Carnegie Virtual Healthcare Seminar 2021 Company Presentation - 12th March 2021 Richard S. Godfrey CEO Oslo Børs: BGBIO - BerGenBio
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Carnegie Virtual Healthcare Seminar 2021
Company Presentation
12th March 2021
Richard S. Godfrey CEO
1 Oslo Børs: BGBIO
BerGenBio – Investment highlights
Pioneering TWO first in Diversified Biomarkers Near term Well resourced
biology class selective Clinical and CDX clinical organisation
AXL inhibitors Pipeline milestones
Proprietary Experienced
World leaders in biomarkers and
understanding AXL Bemcentinib - oral COVID-19 Oxford based R&D
once-a-day AML CLIA lab validated team
biology, as a clinical trial use AML – mOS
mediator of capsule MDS Industry
ready MDS – mOS
aggressive cancer, NSCLC Development
Companion NSCLC partnership and
fibrosis and viral Tilvestamab – Multiple ISTs Diagnostic assays
infections humanised collaborations
functionally Covid-19
blocking mAb
AML – Acute Myeloid Leukaemia
MDS – Myelodysplastic Syndrome
NSCLC – Non-Small Cell Lung Cancer
IST – Investigator Sponsored Trial
2
Leadership Team
Richard Godfrey, MPharmS, MBA Rune Skeie
Chief Executive Officer Chief Financial Officer
Professor Hani Gabra, MD, PhD, FRCPE, FRCP Alison Messon, PhD
Chief Medical Officer Director of Clinical Operations
Nigel McCracken, MSc, PhD, James Barnes, PhD
Chief Scientific Officer Director of Operations
3
Recent Value Driving Achievements
Check point
Relapse AML and Explore Bemcentinib Advance Tilvestamab
combination in
MDS in COVID-19 clinical development
2L NSCLC
Defining a new, emerging and Survival benefit reported in Completed Phase 1a safety
Started an international
substantial relapse patient chemo & CPI refractory study
clinical development
population, with no approved patients - Do DLTs
program for treatment of
treatment option - Dose proportional PK
COVID-19
cAXL proprietary biomarker - 2 randomized phase 2
Encouraging interim POC and CDx development Initiated Phase Ib
studies underway in UK,
survival data from Phase 2 - PK-PD safety study
South Africa& India
studies Translational research - Serial biopsies
- AML support clinical data - Refractory OC
Supportive mechanistic and
- Bem + LDAC
preclinical research
- HR-MDS
- Bem mono
- Biomarker correlation
4
Introduction to bemcentinib 5
Bemcentinib, a first-in-class, potent, oral, highly selective AXL inhibitor
ü Clinical development stage; Phase 2
in oncology indications (haem, solid
tumour) and COVID-19
ü Safety and tolerability profile supports
use in combination with other drugs
ü MOA is synergistic with other
therapies, enhancing response
ü 14 Nanomolar in vitro
potency
ü Size-0 100mg HPMC
capsules ü Favourable safety and tolerability
ü Uniquely selective for AXL, profile in over 400 patients studied
50 to 100-fold over other
ü 30 Months shelf-life
TAM kinases (Tyro3 and Mer)
confirmed
ü Once daily oral dosing
6 CONFIDENTIAL INFORMATION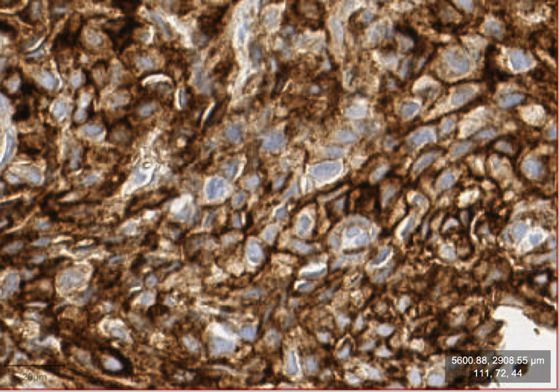
Pipeline of sponsored clinical trials
Targeted
Candidate Preclinical Phase I Phase II Registrational
Indication
Bemcentinib >2L AML & MDS
monotherapy
Bemcentinib
combination with
2L AML
LDAC
2L NSCLC
chemo refractory
Bemcentinib Expansion 16 pts.
combination with 2L NSCLC
Pembrolizumab CPI refractory
2L NSCLC
CPI+chemo refractory
Bemcentinib Hospital COVID-19
monotherapy patients
Tilvestamab Phase I
(BGB149)
7 Ongoing Trial Completed Trial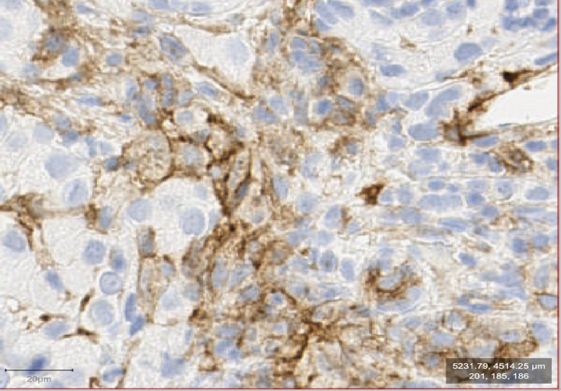
Pipeline of Investigator Sponsored Trials (ISTs)
Targeted
Candidate Phase I Phase II Registrational Sponsor
Indication
Uni. Hospital
COVID-19 Monotherapy Southampton/UKRI funded
European MDS
2L AML Monotherapy Cooperative Group
2L MDS European MDS
Monotherapy Cooperative Group
Sidney Kimmel
Recurrent
Monotherapy Comprehensive Cancer
Glioblastoma
Bemcentinib Expansion 16 pts.
Center at Johns Hopkins
Relapse University of Leicester
Mesothelioma + pembrolizumab
1L Metastatic
Haukeland University
Melanoma + pembrolizumab or +Dabrafenib/Trametinib Hospital
2-4L Stage 4
UT Southwestern Medical
NSCLC + docetaxel Center
1L metastatic or
recurrent PDAC + Nab-paclitaxel +Gemcitabine UT Southwestern Medical
+Cisplatin Center
8 Ongoing Trial Completed Trial
Bemcentinib is most advanced and broadly developed selective AXL inhibitor
Competitor Landscape Modes of AXL inhibition
Small
Selective
molecule
bemcentinib
Biologic
Anti-AXL MAB tilvestamab
Non-selective
Biologic
AVB-S6-500
(decoy receptor))
Small
molecule
preclinical Phase I Phase II Phase III Approved
Benefits of selective AXL inhibitors
No On-target toxicity No Off-target toxicity
Combination with other Patient selection based on
drugs AXL expression (CDx)
9
AXL and reprogramming of the tumour microenvironment 10
AXL is up regulated in hostile cellular micro environments
Very low expression under healthy physiological conditions
AXL signaling mediates aggressive disease Bemcentinib & Tilvestamab selective AXL inhibitors
Cancer Elevated AXL signaling strongly GAS6 GAS6
associated with cancer progression,
• Immune evasive
• Drug resistant immune evasion, drug resistance and tilvestamab
• Metastatic metastasis
Fibrosis
• Renal
Axl regulates cellular plasticity implicated in fibrotic
• NASH pathologies e.g. EMT, EndMT, Macrophage AXL AXL
• IPF polarity
• MF
• COPD
Viral bemcentinib
infection AXL mediates viral entry to cells and
• SARS-CoV-2 dampening of viral immune response Invasion
• Ebola Proliferation
• Zika Immune Migration
suppression
Survival EMT
11AXL is an independent negative prognostic factor in many cancers
Strong AXL expression correlates with poor survival rate Broad evidence of AXL linked with poor prognosis5
Breast carcinoma1 Lung adenocarcinoma (NSCLC)2
Weak AXL (90/6)
Astrocytic brain tumours Melanoma
1 100
AXL IHC low (n=59)
Breast cancer Mesothelioma
Probability of survival
Probability of survival
0.8 80
Gallbladder cancer NSCLC
0.6 60 GI Pancreatic cancer
Strong AXL (64/11) AXL IHC high (n=29)
0.4 40 • Colon cancer Sarcomas
• Oesophageal cancer • Ewing Sarcoma
0.2 AXL expression
20
Log Rank Test, P=0.035 P median
P=0.02
• CML
0 0
0 4 8 12 0 50 100 150
Time after diagnosis (years) Time (months)
12
1 Gjerdrum, 2010; 2 Ishikawa, 2012; 3 Ben-Battala, 2013; 4 Song, 2010, 5 supported by > 100 publicationsAXL is a key survival mechanism ‘hijacked’ by aggressive cancers
and drives drug resistance, immune-suppression & metastasis
very low expression under healthy physiological overexpressed in response to hypoxia, overexpression correlates with worse prognosis
conditions inflammation, cellular stress & drug treatment in most cancers
M2 M2
NK tumour NK tumour
cell cell
DC DC
AXL increases on immune cells AXL increases on the tumour cell
and suppresses the innate immune response and causes cancer escape and survival
• AXL is a unique type I interferon (IFN)
• M1 to M2 macrophage polarisation response checkpoint
• Decreased antigen presentation by DCs • Acquired drug resistance
• Prevent CD8+ T cell mediated cell death • Immune cell death resistant
• Activates Treg cells • Metastasis
13
DC- dendritic cells Treg – Regulatory T CellCompanion Diagnostic Assay Composite AXL score (cAXL) – CLIA Validated Clinical Use Assay simultaneously computes the presence of AXL on membranes of tumor & immune cells Example of high AXL expression on tumour cells: cAXL Example of tumour with a high number of AXL positive status of this patient is positive immune cells: cAXL status of this patient is positive • Arrows directed at examples of positively-stained tumour and immune cell, respectively • Both patients experienced significant tumour shrinkage on bemcentinib + pembrolizumab treatment combination 14
AXL is targeted by enveloped viruses to enter cells and dampen the
viral immune response
Apoptotic mimicry Type I interferon response
Enveloped viruses display Viral-mediated AXL receptor
phosphatidylserine that is activation dampens type I
recognized by GAS6, the AXL interferon responses, a key
receptor ligand, that mediates anti-viral defence mechanism
viral entry through “apoptotic for all cells
mimicry”.
bemcentinib blocks
AXL-dependent viral
entry and enhances anti-
viral interferon response
Bemcentinib potently
inhibits SARS-CoV-2
infection of cells.1
15
1 Maury IOWA unpublished / Meertens L et al. Cell Host & Microbe 2012, 12:544 / Chen J et al. Nat Microbiol 2018 3:302BerGenBio R&D Day with prominent independent expert KOL’s
Professor Wendy Maury, PhD Cory M.Hogaboam, PhD
Department of Microbiology and Immunology, University of Iowa, Iowa, USA Professor of Medicine, Department of Medicine, Cedars-Sinai Medical
Center, Los Angeles, USA
A novel approach for controlling SARS-Cov-2 infection: Bemcentinib
inhibition of AXL signaling The Role of AXL in Fribrosis
• Utilization of AXL contributes to ACE2-dependent entry • Gas6, AXL and pAXL are increased in severe IPF
• AXL enhances virus infection by failitating virus entry via an • Tergeting AXL with bemcentinib abolishes synthetic and
endosmal pathway functional properties of primary IPF fibroblasts in vitro
assays
• Bemcentinib control of virus infection likely involves both
reduced viral entry and enhanced interferon responses • Targeting AXL ameliorates fibrotic responses in an in vivo
model of IPF
Dr. Matthew Krebs, ChB, FRCP, PhD Professor Sonja Loges, MD, PhD
Clinical Senior Lecturer in Experimental Cancer Medicine, The University of Director, Department of Personalised Oncology, University Hospital Mannheim
Manchester & Consultant in Medical Oncology, The Christie NHS Foundation and Division of Personalised Medical Oncology, German Cancer Research
Trust, Manchester, UK Center – DKFZ, Germany
Targeting AXL with Bemcentinib in Lung Cancer AXL by Bemcentinib – a novel opportunity to treat AML and MDS
• AXL expression highly prevalent in mesothelioma • Bemcentinib inhibits AML/MDS cell survival and enhances
• Bemcentinib reverses EMT, repolarizes TAMs and anti-leukemic immunity
potentiates efficacy of immunotherapy in murine cancer • Bemcentinib mode of action is most like most blockade of
models immune suppression.
• cAXL selects for 2L immunotherapy relapse NSCLC patients • LDAC + Bemcentinib is well tolerated and effective in
that benefit from bemcentinib + prembrolizumab combination unfit/elderly AML patients
All presentations
16 and Q&A sessions available on our website: www.bergenbio.comBemcentinib development Acute Myeloid Leukaemia
ØFDA granted Orphan status in AML
ØFDA granted Fast Track Designation in AML
ØDefining a new patient population: relapsed AML and MDS
ØPatients having failed HMA +/- BCL2, FLT3 or IDH inhibitors
ØEncouraging 1L data / opportunities
17Acute Myeloid Leukaemia (AML)
Most common type of acute leukaemia in adults1
AML is a rare aggressive cancer of the blood and bone marrow
characterised by difficult to treat malignancies
AML
25% 70%
Patients unfit
~ 20,000 new cases diagnosed and >10,000 deaths in the US in 20182 for intensive
LEUKAEMIA therapy
350,000 pts globally
AML makes up 32% of all adult leukaemia cases
Occurs in a predominantly elderly, frail patient population;
68% of patients diagnosed with AML were aged >60 years 6
AML Market 3,4,5
2019 2027
$1.46bn $3.56 billion
13%
5-year survival rates of 3-8% in patients over 60 years old 7 annual growth rate
(1) Cancer.gov; (2) SEER; (3) https://www.who.int/selection_medicines/committees/expert/20/applications/AML_APL.pdf?ua=1ble
(4) https://www.cancer.net/cancer-types/leukemia-acute-myeloid-aml/statistics (5) https://www.businesswire.com/news/home/20190319005442/en/ (6)
18
http://asheducationbook.hematologylibrary.org/content/2010/1/62.long, (7) https://www.ncbi.nlm.nih.gov/books/NBK65996/ (8) VIALE A & CBemcentinib inhibits AML/MDS cell survival and enhances anti-
leukemic immunity
AXL is associated with therapy Immunosuppressive niches in the A paracrine axis between AML cells
resistance and poor overall bone marrow show enhanced AXL and the BM stroma establishes an
survival in AML patients. on AML, MDS progenitor and immune and therapy- protective tumor
myeloid cells cell niche
AML cell
Proliferation
cytokines
Survival
(GM-CSF, IL-10)
Drug resistance
Overall survival (%)
!Axl
AXL+
Bone marrow stem
cell niche t !Gas6
time after diagnosis (years) Stromal cells
Source: Loges, 2015; Ben-Battala, 2011
19Relapse AML – the need for new treatment options
• 1L treatment has evolved to include
venetoclax in combination with HMA or low-
dose cytarabine
• CR 37% rate and mOS of 14.7mo.1
• Relapse patients mOS 4.7mo2.
1. VIALE-A NCT02993523
20 2. 2 Leukemia Research
Volume 90, March 2020, 106314Phase Ib/II study of bemcentinib administered as
single agent or in combination with LDAC or
decitabine in patients with AML; or as a single
agent in patients with MDS
21BGBC003
Phase I/II study in elderly AML patients unfit for intensive chemo and transplant
Established safety and recommended Phase 2 dose in this
Phase 1 n=36 population, and biomarker correlation
Single agent bemcentinib dose-finding in
relapsed AML/MDS Recommended Phase 2 dose of bemcentinib in AML or
MDS is 400/200 mg as single agent OR in combination.
Phase 2 Expansion Cohorts
Cohort B2 n=16
Combination with LDAC in Cohort B3 n=14
Cohort B1 n=14 newly diagnosed or Combination with Cohort B4 n=14
Monotherapy AML relapsed AML decitabine in ND or Monotherapy MDS
relapsed AML
Cohort B5 expansion
Combination with LDAC
relapsed AML (ongoing)
LDAC = Low Dose Cytarabine
22
AML = Acute Myeloid Leukaemia
MDS = Myelodysplastic syndromesStrong durable responses observed in 1L AML patients
(bemcentinib + LDAC)
Part B2, n=7 06 Jan 2021
Disease Cytogenetic
Pt ID Age
type risk
203301 83 S A
101302 76 S I
• 70% CBR (5/7)
202301 79 P I • 42% CR/Cri
• 18months mTime-on-Treatment
202302 77 S A
• mOS immature
202304 75 S I
Ø Encouraging cf. SoC!
Ongoing Responder
SD (unchanged disease for at least 3 cycles)
1st CR/CRi reported No benefit (PD or has not completed 3 cycles)
402301 79 P A
1st PR reported
401301 78 P F
0,0 5,0 10,0 15,0 20,0 25,0 30,0 35,0
Months
P – de novo/primary disease
S – secondary disease
A – adverse cytogenetic risk
I – intermediate cytogenetic risk
F – favorable cytogenetic risk
23Encouraging Patient benefit observed in relapsed AML
(bemcentinib +LDAC)
(Part B2+B5 - Recruitment is ongoing)
Disease Cytogenet
Age
Type ic profile
78 P F
78 P A
76 P I
Relapsed disease
75 P I
78 P I • Response rate of 45% to date
72 P I
72 P Not done
• mOS immature >6mo.
86 P F • Current median time on treatment of 6.2 months in
66 S I patients in CR/CRi
74 P A
74 P A
• CR/CRi occurring late (median time to remission: 3.8 months)
75 S A
73 P I Response rate Relapsed disease
74 P I
71 S I
Overall response rate 5/11 (45%)
76 P I CR/CRi rate 4/11 (36%)
Refractory
81 P A
disease
Clinical benefit rate (responses +
74 S I 8/11 (73%)
75 P I SD)
75 P I Data continues to mature.
75 P A
0 2 4 Months on treatment 6 8 10 12
P – de novo / primary
disease Ongoing Responder Patient not evaluable
S – secondary disease for efficacy
First CR/CRi reported Date of progression SD (unchanged disease for at least 3 cycles)
F – favorable risk
I – intermediate risk First PR reported Date of death No benefit (PD or discontinuation within first 3 cycles)
Cut-off date: 29 Oct 2020
A – poor / adverse risk
Response assessed according to IWG revised recommendations in reporting AML (Cheson, et al. 2003)
24
Efficacy-evaluable: subjects completed 1 cycle of treatment and have bone marrow blast count at screening and at Cycle 2 or afterPhase II study of bemcentinib monotherapy in relapsed HR-MDS 25
Myelodysplastic Syndromes (MDS)
a heterogeneous group of closely-related clonal hematopoietic disorders
All are characterized by one or more peripheral blood
cytopenias. 30% of MDS patients
develop AML6
MDS • 14% risk in low-risk disease
• 33% risk in intermediate-risk
The incidence of MDS is estimated to be 4 in 100,000.1 patients • 54% risk in high-risk
• 84% risk in very high-risk
The incidence in those aged >80 years is 50-75 in
100,000, sometimes estimated to be higher.1,2,5
Average age of diagnosis is 60 years3, and only 10% of patients
MDS Market 7
are less than 50 years old.2,4
2018 2028
Approx. 30% of patients with MDS will develop AML, rates $1.6 billion $2.4 billion
4.4%
of transformation dependent on risk classification (IPSS-R, Compound annual
WPSS) growth rate
(1) SEER; (2) Neukirchen et al., 2011 (3) Greenberg et al., 2012, (4) Lubeck et al., 2016, (5) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3143554/,
(6) WPSS, (7) GlobalData, June 2020.
26Encouraging ORR and mOS from bemcentinib monotherapy in relapsed HR-MDS
Biomarker
Signature
A small set of soluble plasma biomarkers (Incl. sAXL
+
& Immune mediators) predictive of response to -
bemcentinib monotherapy in HR-MDS patients +
+
+
Best Response Number (%) n=18 +
+
ORR (CR, CRi, PR, SD) 10 (56%)
+
CR/Cri 4 (22%)
+
CR:1 (4%); CRi:3 (14%)
+
PR 1 (6%)
+
SD/HI 5 (28%) -
-
-
-
Companion Diagnostic -
-
BerGenBio has developed a CLIA Lab validated -
Diagnostic assay ready for clinical trial use.
27
*data cut-off June 2020Bemcentinib clinical development in Non Small Cell Lung Cancer (NSCLC) 1) 2L combination with pembrolizumab 2) 1L & 2L combination with erlotinib in EGFRm patients 28
NSCLC causes more cancer related deaths than breast, colon, pancreas and
prostate combined
The largest cancer killer, most patients depend on
drug therapy
Ø 2.09 million new cases of lung cancer diagnosed/yr
85% of lung cancer worldwide, making up 11.6% of all cancer cases1
are NSCLC
Ø 1.76 million lung cancer deaths/yr worldwide1
85% of lung cancers Ø In the U.S, 5-year survival rate is approximately
are NSCLC 18.6%, and 4.7% in patients with distant
metastases2
Non-small cell lung cancer is the most common type of
lung cancer, making up 80-85% of lung cancers
29 (1) Globocan 2018 (2) SEERLarge unmet need in Refractory NSCLC
NSCLC evolving standard of care (SoC) Opportunity for
High PD-L1 driver
driver
bemcentinib
No or low PD-L1 expression
No or low PD-L1 expression expression mutations*
mutations*
Checkpoint Deepening 1L
Pt chemotherapy +/- checkpoint
1st Line inhibitor Targeted therapy responses,
inhibitor
monotherapy particularly PD-L1
negative/low
Pt chemo Pt chemo
2nd & 3rd
Line Severe unmet medical need Effective and well
tolerated 2L therapies
30 * Mutations / rearrangements with available targeted therapies such as EGFR and ALKBGBC008
2L ad. NSCLC Study with bemcentinib + pembrolizumab
Open-label multi-center single arm phase II study
Cohort A Interim Analysis Final Analysis COMPLETE
• Previously treated with a platinum Stage 1 Stage 2
containing chemotherapy
• CPI-naïve N=22 patients N=48 patients
• Has PD at screening
Cohort B Interim Analysis Final Analysis ONGOING
• Previously treated with a mono Stage 1 Stage 2
therapy PD-L1 or PD-1 inhibitor
• Must have had disease control on N=16 patients N=29 patients
most recent treatment
• Has PD at screening
Cohort C Interim Analysis Final Analysis
• Previously treated 1st line with a Stage 1 Stage 2
combination of checkpoint inhibitor
+ platinum-containing chemotherapy N=13 patients N=29 patients
• Must have had disease control on 1st
line therapy
• Has PD at screening
31Cohort A
cAXL predicts response and survival benefit with Bemcentinib
+ Pembrolizumab in 2L NSCLC CPI naïve patients
Change in tumor size Duration of response Survival benefit
cAXL positive cAXL positive 4 fold improvement in mPFS
100,0%
50,0%
8.4 mo
0,0% 1.9 mo
-50,0%
-100,0%
cAXL negative
80,0% cAXL negative
60,0%
Cohort mOS 12-mo OS
40,0%
Cohort A – cAXL +ve pts** 17.3 mo* 79%
20,0%
Cohort A – cAXL -ve pts** 12.4 mo* 60%
0,0%
64%* (up to
BGB Cohort A – all pts** 12.6 mo*
-20,0% 67%)
-40,0% CheckMate-057 (Opdivo) 12.2 mo 51%
-60,0% KEYNOTE-010 (Keytruda) 10.4 mo 43.2%
32Cohort B1
Cohort B: Patient Disposition and Demographics
Biomarkers
cAXL status
Patient disposition N Patient demographics N (%) n = 12*
Screened 21 Median 64,5
Age cAXL positive
Enrolled 16
Range 40-76 42%
Evaluable* 15 58%
cAXL negative
0 6 (38)
Ongoing 3 ECOG at
screen
* with at least 1 post-baseline scan 1 10 (63)
* Of 15 evaluable patients, 3 not
assessment
evaluable for AXL
Female 3 (19)
Sex
Male 13 (81) PD-L1 status
Disease n = 12**
N (%)
mutations Smoker 6 (38)
Strong positive Negative
None 13 (81)
Ex-smoker 8 (50) (TPS >50%) (TPS 1-49%)
25%
Smoking 33%
KRAS 2 (13) status
Never smoked 0 (0)
BRAF 1 (6) Unknown 1 (6) 42% Positive
(TPS 1-49%)
** Of 15 evaluable patients,
3 not evaluable for PD-L1
33Cohort B1
Best % change in sum of target lesions from baseline
60,0%
PD
PD
40,0%
PD
PD
PD
20,0%
SD
SD
PD
SD PD
++ - + + NE + + - -
0,0%
NE ++ ++ + ++ NE
SD SD
SD
non evaluable
-20,0%
cAXL positive
cAXL negative
PD-L1 Status
-40,0% .- Negative PR
.+ Positive *
.++ Strong Positive
NE non evaluable Data cut-off: 17-April-2020
AD awaiting data * Unconfirmed iPR
-60,0%
34Cohort B1
Time on treatment in patients evaluable for cAXL
Pre Tx PD-L1 cAXL
1L P 20 +
2L A/O 65 +
Responses in cAXL positive
cAXL positive
1L A 95 +
group
2L P 15 +
2L N 100 +
14% 14%
2L P 95 + PR
Responses in cAXL negative
1L I/N 2 + group SD
PD
2L P 35 - 71%
0%
cAXL negative
2L N 30 - PR
2L A 0 - SD
PD
2L C NE - 100%
2L P/O 0 -
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46
Weeks
+ cAXL positive
Previous immunotherapy (1 or 2L)
Data cut-off: 17-April-2020
- cAXL negative P: pembrolizumab; A: atezolizumab; N: nivolumab; C: cetrelimab; I: ipilumimab; O: other
35Cohort B1
mPFS improvement in cAXL +ve patients
!"## -
#"$% -
!"#$%&'()#%)"&*+
#"%# - Median: 1.87mo Median: 4.73 mo
#"'% -
Log-rank test
cAXL+ve
#&&&- cAXL-ve
-
-
-
-
-
-
-
-
-
-
-
!""" #""" $""" %""" &""" +""" '""" (""" )""" *""" #!"""
()*+&,*-./012&&&
36Cohort B1
Clinical translational findings
Whole tumour gene expression of Cohort B1 patients benefiting from bemcentinib-
pembrolizumab
Volcano plot
CohortB, all SD vs PD, no S8, RUVs k=2
RNAseq analysis identifies gene signatures from
40
benefiting patients:
30
• Increased AXL expression
Negative EMT regulators EMT signatures
− Log10 adjusted P
AXL • Genes associated with tumour cell EMT1
TREM2
20 PD-L1 • PD-L1 and IFNg expression do not predict response
CCR7
IFNG
TGFB1
• Presence of TREM2+ TAMs#,2
10
• Presence of CCR7+ mregDC1##,3
0
−10 −5 0 5 10
Log2 fold change
Volcano Plot: Differential gene expression analysis of patients showing benefit (n=5)
NS Log2 FC vs patients with PD (n=3)
Adjusted p−value Adjusted p−value & Log2 FC
#
Total = 18365 variables tumor-associated macrophages
##regulatory dendritic cells
1 Liberzon, Cell Systems 2015;2Katzenelenbogen Cell 2020, Molgora Cell 2020; 3Maier Nature 2020
37Cohort B1
Proposed mechanism
AXL+ suppressive myeloid cells drive T cell dysfunction
• AXL promotes tumour-cell EMT and recently-
described regulatory myeloid cells:
• AXL+ TREM2+ Tumour Associated Macrophage1,2
• AXL+ CCR7+ mregDC13
• AXL expression in these cells promotes T cell
dysfunction/exhaustion2
• Bemcentinib may reverse acquired resistance to
checkpoint inhibition by targeting AXL+ TREM2
macrophages and regulatory DCs
• Bemcentinib inhibition of AXL reverses this state of
immune suppression in the microenvironment, and
promotes checkpoint inhibitor re-engagement
TREM – Triggering receptor Expressed on Myeloid Cells
38 1. Katzenelenbogen Cell 2020; 2. Molgora Cell 2020; 3. Maier. et al. Nature 2020 CCR7 - CC Chemokine receptor 7AXL expression defines a poor prognosis subgroup of NSCLC
cAXL+ patients have significantly enhanced survival with bemcentinib + pembrolizumab
in CPI-naïve and -refractory patients
In NSCLC, the AXL expression
encodes poor-prognosis1: defines
expectations of the control arm Cohort A PFS : CPI-naïve Cohort B1 PFS: CPI-refractory
100
AXL IHC low (n=59)
"#$$ -
80 cAXL+ve cAXL+ve
Probability of survival
cAXL-ve cAXL-ve
$#%& -
60 Median: 8.4 mo
AXL IHC high (n=29)
()*+,-./0*,0)-12
Median: Median: 4.73 mo
1.9 mo
40 $#&$ - Median:
1.87mo
20 $#'& -
PBemcentinib clinical development in COVID-19
To evaluate the efficacy and safety in hospitalized COVID-19 patients
- ACCORD-2 trial
- BGBC020 trial in set up
40Bemcentinib evaluation in COVID-19
§ Therapeutic potential of bemcentinib is supported by sound
scientific rationale and external research and review1
§ Orally available, potent and highly selective inhibitor of AXL tyrosine
kinase
§ Preclinical data confirms bemcentinib inhibits SARS-CoV-2 host
cell entry and promotes anti-viral Type I interferon response1,3
§ MoA independent of spike protein (or mutations) and therefore
should remain effective against current and future variants
§ Currently being investigated in PhII clinical studies in hospitalised
COVID-19 patients (3 ethnically diverse countries UK, South Africa
& India
§ Safety and tolerability profile in COVID-19 patients consistent with
>350 patients studied in oncology programme
§ Mild and reversible adverse events
§ IDMC have twice recommended continuation of BGBC020
without amendment to protocol
41
3 Maury IOWA unpublished 3 Meertens L et al. Cell Host & Microbe 2012, 12:544 / 1Chen J et al. Nat Microbiol 2018 3:302COVID-19 Clinical Progression
Stages of the disease Patient classification
Dexamethas
antagonists
Remdesivir
ACCORD2
BGBC020
receptor
Setting Severity Supportive intervention
Bemcentinib: anti viral / innate immunity / anti fibrotic
IL-6
one
no clinical or
Uninfecte virological
0 evidence of
d
infection
no limitation of
1 activities
Ambulato
ry
limitation of
2 activities
mild no oxygen therapy
bemcentinib
3
oxygen by mask or nasal prongs
4
Hospitali
severe non-invasive ventilation or high-
5 sed
flow oxygen
intubation and mechanical
6 ventilation
ventilation and additional organ
7 support –
Death
8
42 Immunity 2020 Jun 16;52(6):905-909. doi: 10.1016/j.immuni.2020.05.004.Potential of Bemcentinib on SARS-CoV-2 infection of host cells
• Utilization of AXL contributes to
ACE2-dependent entry
• AXL enhances virus infection by
facilitating virus entry via an
endosomal pathway
• Bemcentinib control of virus infection
likely involves both reduced
viral entry and enhanced interferon
responses
43 Professor Wendy Maury, BerGenBio R&D Day 6 Nov 2020Slide for Presentation
Bemcentinib studied in COVID19 across 3 countries
Patient Accrual India South Africa UK Total
Bemcentinib 30 27 TBA 57
SoC 30 27 TBA 57
44 CONFIDENTIAL INFORMATIONBemcentinib randomised Studies in COVID-19 COVID: BGBC020
BGBC019 – ACCORD & BGBC020
Primary objective Primary endpoint
Time to sustained clinical improvement of at least 2 points (from
To evaluate the efficacy of bemcentinib as add-on therapy to
randomisation) on a 9-point category ordinal scale, live discharge from the
standard of care (SoC) in patients hospitalised with
hospital, or considered fit for discharge (a score of 0, 1, or 2 on the ordinal
coronavirus disease 2019 (COVID-19).
scale), whichever comes first, by Day 29 (this will also define the “responder”
for the response rate analyses).
Key Secondary objectives Key Secondary objectives
• To evaluate the ability to prevent deterioration according to • The proportion of patients not deteriorating according to the ordinal scale
by 1, 2, or 3 points on Days 2, 8, 15, and 29
the ordinal scale by 1, 2, or 3 points • Duration (days) of oxygen use and oxygen-free days
• To evaluate the number of oxygen-free days • Qualitative and quantitative polymerase chain reaction (PCR)
determination of severe acute respiratory syndrome coronavirus 2 (SARS-
• To evaluate severe acute respiratory syndrome coronavirus 2 CoV-2) in oropharyngeal/nasal swab while hospitalised on Days 1, 3, 5, 8,
(SARS-CoV-2) viral load 11, 15, and 29
Exploratory objectives
Exploratory objectives
• PK concentration and parameters
• To evaluate PK of bemcentinib
• Qualitative and/or quantitative PCR determination of SARS-CoV-2 in blood
• To evaluate SARS-CoV-2 viral load
(on Day 1) and saliva
• To collect samples for serology research, viral genomics,
• Analysis of samples collected at baseline prior to treatment and at specific
serum antibody production, and COVID-19 diagnostics
time points
45Tilvestamab (BGB149) anti-AXL monoclonal antibody 46
Ref. BGB149-101 / NCT03795142
TILVESTAMAB: Anti-AXL monoclonal antibody
Phase I/II clinical trial ongoing
Functional blocking fully-humanised IgG1 GAS6 GAS6
monoclonal antibody
tilvestamab
Binds human AXL, blocks AXL signalling
High affinity (KD: 500pM), displaces GAS6
Anti-tumour efficacy demonstrated in vivo
AXL AXL
Robust manufacturing process established,
18 months stability
Phase Ia healthy volunteer SAD study complete
Safety – no dose limiting toxicity seen up to 3mg/kg dose bemcentinib
Pharmacokinetics - exposure predictable with dose
proportional Cmax increase Invasion Proliferation
Confirmatory evidence of in vivo target engagement with sAXL Immune Migration
suppression
-- stabilisation in circulation
Survival EMT
Phase Ib patient study recruiting
MAD PK/PD
47Well positioned for continued success 48
Why BerGenBio – key take-aways ……
• Route to first approval is becoming
AXL • Leveraging leadership in AXL biology
• Oncology, Virology, Fibrosis Registration apparent
• FDA approved Fast Track and
orphan designation in AML
• COVID-19 top line clinical
• Bemcentinib – selective oral AXL inhibitor, in
more than 15 active sponsored or IST phase II data end of Q1’21
Pipeline trials
• Tilvestamab – mAb in Ph Ib
News Flow • AML survival data update
• NSCLC clinical & translational
• Biomarkers and CDx assays
data
• Relapse AML – emerging significant patient
population with no approved treatment.
Patient Encouraging efficacy and survival benefit
• Relapse HR-MDS potential survival benefit
• 2L NSCLC – translational data supports
Resources • International experienced team
• 2020 YE cash NOK 722m ($85m)
rationale for chemo-free 2L position.
492021 Anticipated Value Driving Catalysts
Bemcentinib in
Relapse AML and Advance solid tumour Advance Tilvestamab
COVID-19
MDS pipeline clinical development
Report update survival data Top line clinical data from Completed Phase 1b safety
trial in South Africa and NSCLC (2L Keytruda combo) study
- Relapse AML - Report Survival benefit
- Relapse HR-MDS India at end of Q1’21 - Pk/PD
chemo & CPI refractory
- RP2D
patients
Seek regulatory advice on ACCORD data anticipated
potential registration path Q2’21 Initiated Phase 2a study
IST data in multiple indications
Seek regulatory guidance
to accelerate approval if
supported by data
50Thank you
Richard S. Godfrey CEO
51 Oslo Børs: BGBIOYou can also read

















































