (P=0.018), respectively. Conclusions/Implications: In this single institution study we found a learning phase for robot-assisted laparoscopy in cervical cancer of 61 procedures with significant impact on the survival rates. With our analysis we aim to encourage others performing robot-assisted radical surgery for cervical cancer to assess their own learning curves.
11 IGCS20_1039 Oral Plenary Plenary III Oncologic Outcomes and Role of Adjuvant Therapy in Endometrial Cancer Patients with Low Volume Metastasis in the Sentinel Lymph Nodes: An International Multi-Institutional Study. K. Ghoniem1, G. Dinoi2, A. Larish1, X. Zhou3, M. AlHilli4, S. Wallace5, C. Wohlmuth6, G. Baiocchi7, N. Tokgozoglu8, F. Raspagliesi9, A. Buda10, V. Zanagnolo11, I. Zapardiel12, N. Jagasia13, R. Giuntoli14, A. Glickman15, M. Peiretti16, M. Lanner17, E. Chacon18, J. Di Guilmi19, A. Pereira20, E. Faron21, A. Fishman22, C. Nitschmann23, S. Parker3, A. Joehlin-Price4, B. Lees5, A. Covens6, L. De Brot7, C. Taskiran8, G. Bogani9, C. Paniga10, F. Multinu11, A. Hernandez- Gutierrez12, A. L. Weaver24, M. E. McGree24 1 Department of Obstetrics and Gynecology, Mayo Clinic, United States; 2Universita Cattolica del Sacro Cuore, Italy; 3Hartford HealthCare, United States; 4Cleveland Clinic, United States; 5 University of Wisconsin School of Medicine and Public Health, United States; 6Sunnybrook Health Sciences, University of Toronto, Canada; 7A.C. Camargo Cancer Center, Brazil; 8Turkish Society of Gynecologic Oncology, Turkey; 9Fondazione IRCCS Istituto Nazionale Tumori -Milan, Italy; 10University of Milano-Bicocca, Italy; 11IEO, European Institute of Oncology IRCCS, Italy; 12 La Paz University Hospital-IdiPAZ, Spain; 13Mater Hospital Brisbane & Mater Research Institute, University of Queensland, Australia; 14University of Pennsylvania Health System, United States; 15Barcelona Clinic Hospital, Spain; 16University of Cagliari, Italy; 17Medical University of Graz, Austria; 18Clínica Universidad de NavarraClínica Universidad de Navarra, Spain; 19Hospital Britanico de Buenos Aires, Argentina; 20Hospital Universitario Puerta de Hierro-Majadahonda, Spain; 21Breast, gynecology and reconstructive Surgery Unit, Curie Institute, France; 22Meir Medical Center, Faculty of Medicine - Tel-Aviv University, Israel; 23 Lahey Clinic, United States; 24Department of Health Sciences Research, Mayo Clinic, United States Objective: To assess recurrence-free survival (RFS) and role of adjuvant therapy (ATx) in endometrial cancer with low volume metastasis (LVM) in sentinel lymph nodes (SLN). Methods: Patients with SLN LVM (≤2 mm) during 2010-2018 were retrospectively collected from 22 centers; stage IV, adnexal involvement, or unknown ATx were excluded. High-risk characteristics were grade (G) 3, non-endometrioid (NE) histology, lymphovascular invasion (LVSI), uterine serosal invasion (USI), or cervical stromal invasion. Results: 243 patients were included [131 isolated tumor cells (ITCs); 112 micro-metastasis (MM)]. The 186 patients who received ATx (external beam radiation therapy and/or chemotherapy) were
more likely to be high-risk (75.3% vs. 38.6%) or have MM (55.9% vs. 14.0%) compared to patients without ATx. RFS was 78.1% (95% CI, 70.5-86.5%) at 4 years; median follow-up of patients without recurrence was 29.6 (IQR, 19.1-41.5) months. The 4-yr RFS was 83.8% (95% CI 73.1-96.1%) among 57 patients without ATx; no significant risk factors identified. In particular, there were 18 G1 non-high-risk patients with ITC and no ATx, of which only 1 has recurred. G3, NE, LVSI, and USI were associated with recurrence in patients receiving ATx (Table). G3 or NE patients had poor outcome even with receiving ATx, the 4-yr RFS was 59.5% and 56.1%, respectively. Conclusion: In patients with SLN LVM who received ATx, G3, NE, LVSI, and USI were strong prognostic factors. ITCs patients with G1 and non-high-risk characteristics have good prognosis even without ATx; further analysis is needed, when this cohort matures, to know if ATx can be confidently spared.
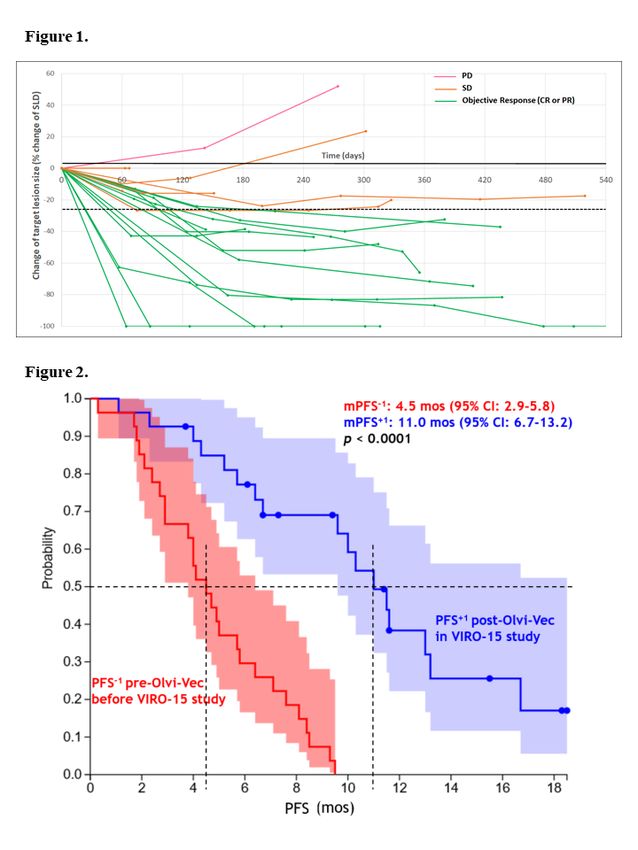
12 IGCS20_1308 Oral Plenary Plenary III Oncolytic Vaccinia (Olvi-Vec) Primed Immunochemotherapy in Platinum- Resistant/Refractory Ovarian Cancer R. Holloway1, A. Mendivil2, J. Kendrick1, L. Abaid2, J. Brown2, C. Fitzsimmons1, J. Kennard1, M. King2, J. LeBlanc1, K. Lopez2, M. Manyam1, N. McKenzie1, K. Mori2, A. Stephens1, S. Ahmad1 1 AdventHealth Cancer Institute, United States; 2Gynecologic Oncology Associates, United States Introduction: Intraperitoneal oncolytic vaccinia virus (Olvi-Vec) was administered to heavily pretreated patients with platinum-resistant/refractory ovarian cancer (PRROC) followed by intravenous carboplatin-doublet (CD) ± bevacizumab (Bev) in a Phase-2 trial (NCT02759588). Primary objectives: RECIST overall response rate (ORR) & progression-free survival (PFS). Methods: Patients with PRROC who progressed after most recent therapies received 2 days of Olvi-Vec followed by CD±Bev, then maintenance with single-agent therapies ± Bev. Pre-&post- virotherapy tumor biopsies were obtained for translational analyses. Results: 27 patients enrolled: median 4 prior regimens, 82% prior Bev, 52% platinum-refractory and 48% platinum-resistant. Mean cycles of CD±Bev were 6(±3). Median follow-up was 26.5 months. RECIST ORR was 54% (95%CI:33-74%): 2(8%) complete response, 11(46%) partial response; 8(33%) stable disease. Median duration of response was 7.6 months (95%CI:3.7- 9.6). Clinical benefit rate was 88%. Median PFS was 11.0 months (95%CI:6.7–13.0), and PFS- 6-month was 77%. CA-125 ORR was 85% (95%CI:65–96%). There were no Grade 4 adverse events with virotherapy. Performance status was preserved/improved in 24 (89%) patients while on CD±Bev. Post-virotherapy intra-tumoral infiltration of CD8+ T-cells and upregulation of STAT1 expression (p=0.008) were demonstrated. Conclusions: Despite PRROC, prior bevacizumab, and progression on last therapy, the majority of patients achieved RECIST response with median PFS exceeding their prior line of therapy. Virus-induced changes in the tumor microenvironment may explain the apparent clinical reversal of platinum resistance.
13 IGCS20_1440 Oral Plenary Plenary III Efficacy on Individualized Starting Dose (ISD) and Fixed Starting Dose (FSD) of Niraparib per Investigator-Assessment (IA) in Newly Diagnosed Advanced Ovarian Cancer (OC) W. Graybill1, M. Mirza2, A. González-Martin3, D. O'Malley4, L. Gaba5, O.W.S. Yap6, E. Guerra7, P.G Rose8, J. Baurain9, S. Ghamande10, H. Denys11, E. Prendergast12, C. Pisano13, P. Follana14, E.I. Braicu15, P.M. Calvert16, J. Korach17, Y. Li18, D. Gupta18, B.J. Monk19 1 Gynecologic Oncology Group (GOG) and Department of Gynecologic Oncology, Medical University of South Carolina, United States; 2Nordic Society of Gynaecological Oncology (NSGO) and Department of Oncology, Rigshospitalet, Copenhagen University Hospital, Denmark; 3Grupo Español de Investigación en Cáncer de Ovario (GEICO) and Medical Oncology Department, Clínica Universidad de Navarra, Spain; 4The Ohio State University – James CCC, United States; 5Hospital Clinic de Barcelona, Medical Oncology Department, Spain; 6University Gynecologic Oncology, United States; 7Hospital Universitario Ramón y Cajal, Spain; 8Cleveland Clinic, United States; 9Cliniques Universitaires Saint-Luc, Université Catholique de Louvain, Belgium; 10Georgia Cancer Center, Augusta University, United States; 11 Ghent University Hospital, Belgium; 12Minnesota Oncology, United States; 13Istituto Nazionale Tumori IRCCS Fondazione Pascale, Italy; 14GINECO and Centre Antoine Lacassagne, France; 15 Charité Medical University, Germany; 16Cancer Trials Ireland, Ireland; 17Department of Gynecologic Oncology, Chaim Sheba Medical Center, Israel; 18GlaxoSmithKline, United States; 19 Arizona Oncology (US Oncology Network), University of Arizona College of Medicine, United States Introduction: Niraparib is a poly(ADP-ribose) polymerase inhibitor approved for maintenance treatment of patients with newly diagnosed or recurrent OC that responded to platinum-based chemotherapy and treatment in heavily-pretreated recurrent OC. Here we report efficacy in patients receiving the FSD and ISD in the PRIMA/ENGOT-OV26/GOG-3012 trial (NCT02655016). Methods: This double-blind, placebo-controlled, phase 3 study randomized 733 patients to receive niraparib or placebo for 36 months or until disease progression/toxicity. A protocol amendment introduced ISD: 200 mg in patients with body weight
Conclusions: The 200- or 300-mg ISD by baseline body weight and platelet counts demonstrated comparable efficacy while improving the safety profile of niraparib. Use of this regimen for first-line maintenance of advanced OC patients is approved by the US FDA. Funded by: GlaxoSmithKline NCT: NCT02655016
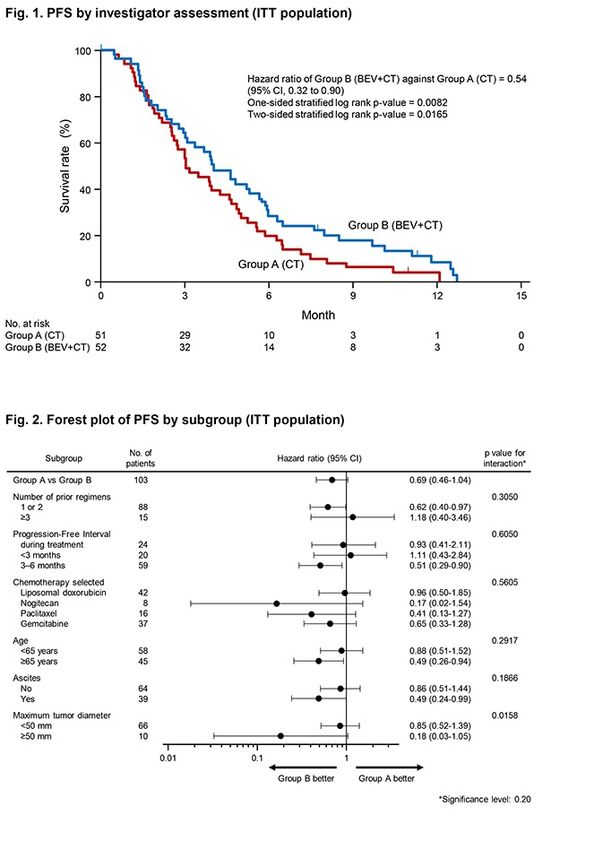
14 IGCS20_1271 Oral Plenary Plenary V Phase II trial evaluating efficacy and safety of standard of care with or without bevacizumab in platinum-resistant epithelial ovarian, fallopian tube, or primary peritoneal cancer N. Nishikawa1, T. Shoji2, T. Enomoto1, M. Abe3, A. Okamoto4, T. Saito5, T. Oishi6, S. Nagase7, M. Mori8, Y. Inokuchi9, S.K. Kamiura10, T. Sugiyama11 1 Niigata University, Japan; 2Iwate Medical University School of Medicine, Japan; 3Shizuoka Cancer Center, Japan; 4The Jikei University School of Medicine, Japan; 5Hachinohe Red Cross Hospital, Japan; 6Tottori University School of Medicine, Japan; 7Yamagata University, Japan; 8 Aichi Cancer Center Hospital, Japan; 9Kitasato University Hospital, Japan; 10Osaka International Cancer Institute, Japan; 11St. Mary's Hospital, Japan Introduction: There are no ongoing clinical trials investigating bevacizumab efficacy beyond disease progression in platinum-resistant recurrent ovarian cancer; however, improving outcomes in these patients is a critical unmet need. Methods: This open-label, randomized phase II trial (JGOG3023; UMIN000017247) enrolled patients aged ≥20 years with histologically confirmed epithelial ovarian, fallopian tube, or primary peritoneal carcinoma with platinum-resistant disease (progression occurring ≤6 months from completing ≥3 platinum cycles, including bevacizumab). Patients were randomized 1:1 to single-agent chemotherapy (group A) or single-agent chemotherapy combined with bevacizumab (group B). The primary endpoint was investigator-assessed PFS. Secondary endpoints included OS, ORR, and safety. Results: Patient characteristics were balanced between group A (n=51) and group B (n=52). Median PFS was longer in group B versus group A (4.0 [95% CI: 3.0–5.7] vs 3.1 [2.5–4.6] months; HR, 0.54 [0.32–0.90]; one-sided p=0.0082) (Fig.1). Maximum tumor diameter and ascites were significantly associated with greater prolongation in PFS in group B (Fig.2). Median OS was numerically longer in group B versus group A (15.3 vs 11.3 months; HR, 0.67 [0.38– 1.17]; two-sided p=0.1556). ORR was 13.7% and 25.0% in group A and B, respectively. The safety profile was similar across both groups (Table 1). Conclusion: These results suggest chemotherapy combined with bevacizumab has efficacy beyond disease progression. A phase III trial is warranted to confirm our findings.
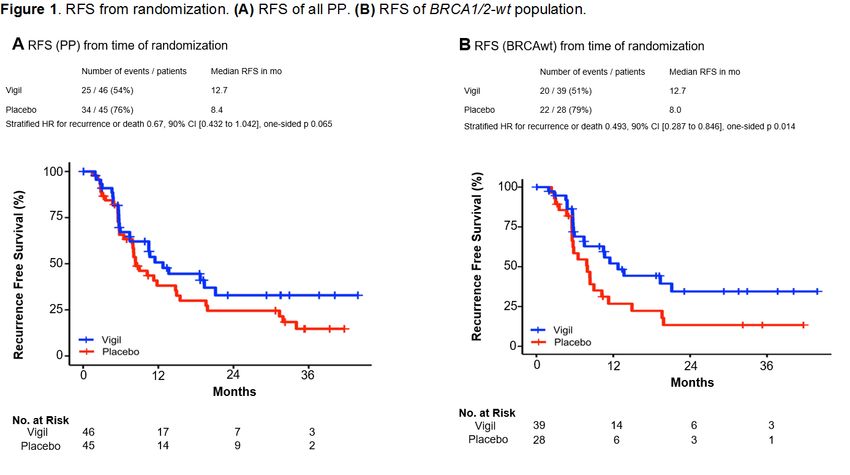
15 IGCS20_1306 Oral Plenary Plenary V Randomized Double-Blind Placebo Controlled Trial of Frontline Maintenance Vigil Immunotherapy (VITAL study) in Stage III/IV Ovarian Cancer: Efficacy Assessment in BRCA1/2-wt Patients R. Rocconi1, E. Grosen2, S. Ghamande3, J. Chan4, M. Barve5, J. Oh6, D. Tewari7, P. Morris8, E. Stevens9, J. Bottsford-Miller9, M. Tang10, P. Aaron11, G. Wallraven11, E. Bognar11, L. Manning11, J. Nemunaitis11, B. Slomovitz12, T. Herzog13, B. Monk14, R. Coleman15 1 University of South Alabama - Mitchell Cancer Institute, United States; 2Cancer Care Northwest, United States; 3Georgia Regents University, United States; 4California Pacific Medical Center Research Institute, United States; 5Mary Crowley Cancer Research Centers, United States; 6Texas Oncology, United States; 7Kaiser Permanente, United States; 8Nebraska Methodist Hospital, United States; 9Billings Clinic, United States; 10StatBeyond Consulting, LLC., United States; 11Gradalis, Inc., United States; 12University of Miami – Sylvester Comprehensive Cancer Center, United States; 13University of Cincinnati Cancer Institute, United States; 14 Arizona Oncology, United States; 15MD Anderson Cancer Center, United States Introduction: Vigil is an autologous tumor cell vaccine constructed from tumor tissue transfected with a DNA plasmid encoding GMCSF and bi-shRNA-furin thereby reducing TGFβ expression. Methods: A randomized double-blind placebo-controlled trial of Vigil was performed in advanced stage frontline (1L) Ovarian Cancer (OC) patients. Relapse-free survival (RFS), overall survival (OS), and safety were endpoints. Patients were randomized [1:1 to placebo (control group, CG) or Vigil (Vigil group, VG), 1 x 10e7 cells/dose for up to 12 doses] after complete response to 1L surgery and chemotherapy. Results: 91 patients were randomized in the per-protocol population (PP), (VG: n=46; CG: n=45). VG demonstrated no Grade 3 or 4 toxicity. From time of randomization median RFS (mRFS) for all 91 patients was favorable in the VG (HR 0.67, one-sided p 0.065). All 91 patients were tested for BRCA1/2 status. An advantage in mRFS was seen in the BRCA1/2-wt patients in VG (12.7 mo) compared to CG (8 mo), (HR 0.493, 90% CI [0.287 to 0.846], one-sided p 0.014) from time of randomization as well as OS benefit in VG (median not reached) vs. CG (41.4 mo) (HR of 0.417, 90% CI [0.202 to 0.86], p 0.02). 51% BRCA1/2-wt Vigil treated patients relapsed compared to 79% of placebo (median follow-up of 38.6 mo for PP). Homologous recombination deficiency status (HRD) and further determination of predictive biomarkers of response are underway. Conclusion: Vigil immunotherapy as 1L maintenance in Stage III/IV ovarian cancer is well tolerated and showed significant RFS clinical benefit, particularly in BRCA1/2-wt disease.
16 IGCS20_1101 Oral Plenary Plenary V Quality-adjusted (QA) progression-free survival analyses of veliparib + carboplatin/paclitaxel (CP) vs CP alone in patients with newly diagnosed ovarian cancer A. Alvarez Secord1, M. Bookman2, R. Coleman3, M. Dinh4, N. Khandelwal4, K. Benjamin4, R. Kamalakar4, D. Sullivan4, D. Cella5 1 Department of Obstetrics and Gynecology, Duke University School of Medicine, Duke Cancer Institute , United States; 2Department of Medicine, University of Arizona Health Sciences, , United States; 3Department of Gynecologic Oncology and Reproductive Medicine, Division of Surgery, MD Anderson Cancer Center; , United States; 4Abbvie Inc, United States; 5Department of Medical Social Sciences, Northwestern University, United States Objective: Veliparib, a poly (ADP-ribose) polymerase inhibitor, was evaluated in a Phase 3 trial (VELIA, NCT02470585) among patients with newly diagnosed stage III/IV high-grade serous epithelial ovarian/fallopian tube/primary peritoneal cancer. VELIA examined veliparib added to CP followed by veliparib maintenance compared to placebo added to CP followed by placebo maintenance. This analysis compared QA progression-free survival among patients enrolled in VELIA. Methods: Patient-centered outcomes were assessed in 344 Veliparib+ CP and 351 CP alone subjects. Progression-free survival (PFS) time was partitioned into two health states: time with toxicity (Tox) and time without Tox. Tox included three clinically meaningful adverse events (AEs) including nausea, vomiting and fatigue. QA-PFS was assessed for duration of good quality of life, incorporating PFS and health states. Q-TWiST (QA time without disease symptoms or treatment Tox) was calculated as utility-weighted sums of mean health state durations. Sensitivity analyses were conducted utilizing Grade 2+ or Grade 3+ AEs. Similar analyses were conducted on HRD and BRCA-deficient subgroups. Results: A significant difference in mean QA-PFS was seen in favor of Vel throughout compared to CP alone (19.5 months vs 16.5 months; 95% CI 1.42, 4.61; p
17 IGCS20_1131 Oral Plenary Plenary V Safety and patient-reported outcomes in patients receiving niraparib in the PRIMA/ENGOT-OV26/GOG-3012 trial G. Freyer1, B. Pothuri2, S. Han3, D. Chase4, B. Monk4, F. Heitz5, R. Burger6, L. Gaba7, L. Van Le8, E. Guerra9, D. Bender10, J. Korach11, N. Cloven12, C. Churruca13, P. Follana14, P. DiSilvestro15, J.F. Baurain16, K. Jardon17, C. Pisano18, U. Peen19, J. Maenpaa20, P. Hoskins21, E. Bacque22, Y. Li22, L. Eliason22, A. González-Martín23 1 Groupe d’Investigateurs Nationaux pour l’Etude des Cancers Ovariens and Service d’Oncologie Médicale, Centre Hospitalier Lyon-Sud, France; 2Gynecologic Oncology Group (GOG) and the Department of Obstetrics/Gynecology, Perlmutter Cancer Center, NYU Langone Health, United States; 3Department of Obstetrics and Gynecology, University Hospitals Leuven, Belgium; 4Arizona Oncology (US Oncology Network), University of Arizona College of Medicine, United States; 5Department for Gynecology and Gynecologic Oncology, Kliniken Essen-Mitte, Germany; 6University of Pennsylvania , United States; 7Medical Oncology Department, Hospital Clinic de Barcelona, Spain; 8Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, University of North Carolina at Chapel Hill, United States; 9Medical Oncology Department, Breast and Gynecological Cancer Unit, Hospital Ramon y Cajal, United States; 10 Department of Obstetrics and Gynecology, University of Iowa, United States; 11Department of Gynecologic Oncology, Chaim Sheba Medical Center, Israel; 12Texas Oncology, United States; 13 Hospital Universitario Donostia, Spain; 14GINECO and Centre Antoine Lacassagne, France; 15 Department of Obstetrics and Gynecology, Women and Infants Hospital/Alpert School of Medicine at Brown University, United States; 16Université Catholique de Louvain and Cliniques Universitaires Saint-Luc, Belgium; 17Department of Obstetrics and Gynecology, McGill University, Canada; 18Department of Urology and Gynecology, Istituto Nazionale Tumori IRCCS Fondazione G. Pascale, Italy; 19Herlev University Hospital, Denmark; 20Tampere University Central Hospital, Finland; 21British Columbia Cancer Agency, Vancouver Centre, Medical Oncology, Canada; 22GlaxoSmithKline, United States Introduction: Niraparib is a poly(ADP-ribose) polymerase inhibitor approved for treatment in heavily pretreated patients and maintenance of patients with newly diagnosed or recurrent ovarian cancer following a response to platinum-based chemotherapy. Here we report safety and patient-reported outcomes (PROs) in the overall population and subgroups from PRIMA/ENGOT-OV26/GOG-3012 (NCT02655016). Methods: This double-blind, placebo-controlled, phase 3 study randomized 733 patients. Patients received a 300-mg QD fixed starting dose (FSD) of niraparib or placebo for 36 months or until progression/toxicity. A protocol amendment introduced an individualized starting dose (ISD): 200 mg in patients with body weight
5D-5L, EORTC-QLQ-C30, and EORTC-QLQ-OV28) were collected Q8W for 56 weeks, then Q12W while a patient received treatment. Results: In the overall population, the most common grade ≥3 treatment-emergent adverse events (TEAEs) were hematologic (Table). In patients receiving ISD, these TEAEs decreased. No treatment-related deaths occurred. PRO analysis showed no difference in niraparib-treated patients versus placebo in the overall population or in the homologous recombination deficient, homologous recombination proficient, FSD, and ISD subgroups. Conclusions: ISD incorporation improved the safety profile of niraparib without compromising efficacy. Niraparib was well tolerated, with similar PRO scores across the treatment period. Hematologic toxicities were manageable through implementation of dose interruptions and reductions. Funding: GlaxoSmithKline NCT: NCT02655016
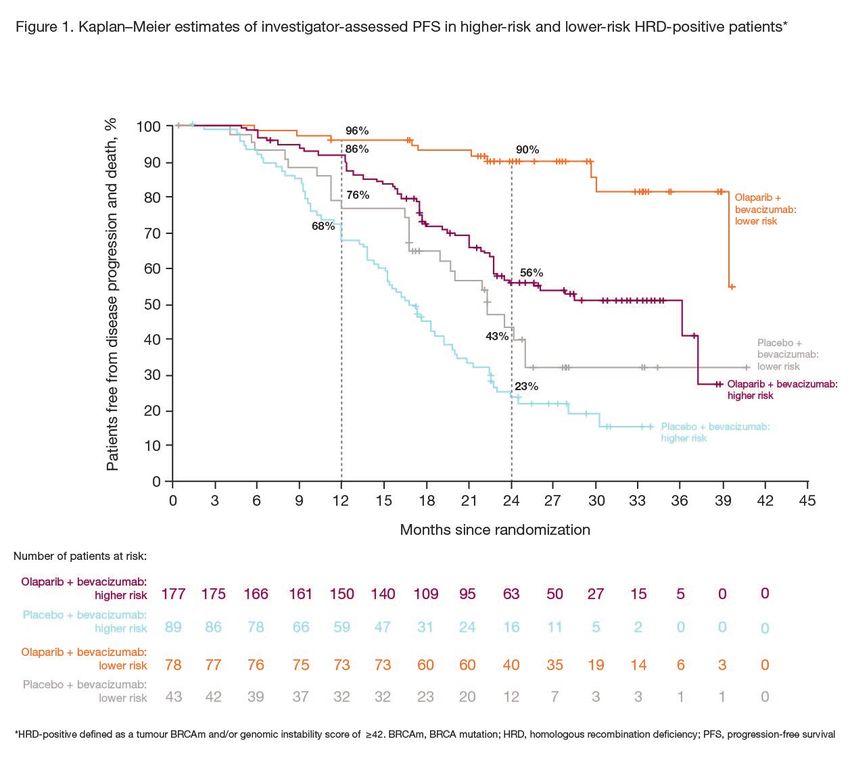
18 IGCS20_1207 Oral Plenary Plenary V Efficacy of maintenance olaparib plus bevacizumab by biomarker status in clinical higher- and lower-risk patients with newly diagnosed, advanced ovarian cancer in the PAOLA-1 trial P. Harter1, D. Petran2, G. Scambia3, E. Ortega4, I. Tsibulak5, S. Nagao6, I. Vergote7, J. Meunier8, F. Priou9, R. Sverdlin10, T. Milenkova12, I. Ray-Coquard13, I. Ray-Coquard13 1 Kliniken Essen Mitte, and AGO, Germany; 2Centre Hospitalier Mont de Marsan, and GINECO, France; 3Fondazione Policlinico Universitario A. Gemelli IRCCS Università Cattolica, and MITO, Italy; 4Hospital Universitari Arnau de Vilanova , Spain; 5Medical University of Innsbruck, and AGO-Austria, Austria; 6Hyogo Cancer Center, and GOTIC, Japan; 7University Hospital Leuven, Leuven Cancer Institute, and BGOG, Belgium; 8Centre Hospitalier Régional d'Orléans, and GINECO, France; 9Centre Hospitalier Départemental Les Oudairies, and GINECO, France; 10 GH Saint Joseph, and GINECO, France ; 12Centre Paul Strauss, and GINECO, France; 13 AstraZeneca, United Kingdom Introduction: In the Phase III PAOLA-1/ENGOT-ov25 trial (NCT02477644), adding maintenance olaparib to bevacizumab improved progression-free survival (PFS) in patients with advanced ovarian cancer in response after first-line platinum-based chemotherapy plus bevacizumab (HR 0.59; 95% CI 0.49–0.72) (Ray-Coquard et al. NEJM 2019). Outcomes in patients classified by clinical risk according to biomarker status are unknown. Methods: Patients were classified as higher-risk (stage III patients with upfront surgery and residual disease or who received neoadjuvant chemotherapy, or stage IV patients) or lower-risk (stage III patients with upfront surgery and no residual disease). This exploratory analysis evaluated PFS in higher-risk and lower-risk patients, including by biomarker status: homologous recombination deficiency (HRD)-positive, HRD-negative/unknown and tumour BRCA mutation (BRCAm)-positive. Results: Of 806 randomized patients, 74% were higher risk and 26% were lower risk, with median follow-up of 22.4 and 23.8 months, respectively. PFS significantly favoured olaparib plus bevacizumab versus placebo plus bevacizumab in higher-risk and lower-risk patients. In both higher- and lower-risk patients, the greatest PFS benefit was seen with olaparib plus bevacizumab versus bevacizumab alone in the HRD-positive subgroup (Figures 1 and 2) and the subgroup with a tumour BRCAm (Figure 2). Outcomes in the higher- and lower-risk HRD- negative/unknown subgroups are shown in Figure 2. Conclusions: In PAOLA-1, maintenance olaparib plus bevacizumab provided a substantial PFS benefit over bevacizumab alone in higher-risk and lower-risk patients, especially in the HRD- positive and BRCAm populations.
You can also read