Clinical Electrodiagnostics in the Diagnosis of Radiculopathy January 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Clinical Electrodiagnostics in the
Diagnosis of Radiculopathy
January 2021
Jeremy Simon, MD
Assistant Professor of Rehabilitation Medicine
Sidney Kimmel Medical College of Thomas
Jefferson University
Division Chief, Department of Physical
Medicine and Rehabilitation
The Rothman Institute
Outline Pathophysiology Nerve conduction studies Late responses Needle Electromyography Cases

Rothman Institute of Orthopaedics at
Thomas Jefferson University
My Clinical Criteria
for Diagnosing
Radiculopathy
Myotomal pain
Dermatomal symptoms
Physical exam findings
Provocative
Reflex changes/pathologic
Gait/balance testing
Rothman Institute of Orthopaedics at
Thomas Jefferson University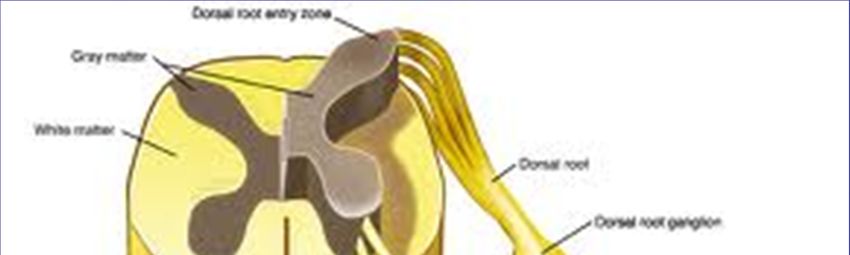
What Do I Use
Electrodiagnostics
For?
Rule out other IN A CLEAR CUT
conditions: RADICULOPATHY, I
CTS DON’T BELIEVE THAT
AIDP/CIDP EDX CONTRIBUTES TO
Diabetic amyotrophy MANAGEMENT
Peroneal Neuropathy
Rothman Institute of Orthopaedics at
Thomas Jefferson University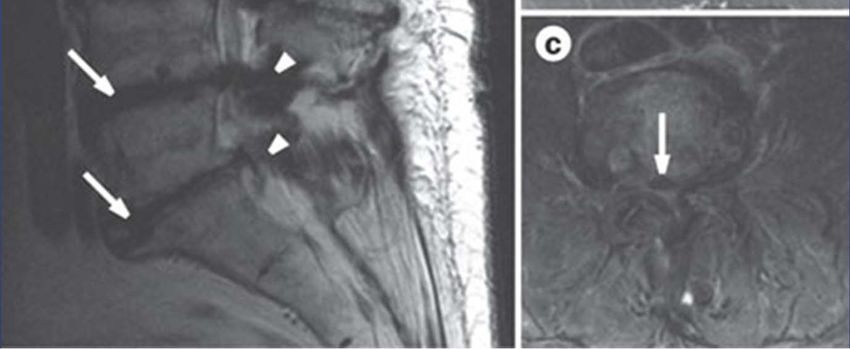

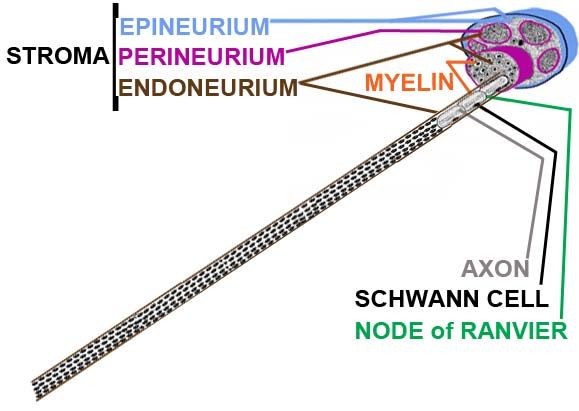
Anatomy
Rothman Institute of Orthopaedics at
Thomas Jefferson University
Pathophysiology Compressive
Pathophysiology Compressive
Pathophysiology (other)
Idiopathic (autoimmune/microvascular?)
Diabetic/Non‐Diabetic
Lumbosacralradiculoplexopathy (Bruns‐Garland
Syndrome)
Neuralgic amyotrophy (Parsonage‐Turner
Syndrome)Electrodiagnostics in Radiculopathies
Nerve Conduction Studies
Motor NCS
Latency
Conduction velocity
Amplitude
Dysmyelination/conduction block vs axonopathySensory Nerve Conductions
Preganglionic
sensory
neurons
Anterior
disc horn cell
Post‐ganglionic
motor neuronsL5-S1 Axial View
Late Responses
F‐Waves
Motor‐motor,5% CMAP Dual innervation of
Roots studied? muscle
Frequently normal Sensory neurons not
Slowing may not occur studied
in the fibers tested, F waves in compressive
obscured radiculopathy
(Wilbourn)?
Rothman Institute of Orthopaedics at
Thomas Jefferson UniversityH‐Reflex
Sensory‐motor
Like F‐wave, abnormal if any portion is
affected in the pathway
Mostly performed in the S1 pathway
Can use amplitude ratio and/or latency side to
side (Needle Electromyography
Oldest/most established method of defining
nerve root compromise (Johnson 1965)
Assesses motor fibers only, majority of
findings in axonal loss (Wilbourn 1988)
Fibrillations/sharp waves in specific nerve root
distribution with absence in other myotomes
if axonal death is recent.Needle Electromyography
Fibrillations/sharp waves: MOST sensitive
indications of recent motor axon loss
Motor unit action potential abnormalities may
be minimal and not detectable (Wilbourn 1988,
Dumitru 2002)
Sensitivity 50‐71% (AANEM practice
parameters 1999)
Correlation with imaging and surgical findings
65‐85% (ibid)Needle EMG
(Lumbosacral)
Utility for :
Peripheral limb EMG (Class II, Level B rec.)
Paraspinal mapping (beyond scope, Class II
Level B)
H reflex for S1 (Class II and III, Level C)
Low sensitivity for :
F waves
Cho et al Utility of edx testing in evaluating pts with ls radiculopathy: an
evidence based review MuscNer 2010Needle EMG
Fibrillations occur in proximal to distal
sequence in recent axonopathy
Acute lesion: can take up to 5 to 6 weeks to
develop fibrillations in the distal lower
extremity muscles, usually seen in 3 weeks
(Lambert 1971)Needle EMG
Total myotomal involvement rare (Wilbourn
1998)
Variable root innervation of muscles
Root compromise often incomplete/minority
of fibers affected
Timing
Irregular fibrillations and acuity (Wilbourn)Needle EMG
• Earliest finding can be REDUCED
RECRUITMENT PATTERN
• “Chronic” polyphasic –what does it imply?
• Old static lesions polys only; not an indicator
of an active ongoing lesion (Wilbourn 1998)NORMAL NERVE CRUSH from DISK
CRUSH > AXONAL DEATH AXONAL DEATH > SCHWANN
CELL PROLIFERATION CALLED
BAND of BUNGNERAXONAL REGENERATION after MORE AXONAL REGENERATION 6 MONTHS. SMALLER AXON & after 1 YEAR. FURTHER SHRINKAGE INCREASED INTERNODES DISTAL ENDONEURIAL TUBE
DISTAL ENDONEURIAL > FIBROTIC INTRANEURAL NEUROTMESIS:
= INTRANEURAL NEUROTMESIS ONLY REINNERVATION from
REMAINING INTACT AXONSCRUSH from DISK AXON DEMYELINATED >
RAPID REMYELINATION
and RECOVERYNeedle EMG
• C5 and C6 radiculopathy
– Difficult to distinguish, often grouped together
– Difficult to make a distinction from upper trunk
lesion
– Rhomboids
– C6 more common clinically (Dumitru 2002)
• C7 radiculopathy
– Most common cervical radiculopathy (Yoss 1957)
– Easiest to localize; circumscribe lesion by normal
C5/6 and C8/T1 innervatedmuscles and
abnormalities in C7 distributionNeedle EMG
C8/T1 radiculopathy
Significant myotomal overlap
C8 more common clinically (C7‐T1 disc herniation)
Lower trunk lesions may mimic
Paraspinals helpful
Medial antebrachial cutaneous responseNeedle EMG
L2,3,4 radiculopathies
Significant overlap
Tibialis anterior
Mostly proximal lower limb muscles therefore
reinnervate sooner
Diabetic amyotrophy?
No reliable sensory NCS for evaluating L2‐4
Difficult to distinguish from plexopathy.
Saphenous technically difficultNeedle EMG
• L5 radiculopathy
– EMG findings
– Normal superficial peroneal response…except if not (Levin
K 1998)
– CMAPs
• S1/2 radiculopathy
– Often lumped together, but S2 radiculopathy clinically rare
– H-reflex
– CMAP amplitude
– Can be bilateral (Hasegawa 1996)
– Location of DRG may be vulnerable (more medial in canal)Guidelines (NOT standards)
EMG/NCS‐ What to test?
• American Association of Neuromuscular and Electrodiagnostic
Medicine (AANEM) guidelines, for radiculopathy screen, a
“reasonable examination consists of”:
• Cervical radiculopathy
– A sensory and motor NCS (low threshold for examining ulnar
and median)
– An F wave to exclude polyneuropathy (optional)
– A needle EMG screen: 6 upper limb muscles, including the
paraspinals (marginal increase in sensitivity if 7) (Lauder TD
1996, Dillingham 1999, 2001, 2002)
– Contralateral 1 or more muscles if abnormalites (optional)
– At least 1 muscle innervated by C5, C6, C7, C8, T1 in
symptomatic limb.What to study (guidelines)?
Lumbar radiculopathy:
One motor and sensory NCS
F wave or H‐reflex to exclude polyneuropathy
(optional)
Needle EMG screen: 5 lower limb muscles
including the paraspinals (adding one muscle
marginally increases sensitivity). If s/p posterior
lumbar surgery, can exclude paraspinals and 8
distal muscles optimal (Dillingham 2000, 2002)Pitfalls
DRG location (Levin 1998)
L5 up to 40% DRG in spinal canal
Abnormalities in foot muscles
Dysmyelation vs predominance of axonal
pathology
Timing/reinervation
Overlap of innervation
Prior spinal surgery/paraspinalsCases (names have been changed)
50 year old with pain
radiating right posterior
limb
Lifting twisting injury 3
months ago
pain worse w/sitting and
flexion activities, can’t sit
>20 mins
“Can I return to work
today?” Positive SLR and slump test
on right
4/5 FHL, gastroc, TFL
strength on right
Decreased sensation to light
touch in S1 dermatome right
Absent right ankle jerk
Why do it?Electrodiagnostic study
Normal sensory and motor NCS
Reduced right H‐reflex amplitude, normal left
H‐reflex (ratio 0.2)
Needle EMG: +1 fibs/sharp waves in the
medial gastroc, TFL and lower lumbar
paraspinals remainder normal.Clinical and
Electrodiagnostic
Impression
There is clinical and electrodiagnostic
evidence of SUBACUTE RIGHT S1
RADICULOPATHY as demonstrated by the
fibrillations in the S1 innervated muscles.
‐‐‐does the H reflex abnormality say it’s a new
problem?
‐‐‐what if sural response had reduced
amplitude?REASONS FOR PROGNOSIS Seddon & Sunderland’s classification systems can be broadened to include the potential for an axonotmesis to evolve into an intraneural neurotmesis.
PRE-CRUSH – 4 NORMAL INTERNODES
(NEURAPRAXIA0• pain radiating right
posterior limb for 1 month
• 3 previous work comp
claims for back pain over 12
years, months of PT, anti-
inflammatory meds, muscle
relaxers, membrane
stabilizers, oxycodone
• MRI disc bulges at L4-5, L5-
S1
• “I can’t go back to work!
They don’t follow the
restrictions you gave!”
Rothman Institute of Orthopaedics at
Thomas Jefferson University• Positive supine SLR right,
negative slump and seated
SLR
• Decreased sensation to pin
prick but not light touch in a
non-dermatomal
distribution
– Why is that important?
• Normal reflexes except +1
right ankle jerk
• 5/5 strength left, poor effort
right/give-way weakness
• Why do the study?Electrodiagnostic study
Normal sensory and motor NCS
Prolonged right H‐reflex, normal left H‐reflex
Needle EMG: polyphasic motor units of
increased duration in the medial gastroc, TFL,
remainder normalPRE-CRUSH – 4 NORMAL INTERNODES
Clinical and
Electrodiagnostic
Impression
There is electrodiagnostic evidence for an OLD
(static) RIGHT S1 RADICULOPATHY. Clinically,
this does not support the patient’s sensory
symptoms involving the entire right lower
extremity as well as the imaging findings.Bigg Hits‐ History
• Professional football
safety
• Head-first tackle 4 weeks
ago, immediate pain in
neck and right arm
• 4/5 strength in right
deltoid, biceps, and
triceps
• Altered sensation in the
1st digit of left hand,
reduced bicep reflex
• MRI right C5-6 HNP
Rothman Institute of Orthopaedics at
Thomas Jefferson UniversityElectrodiagnostic Study
Normal median/ulnar CMAPs
Normal median, ulnar, radial and lateral
antebrachial cutaneous SNAPs
Needle EMG: +2 fibrillations in the right
deltoid, biceps and cervical paraspinals
without polyphasia, remainder of study
normalClinical and
Electrodiagnostic
Impression
There is clinical and electrodiagnostic
evidence of a acute right C6 radiculopathy.
Uh, oh! Bad, right?Addendum…
This player had a cervical epidural steroid
injection, no pain and full strength at 4 weeks,
went back to play pro football!PRE-CRUSH – 4 NORMAL INTERNODES
CRUSH from DISK AXON DEMYELINATED >
RAPID REMYELINATION
and RECOVERYMya Sholdahurtz
• 58 year old female factory worker with h/o
neck pain
• September 28, 2012 awoke at 2 am with
severe right shoulder pain
• Went to ER, rx with pain meds, muscle
relaxer and antiinflammatories
• Pain subsided 3 days later, followed by
inability to raise right arm
• Sent to shoulder surgeon, minimal arthritic
and cuff tendonosis on MRI shoulderPhysical examination 2/5 right external rotator cuff, biceps strength 4/5 wrist extensor, 4+/5 right triceps Sensation normal Absent right biceps reflex Negative Hoffman’s sign
Mya Sholdahurtz
MRI cervical spine large right sided C5‐6
disc/osteophyte complex, C4‐5 small
foraminal discElectrodiagnostic Study
• Normal Motor NCS Median, Ulnar, Radial
• Normal Sensory NCS Median, Ulnar, Radial,
Lateral and Medial Antebrachial cutaneous
• EMG 3+ large irregular fibs and sharp waves,
reduced recruitment in deltoid, biceps,
polyphasic units
• Pronator and ECRB 2+ large fibs, psw,
reduced recruitment, polyphasic motor units
• +1 fibs, small in cervical pspDiagnosis?
Acute right motor axonal brachial plexopathy
involving the upper trunk consistent with
neuralgic amyotrophy (Parsonage‐Turner
Syndrome) with superimposed chronic C6
radiculopathyIya Trojenick
71 year old female with bilateral lower
limb claudication and back pain
Severe L4/5 foraminal and central stenosis
and grade 2 spondylolithesis,moderate L5
central stenosis, severe bilateral L5-S1
foraminal stenosis
Underwent bilateral L5 TF ESI
Left side ok, severe pain during and after
right side procedure Right foot drop following procedure
Dr. Charlatan orders MRI knee:“Baker’s
cyst”
Told nothing to do for it
Exam: 2/5 right TFL, tib anterior, 4/5
gastroc, reduced sensation in the dorsum
of right foot
Trendellenberg and steppage gait EMG: right peroneal amplitude 0.5mV,
left 2.5mV, +3 fib/sharp waves in TA, TFL,
peroneus longus, reduced recruitment
with polyphasic units of increased
durationElectrodiagnostic
Impression
There is clinical and electrodiagnostic
evidence for a SEVERE RIGHT L5
RADICULOPATHY. GIVEN THE TIMING
AND MECHANISM OF THE INJURY
WITH PERSISTENT WEAKNESS AND
SPONTANEOUS ACTIVITY IN BOTH
THE PROXIMAL AND DISTAL
MUSCULATURE THE PROGNOSIS FOR
RECOVERY IS POOR.INTRANEURAL NEUROTMESIS: ONLY RINNERVATION from REMAINING INTACT AXONS ENDONEURIAL FIBROSIS = INTRANEURAL NEUROTMESIS
Fancy Mainline-
Sonsadoc
90 year old female with history of mild low
back pain
Awoke with acute onset of bilateral lower
cramping pain, lower extremity weakness
and tingling
Previously ambulatory without assistive
device, now in wheelchair after 2 daysPeasant’s Examination
Reduced sensation to light touch, pinprick,
and vibration in a stocking distribution in
the legs
Absent patellar and quad reflexes
3/5 TA, gastroc, peroneus longus
5/5 Quad, TFL, hip abductor strengthNCS findings
Peroneal distal latency 12.5ms, amplitude
0.8mV, increased duration, conduction
velocity 20m/s
Tibial distal latency 13ms, amplitude 1mV,
increased duration, conduction velocity
21m/s
Absent sural, superficial peroneal and F
waves
Ulnar prolonged, increased duration,
reduced velocity, prolonged F wavesEMG findings
Reduced recruitment with 1+fib in
bilateral TA, gastroc, peroneus longusImpression
There is clinical and electrodiagnostic
evidence for an ACQUIRED DIFFUSE
SENSORY AND MOTOR
DYSMYELINATING PERIPHERAL
POLYNEUROPATHY CONSISTENT
WITH GUILLAIN-BARRE SYNDROMESummary
CLINICAL SUSPICION
Electrodiagnostics are a useful tool in
confirming your clinical impression and ruling
out other causes of patient symptoms and
signs
Limitations/Pitfalls
Keep in mind the timing and potential for
false negativesThank you!
References
• Johnson EW, Melvin J: Value of electromyography in lumbar
radiculopathy. Arch Phys Med Rehabil 1971;52:239-243.
• MacIntosh JE, Valencia F, Bogduk N, Munro RR: The morphology
of the human lumbar multifidus. Clin Biomech 1986;1:196-204.
• Nicotra A, Khalil NM, O'neill K.Br J: Cervical radiculopathy:
discrepancy or concordance between electromyography and
magnetic resonance imaging? Neurosurg. 2011 Sep 7
• Tong HC.Am J: Specificity of needle electromyography for
lumbar radiculopathy in 55- to 79-yr-old subjects with low back pain
and sciatica without stenosis Phys Med Rehabil. 2011
Mar;90(3):233-8
• Plastaras CT, Joshi AB The electrodiagnostic evaluation
of radiculopathy. Phys Med Rehabil Clin N Am. 2011 Feb;22(1):59-
74. Epub 2010 Dec 3.
• Cauda equina anatomy II: extrathecal nerve roots and dorsal root
ganglion. Spine 1990; 15:1248-51.References
• Lambert E: Electromyography, in Youmans J (Ed): Neurological Surgery, Vol 1. Philadelphia, W.B.
Saunders, 1973, pp 358-367
• Wilbourn AJ: The value and limitations of electromyography in the diagnosis of lumbosacral
radiculopathy. In Hardy (Ed): Lumbar disc disease. New York, Raven, 1982 pp 65-109.
• Yoss RE et al: Significance of asigns and symptoms in localization of involved roots in cervical disc
protrusion. Neurology 7:673-683, 1957.
• Dillingham TR: Electrodiagnosis of radiculopathies: How many and which muscles to study. AANEM
course 2000 pp23-35.
• Lauder TD, Dillingham TR. The cervical radiculopathy screen: optimizing the number of muscles
studied. Muscle Nerve 1996;19:662-665.
• Haig AJ, Talley C et al: Paraspinal Mapping: Quantified needle electromyography in lumbar
radiculopathy. Muscle Nerve 1993;16:477-484.
• Haig AJ, Lebreck DB et al: Paraspinal Mapping: Quantified needle electromyography of the paraspinal
muscles in persons without low back pain. Spine 1995;20:715-721.
• Dillingham TR, Lauder TD, Andary M, Kumar S, Pezzin LE, Stephens RT, et al.Identifying lumbosacral
radiculopathies: an optimal electromyographic screen. Am J PhysMed Rehabil 2000;79:496–503.
• Dillingham TR, Lauder TD, Andary M, Kumar S, Pezzin LE, Stephens RT, et al.
Identificationofcervicalradiculopathies:optimizingtheelectromyographicscreen.AmJPhys Med Rehabil
2001;80:84–91.
• T.R. Dillingham, Electrodiagnostic approachto patients with suspected radiculopath. Phys Med Rehabil
Clin N Am 13 (2002) 567–588References
• Levin K: L5 Radiculopathy with reduced superficial
peroneal responses: intraspinal and extraspinal
causes. MuscNerv.1998;213-7.
• Hasegawa, Toru et al: Morphometric Analysis of the
Lumbosacral Nerve Roots and Dorsal Root Ganglia by
Magnetic Resonance Imaging. Spine. May 1996,
Volume 21(9), 1;1005-1009.
• Jankus WR, Robinson LR et al: Normal limits of side-
to-side H-reflex amplitude variability. Arch Phys Med
Rehabil.; 1994 Jan75(1):3-7
• Cho SC, Utility of electrodiagnostic testing in
evaluating patients with lumbosacral radiculopathy:
an evidence based review MuscNer; 2010 42:276-82You can also read

















































