RANDOMIZED ALL-COMERS EVALUATION OF A PERMANENT POLYMER ZOTAROLIMUS-ELUTING STENT VERSUS A POLYMER-FREE AMPHILIMUS-ELUTING STENT: (RECRE8) A ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
10.1161/CIRCULATIONAHA.118.037707
Randomized All-Comers Evaluation of a Permanent Polymer
Zotarolimus-Eluting Stent Versus a Polymer-Free Amphilimus-Eluting
Stent: (ReCre8) A Multicenter, Non-Inferiority Trial
Running Title: Rozemeijer et al.; The ReCre8 Trial
Rik Rozemeijer, MD, MSc, PharmD1*; Mera Stein, MD, PhD1,2*; Michiel Voskuil, MD, PhD1;
Rutger van den Bor, MSc, PhD3; Peter Frambach, MD4; Bruno Pereira, MD4;
Stefan Koudstaal MD, PhD1,5; Geert E. Leenders, MD, PhD1; Leo Timmers, MD, PhD1; Saskia
Z. Rittersma, MD, PhD1; Adriaan O. Kraaijeveld, MD, PhD1;
Pierfrancesco Agostoni, MD, PhD1,6; Kit Roes, MSc, PhD3;
Pieter A. Doevendans, MD, PhD, FESC1; Pieter Stella, MD, PhD1;
The ReCre8 Study Investigators.
1
Department of Cardiology, University Medical Center Utrecht, Utrecht, The Netherlands;
2
Department of Cardiology, Zuyderland Medical Center, Heerlen, The Netherlands;
3
Department of Biostatistics and Research Support, University Medical Center Utrecht, Utrecht,
Downloaded from http://ahajournals.org by on September 22, 2018
The Netherlands; 4National Institute of Cardiac Surgery and Interventional Cardiology,
Luxembourg, Luxembourg; 5Farr Institute of Health Informatics, University College London,
United Kingdom; 6Department of Cardiology, St. Antonius Hospital, Nieuwegein,
The Netherlands
*Shared first authorship since both authors contributed substantially and equally.
Address for Correspondence:
Pieter R. Stella, MD, PhD
University Medical Center Utrecht
Department of Cardiology
Heidelberglaan 100
room E.04.201, 3584 CX
Utrecht, The Netherlands
Tel: +31 88 7556167
Fax: +31887555427
Email: p.stella@umcutrecht.nl
1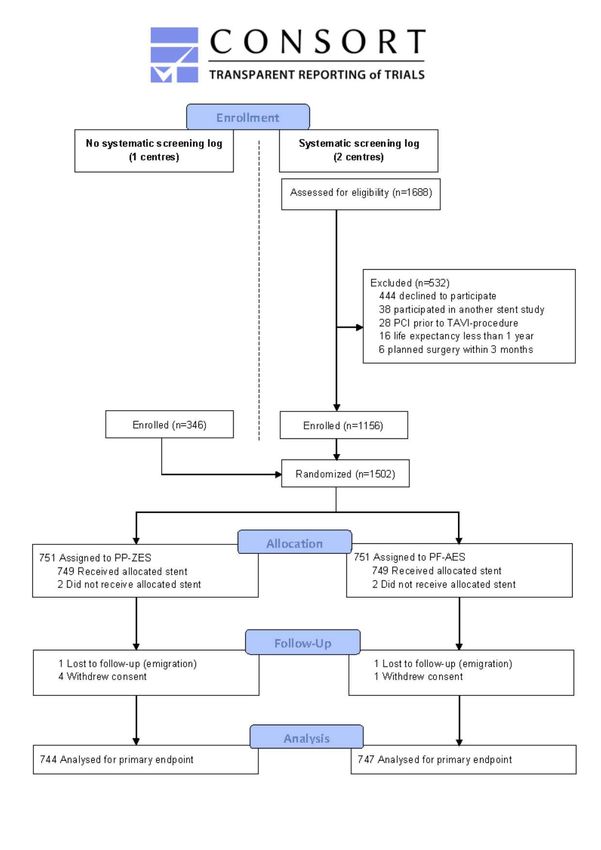
10.1161/CIRCULATIONAHA.118.037707
Abstract
Background: Polymer-free amphilimus-eluting stents (PF-AES) represent a novel elution-
technology in the current era of drug-eluting stents. The clinical safety and efficacy of PF-AES
as compared to latest-generation permanent-polymer zotarolimus-eluting stents (PP-ZES) have
not yet been investigated in a large randomized trial.
Methods: In this physician-initiated, prospective, multicenter, randomized, non-inferiority trial,
an all-comers population requiring percutaneous coronary intervention was enrolled across three
European sites. Randomization (1:1 ratio) to PP-ZES or PF-AES was performed after
stratification for troponin-status, and diabetes. In both treatment arms, troponin-positive patients
were planned for 12-month dual antiplatelet therapy (DAPT), whereas troponin-negative patients
were planned for 1-month DAPT. Outcome assessors were blinded to the allocated treatment.
The device-oriented primary endpoint of target-lesion failure was defined as cardiac death,
target-vessel myocardial infarction, or target-lesion revascularization at 12-months as analyzed
by modified intention-to-treat (80% power, and a 3∙5% non-inferiority margin).
Results: In total 1502 patients were randomized and 1491 treated with the assigned stent and
available for follow-up. The primary endpoint occurred in 42 (5.6%) of the 744 patients
receiving PP-ZES versus 46 (6∙2%) of the 747 patients receiving PF-AES. PF-AES were
clinically non-inferior to PP-ZES (risk difference 0∙5%, upper limit one-sided 95% confidence
interval 2∙6%, pnon-inferiority=0∙0086). Cardiac death occurred in 10 (1∙3%) vs. 10 patients (1∙3%, p-
value for difference 1∙00), target-vessel myocardial infarction occurred in 18 (2∙4%) vs. 17
patients (2∙3%, p-value for difference 0∙87), and target-lesion revascularization occurred in 22
(2∙9%) vs. 20 patients (2∙6%, p-value for difference 0∙75) for PF-AES as compared to PP-ZES.
Overall, definite or probable stent thrombosis occurred in 1∙0%.
Downloaded from http://ahajournals.org by on September 22, 2018
Conclusions: PF-AES were non-inferior to PP-ZES regarding target-lesion failure at 12 months.
Findings regarding the secondary endpoint and pre-specified subgroups were generally
consistent with that of the primary endpoint.
Clinical Trial Registration: URL: http://www.clinicaltrials.gov. Unique identifier:
NCT02328898.
Key Words: Coronary Artery Disease; Drug-eluting Stents; Dual Antiplatelet Therapy;
Polymer-free; Stent Trombosis
210.1161/CIRCULATIONAHA.118.037707
Clinical Perspective
What is new ?
• The ReCre8 study is a prospective, randomized, multicenter study comparing polymer-
free amphilimus-eluting stents (PF-AES) and permanent polymer zotarolimus-eluting
stents (PP-ZES) in patients undergoing percutaneous coronary intervention.
• Based on troponin level at the time of randomisation, troponin-positive patients were
treated with 12 months dual antiplatelet therapy (DAPT), whereas troponin-negative
patients were treated with 1 month of DAPT.
• Stratification was performed for troponin status and the presence of diabetes.
What are the clinical implications ?
• PF-AES is non-inferior to PP-ZES in regard to the primary endpoint of target-lesion
failure at 12 months follow-up.
• Low rates of stent thrombosis were observed using these latest-generation drug-eluting
stents, even with short duration of DAPT.
Downloaded from http://ahajournals.org by on September 22, 2018
• A future dedicated trial on PF-AES in diabetic patients is required in order to explore
efficacy of this novel drug-eluting technology in this specific subgroup.
310.1161/CIRCULATIONAHA.118.037707
Introduction
Drug-eluting stents (DES) that release antiproliferative agents have lower rates of restenosis than
bare-metal stents and are now considered the standard of care in patients undergoing
percutaneous coronary intervention.1, 2 Development of new-generation DES focused on
improving (1) stent alloy composition or stent design, (2) biocompatibility of the drug-eluting
polymer coating, or (3) properties and release of the antiproliferative agent.
One of the incentives to improve the biokinetics of the polymer coating was based on
several reports3, 4 that linked presence of permanent polymers to impaired arterial healing and
incomplete stent strut endothelialisation, leading to late stent thrombosis5 particularly in
multimorbid patients with complex lesions. In an attempt to circumvent these late adverse
events, one of the latest-generation DES is polymer-free and releases the antiproliferative drugs
by means of an amphipilic carrier stored in abluminal laser-dug wells. As a result, this stent
Downloaded from http://ahajournals.org by on September 22, 2018
exhibits the properties of a DES in the first months after implantation6, and potentially without
the risk on late polymer-induced adverse events. A previous study7 showed that polymer-free
amphilimus-eluting stents (PF-AES) were associated with a reduction in late restenosis
compared to a permanent polymer paclitaxel-eluting stent. However, the clinical safety and
efficacy of PF-AES have not yet been compared to the latest-generation permanent polymer
coated stents in a large randomized all-comers population. The main study interest was a head-
to-head comparison between both stents, however an explorative subanalysis was performed on a
reduced duration of dual antiplatelet therapy (DAPT) in troponin-negative patients, and diabetic
status.
410.1161/CIRCULATIONAHA.118.037707
To address these important issues, the ReCre8 trial was designed to evaluate clinical non-
inferiority of PF-AES as compared to latest-generation permanent polymer zotarolimus-eluting
stents (PP-ZES) in all-comers requiring percutaneous coronary intervention.
Methods
Study Design and Participants
ReCre8 (Randomized All-comers Evaluation of a Permanent Polymer Zotarolimus-eluting Stent
Versus a Polymer-Free Amphilimus-eluting Stent: a Multicenter, Non-inferiority Trial) was a
physician-initiated, prospective, multicenter, randomized trial comparing latest-generation PP-
ZES versus PF-AES across three European centers (University Medical Center Utrecht, and
Zuyderland Medical Center Heerlen both in The Netherlands, and the National Institute of
Cardiac Surgery and Interventional Cardiology in Luxembourg (Appendix I in the online
Downloaded from http://ahajournals.org by on September 22, 2018
Supplement). The study design and rationale has been reported and described previously.8
Briefly, this study used broad eligibility criteria and minor exclusion criteria to reflect routine
clinical practice. Patients were eligible if they were capable of providing informed consent, aged
18 years or older, and had clinical evidence of ischemic heart disease presenting with stable
coronary artery disease or acute coronary syndromes including myocardial infarction with or
without ST-segment elevation. Angiographic inclusion criterion was a reference vessel diameter
of 2.5 to 4.5 mm. There were no restrictions for lesion types, lesion length, or number of treated
lesions. The exclusion criteria were: participation in another randomized stent study before
reaching the primary endpoint, planned surgery within the first three months, assumed life-
expectancy of less than one year, and revascularization prior to transcatheter aortic valve
implantation. The study protocol was designed and executed according to Good Clinical
510.1161/CIRCULATIONAHA.118.037707
Practice, and was approved by the Medical Research Ethics Committee Utrecht and the
institutional review boards of each participating center. The trial is conducted in accordance with
the Declaration of Helsinki and reported in accordance with the CONSORT 2010 Statement9.
The manuscript adheres to Transparency and Openness Promotion Guidelines, and data will be
made available based upon reasonable request and contact to the corresponding author. This
study was monitored by an independent clinical research organization. Each participating patient
provided written informed consent to participate in this study. This study is registered with
ClinicalTrials.gov, number NCT02328898.
Randomization and blinding
Patients were randomly assigned after diagnostic coronary angiography and before percutaneous
coronary intervention to receive either PP-ZES or PF-AES in a 1:1 ratio in random blocks of 4
after stratification for troponin-status, and the presence of diabetes. Randomisation was done
Downloaded from http://ahajournals.org by on September 22, 2018
using a web-based system that was designed and maintained by an independent research
organization. Healthcare providers were aware of the treatment allocation. Outcome assessors
and the members of the independent clinical event committee were blinded to the allocated
treatment.
Procedures
Percutaneous coronary intervention was performed according to standard techniques. Lesion
predilatation, the use of glycoprotein IIb/IIIa receptor antagonists, techniques such as rotational
atherectomy, direct stenting, bifurcation strategy, advanced chronic total occlusion techniques,
and post-dilatation were left to the operators discretion. Full lesion coverage was attempted by
the implantation of one or more assigned study stents. A patient with multiple lesions was treated
with the allocated study stent for all lesions. Staged procedures using the same stent according to
610.1161/CIRCULATIONAHA.118.037707
randomization were permitted within six weeks after index procedure. PP-ZES (Resolute
Integrity, Medtronic Vascular, Santa Rosa, USA) available for use in this trial were 2∙50, 2∙75,
3∙00, 3∙50, and 4∙00 mm, with stent length of 8 to 38 mm. PF-AES (Cre8, Alvimedica, Istanbul,
Turkey) available for use were similar in diameter and lengths of those of the PP-ZES (i.e. 2∙50
to 4∙00 mm, and up to 38 mm).
Prior to stent implantation, patients received aspirin and clopidogrel in elective
procedures, and ticagrelor (or prasugrel) in case of non-elective procedures, together with an
intravenous dose of 70 to 100 IU/kg unfractionated heparin. After the procedure troponin-
negative patients received 1-month DAPT (i.e. 100 mg aspirin and 75 mg clopidogrel daily).
Patients who were troponin-positive received 12-month DAPT (i.e. 100 mg aspirin and 90 mg
ticagrelor twice daily or 10 mg prasugrel once daily). Electrocardiographs were systematically
performed before and within 24 h after the intervention, or for any suspected recurrent symptoms
Downloaded from http://ahajournals.org by on September 22, 2018
or signs of ischemia. Cardiac markers (e.g. creatine kinase, creatinine kinase myocardial band,
and troponin T or I) were drawn within 24 hours before percutaneous coronary intervention and
approximately three to six hours after the procedure. No routine angiographic follow-up was
specified in the study protocol.
Outcomes
The device-oriented primary endpoint was target-lesion failure, defined as a composite of safety
(cardiac death, target-vessel myocardial infarction) and efficacy (target-lesion revascularization)
at 12 months. The patient-oriented secondary endpoint was a composite of death, stroke,
myocardial infarction, any unplanned repeated revascularization or major bleeding. Clinical
endpoints were defined as proposed by the Academic Research Consortium10. Death was
considered cardiac when due to an evident cardiac cause, when related to percutaneous coronary
710.1161/CIRCULATIONAHA.118.037707
intervention, unwitnessed death, or death from unknown causes. Myocardial infarction was
classified by the electrocardiogram according to the Minnesota code into Q-wave or Non Q-
wave myocardial infarction, and defined according to the Academic Research Consortium
criteria10. Periprocedural myocardial infarction was defined as a typical rise and fall in cardiac
markers of at least three times the upper reference limit. Spontaneous myocardial infarction was
defined a typical rise and fall in cardiac markers of at least one time the upper reference limit.
Stent thrombosis was defined and classified according to criteria provided by the Academic
Research Consortium.10 Target-lesion revascularization was defined as any repeat percutaneous
coronary intervention or coronary bypass surgery caused by a more than 50% stenosis within a 5
mm border adjacent to the study stent. Target-vessel revascularization was defined as a repeat
percutaneous coronary intervention or bypass surgery for the coronary artery with the target-
lesion. Revascularization was deemed clinically driven if any of the target lesion or vessel
Downloaded from http://ahajournals.org by on September 22, 2018
showed at least 50% stenosis in the presence of objective evidence of ischemia from non-
invasive or invasive testing, and/or symptoms. Any unplanned revascularization was defined as
any repeat revasculization that was not detected during the index coronary angiogram and
demanded treatment by percutaneous coronary intervention. Bleeding events were classified
according to Bleeding Academic Research Criteria11, and considered major if BARC3 or above.
Data were captured in dedicated web-based electronic case report forms that were
designed by an independent research organization (i.e. Julius Clinical Research, Zeist, The
Netherlands). On-site monitoring was performed by independent trained personnel of Julius
Clinical Research with data complete source verification of serious adverse events. An
independent clinical event committee that was blinded to the allocated treatment reviewed and
adjudicated all clinical endpoints.
810.1161/CIRCULATIONAHA.118.037707
Statistical Analysis
The study was powered to evaluate clinical non-inferiority of PF-AES versus PP-ZES regarding
the device-oriented primary endpoint and patient-oriented secondary endpoint at 12-months. A
proportion of approximately 5∙5% for the primary device-oriented endpoint, and 8∙0% for the
secondary patient-oriented endpoint in both treatment arms was assumed as was found on event
endpoints in similar previous trials12, 13. We chose a non-inferiority margin of 3∙5% as an
acceptable difference. Consequently, to evaluate clinical non-inferiority on both the 12-months
device-oriented primary and the patient-oriented secondary endpoint, we estimated that 1486
patients were required (743 patients in each group) to obtain a power of at least 80%, a one-sided
alpha level of 0∙05. To account for a maximum lost-to-follow-up of 3∙0% we anticipated the
required number of patients to be 1532. Sample size calculations were performed using PASS
2008 version 08.0.16 (NCSS, Kaysville, USA).
Downloaded from http://ahajournals.org by on September 22, 2018
In the primary analysis a risk difference was calculated (i.e. the proportion of patients
with a primary or secondary endpoint following the PF-AES minus the proportion of patients
following PP-ZES) along with the upper bound of the one-sided 95% Newcombe hybrid score
confidence interval and the Farrington-Manning’s test for non-inferiority. In a secondary
analysis, Cox proportional-hazards regression with covariate adjustment of stratification factors
and study site included as stratum was performed to regress the time-to-first endpoint for the
allocated study stent for the primary and secondary endpoint. Pre-specified subgroup analysis
were troponin-status and diabetes mellitus, whereas sex, age, and complex lesions were
analyzed post-hoc to investigate the consistency of the primary endpoint including a possible
interaction with the allocated stent type. Finally, a Fine and Gray competing risk regression
910.1161/CIRCULATIONAHA.118.037707
model was used to evaluate non-cardiovascular death as a competing risk. Analyses were
performed based on the modified intention-to-treat principle.
Time-to-first-event for the primary and secondary endpoint and separate components
were analyzed using Kaplan-Meier methods with log-rank tests, and reported in accordance with
good practice14. Time-to-event was defined as the number of days between intervention and
occurrence of any component of the primary or secondary endpoints. Patients were censored at
one year, or the time of their last follow-up, whichever came first. All statistical analyses were
performed using SAS version 9.4 (SAS Institute, Cary, USA).
Results
Between Nov 3, 2014, and July 10, 2017, 1502 eligible all-comers patients with 2133 lesions,
aged 29-93 years, consented to study enrollment. The study flowchart is shown in Figure 1.
Downloaded from http://ahajournals.org by on September 22, 2018
Almost all patients (>99%) were successfully treated with at least one assigned study stent, and
the proportion of patients with deviation from the allocated treatment was10.1161/CIRCULATIONAHA.118.037707
and complex lesions in 59%. Diabetes mellitus was diagnosed in 20% of the patients and equally
distributed.
Lesion and procedural characteristics (Table 2) including direct stenting (30%), and the
use of glycoprotein IIb/IIIa antagonists (15%) were comparable for both groups, except for a
higher rate of post-dilatation in PF-AES (60 vs. 68%, p10.1161/CIRCULATIONAHA.118.037707
Definite or probable stent thrombosis occurred in 6 (0∙8%) of 744 patients receiving PP-ZES
versus 9 (1∙2%) of 747 patients receiving PF-AES (p=0∙44). Detailed information on the clinical
circumstances and consequences regarding definite stent thrombosis was provided (Appendix IV
Table 2 in the online Supplement).
Discussion
The ReCre8 study shows that PF-AES are clinically non-inferior to latest-generation PP-ZES
regarding target-lesion failure at 12-months. The overall rates of the device-oriented primary
endpoint of target-lesion failure, a composite of cardiac death, target-vessel myocardial
infarction, or target-lesion revascularization did not differ significantly for both stents, nor did
any of the individual components. The patients included in the current trial consisted of a true
all-comers population as reflected by a high proportion of patients with ST-segment elevation
Downloaded from http://ahajournals.org by on September 22, 2018
myocardial infarction in this study, and was among the highest of recently published all-comer
trials13, 15-17. Also, the population was characterized by a high number of left main disease,
bifcation lesions, and chronic total occlusions. The number of complex type C lesions was
equivalent to previous reports12, 13, 15, 18.
The frequency of target-lesion failure at 12-months in PP-ZES in this study was low, and
consistent with those reported in previous studies using PP-ZES12, 13, that used similar endpoint
definitions. In DUTCH PEERS12 target-lesion failure defined as cardiac death, target-vessel
related myocardial infarction or clinically-driven target-lesion revascularization for PP-ZES was
5∙1% at 12-months. In SORT OUT VI13 target-lesion failure defined as cardiac death, myocardial
infarction not clearly attributable to non-target lesion and clinically indicated target-lesion
1210.1161/CIRCULATIONAHA.118.037707
revascularization, and 5∙3%. These results are consistent with the 5∙6% rate of the primary
endpoint at 12-months in the ReCre8 trial.
The rate of target-lesion failure for PF-AES at 12-months matched those with a previous
non-randomized report19 on this novel device, despite a higher baseline risk in our study
population. The increased frequency of post-dilatation in PF-AES was not anticipated, and the
reason for this finding remains unclear to us. It seems unlikely, however, that this may have
substantially influenced clinical outcomes. Counterintuitively, the rate of target-lesion failure
observed in troponin-positive patients was lower than that of troponin-negative patients. This
might be explained by more complex lesions in troponin-negative patients. Based on our
findings, however, a negative effect of short DAPT on target-lesion failure cannot be ruled out.
The possibility that short DAPT may have caused an increase in TLF in troponin-negative
patients needs further investigation. These findings do not support deviating from current
Downloaded from http://ahajournals.org by on September 22, 2018
guidelines on DAPT duration20.
The proportion of patients with target-vessel myocardial infarction were similar in both
arms and correspond well to those reported by previous studies ranging from 2%12, 18, 21 to even
up to 6%22, depending on study population and definitions used. Myocardial infarction related to
the target-vessel occurred within the periprocedural period in the majority of patients (80%).
The occurrence of definite or probable stent thrombosis, as an important safety indicator, did not
differ between the two DES types (0∙8% versus 1∙2%), and was comparable to other reports12, 15,
21
. It should be empathized, however, that this trial did not yield the power to detect differences
for endpoints with such low incidences. Six cases of definite stent thrombosis were observed
after one month in the troponin-negative arm. Indeed, the finding that most cases of definite stent
1310.1161/CIRCULATIONAHA.118.037707
thrombosis occurred in complex lesions using multi-overlapping stents, treatment of bifurcations,
or chronic total occlusions may need further investigation.
Current literature shows that stent performance in diabetic patients is still worse than
those in non-diabetics, with high rates of in-stent restenosis and target-lesion revascularization
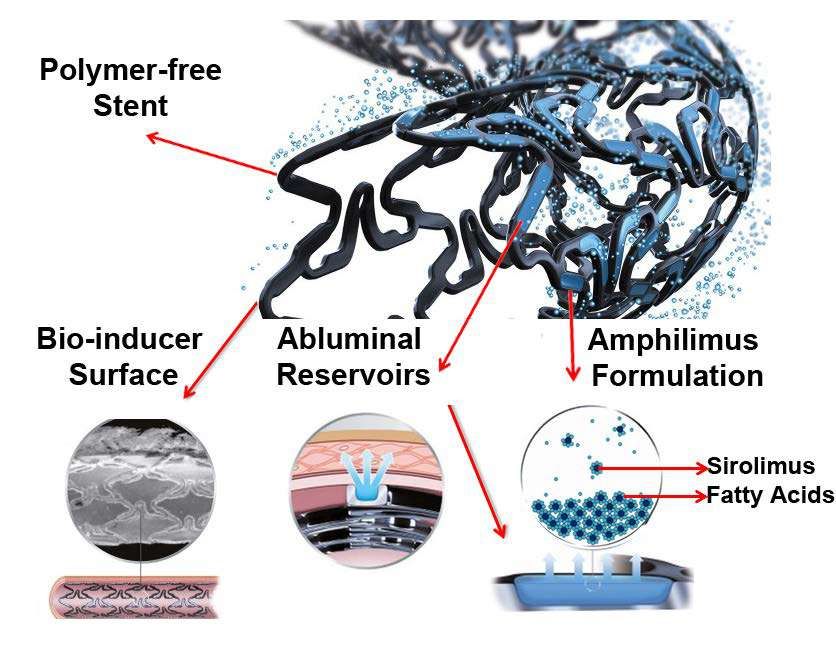
reaching up to 13.5%23. The amphilimus formulation – a mixture of sirolimus and long-chained
fatty acids – used in PF-AES enhances the uptake of antiproliferative agents24 and may be
associated with a higher antirestenotic potency in diabetics. The abluminal reservoirs (figure 4)
that are filled with the amphilimus formulation reflect a novel strategy that needs further
investigation. As previous clinical reports7, 25 revealed encouraging results on PF-AES in
diabetes, a pre-specified analysis of PF-AES versus PP-ZES was performed.8 No between stent
differences were detected in the diabetic subgroup. Most likely this was due to a relatively low
enrolment of diabetic patients, and a lower-than-expected event rate in this subgroup. Since
Downloaded from http://ahajournals.org by on September 22, 2018
significant differences in target-lesion revascularization and target-vessel revascularization were
found at 3 years clinical follow-up in the Next trial7 , the duration of follow-up may also be a
factor that explains the observed event rate.
This trial has several limitations we should acknowledge. First, like most coronary stent
studies ReCre8 was an open-label study, where physicians were not blinded to the allocated
treatment. We believe, however, that this does not change our findings since we used well-
standardized clinical endpoints10, 11 with rigorous event adjudication by an independent clinical
event committee which was blinded to the allocated treatment. Second, even though this large-
scale study has established clinical non-inferiority of PF-AES, the non-inferiority margin of
3∙5% was relatively large which needs to be taken into consideration in the interpretation of the
results limiting the precision with which non-inferiority could be established. It was not powered
1410.1161/CIRCULATIONAHA.118.037707
to address potential differences in adverse clinical events that occur at low rates. Third, one
center did not provide data on the screening for enrollment of the corresponding 20% of the
patients which may have caused selection bias. Even though we acknowledge it would be best to
have a screenings log of all patients, we believe that the risk of selection bias was low and did
not change the overall conclusions of this study. Fourth, this trial was conducted at three North-
western European sites, and may therefore not be applicable to other geographical regions with
differences in clinical baseline characteristics (such as diabetes or lesion complexity), or
procedural characteristics.
Conclusions
This trial demonstrates that PF-AES is non inferior to a latest-generation PP-ZES with regards to
target-lesion failure at 12-months follow-up. Findings regarding the secondary endpoint and pre-
specified subgroups were generally consistent with that of the primary endpoint. Further clinical
Downloaded from http://ahajournals.org by on September 22, 2018
follow-up until 3 years will be performed in order to test the long-term outcomes of these
devices.
Sources of Funding
The University Medical Center Utrecht was the main sponsor of the study. No funding by
industry was involved. The stent manufacturers had no role in the design of the study, collection,
analysis or interpretation of the data, nor in the writing of this report, or in the decision to submit
this manuscript for publication. The corresponding author had full access to all of the data in the
study and had the final responsibility for the decision to submit for publication.
1510.1161/CIRCULATIONAHA.118.037707
Acknowledgments
To all involved (research) nurses, technicians, and personnel who made great efforts for the
successful enrolment and completion of this study. Special thanks goes out to Yvonne Breuer,
manager of the R&D department, UMCU, Astrid Links, data manager, UMCU, and all fellows
and physicians involved in study enrolment and data collection.
Disclosures
PRS is member of speakersbureau, Alvimedica, all other authors have no conflicts of interest to
declare.
References
1. Stefanini GG and Holmes DR, Jr. Drug-eluting coronary-artery stents. N Engl J Med.
2013;368:254-265.
Downloaded from http://ahajournals.org by on September 22, 2018
2. Stettler C, Wandel S, Allemann S, Kastrati A, Morice MC, Schomig A, Pfisterer ME,
Stone GW, Leon MB, de Lezo JS, Goy JJ, Park SJ, Sabate M, Suttorp MJ, Kelbaek H, Spaulding
C, Menichelli M, Vermeersch P, Dirksen MT, Cervinka P, Petronio AS, Nordmann AJ, Diem P,
Meier B, Zwahlen M, Reichenbach S, Trelle S, Windecker S and Juni P. Outcomes associated
with drug-eluting and bare-metal stents: a collaborative network meta-analysis. Lancet.
2007;370:937-948.
3. Daemen J, Wenaweser P, Tsuchida K, Abrecht L, Vaina S, Morger C, Kukreja N, Juni P,
Sianos G, Hellige G, van Domburg RT, Hess OM, Boersma E, Meier B, Windecker S and
Serruys PW. Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting
stents in routine clinical practice: data from a large two-institutional cohort study. Lancet.
2007;369:667-678.
4. Stone GW, Moses JW, Ellis SG, Schofer J, Dawkins KD, Morice MC, Colombo A,
Schampaert E, Grube E, Kirtane AJ, Cutlip DE, Fahy M, Pocock SJ, Mehran R and Leon MB.
Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N Engl J Med.
2007;356:998-1008.
5. Joner M, Finn AV, Farb A, Mont EK, Kolodgie FD, Ladich E, Kutys R, Skorija K, Gold
HK and Virmani R. Pathology of drug-eluting stents in humans: delayed healing and late
thrombotic risk. J Am Coll Cardiol. 2006;48:193-202.
6. Prati F, Romagnoli E, Valgimigli M, Burzotta F, De Benedictis M, Ramondo A, Mehran
R and Stella PR. Randomized comparison between 3-month Cre8 DES vs. 1-month
Vision/Multilink8 BMS neointimal coverage assessed by OCT evaluation: the DEMONSTRATE
study. Int J Cardiol. 2014;176:904-909.
1610.1161/CIRCULATIONAHA.118.037707
7. Carrie D, Berland J, Verheye S, Hauptmann KE, Vrolix M, Violini R, Dibie A, Berti S,
Maupas E, Antoniucci D and Schofer J. A multicenter randomized trial comparing amphilimus-
with paclitaxel-eluting stents in de novo native coronary artery lesions. J Am Coll Cardiol.
2012;59:1371-1376.
8. Rozemeijer R, Stein M, Frambach P, Voskuil M, Kraaijeveld AO, Rodriguez-Olivares R,
Timmers L, Pereira B, Rittersma SZ, Agostoni P, Doevendans PA and Stella PR. Rationale and
design of amphilimus sirolimus-eluting stents versus zotarolimus-eluting stents in all-comers
requiring percutaneous coronary intervention (ReCre8): A multicenter randomized clinical trial.
Catheter Cardiovasc Interv. 2018;91:410-416.
9. Piaggio G, Elbourne DR, Pocock SJ, Evans SJ, Altman DG and Group C. Reporting of
noninferiority and equivalence randomized trials: extension of the CONSORT 2010 statement.
JAMA. 2012;308:2594-2604.
10. Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, Steg PG, Morel
MA, Mauri L, Vranckx P, McFadden E, Lansky A, Hamon M, Krucoff MW, Serruys PW and
Academic Research C. Clinical end points in coronary stent trials: a case for standardized
definitions. Circulation. 2007;115:2344-2351.
11. Mehran R, Rao SV, Bhatt DL, Gibson CM, Caixeta A, Eikelboom J, Kaul S, Wiviott SD,
Menon V, Nikolsky E, Serebruany V, Valgimigli M, Vranckx P, Taggart D, Sabik JF, Cutlip DE,
Krucoff MW, Ohman EM, Steg PG and White H. Standardized bleeding definitions for
cardiovascular clinical trials: a consensus report from the Bleeding Academic Research
Consortium. Circulation. 2011;123:2736-2747.
12. von Birgelen C, Sen H, Lam MK, Danse PW, Jessurun GA, Hautvast RW, van
Houwelingen GK, Schramm AR, Gin RM, Louwerenburg JW, de Man FH, Stoel MG, Lowik
MM, Linssen GC, Said SA, Nienhuis MB, Verhorst PM, Basalus MW, Doggen CJ and Tandjung
Downloaded from http://ahajournals.org by on September 22, 2018
K. Third-generation zotarolimus-eluting and everolimus-eluting stents in all-comer patients
requiring a percutaneous coronary intervention (DUTCH PEERS): a randomised, single-blind,
multicentre, non-inferiority trial. Lancet. 2014;383:413-423.
13. Raungaard B, Jensen LO, Tilsted HH, Christiansen EH, Maeng M, Terkelsen CJ, Krusell
LR, Kaltoft A, Kristensen SD, Botker HE, Thuesen L, Aaroe J, Jensen SE, Villadsen AB,
Thayssen P, Veien KT, Hansen KN, Junker A, Madsen M, Ravkilde J, Lassen JF and
Scandinavian Organization for Randomized Trials with Clinical O. Zotarolimus-eluting durable-
polymer-coated stent versus a biolimus-eluting biodegradable-polymer-coated stent in unselected
patients undergoing percutaneous coronary intervention (SORT OUT VI): a randomised non-
inferiority trial. Lancet. 2015;385:1527-1535.
14. Pocock SJ, Clayton TC and Altman DG. Survival plots of time-to-event outcomes in
clinical trials: good practice and pitfalls. Lancet. 2002;359:1686-1689.
15. Smits PC, Hofma S, Togni M, Vazquez N, Valdes M, Voudris V, Slagboom T, Goy JJ,
Vuillomenet A, Serra A, Nouche RT, den Heijer P and van der Ent M. Abluminal biodegradable
polymer biolimus-eluting stent versus durable polymer everolimus-eluting stent (COMPARE II):
a randomised, controlled, non-inferiority trial. Lancet. 2013;381:651-660.
16. Pilgrim T, Heg D, Roffi M, Tuller D, Muller O, Vuilliomenet A, Cook S, Weilenmann D,
Kaiser C, Jamshidi P, Fahrni T, Moschovitis A, Noble S, Eberli FR, Wenaweser P, Juni P and
Windecker S. Ultrathin strut biodegradable polymer sirolimus-eluting stent versus durable
polymer everolimus-eluting stent for percutaneous coronary revascularisation (BIOSCIENCE): a
randomised, single-blind, non-inferiority trial. Lancet. 2014;384:2111-2122.
1710.1161/CIRCULATIONAHA.118.037707
17. Park KW, Kang SH, Kang HJ, Koo BK, Park BE, Cha KS, Rhew JY, Jeon HK, Shin ES,
Oh JH, Jeong MH, Kim S, Hwang KK, Yoon JH, Lee SY, Park TH, Moon KW, Kwon HM, Hur
SH, Ryu JK, Lee BR, Park YW, Chae IH, Kim HS and Investigators H-A. A randomized
comparison of platinum chromium-based everolimus-eluting stents versus cobalt chromium-
based Zotarolimus-Eluting stents in all-comers receiving percutaneous coronary intervention:
HOST-ASSURE (harmonizing optimal strategy for treatment of coronary artery stenosis-safety
& effectiveness of drug-eluting stents & anti-platelet regimen), a randomized, controlled,
noninferiority trial. J Am Coll Cardiol. 2014;63:2805-2816.
18. von Birgelen C, Kok MM, van der Heijden LC, Danse PW, Schotborgh CE, Scholte M,
Gin R, Somi S, van Houwelingen KG, Stoel MG, de Man F, Louwerenburg JHW, Hartmann M,
Zocca P, Linssen GCM, van der Palen J, Doggen CJM and Lowik MM. Very thin strut
biodegradable polymer everolimus-eluting and sirolimus-eluting stents versus durable polymer
zotarolimus-eluting stents in allcomers with coronary artery disease (BIO-RESORT): a three-
arm, randomised, non-inferiority trial. Lancet. 2016;388:2607-2617.
19. Godino C, Pivato CA, Chiarito M, Donahue M, Testa L, Colantonio R, Cappelletti A,
Milazzo D, Parisi R, Nicolino A, Moshiri S, Aprigliano G, Palloshi A, Zavalloni Parenti D,
Rutigliano D, Locuratolo N, Melillo F, Scotti A, Arrigoni L, Montorfano M, Fattori R, Presbitero
P, Sardella G, Bedogni F, Margonato A, Briguori C, Colombo A, Italian Nobori Stent
ProspectIve R and Amphilimu Simri. Polymer-free amphilimus-eluting stent versus
biodegradable polymer biolimus-eluting stent in patients with and without diabetes mellitus. Int J
Cardiol. 2017;245:69-76.
20. Valgimigli M, Bueno H, Byrne RA, Collet JP, Costa F, Jeppsson A, Juni P, Kastrati A,
Kolh P, Mauri L, Montalescot G, Neumann FJ, Petricevic M, Roffi M, Steg PG, Windecker S,
Zamorano JL, Levine GN, Group ESCSD, Guidelines ESCCfP and Societies ESCNC. 2017 ESC
Downloaded from http://ahajournals.org by on September 22, 2018
focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration
with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the
European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic
Surgery (EACTS). Eur Heart J. 2018;39:213-260.
21. de Winter RJ, Katagiri Y, Asano T, Milewski KP, Lurz P, Buszman P, Jessurun GAJ,
Koch KT, Troquay RPT, Hamer BJB, Ophuis TO, Wohrle J, Wyderka R, Cayla G, Hofma SH,
Levesque S, Zurakowski A, Fischer D, Kosmider M, Goube P, Arkenbout EK, Noutsias M,
Ferrari MW, Onuma Y, Wijns W and Serruys PW. A sirolimus-eluting bioabsorbable polymer-
coated stent (MiStent) versus an everolimus-eluting durable polymer stent (Xience) after
percutaneous coronary intervention (DESSOLVE III): a randomised, single-blind, multicentre,
non-inferiority, phase 3 trial. Lancet. 2018;391:431-440.
22. Kandzari DE, Mauri L, Koolen JJ, Massaro JM, Doros G, Garcia-Garcia HM, Bennett J,
Roguin A, Gharib EG, Cutlip DE, Waksman R and Investigators BV. Ultrathin, bioresorbable
polymer sirolimus-eluting stents versus thin, durable polymer everolimus-eluting stents in
patients undergoing coronary revascularisation (BIOFLOW V): a randomised trial. Lancet.
2017;390:1843-1852.
23. Silber S, Serruys PW, Leon MB, Meredith IT, Windecker S, Neumann FJ, Belardi J,
Widimsky P, Massaro J, Novack V, Yeung AC, Saito S and Mauri L. Clinical outcome of
patients with and without diabetes mellitus after percutaneous coronary intervention with the
resolute zotarolimus-eluting stent: 2-year results from the prospectively pooled analysis of the
international global RESOLUTE program. JACC Cardiovasc Interv. 2013;6:357-368.
1810.1161/CIRCULATIONAHA.118.037707
24. Moretti C, Lolli V, Perona G, Vignolini MC, Cabiale K, Falzone M and Galloni M. Cre8
coronary stent: preclinical in vivo assessment of a new generation polymer-free DES with
Amphilimus formulation. EuroIntervention. 2012;7:1087-1094.
25. Romaguera R, Gomez-Hospital JA, Gomez-Lara J, Brugaletta S, Pinar E, Jimenez-
Quevedo P, Gracida M, Roura G, Ferreiro JL, Teruel L, Montanya E, Fernandez-Ortiz A,
Alfonso F, Valgimigli M, Sabate M and Cequier A. A Randomized Comparison of Reservoir-
Based Polymer-Free Amphilimus-Eluting Stents Versus Everolimus-Eluting Stents With Durable
Polymer in Patients With Diabetes Mellitus: The RESERVOIR Clinical Trial. JACC Cardiovasc
Interv. 2016;9:42-50.
Downloaded from http://ahajournals.org by on September 22, 2018
1910.1161/CIRCULATIONAHA.118.037707
Table 1. Baseline characteristics
Overall PP-ZES PF-AES p-value
(n=1491) (n=744) (n=747)
Clinical Characteristics
Age (years) 64∙9 ± 11∙0 65∙1 ± 10∙6 64∙7 ± 11∙3 0∙55
Male Sex 1142 (76∙6) 577 (77∙6) 565 (75∙6) 0∙38
Body-Mass Index (kg/m2) 27∙3 ± 4∙43 27∙2 ± 4∙40 27∙5 ± 4∙46 0∙34
Hypertension 823 (55∙2) 411 (55∙2) 412 (55∙2) 0∙85
Hypercholesterolemia 665 (44∙6) 340 (45∙8) 325 (43∙5) 0∙49
Diabetes Mellitus 304 (20∙4) 149 (20∙0) 155 (20∙8) 0∙67
Insulin-treated 96 (6.4) 47 (6∙3) 49 (6∙6) 0.97
Current smoker 384 (25∙8) 191 (25∙7) 193 (25∙9) 0∙71
Family history of cardiovascular disease 566 (38∙0) 275 (37∙0) 291 (39∙0) 0∙70
Renal insufficiency (eGFR20 mm) 744 (50∙2) 415 (56∙1) 329 (44∙3)10.1161/CIRCULATIONAHA.118.037707
Number of diseased coronary vessels 0∙67
One 839 (56∙3) 433 (58∙2) 406 (54∙4)
Two 425 (28∙5) 200 (26∙9) 225 (30∙1)
Three or more 227 (15∙2) 111 (14∙9) 116 (15∙5)
Data are n (%), or means (SD). * Renal insufficiency was defined as an estimated glomerular filtration
rate of less than 60 mL per min per 1∙73 m². † De-novo coronary lesions include chronic total occlusions,
but not grafts or in-stent restenosis. ‡ Complex lesions were defined as lesion classification type B2 or C
according to the American College of Cardiology/American Heart Association.
ACS = Acute Coronary Syndrome, DAPT = Dual Antiplatelet Therapy, NSTEMI = non-ST-segment
elevation-myocardial infarction, PF-AES = Polymer-free Amphilimus-eluting Stents, PP-ZES =
Permanent Polymer Zotarolimus-eluting stents, RVD = reference vessel diameter, SD = Standard
Deviation, STEMI = ST-segment elevation-myocardial infarction.
Downloaded from http://ahajournals.org by on September 22, 2018
2110.1161/CIRCULATIONAHA.118.037707
Table 2. Lesion and procedural characteristics
Overall PP-ZES PF-AES p-value
(2111 lesions) (1024 lesions) (1087 lesions)
Procedural characteristics
No of stents per lesion* 1∙27 ±0∙58 1∙25±0∙57 1∙29±0∙59 0∙12
No of stents per patient* 1∙81 ± 1∙18 1∙73 ± 1∙09 1∙89 ± 1∙25 0∙05
Total stent length (mm)† 47∙7 ± 21∙2 47∙7 ± 21∙4 47∙7 ± 21∙2 0∙68
Stent diameter (mm) 3∙02 ± 0∙45 3∙01 ± 0∙45 3∙03 ± 0∙45 0∙14
Multi overlapping stents 394 (18∙7) 177 (17∙4) 219 (20∙02) 0∙13
Pre-dilatation 1886 (69∙8) 904 (70∙5) 973 (69∙2) 0∙48
Post-dilatation 1699 (64∙0) 757 (59∙6) 942 (68∙0)10.1161/CIRCULATIONAHA.118.037707
Table 3. Clinical events at 12 months after stent implantation
Overall PP-ZES PF-AES p-value
(n=1491) (n=744) (n=747)
Device-oriented primary endpoint* 88 (5∙9) 42 (5∙6) 46 (6∙2) 0∙67
Patient-oriented secondary endpoint† 177 (11∙9) 86 (11∙6) 91 (12∙2) 0∙69
Any death 35 (2∙3) 18 (2∙4) 17 (2∙3) 0∙86
Cardiac death 20 (1∙3) 10 (1∙3) 10 (1∙3) 1∙00
Myocardial infarction 53 (3∙6) 24 (3∙2) 29 (3∙8) 0∙49
Target-vessel myocardial 35 (2∙3) 17 (2∙3) 18 (2∙4) 0∙87
infarction
Stent thrombosis (definite, or probable)‡ 15 (1∙0) 6 (0∙8) 9 (1∙2) 0∙61
Acute (< 24 h) 4 (0∙3) 0 4 (0∙5) 0∙12
Subacute (24 h to 30 days) 5 (0∙3) 2 (0∙3) 3 (0∙4) 1∙00
Late (31 days to 12 months) 6 (0∙4) 4 (0∙5) 2 (0∙3) 0∙45
Any unplanned revascularization 73 (4∙9) 38 (5∙1) 35 (4∙7) 0∙71
Target-lesion revascularization 42 (2∙8) 20 (2∙6) 22 (2∙9) 0∙75
Stroke 12 (0∙8) 6 (0∙8) 6 (0∙8) 1∙00
Major Bleeding (BARC ≥ 3) 25 (1∙7) 13 (1∙7) 12 (1∙6) 0∙84
Data are n (%). Clinical outcomes were evaluated using Kaplan-Meier method using log-rank test, with p-
values that were indicative for superiority. * Device-oriented primary outcome of target-lesion failure was
defined as cardiac death, target-vessel myocardial infarction, or clinically driven target-lesion
revascularization. † Patient-oriented primary outcome of net adverse cardiac events was defined as: death,
myocardial infarction, stroke, any unplanned revascularization, or major bleeding (BARC>3) according
to bleeding academic research consortium. ‡ Stent thrombosis according to Academic Research
Downloaded from http://ahajournals.org by on September 22, 2018
Consortium definitions.
BARC = Bleeding Academic Research Consortium, DAPT = Dual Antiplatelet Therapy, PF-AES =
Amphilimus Eluting Stent, PP-ZES = Permanent Polymer Zotarolimus Eluting Stent, TLF = Target-lesion
Failure, ST = Stent Thrombosis.
2310.1161/CIRCULATIONAHA.118.037707
Figure Legends
Figure 1. Trial profile.
PCI = Percutaneous Coronary Intervention, TAVI = Transcatheter Aortic Valve Implantation,
PF-AES = Polymer-free Amphilimus-eluting Stent, PP-ZES = Permanent Polymer Zotarolimus-
eluting Stent.
Figure 2. Kaplan-Meier estimates of the device-oriented primary endpoint, and individual
components.
(A) Target-lesion Failure, (B) Cardiac Death, (C) Target-vessel Myocardial Infarction, and (D)
Target-lesion Revascularisation. PF-AES = Polymer-free Amphilimus-eluting Stent, PP-ZES =
Permanent Polymer Zotarolimus-eluting Stent.
Downloaded from http://ahajournals.org by on September 22, 2018
Figure 3. Subgroup analysis on the primary endpoint at 12-months.
Troponin-status and diabetes mellitus were pre-specified subgroups whereas sex, age, and
complex B2/C lesions were performed post-hoc.
AES = Amphilimus-eluting Stent, B2/C lesions according to the American College of
Cardiology/American Heart Association classification, DAPT = Dual Antiplatelet Therapy, HR
= Hazard Ratio, CI = Confidence Interval, PF-AES = Polymer-free Amphilimus-eluting Stent,
PP-ZES = Permanent Polymer Zotarolimus-eluting Stent, ZES = Zotarolimus-eluting Stent.
2410.1161/CIRCULATIONAHA.118.037707
Figure 4. Principal characteristics of the Polymer-free Amphilimus-eluting Stent.
The coronary stent platform is made from a thin-strut (80µm) cobalt-chromium alloy, coated
with an ultra-thin (Downloaded from http://ahajournals.org by on September 22, 2018
Downloaded from http://ahajournals.org by on September
Downloaded from http://ahajournals.org by on September 22, 2018
Downloaded from http://ahajournals.org by on September 22, 2018
You can also read

















































